


Vitamin D is a vitamin-hormone which is not only crucial for Ca homeostasis but also to general health(Reference Holick1). Vitamin D is obtained from sun exposure, food and supplementation. While it is well known that severe vitamin D deficiency leads to osteomalacia and rickets, and that mild to moderate deficiency can result in osteoporosis and an increased risk of fractures(Reference Thomas and Demay2), more recent research has been linking vitamin D deficiency to autoimmune disorders, CVD and cancers(Reference Holick3, Reference Stokstad4).
Dietary sources of vitamin D are limited to few foods, such as fish oils, fatty fish, eggs, organ meat and UV-irradiated mushrooms. In Saudi Arabia, fortified foods are limited to very few dairy products and cereals(Reference Madani, Al-Amoudi and Kumosani5). Therefore, the major source of vitamin D is via exposure of uncovered skin to solar UV-B radiation(Reference Holick6). UV rays are strongest in areas close to the Equator because: (i) the sun is directly over the Equator and thus the UV rays travel a shorter distance through the atmosphere to reach the surface of the Earth; and (ii) the ozone layer, which absorbs UV radiation, is naturally thinner in these areas(Reference Frederick7). It has been shown that seasons other than summer (i.e. winter, autumn and spring) can contribute to vitamin D deficiency(Reference Mavroeidi, O'Neill and Lee8–Reference Manios, Moschonis and Lyritis10), even with a daily supplement regimen of vitamin D3 (7·5 μg) taken for 12 months(Reference Manios, Moschonis and Lyritis10).
Although one would presume that living at lower latitudes would guarantee protection against vitamin D deficiency, a previous study on the adult population residing in south Florida has shown otherwise(Reference Levis, Gomez and Jimenez11). Furthermore, vitamin D deficiency is common in India, Australia, Brazil and the Middle East, because of cultural habits and sun avoidance(Reference Agarwal and Arya12–Reference Gannage-Yared, Chemali and Sfeir17).
Our goal was to establish the prevalence of vitamin D deficiency and to assess seasonal variations in vitamin D levels in adult Saudi female out-patients in Riyadh, Saudi Arabia (24°42′N), an area of year-round sunny weather. The study was conducted in both postmenopausal and premenopausal women in order to investigate the effect of menopausal status on vitamin D levels.
Experimental methods
Data were collected retrospectively using medical record abstraction for the present cross-sectional study of adult female out-patients (≥19 years). Values of serum levels of vitamin D were extracted for 1556 women attending out-patient care at King Abdulaziz Medical City (KAMC), which is part of the National Guard Health Affairs in Riyadh, between January 2009 and December 2009. The patients were attending various clinics at the hospital which included rheumatology, neurology, orthopaedic, internal medicine and endocrinology clinics, among many others. In addition, the KAMC has a number of clinics which offer primary care to the community. Women attending clinics for issues related to their bone health were excluded from the study. Information related to the date of birth and the clinics the patients were attending were extracted from the record. Women were subdivided into two groups: patients treated during the summer (June, July and August, n 659) and patients treated during the winter (January, February and March, n 897). The summer group (group A) was further subdivided into premenopausal (group A1, age 19–49 years; n 425) and postmenopausal subgroups (group A2, age ≥50 years, n 234). The winter group (group B) was also subdivided into premenopausal (group B1, n 543) and postmenopausal (group B2, n 354) subgroups. The age of 50 years was used as a cut-off point for determining menopausal status(Reference Frommer18).
Serum levels of total 25-hydroxyvitamin D (25(OH)D; sum of D2 and D3) were measured in the central laboratory of KAMC using HPLC. The analysis was performed on HPLC columns (CV = 3 %) from Chromsystems (Munich, Germany). Results were expressed in nmol/l. Vitamin D deficiency was described for levels of 25(OH)D falling below <50 nmol/l(Reference Holick, Binkley and Bischoff-Ferrari19), whereas insufficiency was at 50–75 nmol/l, and optimum level was at 76–200 nmol/l.
Statistical analysis
Data were analysed using the SPSS for Windows statistical software package version 15·0 and Microsoft Excel™ 2007. Age was expressed as mean and standard deviation, 25(OH)D levels were expressed as means with their standard errors, and prevalence of vitamin D deficiency was calculated as percentage. Comparison of prevalence of vitamin D deficiency among groups was done using the χ 2 test, whereas comparison of vitamin D levels was performed using the unpaired t test. A P value of < 0·05 was considered significant.
Results
The patients’ mean age was 44·4 (sd 16·1) years for the summer group and 46·1 (sd 15·9) years for the winter group. We found that our studied population had a high prevalence of vitamin D deficiency in both seasons (Table 1). Indeed, during the summer, the prevalence of vitamin D deficiency (25(OH)D <50 nmol/l) in premenopausal and postmenopausal patients was 80 % and 68 %, respectively. This high prevalence of vitamin D deficiency was even more pronounced in the winter season (85 % and 76 % for premenopausal and postmenopausal, respectively). This seasonal variation was statistically significant only in the postmenopausal group, where the prevalence of vitamin D deficiency was significantly higher in the winter compared with the summer (P = 0·035).
Table 1 Comparison of vitamin D status among premenopausal and postmenopausal women in summer and winter groups: Saudi female out-patients, January–December 2009

The premenopausal group had a higher level of 25(OH)D in the summer (33·3 (se 1·65) nmol/l) than in the winter (28·5 (se 1·16) nmol/l; P < 0·05). Similarly, the postmenopausal group had a higher level of 25(OH)D in summer (44·4 (se 2·3) nmol/l) compared with the winter (36·3 (se 1·51) nmol/l; Table 2 and Fig. 1). Moreover, in the summer season, the postmenopausal group (44·4 (se 2·3) nmol/l) had a significantly higher level of 25(OH)D compared with the premenopausal group (33·3 (se 1·65) nmol/l; P < 0·05). A similar trend was also observed in the winter, where the postmenopausal group (36·3 (sem 1·51) nmol/l) had a significantly higher level of 25(OH)D compared with the premenopausal group (28·5 (se 1·16) nmol/l; P < 0·05; Table 2 and Fig. 2).
Table 2 Comparison of total 25-hydroxyvitamin D (25(OH)D) concentrations among premenopausal and postmenopausal women in summer and winter groups: Saudi female out-patients, January–December 2009

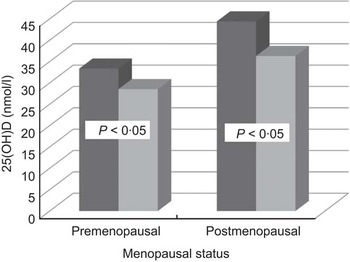
Fig. 1 Comparison of total 25-hydroxyvitamin D (25(OH)D) levels between premenopausal (age 19–49 years) and postmenopausal (age ≥50 years) groups according to season ( $$$$, summer, premenopausal n 425, postmenopausal n 234;
$$$$, summer, premenopausal n 425, postmenopausal n 234;  $$$$, winter, premenopausal n 543, postmenopausal n 354): Saudi female out-patients, January–December 2009
$$$$, winter, premenopausal n 543, postmenopausal n 354): Saudi female out-patients, January–December 2009
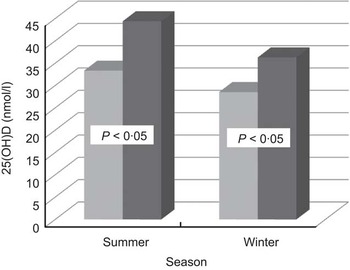
Fig. 2 Comparison of total 25-hydroxyvitamin D (25(OH)D) between summer and winter groups according to menopausal status ( $$$$, premenopausal, age 19–49 years, n 425 in summer, n 543 in winter;
$$$$, premenopausal, age 19–49 years, n 425 in summer, n 543 in winter;  $$$$, postmenopausal, age ≥50 years, n 234 in summer, n 354 in winter): Saudi female out-patients, January–December 2009
$$$$, postmenopausal, age ≥50 years, n 234 in summer, n 354 in winter): Saudi female out-patients, January–December 2009
In summary, we found a high prevalence of vitamin D deficiency year-round among Saudi female out-patients. However, 25(OH)D levels were relatively higher in summer for both premenopausal and postmenopausal patients. It is noteworthy that postmenopausal patients had slightly higher levels of 25(OH)D compared with their premenopausal counterparts.
Discussion
The high prevalence of vitamin D deficiency in the Kingdom of Saudi Arabia has been well established in several subpopulations(Reference Elsammak, Al-Wosaibi and Al-Howeish20–Reference Abokrysha28). Moreover, this micronutrient deficiency has been well documented across the entire Middle East and the developing world(Reference Hamilton, Grantham and Racinais16, Reference Racinais, Hamilton and Li29–Reference Mithal, Wahl and Bonjour33). However, no such cohort of female out-patients was investigated previously.
The highlight of the present study is the discovery that there is a year-round high prevalence of vitamin D deficiency among Saudi female out-patients regardless of their menopausal status. The study subjects represent a population who has free access to optimal health care and all complementary benefits including routine supplementation of Ca and vitamin D for postmenopausal women.
While regular exposure to sunlight is considered an effective prophylaxis against vitamin D deficiency(Reference Reid, Gallagher and Bosworth34), studies in regions located at low latitude with abundant sunlight have also shown a high prevalence of vitamin D deficiency(Reference Agarwal and Arya12–Reference Gannage-Yared, Chemali and Sfeir17). These findings have been explained as being mostly due to the region's customary clothing and sun avoidance(Reference Mithal, Wahl and Bonjour33). In addition, scientists have suggested that in the Saudi population, vitamin D deficiency among women may be due to lack of public awareness(Reference Siddiqui and Kamfar23). However, hot desert climate, social and religious habits all act against sun exposure. Moreover, the widespread occurrence of obesity and darker skin in the region increase the length of time required to achieve optimum vitamin D level from sun exposure.
An interesting finding in our study was that postmenopausal patients had relatively higher vitamin D levels, which is in contradiction with the previous finding in another study on healthy Saudi women(Reference Ardawi, Qari and Rouzi26). Having our study groups as out-patients may give an explanation for this phenomenon, where many clinicians tend to prescribe 1 g Ca and 10–20 μg vitamin D for postmenopausal women as a protection against osteoporosis, without assessing their vitamin D status.
The high prevalence of vitamin D deficiency in Saudis has been reported in the literature since the 1980s(Reference Sedrani, Elidrissy and El Arabi24, Reference Fonseca, Tongia and El-Hazmi35). This deficiency remains unresolved and might have been accentuated in recent times by increased sun avoidance caused by many factors including more urbanized lifestyles and aesthetic reasons, where the culture tends to favour fair skin which is not suntanned. Therefore, even in the privacy of their own homes, women from this culture tend to avoid sun exposure.
The authors acknowledge some limitations to the study. For example, our studied population consisted of patients with mild to severe illnesses of various lengths. Therefore, the pathological conditions or treatment regimen could have contributed to the lower serum 25(OH)D levels. Nevertheless, severe hepatic or renal failure was very rare in our patients. Another limitation is the absence of comprehensive data on the levels of parathyroid hormone. However, parathyroid hormone values were obtained for some but not all patients (data not shown). Preliminary observations indicate that not all patients with vitamin D deficiency had elevated parathyroid hormone, a finding which requires further investigation.
The strengths of the study include, but are not limited to, a sample size that is large enough to infer generalizations across the entire population with the same criteria. Another major strength in our study is the use of the gold standard method of HPLC for the quantification of 25(OH)D.
Conclusions
The prevalence of vitamin D deficiency among Saudi women is alarmingly high. In a region with abundant sunshine throughout the year, this deficiency is independent of seasonal influence. Clinicians should have an active role in screening and treating this widespread deficiency which has serious impacts on health that go far beyond bone health. Clinicians seeing these patients must make an increased effort to prevent vitamin D deficiency by checking vitamin D levels and educating these patients about the benefits of sun exposure. Clinicians should also attempt to correct these deficiencies by prescribing vitamin D supplements at the appropriate dosage.
Acknowledgements
This research did not receive any grant from any funding agency in the public, commercial or not-for-profit sectors. The authors declare having no conflict of interest. All authors have participated sufficiently in the intellectual content, conception and design of this work or the analysis and interpretation of the data, as well as the writing of the manuscript, and have approved the final version of the submitted manuscript.




