This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.

The COVID-19 pandemic has changed social, family, and interpersonal relationships and behaviors. Several studies have identified the increase in psychiatric disorders in the general population (Fountoulakis et al. Psychiatry Res 2022; 315 114702) and an increase in episodes of disease in people already affected by these diseases (Taquet et al. Lancet Psychiatry 2022; 9 815-827; Zhu et al. Adults Psychiatry Res 2021; 301 113959). These episodes were accentuated by the severe limitations that occurred during the greatest peaks of the pandemic. However, few studies have evaluated the effects of these restriction periods on the levels of hetero or self-directed aggression in patients staying in residential facilities.
To evaluate the effects of the COVID-19 pandemic on aggression and psychomotor agitation crises in patients hospitalized in a psychiatric rehabilitation centre.Evaluate the differences in these behaviors in the different stages of external limitation in patients suffering from psychiatric disorders.
This observational study was conducted in a residential psychiatric rehabilitation facility since the outbreak of the COVID-19 pandemic in Italy (March 2020 through September 2020). 354 patients were enrolled in the study. All guests had psychiatric disorders defined according to DSM-5 diagnostic criteria. Table 1 shows age mean and diagnosis at admission.
The several periods were recorded in the number of cases of psychomotor agitation and heterodirect aggression and an increase in emergency pharmacological interventions.
The following rating scales were administered in all patients: BPRS-18, BPRS Agitation (item item 6 tension + 10 hostility+ 17 excitement), GAF, and Epitrack.
The collected data were collected and statistically analyzed with the EZAanalyze 3.0 software in the Microsoft Excel Office.
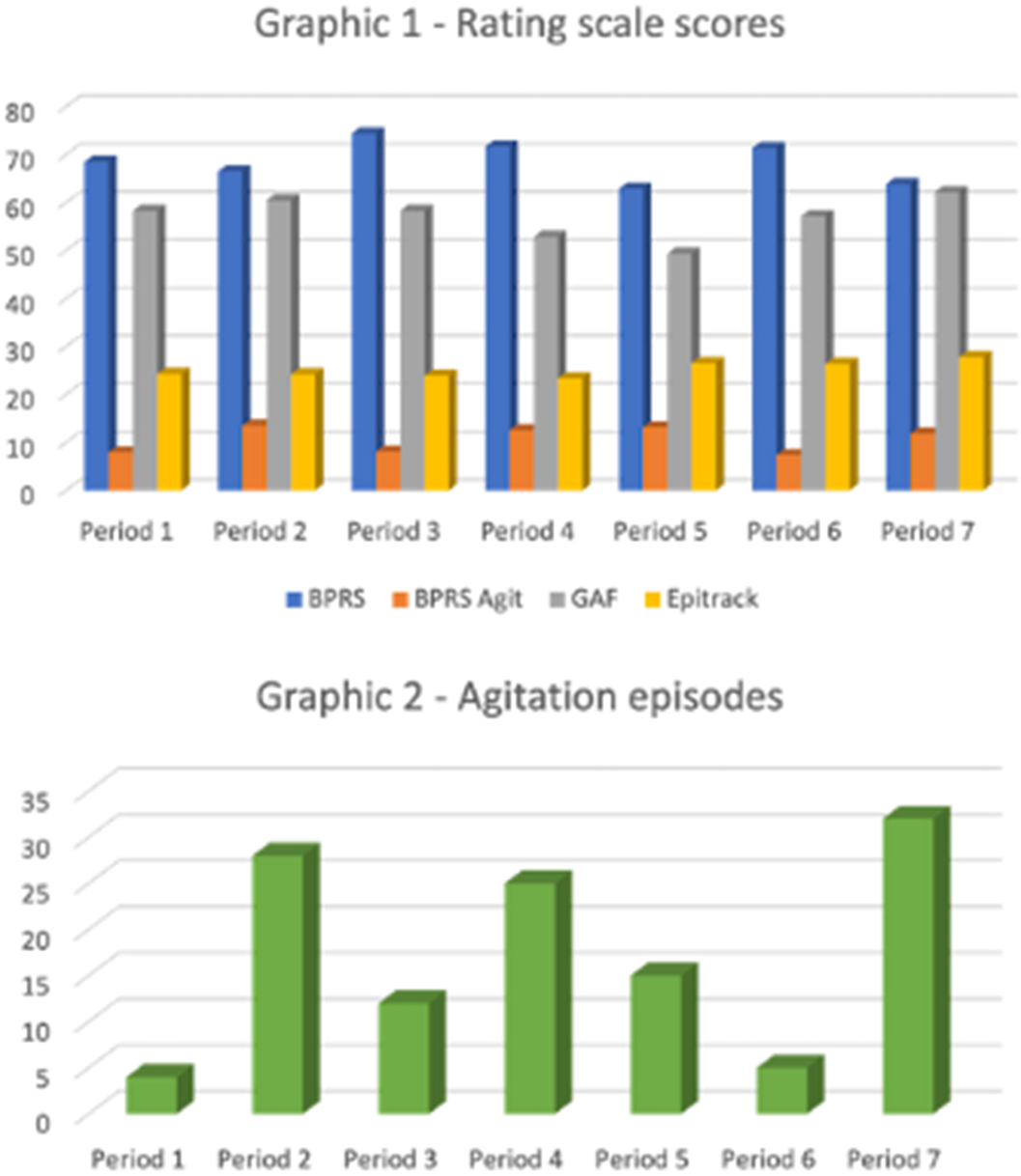
In tables 1 and 2 and in Graphics 1 and 2 the results obtained from our study are shown. We observed a reduction in the number of agitation and aggression episodes in periods 1, 3 and 6 (4, 12 and 5, respectively). In these same periods, the BPRS agit subscore score was also lower than in the other periods (7.92, 8.08, 7.42, respectively).
Image:
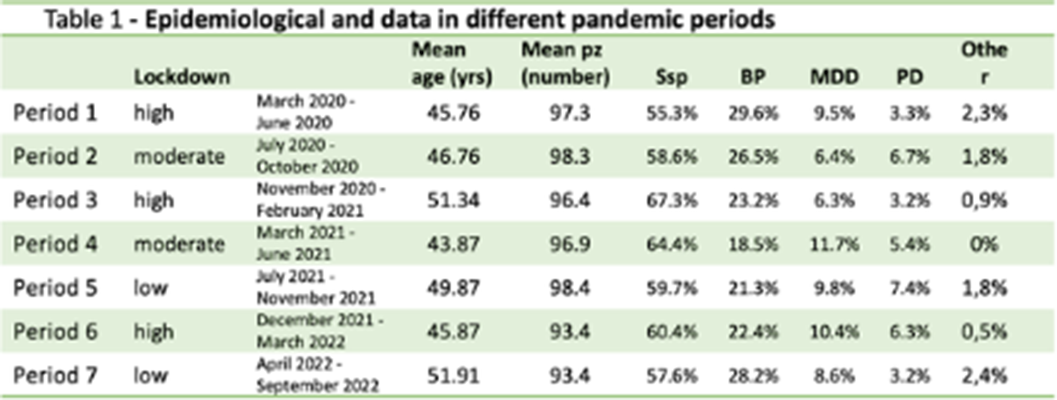
Image 2:
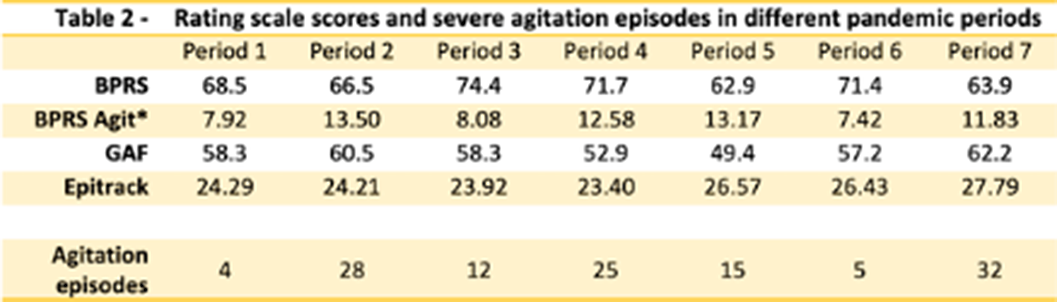
Image 3:
Differently to expected data, the number of episodes of psychomotor agitation and heterodirect aggression proved to be reduced in the periods of greater restraint and limitation. Instead, the levels increased in the month following the reduction of such restrictions characterized by visits with family members, planned outings. it is difficult to give a reliable and definitive explanation to these results. However, the feeling of protection, risk reduction and potentially dangerous stimuli could guide the explanation of the results obtained.
None Declared
Multiple sclerosis is considered one of the leading causes of neurological non-traumatic disability among young people. Given the chronic progressive nature of the disease, psychiatric disorders are more prevalent among those patients as reported in the literature; however, the data in Saudi Arabia is lacking.
The study aimed to estimate the prevalence of psychiatric disorders among MS patient in Saudi Arabia.
This was a cross-sectional multi-centered study, including patients with multiple sclerosis. Participants were interviewed and asked to fill a validated survey that consisted of demographics, Patient Health Questionnaire-9 (PHQ-9), and Generalized Anxiety Disorder-7 (GAD-7) questionnaire. Descriptive statistics were performed, and the analysis were made using Chi-square, Fisher’s exact, and ANOVA tests as appropriate.
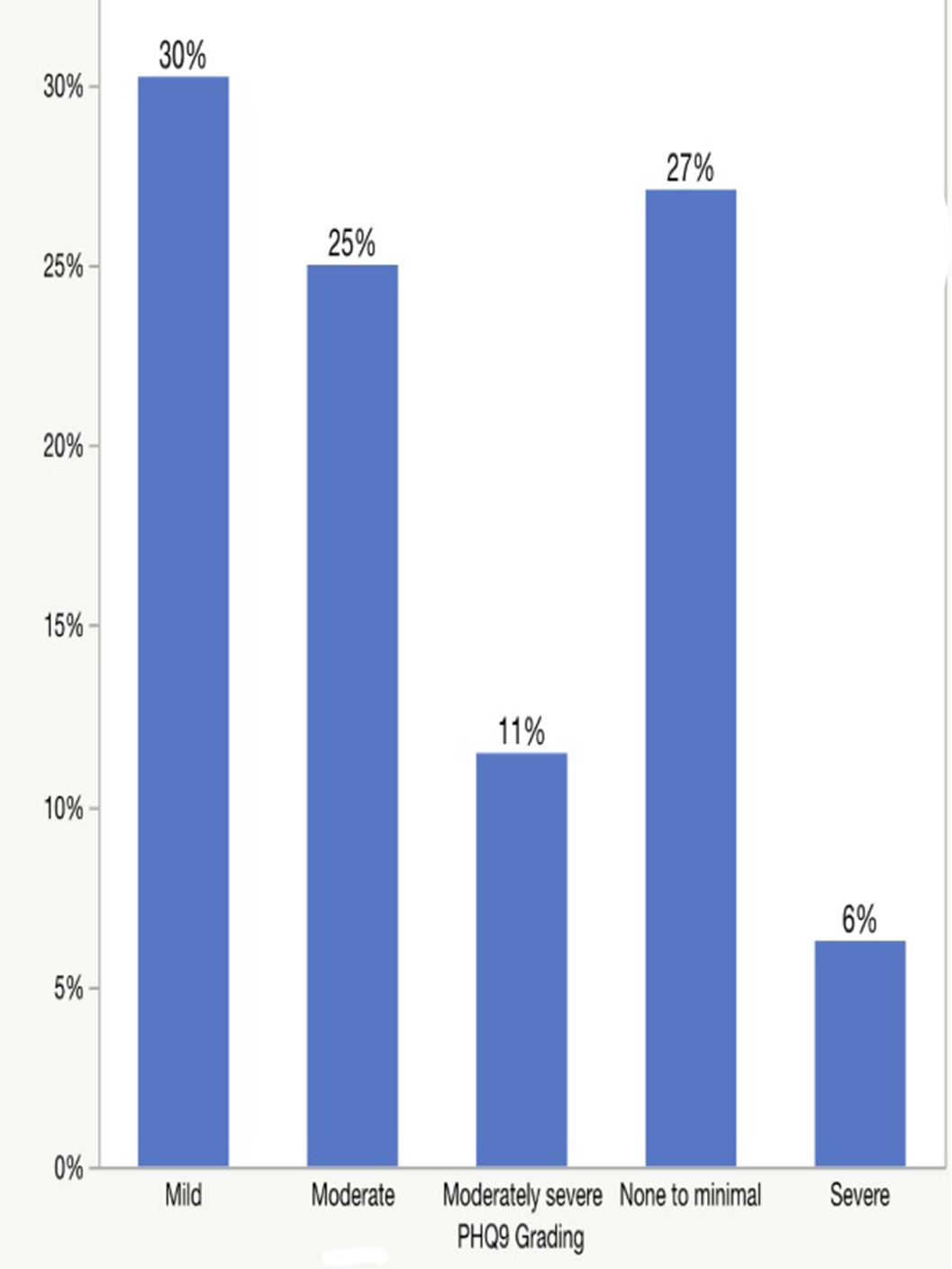
A total of 192 participants were included in the study. Based on a cutoff score of > 10 in the GAD-7 and PHQ-9 scales, the prevalence of anxiety was 26.1% (n-50), with majority of the participants having minimal anxiety (40%); meanwhile, the prevalence of depression was 42.7% (n=82), and most of them had mild depression (30%). [table 1, image 1 and 2] Females participants significantly scored higher in GAD-7 and PHQ-9 compared to males (p-value= 0.0376 and 0.1134, respectively). [table 2 and 3] In addition, no significant association was detected between functional disability (EDSS score) and the prevalence of anxiety and depression.Items GAD 7 score, Mean (SD) 6.5 (±4.9) GAD 7, N (%) Fit for Anxiety (>10) * 50 (26%) Not Fit for Anxiety (<10) * 142 (74%) PHQ 9 score, Mean (SD) 8.8 (±6.1) PHQ 9, N (%) Fit for Depression (>10) * 82 (42.7%) Not Fit for Depression (<10) * 110 (57.3%) Fit for Anxiety (n=50) Not Fit for Anxiety (n=142) P Value Gender, N (%) - Male 10 (20%) 51 (35.9%) 0.0376 - Female 40 (80%) 91 (64.1%) N(%) Fit for Depression (n=82) Not Fit for Depression (n=110) P Value Gender, N (%) - Male 21 (25.6%) 40 (36.4%) 0.1134 - Female 61 (74.4%) 70 (63.6%)
Image:
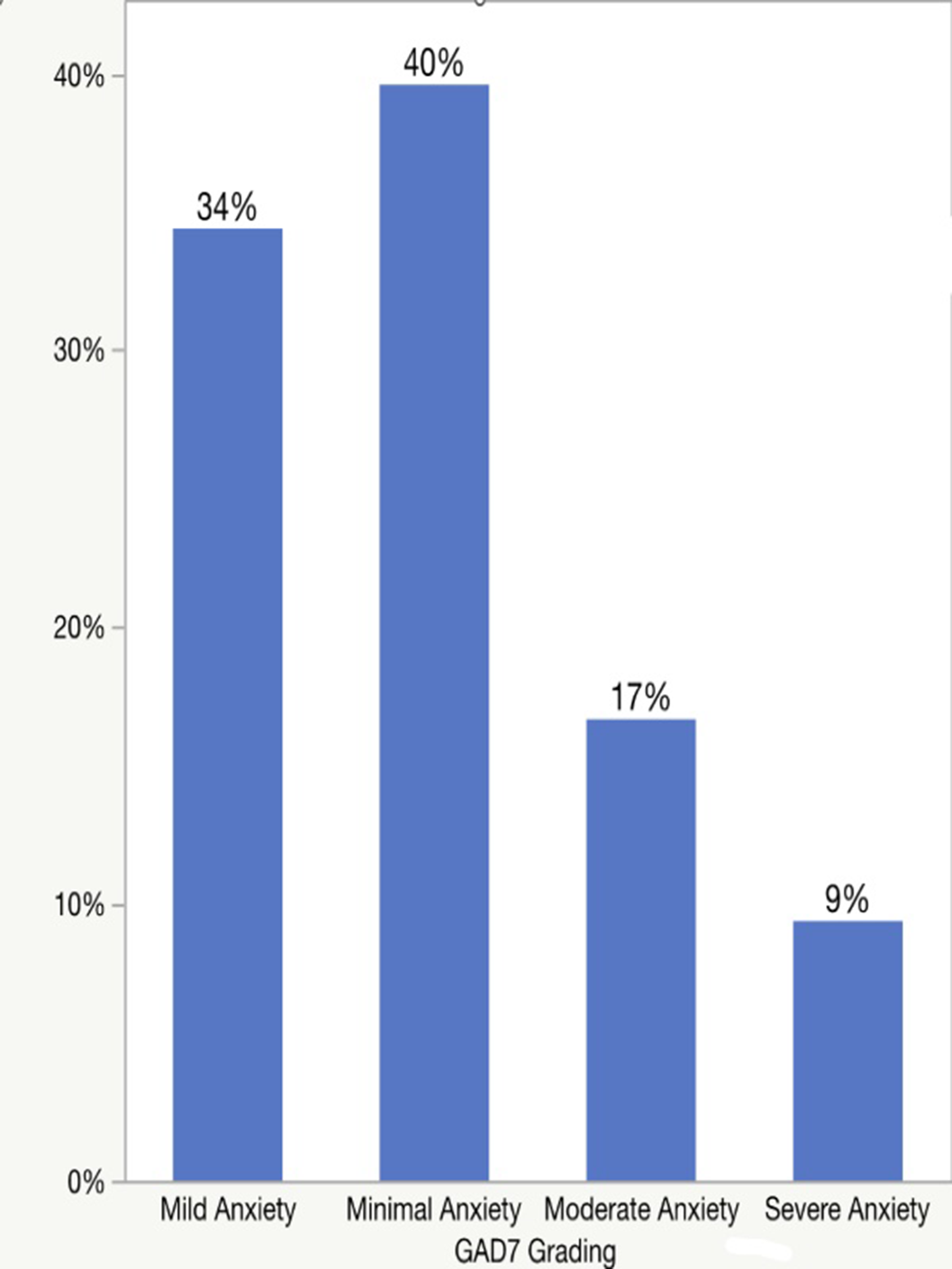
Image 2:
This study reported high level of anxiety and depression among MS patients, with females being more affected. Since these co-morbid disorders could affect the disease course negatively, screening is of paramount significance.
None Declared
