This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.

Following the protracted duration of the coronavirus pandemic, the Serbian health system now faces a period of mid- and long-term health consequences in patients that have recovered from the acute phases of infection.
A 57-year-old woman presented at a psychiatric examination complaining of forgetfulness, listlessness, fatigue, insomnia, low mood, and decreased efficacy in daily activities, two months after infection with the SARS-CoV-2 virus. The clinical picture of acute COVID-19 infection was accompanied by an elevated body temperature, a cough, an increases of CRP, and X-ray verified bilateral pneumonia with band-like speckled shadows of milk glass density. Before infection, she was vaccinated with 3 doses of the Sinopharm Covid-19 vaccine.
The following examinations were made: MRI of endocranium, HDRS, laboratory examination, and neuropsychological testing.
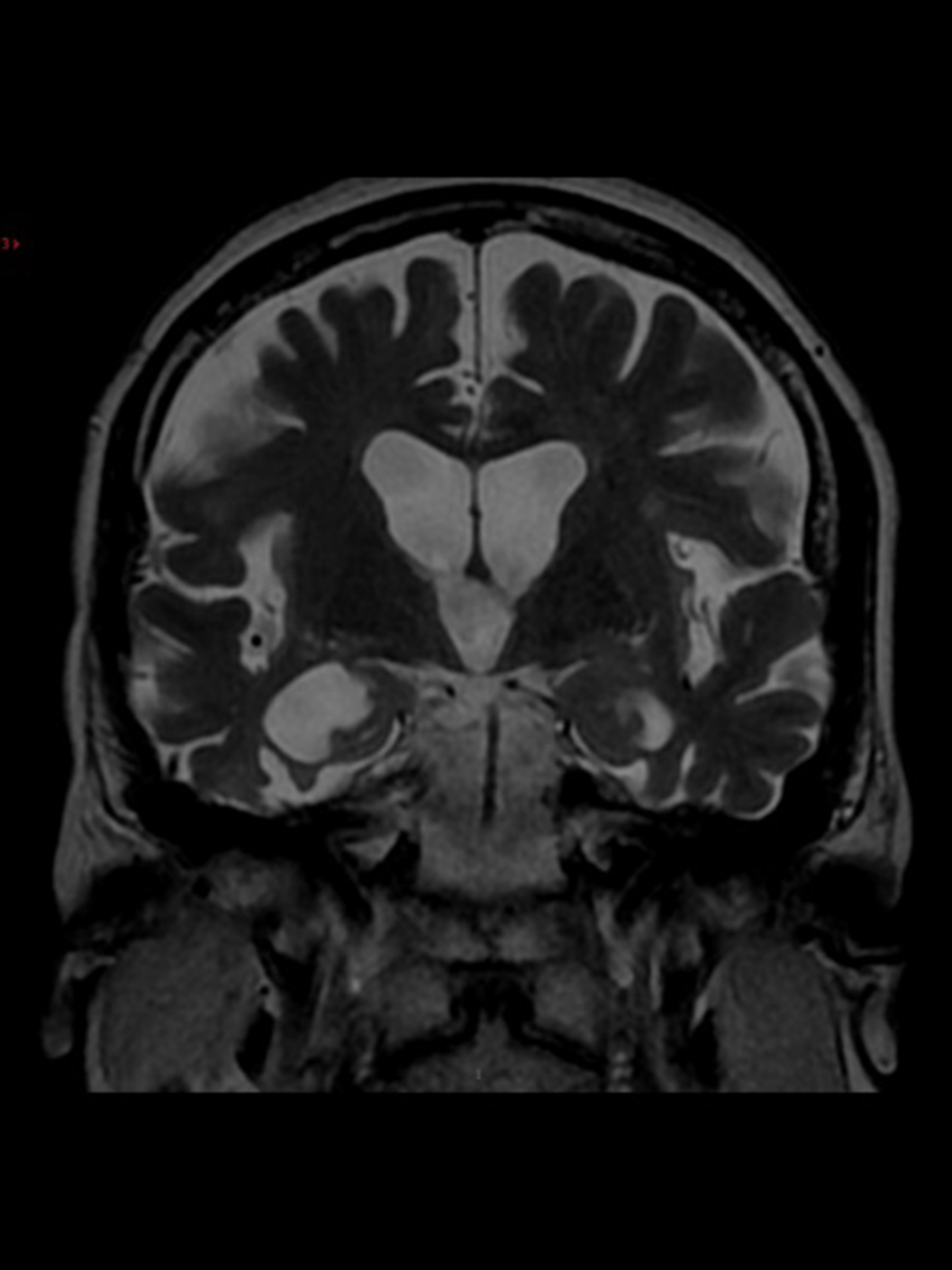
MRI of endocranium (figure 1): extensively cortico-subcortical lesions extensively within both cerebral hemispheres, dominantly in the temporo-insular regions, in association with partial parenchymal defects and a high degree of atrophy - the overall morphology corresponds to chronic encephalopathy, which is of non-specific morphology; HDRS score of 24; elevated serum levels of IgM, IgG, albumin in serum 7.05 (35-55), albumin in cerebrospinal fluid 812.0 (0-35), albumin index 115.8 (<9.0); IEF: oligoclonal bands in CSF and serum; neuropsychological testing: decrease in general mental activity and visuoperceptive and visuospatial ability. Due to the temporal connection between infection with the SARS-CoV-2 virus and presented symptoms, the patient was diagnosed with post-acute COVID-19 encephalopathy.
Image:
A meticulous follow-up post-acute SARS-CoV-2 infection monitoring and care could decrease mortality and prevent debilitating neurological and other burdens, especially in risk groups.
None Declared
