


In the European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk), dietary supplements were reported by 44·8 % of women and 31·7 % of men in their 7 d diet diary (7dDD)( Reference Lentjes, Welch and Luben 1 ), of which cod-liver oil was the most commonly consumed supplement( Reference Lentjes, Bhaniani and Mulligan 2 ). Studies in the UK have identified the characteristics of supplement users (SU) and found that SU are more likely to have a normal weight, a higher social class and show more health-conscious behaviours( Reference Harrison, Holt and Pattison 3 – Reference McNaughton, Mishra and Paul 5 ). They have focused on the SU as an individual; however, people sharing a household could influence each other’s behaviour, as has been shown for other types of behaviours such as smoking( Reference Di Castelnuovo, Quacquaruccio and Donati 6 ). Concordance in the choice of using a supplement might partly explain why not all SU consistently show healthy behaviours; their spouse might have influenced them without the SU showing the known characteristics of a SU.
A UK survey among health-conscious women aged 33–72 years( Reference Kirk, Cade and Barrett 4 ) applied the theory of planned behaviour to analyse why women took dietary supplements( Reference Conner, Kirk and Cade 7 ). The study found that participants rated family and health experts with the same intensity of normative beliefs regarding supplement use, defined as ‘perception of whether specific significant others believe you should perform the behaviour or not’( Reference Conner, Kirk and Cade 7 ). A ‘significant other’ could be a spouse. A study investigating complementary alternative medicine use among women with a median of 4 years since breast cancer diagnosis reported 15 % more use of complementary alternative medicine (of which dietary supplement use is considered one) among their spouses v. women who were not using complementary alternative medicine themselves( Reference McLay, Stewart and George 8 ).
There are two reasons why understanding more about spouse concordance is important. First, health interventions encouraging or discouraging supplement use in a specific group could affect the nutritional status or risk of overdosing of people outside the intervention group. Second and conversely, spouse concordance in supplement use could be useful in health interventions to strengthen a message( Reference Di Castelnuovo, Quacquaruccio and Donati 6 ).
In EPIC-Norfolk, we found stronger associations for women than for men between supplement use and BMI and season, as well as conflicting results between men and women for sociodemographic variables such as age, education and marital status (MAH Lentjes, AA Welch, AA Mulligan et al., unpublished results). Therefore, we set out to find what level of concordance exists in SU in a large population of men and women. In the present communication we hypothesise that spouses influence each other’s choices in using dietary supplements. We studied the existence of concordance and discordance in supplement use and how this relates to other known sociodemographic variables in order to understand the relative importance between spouse concordance, other participants’ characteristics and supplement use.
Methods
Study design
EPIC-Norfolk is a prospective cohort study based in East Anglia (UK) that started recruitment in 1993 (up to 1998) to investigate risk factors for chronic diseases such as cancer and CVD( Reference Day, Oakes and Luben 9 ). Men and women aged 39–79 years, recruited from thirty-five general practitioners’ clinics, completed an informed consent and a health and lifestyle questionnaire. This questionnaire provided information on: (i) marital status (‘single’, ‘married or living as married’, ‘widowed’, ‘separated’, ‘divorced’); (ii) current or past occupation, from which social class was derived according to the Registrar General’s occupation-based classification scheme; (iii) highest education level obtained (categorised into ‘no qualifications’, ‘A-level’, ‘O-level’ or ‘degree/equivalent’); (iv) smoking status (‘current’, ‘former’ or ‘never’; derived from two questions: ‘Have you ever smoked as much as one cigarette a day for as long as a year?’ and ‘Do you smoke cigarettes now?’); and (v) self-reported physical activity, from which a validated 4-point score of work-related and leisure-time activity was compiled( Reference Wareham, Jakes and Rennie 10 ). A health examination was attended by 25 639 participants at their general practitioner’s clinic. A trained nurse measured height (in centimetres) and weight (in kilograms), with participants wearing light clothing and no shoes.
Supplement use
Dietary supplements were defined according to the EU directive 2002/46/EC: ‘foodstuffs the purpose of which is to supplement the normal diet and which are concentrated sources of nutrients or other substances with a nutritional or physiological effect, alone or in combination, marketed in dose form…’. During the health examination, participants were given a 7dDD that measured dietary supplement use by asking, ‘Please name any vitamins, minerals or other food supplements taken on each day of last week’( Reference Lentjes, Bhaniani and Mulligan 2 ). Participants recording one or more supplements taken on at least one diary day were considered supplement users (SU). Participants who mentioned medication, e.g. ferrous sulfate or prescribed calcium, without further use of dietary supplements, were defined as non-supplement users (NSU). Since cod-liver oil (CLO) is the most commonly consumed supplement in the UK and nearly 25 % in EPIC-Norfolk consumes CLO( Reference Lentjes, Bhaniani and Mulligan 2 ), participants who consumed CLO or fish-oil supplements, with or without other types of supplements, were grouped as a separate category of SU (SU+CLO) to partly account for heterogeneity among SU( Reference Denison, Jameson and Syddall 11 , Reference Radimer, Bindewald and Hughes 12 ).
Household identification
Participants sharing the same address were identified by their surname and postal address at the time of recruitment; the same addresses were given the same household ID, leaving 15 956 participants eligible (7978 households). Participants who (i) both attended a health examination (86·7 % of 15 956), (ii) were living in a household where both EPIC participants were married (or living as married; 98·3 %) and (iii) went on to complete their 7dDD including the supplement question (92·3 %) were included for the current analysis (n 11 060). The age range of this sample was 39–79 years; mean age among men was 61·1 (sd 8·4) years and among women, 58·5 (sd 8·3) years.
Statistical analysis
Analyses were sex-stratified for observations to be uncorrelated, unless households rather than participants were the denominator. We use the term ‘spouse concordance’ to refer to agreement in supplement use, although not all couples were married. The percentages of participants who were concordant in supplement use, i.e. where both members took supplements or both did not take supplements, are given for each stratum of the sociodemographic variables for which we wanted to test the associations with supplement use. For equal presentation purposes, continuous variables, such as age, BMI (kg/m2) and month of 7dDD completion, were grouped. Differences in sociodemographic variables between SU+CLO, SU−CLO and NSU, as well as spouse concordance, were tested using the χ 2 test. Supplement use, as a categorical variable with three categories (NSU, SU+CLO, SU−CLO), was then used as the dependent variable in multinomial logistic regression with ‘supplement use by spouse’ as a predictor, including all the sociodemographic variables from Table 1. Participants for whom one or more variables were missing were removed from the regression analysis (2 %). Statistical analysis was performed using the statistical software package IBM SPSS Statistics version 21. P values below 0·05 were considered statistically significant.
Table 1 Characteristics of supplement users and spouse concordance among married (or living as married) participants sharing a household, European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) cohort study (n 11 060)
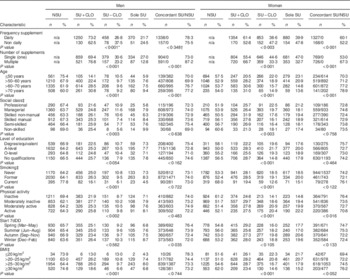
NSU, non-supplement user; SU, supplement user; SU+CLO, cod-liver oil supplement user; SU−CLO, supplement user who does not consume-cod liver oil; sole SU, participant is the only SU in the household; concordant SU/NSU, concordance in supplement use (i.e. both spouses NSU or both spouses SU); 7dDD, 7 d diet diary; n/a, not applicable.
* From χ 2 testing of the hypothesis that there is no difference between SU+CLO, SU−CLO and NSU regarding the sociodemographic variables.
† From χ 2 testing of the hypothesis that there is no difference between concordant and discordant spouses regarding the sociodemographic variables.
‡ Because of missing values, the numbers do not add up to 11 060.
Results
Of the 11 060 participants, 4445 (40·2 %) were SU; 34·6 % among men and 45·7 % among women. In the 5530 households, nearly 75 % were concordant in their supplement use, with 46·7 % not using supplements (i.e. both NSU) and 27·0 % using supplements (i.e. both SU).
Concordance in supplement use was significantly higher among daily SU v. non-daily SU (women only) and for those consuming multiple supplements v. single SU (Table 1). Concordance in supplement use increased significantly with age in both sexes. A higher BMI among women was associated with increased concordance in supplement use, but less concordance among men. The column marked ‘sole SU’ shows the percentage of men/women who used a supplement when their spouse did not. For all participants’ characteristics, in all strata, this percentage was higher among women. For age and social class the trends for men and women were opposite. For example, where among women sole supplement use increased with increasing social class, for men this percentage decreased. And where for men physical activity had no association with sole supplement use, for women more physical activity was associated with more sole supplement use.
The odds of the participant being a SU were higher among women than men, irrespective whether the spouse was a SU or NSU (Fig. 1). The odds of using a supplement were higher among participants whose spouses were SU. The OR was 8·86 (95 % CI 7·78, 10·09), indicating that participants with a spouse who used supplements were nearly nine times more likely to be SU than participants whose spouse was a NSU.
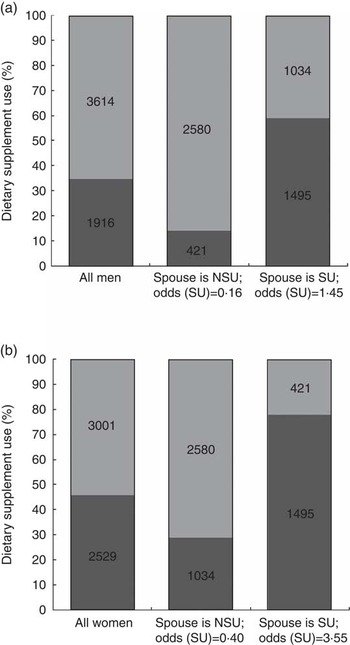
Fig. 1 Dietary supplement use (![]() , participant NSU;
, participant NSU; ![]() , participant SU) of (a) men (n 5530) and (b) women (n 5530) by spouse’s supplement use (NSU, non-supplement user; SU, supplement user) among married (or living as married) participants sharing a household, European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) cohort study (n 11 060)
, participant SU) of (a) men (n 5530) and (b) women (n 5530) by spouse’s supplement use (NSU, non-supplement user; SU, supplement user) among married (or living as married) participants sharing a household, European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) cohort study (n 11 060)
All sociodemographic variables from Table 1 were entered one by one into a multinomial logistic regression model (SU+CLO v. NSU; SU−CLO v. NSU); sex-stratified results are presented in Table 2. The OR for ‘supplement use by spouse’ attenuated only slightly after inclusion of all other sociodemographic variables. Having a spouse who used supplements was the strongest predictor for both SU+CLO and SU−CLO groups in both sexes, followed at some distance by current smoking. Binary logistic regression, where only SU+CLO and SU−CLO were included, confirmed these differences between the two SU groups and also found ‘supplement use by spouse’ to be significantly different.
Table 2 Adjusted odds ratios of using supplements containing cod-liver oil or supplements not containing cod-liver oil compared with not using a supplement at all among married (or living as married) participants sharing a household, European Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) cohort study (n 10 855Footnote *)
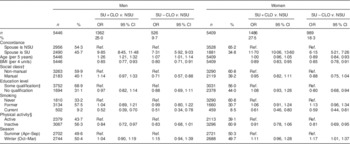
SU+CLO, cod-liver oil supplement user; NSU, non-supplement user; SU−CLO, supplement user who does not consume cod-liver oil, Ref., referent category.
* Participants with complete variable data (list-wise) were included in the analysis (98 %).
† Some qualification takes the summed categories of A-level, O-level and degree/equivalent.
‡ Manual takes the summed categories of: skilled manual, semi-skilled and non-skilled. Non-manual takes the summed categories of: professional, managerial and skilled non-manual.
§ Active takes the summed categories of active and moderately active. Inactive contains the categories inactive and moderately inactive.
The model without ‘supplement use by spouse’ (data not shown) showed small differences for age among women (SU+CLO: OR =1·08; 95 % CI 1·04, 1·13; SU−CLO: OR =0·94; 95 % CI 0·90, 0·98), a stronger association with social class in men (SU−CLO: OR =0·66; 95 % CI 0·53, 0·81) and a stronger association for education in women (SU−CLO: OR =0·76; 95 % CI 0·65, 0·89) compared with Table 2. This indicates that ‘supplement use by spouse’ was not a strong confounder for these variables that are known to be associated with supplement use.
Discussion
Spouse concordance in supplement use was 73·7 %, with increased age being strongly associated with increased concordance. The strongest predictor for dietary supplement use was supplement use of a spouse. This factor was stronger for participants consuming CLO supplements v. non-CLO supplements.
The associations between dietary supplement use and sociodemographic characteristics found in studies in the UK( Reference Harrison, Holt and Pattison 3 , Reference Kirk, Cade and Barrett 4 ) and other countries( Reference Radimer, Bindewald and Hughes 12 – Reference Touvier, Kesse and Volatier 14 ) were also found in this sub-cohort of spouses in the EPIC-Norfolk study. EPIC-Norfolk was able to include ‘supplement use by spouse’ and found it to have the strongest association with dietary supplement use compared with known characteristics of SU, while minimally changing the association between the other sociodemographic variables and supplement use.
The positive association found for increased age and spouse concordance has been described by others as concordance due to cohabitation( Reference Di Castelnuovo, Quacquaruccio and Donati 6 ). In our study, being older independently increased supplement use among men (more strongly for CLO than for non-CLO supplements) and decreased the odds for non-CLO use in women. Assuming that age is correlated with the number of years of marriage, and hence length of cohabitation, we assumed that the correlation between age and supplement use would increase after ‘supplement use by spouse’ was excluded from the model; however, the OR for age were minimally affected. Positive assortative mating, defined as ‘the tendency of individuals to choose a spouse with similar characteristics’( Reference Di Castelnuovo, Quacquaruccio and Donati 6 ), could explain the slight attenuation seen for social class and education level with inclusion of ‘supplement use by spouse’. Although even in the fully adjusted model ‘supplement use by spouse’ remained the strongest predictor, we cannot rule out residual confounding.
Strengths of the current analysis included the detailed recording of supplement use( Reference Lentjes, Bhaniani and Mulligan 2 ), as well as detailed assessment of sociodemographic characteristics( Reference Day, Oakes and Luben 9 ). We were able to identify over 5500 households in this free-living UK cohort which, apart from a lower smoking prevalence, represents the UK population aged 40–79 years reasonably well( Reference Day, Oakes and Luben 9 ). The analysis described here was, by design, restricted to a sub-cohort – which can be considered a selective group of participants, considering that both participants were willing to participate in a long-term prospective study. Compared with the whole cohort, the mean age among men in this subset increased by 2 years (see online supplementary material, Supplemental Table 1) and might explain the 3 % increase in supplement use. The proportion of SU among women was only 1 % higher compared with the whole cohort. Smoking was approximately 3 % less prevalent in both men and women, and might be indicative of more similar health-related behaviours among these spouses overall and hence could have overestimated the spouse concordance for supplement use found in the present study. Weaknesses of the analysis include that only ‘supplement use by spouse’ in EPIC-Norfolk could be assessed; however, other relations/resources (such as magazines, health professionals and friends) exist that can influence beliefs relating to supplement use( Reference Conner, Kirk and Cade 7 ). Alternatively, other motives for using supplements, such as prevalent illness or health concerns, were not taken into account in the analysis, but are known to influence specific types of supplements( Reference Satia-Abouta, Kristal and Patterson 15 , Reference Bailey, Gahche and Miller 16 ).
The sequence of who in the household started with the use of supplements remains unknown. Future studies would benefit from not only requesting supplement information from the participant, but also establishing whether any of the other household members use supplements; as well as asking who first commenced use, since this additional information will help to identify different motivations and characteristics of SU and could aid the development of health interventions and risk assessment.
Conclusion
‘Supplement use by spouse’ was the strongest predictor of participants’ supplement use and hence can be of importance when developing public health messages to encourage or discourage supplement use, since the nutritional status of people beyond the SU could be affected.
Acknowledgements
Acknowledgements: The authors would like to thank the EPIC-Norfolk participants and staff. Financial support: This work was supported by Cancer Research UK (SP2024-0201 and SP2024-0204) and the Medical Research Council (G9502233). Cancer Research UK and the Medical Research Council had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: M.A.H.L. wrote the manuscript and analysed the data, developed the concepts of the Vitamin and Mineral Supplement (ViMiS) nutrient calculation and contributed to the development of the ViMiS database. A.A.W. instigated the work on the dietary supplement data and oversaw its later developments. R.H.K. advised on the statistical analysis and helped with the interpretation of the data. R.N.L. is responsible for overall data management and created the household concordance variable. K.-T.K. is principal investigator of the EPIC-Norfolk study. All authors critically read and reviewed the manuscript. Ethics of human subject participation: The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Norwich District Health Authority Ethics Committee. Written informed consent was obtained from all subjects/patients.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1368980014001396





