
Abstracts of the 31st European Congress of Psychiatry
Volume
66 -
Special Issue S1
-
March 2023

Contents
e-Poster Viewing
Abstract
Early-onset schizophrenia: an adolescent case report
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1049
-
- Article
-
- You have access
- Open access
- Export citation
Extrapyramidal syndrome in psychotic depression: a case report.
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1049-S1050
-
- Article
-
- You have access
- Open access
- Export citation
Effectiveness and quality of life improvement in young adult schizophrenia patients treated with Abilify Maintena
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1050
-
- Article
-
- You have access
- Open access
- Export citation
Schizophrenia and myasthenia gravis: a case report
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1050
-
- Article
-
- You have access
- Open access
- Export citation
Schizophrenia and Mega cisterna magna: a Case report
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1051
-
- Article
-
- You have access
- Open access
- Export citation
Paraphrenia - forgotten or undiagnosable psychosis?
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1051
-
- Article
-
- You have access
- Open access
- Export citation
Relation between Negative Symptoms and Core Stability as an Indicator of Functional Exercise Capacity in Schizophrenia
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1051-S1052
-
- Article
-
- You have access
- Open access
- Export citation
Evaluation of Vitamin D in the serum of in-hospital patients with psychosis. Retrospective study.
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1052-S1053
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
The reduction of vitamin D (VitD) has often been associated with pathological cognitive processes and in general with various mental illnesses2,3. More frequent reports of reduced concentrations of VitD concern patients with schizophrenia, however it has not been clarified whether this concerns the pathology itself of the disorder or if nutritional factors are involved1.
ObjectivesThe measurement of VitD in the serum of hospitalized patients with mental illness (schizophrenia) compared to the levels of people without mental illness.
MethodsThe serum levels of VitD were measured in the serum of 45 psychiatric patients of psychiatric hospital “Dromokaiteion” (22 men and 23 women) mean age 59 ±14 years. The control group consisted of 49 healthy subjects (24 men and 25 women) with a mean age of 57 ±14 years (Table 1). Serum VitD levels were measured on the Architect ci4100 immunobiochemical analyzer, Abbott Laboratories Ltd, by the chemiluminescent microparticle immune assay (CMIA) method and according to the manufacturer’s instructions. The statistical analysis of the data was done with the software program SPSS V.25.
ResultsMean values of Vit D (ng/ml) were 15.8±10.7 and 15.3±12.5 in male and female patients, respectively. For the control group the mean values were 22.4±7.9 in men and 26.4±13.9 in women. Vit D values in the psychiatric patients of both groups compared to the control group were statistically significantly different (men p=0.021 and women p=0.006). (Table2, 3).
Image:
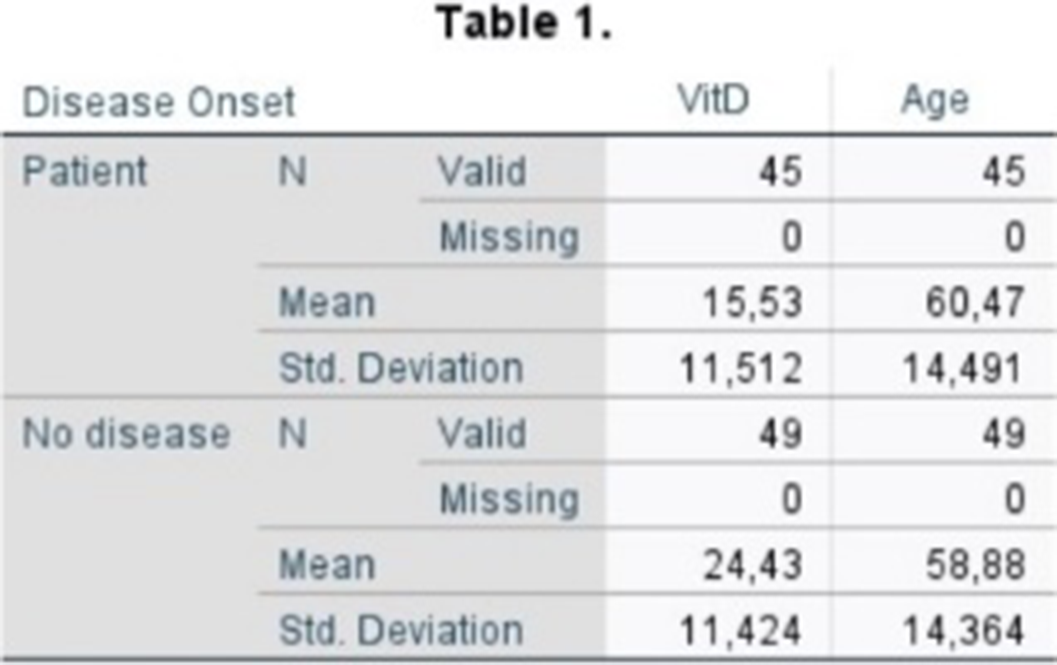
Image 2:

Image 3:
 Conclusions
ConclusionsThe findings of the study are consistent with those of similar studies confirming low concentrations of VitD in the serum of patients with mental illness. This parameter should be taken into account as its measurement is not included in the routine laboratory control to date. Further future studies should correlate VitD deficiency with specific demographic and clinical characteristics.
1. Belvederi Murri M, Respino M, Masotti M, et al. Vitamin D and psychosis: mini meta-analysis. Schizophr Res. 2013;150(1):235-239. doi:10.1016/j.schres.2013.07.017
2. Kalueff A, Minasyan A, Keisala T, Kuuslahti M, Miettinen S, Tuohimaa P. The vitamin D neuroendocrine system as a target for novel neurotropic drugs. CNS Neurol Disord Drug Targets. (2006) 5:363–71. doi: 10.2174/187152706784111506
3. Oudshoorn C, Mattace-Raso FU, van der Velde N, Colin EM, van der Cammen TJ. Higher serum vitamin D3 levels are associated with better cognitive test performance in patients with Alzheimer’s disease. Dement Geriatr Cogn Disord. (2008) 25:539–43. doi: 10.1159/000134382
Disclosure of InterestNone Declared



EFFECT OF EMDR THERAPY ON POST-TRAUMATIC STRESS SYMPTOMS, SYMPTOM SEVERITY AND ANXIETY LEVEL IN PSYCHOTIC PATIENTS WITH AT LEAST ONE TRAUMATIC EVENTS
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1053
-
- Article
-
- You have access
- Open access
- Export citation
Hyperammonemic Encephalopathy: valproic acid-induced adverse reaction
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1053-S1054
-
- Article
-
- You have access
- Open access
- Export citation
PREVALENCE OF SUICIDAL IDEATION IN PATIENTS WITH SCHIZOPHRENIA TREATED AT THE PSYCHIATRIC OUTPATIENT CLINIC OF A TEACHING HOSPITAL
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1054
-
- Article
-
- You have access
- Open access
- Export citation
ADDICTION AND THE EVOLUTION AND COMPLIANCE OF SCHIZOPHRENIC PATIENTS
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1054-S1055
-
- Article
-
- You have access
- Open access
- Export citation
Schizophrenia: the announcement of the diagnosis
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1055
-
- Article
-
- You have access
- Open access
- Export citation
Anxiety and depression in natural caregivers of patients with schizophrenia
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1055-S1056
-
- Article
-
- You have access
- Open access
- Export citation
Management of comorbid schizophrenia with prolactinome (about a case)
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1056
-
- Article
-
- You have access
- Open access
- Export citation
Role of peripheral markers of inflammation in cognitive dysfunction in schizophrenic patients: a systematic review
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1056
-
- Article
-
- You have access
- Open access
- Export citation
Acute psychosis with compulsive behaviour caused by hypothyroidism: a case report
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1057
-
- Article
-
- You have access
- Open access
- Export citation
How sexuality is affected and managed in patients under antipsychotic drugs
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1057
-
- Article
-
- You have access
- Open access
- Export citation
A Case Report of Complex Clozapine Initiation Despite Contraindications
-
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1057-S1058
-
- Article
-
- You have access
- Open access
- Export citation
Post Cerebrovascular Stroke Catatonic Psychosis: A Case Report
-
- Published online by Cambridge University Press:
- 19 July 2023, p. S1058
-
- Article
-
- You have access
- Open access
- Export citation