
24 results
Posttraumatic growth in young adults with parents diagnosed with cancer: Application of the self-regulation model
-
- Journal:
- Palliative & Supportive Care / Volume 23 / 2025
- Published online by Cambridge University Press:
- 08 November 2024, e5
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Resilience Mediates the Relationship Between Parental Attachment and Posttraumatic Growth in Adolescents: A Longitudinal Study
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 26 April 2023, e381
-
- Article
- Export citation
How clinicians can support posttraumatic growth following psychosis: a perspective piece
-
- Journal:
- Irish Journal of Psychological Medicine , First View
- Published online by Cambridge University Press:
- 17 February 2023, pp. 1-6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Chapter 2 - Reproductive Psychology and Fertility Counseling
- from I - Introduction
-
-
- Book:
- Fertility Counseling: Clinical Guide
- Published online:
- 24 November 2022
- Print publication:
- 08 December 2022, pp 31-38
-
- Chapter
- Export citation
Chapter 4 - Fertility Counseling for Couples
- from II - Therapeutic Approaches
-
-
- Book:
- Fertility Counseling: Clinical Guide
- Published online:
- 24 November 2022
- Print publication:
- 08 December 2022, pp 49-58
-
- Chapter
- Export citation
Effectiveness of Posttraumatic Growth Interventions among Cancer Survivors: A Systematic Review and Meta-analysis
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S139-S140
-
- Article
-
- You have access
- Open access
- Export citation
-
 Introduction
IntroductionAlthough cancer is a debilitating experience, it can also increase meaning and satisfaction in one’s life.
ObjectivesTo investigate the effectiveness of interventions that aim to develop posttraumatic growth among cancer survivors.
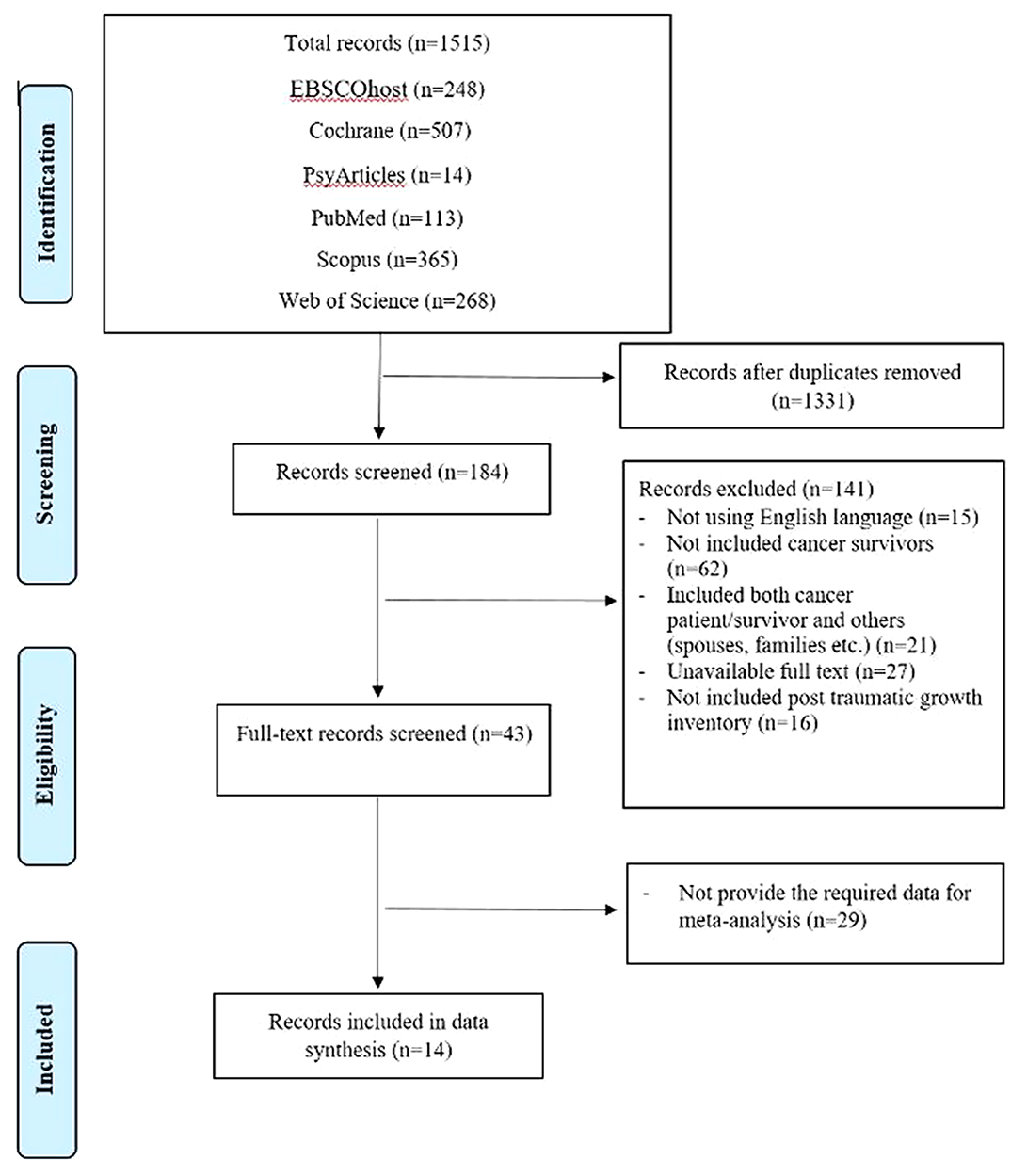
MethodsSeven databasis were searched for relevant articles published between 2000 and 2020. The findings of randomized controlled trials related to interventions to effect posttraumatic growth of cancer survivors were included. Hedges’ g and 95% confidence intervals were computed to estimate the effect.
 Results
ResultsThe effect of the interventions on posttraumatic growth among cancer survivors were heterogeneous. The effect size was statistically significant (Tables 1,2).
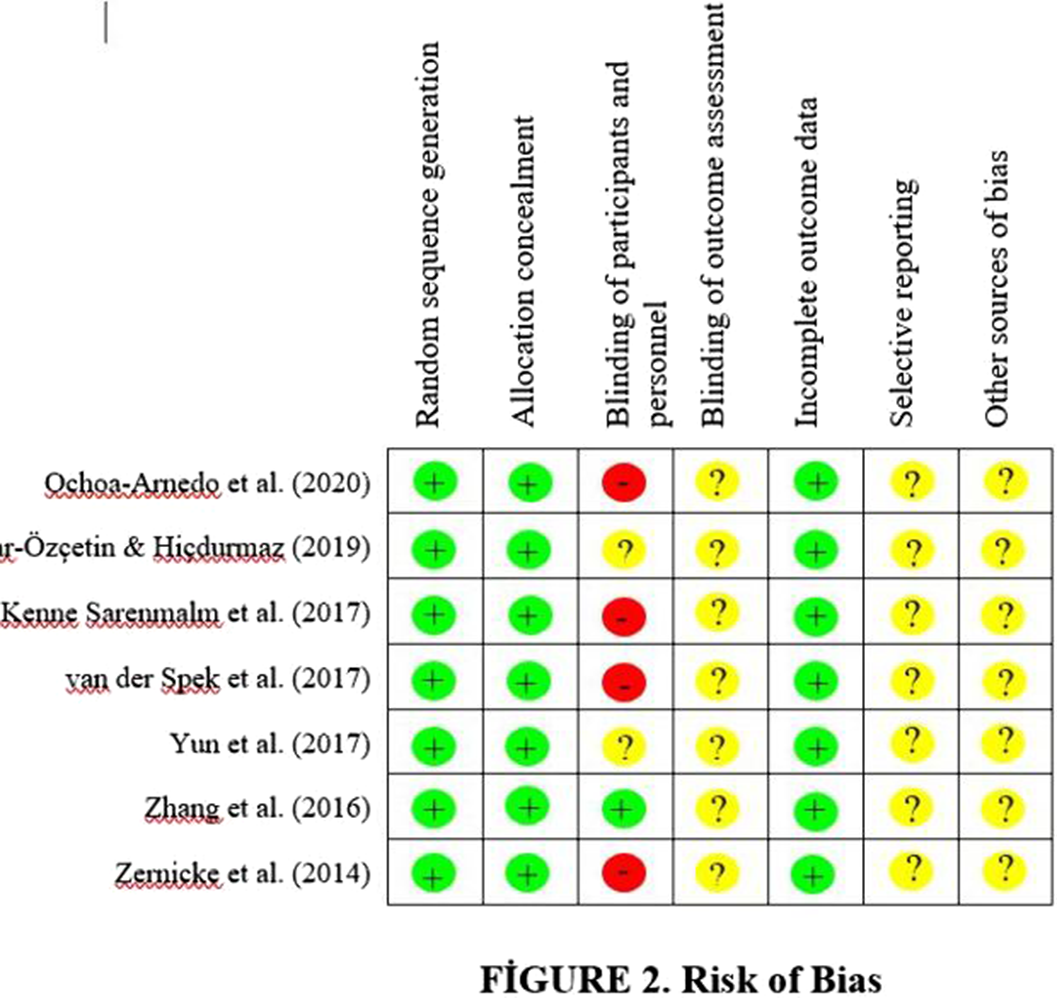
Table 1 k Total n Hedges’g SE 95% CI z p Q Value I2 Eggers t Eggers p Overall studies t 715 1.761 0.484 [0.812, 2.709] 3.637 < 0.001 182.807 96.718 4.66 .871 Table 2 Intervention Effect Design Studies k Total n Hedges’g SE 95% CI RCT Ochoa-Arnedo et al. (2020) 7 140 0.113 0.168 [-0.217, 0.443] Üzar-Özçetin & Hiçdurmaz (2019) 76 13.965 1.155 [11.700, 16.229] Kenne Sarenmalm et al. (2017) 114 0.423 0.189 [0.053, 0.793] van der Spek et al. (2017) 91 -0.161 0.208 [-0.569, 0.247] Yun et al. (2017) 174 0.331 0.162 [0.014, 0.648] Zhang et al. (2016) 58 2.033 0.321 [1.405, 2.662] Zernicke et al. (2014) 62 1.254 0.275 [0.715, 1.793] Z = 3.637 P= < 0.001 SE = 0.484 Sd = 1.777
ConclusionsPosttraumatic growth interventions significantly increased posttraumatic growth among cancer survivors. Health care providers as the main sources of cancer care should be more focused on the achievement of positive outcomes.
DisclosureNo significant relationships.


Latent Profiles of Posttraumatic Growth: 17 years After the Bam Earthquake in Iran
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 17 / 2023
- Published online by Cambridge University Press:
- 25 March 2022, e127
-
- Article
- Export citation
Posttraumatic growth in palliative care patients and its associations with psychological distress and quality of life
-
- Journal:
- Palliative & Supportive Care / Volume 20 / Issue 6 / December 2022
- Published online by Cambridge University Press:
- 14 February 2022, pp. 846-853
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Does bipolar disorder cause posttraumatic growth? Relationship between psychological resistance in patients with bipolar disorder and caregivers
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, p. S193
-
- Article
-
- You have access
- Open access
- Export citation
The interaction effect between gender and profession in posttraumatic growth among hospital personnel
-
- Journal:
- Primary Health Care Research & Development / Volume 21 / 2020
- Published online by Cambridge University Press:
- 24 September 2020, e35
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Making and Receiving Offers of Help on Social Media Following Disaster Predict Posttraumatic Growth but not Posttraumatic Stress
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 15 / Issue 4 / August 2021
- Published online by Cambridge University Press:
- 30 April 2020, pp. 484-490
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Meaning and Purpose (MaP) therapy II: Feasibility and acceptability from a pilot study in advanced cancer
-
- Journal:
- Palliative & Supportive Care / Volume 17 / Issue 1 / February 2019
- Published online by Cambridge University Press:
- 02 January 2019, pp. 21-28
-
- Article
- Export citation
The Mediating Roles of Acceptance and Cognitive Reappraisal in the Relation Between Hope and Posttraumatic Growth Among Adolescents After the Ya'an Earthquake
-
- Journal:
- Journal of Pacific Rim Psychology / Volume 12 / 2018
- Published online by Cambridge University Press:
- 11 June 2018, e25
- Print publication:
- 2018
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Examining cancer survivorship trajectories: Exploring the intersection between qualitative illness narratives and quantitative screening instruments
-
- Journal:
- Palliative & Supportive Care / Volume 16 / Issue 6 / December 2018
- Published online by Cambridge University Press:
- 28 December 2017, pp. 712-718
-
- Article
- Export citation
Post-Traumatic Growth Following Politically Motivated Acts of Violence: 10 Years Post Injury
-
- Journal:
- The Australian Journal of Rehabilitation Counselling / Volume 23 / Issue 1 / July 2017
- Published online by Cambridge University Press:
- 10 May 2017, pp. 1-18
-
- Article
- Export citation
High-level construal benefits, meaning making, and posttraumatic growth in cancer patients
-
- Journal:
- Palliative & Supportive Care / Volume 14 / Issue 5 / October 2016
- Published online by Cambridge University Press:
- 20 October 2015, pp. 510-518
-
- Article
- Export citation
Posttraumatic growth and demoralization after cancer: The effects of patients' meaning-making
-
- Journal:
- Palliative & Supportive Care / Volume 13 / Issue 5 / October 2015
- Published online by Cambridge University Press:
- 05 March 2015, pp. 1449-1458
-
- Article
- Export citation
Posttraumatic Growth and Spirituality After Brain Injury
-
- Journal:
- Brain Impairment / Volume 12 / Issue 2 / 01 September 2011
- Published online by Cambridge University Press:
- 21 February 2012, pp. 82-92
-
- Article
- Export citation
Enhanced Appreciation of Life Following Acquired Brain Injury: Posttraumatic Growth at 6 Months Postdischarge
-
- Journal:
- Brain Impairment / Volume 12 / Issue 2 / 01 September 2011
- Published online by Cambridge University Press:
- 21 February 2012, pp. 93-104
-
- Article
- Export citation
Growth in a ‘New World’: Case Studies of Peer Leader Experiences in the STEPS Program for People With Acquired Brain Injury
-
- Journal:
- Brain Impairment / Volume 12 / Issue 2 / 01 September 2011
- Published online by Cambridge University Press:
- 21 February 2012, pp. 152-164
-
- Article
- Export citation
