Enabling communities and consumers to choose a healthy diet is dependent on the food system, which influences population health. Micronutrient malnutrition is a global health issue and represents a major challenge to social and economic development in developing countries( Reference Black, Allen and Bhutta 1 ). National surveys such as the National Family Health Survey-4 in India estimate the death rate among children under 5 years of age at 50 per 1000( 2 ). The main reason is insufficient food intake leading to deficiencies of both macronutrients and micronutrients. Medium- and short-term strategies to combat micronutrient deficiencies, such as fortification and supplementation respectively, have been adopted worldwide. Although these strategies have been successful in reducing specific clinical forms of micronutrient deficiencies in the population, subclinical forms of vitamin A deficiency are still prevalent( Reference Laxmaiah, Nair and Arlappa 3 ). However, there is a need for a more comprehensive, long-term sustainable approach for addressing multiple micronutrient deficiencies. Diet diversification, which provides a package of micronutrients along with nutrition education, is considered a sustainable strategy( Reference Nair, Augustine and Konapur 4 ).
The diets of school-going children in lower- and middle-income countries are deficient in micronutrients, the major factor being lack of diet diversity, more so in rural areas. In India, the rural diet survey revealed that the consumption of all five food groups is less than 50 % of recommended intake, except for cereals, across all age groups( 5 ). Evidence-based interventions are the need of the hour, to fundamentally bring about a sustainable social and behavioural change regarding micronutrient malnutrition. In order to set quantifiable goals and priorities for reducing micronutrient malnutrition through diet diversification, data must be collected not only on dietary intake but also on local availability, accessibility and affordability of foods, to enable purchase and consumption of a diversified diet by all people as well as the target population. This information is crucial in developing and assisting public health interventions targeting behaviour change through dietary diversification to combat micronutrient malnutrition globally.
The success of public health interventions in resource-limited settings depends critically on our understanding of the socio-anthropological and economic aspects of the context in which these interventions are implemented( 6 – Reference Wilkinson, Parker and Martineau 8 ). For promoting dietary diversification and to push people towards consumption of micronutrient-rich foods, one has to understand the current knowledge, attitudes and practices (KAP) prevalent in the community. Understanding the inadequacies in KAP prevalent in the community aids in developing targeted nutrition communication interventions specific to the target population. The targeted nutrition communication intervention, when implemented in the community, will bring the needed change in the practice of the target population. KAP of the people, in turn, depends on other factors such as level of education, cultural beliefs and practices, income, availability, proximity to markets and affordability.
There is realization that the poor association between nutrition knowledge and dietary intake may be due to the poor assessment of knowledge as one of the major hindering factors( Reference Augustine, Vazir, Rao and Rao 9 ). The development of validated and customized KAP tools is a demanding and continuous process which is neglected/out of the focus of most interventions. Thus, the need for valid and reliable tools in nutrition education research for assessment of knowledge is now well recognized. Therefore, the present study attempted to develop a KAP questionnaire specific to micronutrients and factors affecting micronutrient status in rural areas of Telangana state, India, using qualitative data. The purpose of developing the KAP questionnaire was to use it as an intervention assessment tool in an ongoing communication intervention project on promoting diet diversification to improve micronutrient status in rural households.
Methodology
Approvals
The study employed a mixed-methods, sequential exploratory approach for development and validation of the KAP questionnaire. Permission was obtained from the District Collector and Department of Women and Child Welfare, Government of Telangana, India. Supervisors of the Integrated Child Development Scheme (which is an Indian public health-care system providing basic health care including nutrition education and supplementation for pregnant and lactating women and children under 5 years of age) and village heads (Ghatkesar sub-district) were approached and seven villages with >500 households were included for the study. The purpose, methodology and their crucial role in the study were explained and discussed with them. The study was registered at the Clinical Trial Registry of India (CTRI registration number CTRI/2015/06/005836). As per the norms of the Institutional Ethics Committee of the National Institute of Nutrition, Hyderabad (which cleared the protocol; 08/I/2014), written informed consent was obtained from the participants.
Study site
The present study was conducted in Ghatkesar sub-district, Medchal district, Telangana state, India. Ghatkesar has 44 004 households with a population size of 188 380, 71 % literacy and a sex ratio of 926 women:1000 men. Out of fifteen villages in Ghatkesar, seven villages with >500 households (Aushapur, Annojiguda, Kondapur, Edulabad, Yamnampet, Ankushapur and Korremula) were randomly selected for conducting the study. The study area met the inclusion criteria of: (i) availability and accessibility to the food market as it is near the national highway; (ii) majority of the families residing there were expected to be middle-income families; and (iii) 10–15 % of the population was expected to have a child aged 6–10 years in the household.
Study design
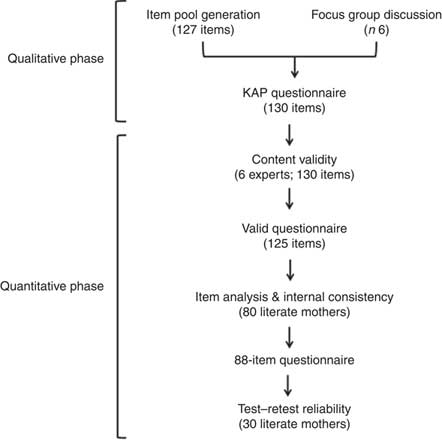
There were two distinct phases, qualitative and quantitative, in the development of the KAP questionnaire. In the qualitative phase, literature was reviewed to prepare an item pool and focus group discussions (FGD) were conducted to get an overview of existing knowledge and practices. In quantitative phase, the item pool was tested for its validity, internal consistency and reliability (Fig. 1).
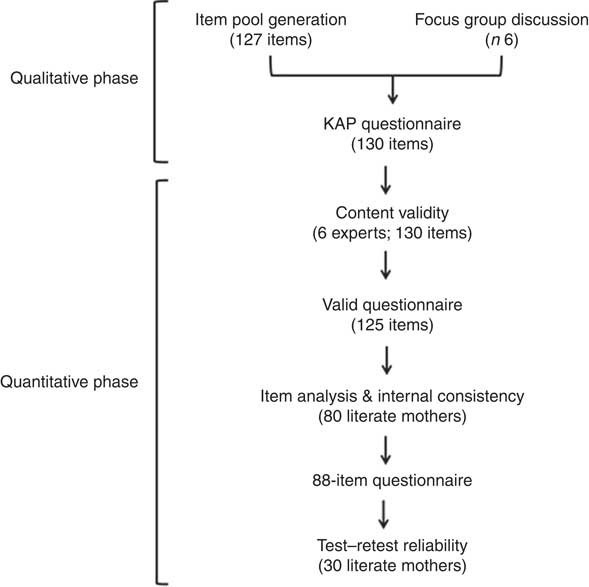
Fig. 1 Study design: sequential exploratory mixed-methods approach (KAP, knowledge, attitude and practice)
Qualitative data collection phase
Focus group discussions
Participants
FGD were conducted among participants from the randomly selected villages of Aushapur, Annojiguda, Kondapur and Edulabad. The inclusion criteria for the participants included a household with a 6–10-year-old child, a literate mother and a middle-income family (Standard of Living Index >24) with family size of three to five members. Although the number of FGD to be conducted was not predetermined, it was decided to conduct no new FGD at the point of data and theoretical saturation, which are defined as criteria where conducting further FGD with a new group of participants would not yield new information and new themes, respectively( Reference Krueger 10 ). According to the standard format, the number of participants in each FGD should be six to twelve for utmost participation in the discussion( Reference Krueger 11 , Reference Krueger 12 ). In the present study, data and theoretical saturation were reached at six FGD. In all groups, there were six to eight participants, except in one FGD where there were twelve. The total number of participants in this qualitative phase of research was forty-four.
Conducting focus group discussions
The standard method of conducting FGD was followed( Reference Krueger 11 , Reference Krueger 12 ). Briefly, a theme guide was conceived with five major themes: (i) micronutrients (including food sources, bioavailability and deficiency symptoms); (ii) diet diversification (including availability, accessibility and affordability); (iii) cooking and eating practices (frequency of foods purchased and prepared); (iv) national programmes (vitamin A drops, iron tablets, iodized salt, services for beneficiaries at anganwadi centres); and (v) sunlight exposure (time and duration of physical activity). Each theme had open-ended questions and probes for discussion (Table 1).
Table 1 Discussion points included in the theme guide for conducting focus group discussions with rural, literate, middle-income mothers of school-age children (6–10 years), Ghatkesar sub-district, Medchal district, Telangana state, India (n 44)

FGD were conducted by a team consisting of a trained moderator and two note-takers( Reference Krueger and Casey 13 ). The meeting was arranged at the local anganwadi centre and community halls. The entire discussions were carried out in the local language (Telugu). The FGD lasted for 35–45 min. Mothers sat in a semi-circle with the moderator at the centre. After explaining the purpose of the study, written consent to participate in the discussion was obtained. With the permission of the participants, all the discussions were video/audio-recorded except one FGD, where the participants did not agree to video-record the discussion.
The participants were engaged with ice-breaking questions, such as ‘What foods do your children like the most?’ and ‘Are green leafy vegetables grown in your village?’, prior to beginning the session, to make them comfortable with the discussion and also to identify active participants. The discussion started with the themes included in the questionnaire and probes were applied wherever needed. No specific order of the questions in the themes was followed; whatever order was convenient at the time of conducting the FGD was used. Non-participant observers took notes and recorded videos simultaneously. The discussion ended with clearing participants’ queries on nutrition and a vote of thanks.
Analysis
Coding
A summary of the FGD was written down immediately after every discussion by the focus group team. Transcripts were prepared using field notes/video recordings on the same day. These scripts were in turn compiled into individual reports, organizing raw data into codes. A grounded theory approach was used to manually code the data with open and axial coding. At first, we looked for distinct concepts and categories in the data (open coding), which formed the basic themes of analysis. Using the codes developed at the first level, the researchers re-read the transcripts and categorized statements that fit to themes of analysis (axial coding). Quotes from the transcripts that addressed these themes were flagged, and the ones that were in complete contrast with others were included. Majority responses of the mothers to the questions and probes during the FGD were considered for deleting, retaining, modifying and adding in the item pool.
Item pool generation
The item pool consisting of 132 KAP questions was formulated based on a review of the literature( Reference Augustine, Vazir, Rao and Rao 9 , Reference Parmenter and Wardle 14 – Reference Marías and Glasauer 18 ) and discussion with nutrition experts, with four major domains. The domains under which questions were categorized were: (i) diet diversity; (ii) micronutrients; (iii) cooking and eating practices; and (iv) sunlight exposure. The micronutrients focused upon were iron, zinc, calcium, vitamin A, vitamin D, folate and vitamin B12, deficiencies which have been documented among 6–10-year-old children in India( 19 ).
Development of the knowledge, attitude and practice questionnaire
Responses of mothers to the questions and probes during the FGD were considered for making the item pool contextual. Questions in each domain which were never heard by the mothers were deleted. Some of the questions retained in the item pool were reframed to make them more understandable to the mothers. A few new questions that were not initially present in the item pool were also added. Some questions on a few topics, which had not been included earlier because they were thought to be too elementary, had to be added as the FGD revealed that such knowledge was not uniform. For example, in one FGD, all mothers knew that a branded salt available in that village is iodized, but one mother did not know that branded salt is iodized and only a few mothers knew the function of iodine. As caregivers had low knowledge on micronutrients, the majority of the new questions were added in the micronutrients domain, followed by cooking and eating practices, diet diversification and sunlight exposure. This resulted in a new 132-item KAP questionnaire, which was subjected to content analysis (Table 2).
Table 2 Number of items in the questionnaire during the process of testing the validity and reliability of the knowledge, attitude and practice questionnaire
FGD, focus group discussion.
Quantitative validation phase
Content validity
The KAP questionnaire was subjected to content validity by six experts drawn from various fields like nutrition (n 1), dietetics (n 2), psychology (n 1), medicine (n 1) and communication (n 1). The experts rated each question on a 4-point Likert scale that included different parameters such as relevance, clarity, simplicity and ambiguity.
Content validity index
The content validity index (CVI) was computed as the number of experts giving a rating of either 3 or 4, divided by the total number of experts who rated the questions. An item with CVI>0·8 was retained( Reference Yaghmaei 20 , Reference Polit and Beck 21 ).
The questionnaire was translated into the regional language, Telugu, using the forward–backward translation method. After translation, the questionnaire was pre-tested among five members from the study area with the same inclusion criteria but who were not a part of the main study.
Psychometric validation
Sample size
Estimating a 20 % increment in nutrition knowledge score, with a moderate effect size of 0·5 based on previous studies( Reference Hemlatha and Prakash 22 – Reference Vijayapushpam, Subba Rao and Antony 26 ) on health and education interventions in different community groups, with 95 % confidence and 80 % power, the required number of households was 160 with 20 % dropout rate in the ongoing project (CTRI registration number CTRI/2015/06/005836). As per the literature( Reference Javali, Gudaganavar and Raj 27 ), a sample size of fifty is sufficient to test the internal consistency of a questionnaire. As the sample size for the ongoing project is 160, the internal consistency of the questionnaire was tested in sub-samples of eighty participants. With a correlation (r) of 0·5 considering 95 % CI and 80 % power, the required sample size for reliability testing using the test–retest method was twenty-nine (thirty participants were recruited).
Administration of the questionnaire
Households meeting the inclusion criteria were approached and the questionnaire was administered by the investigators in the interview mode to the individual mothers at their households in their leisure period between 09.00 and 13.00 hours. The questionnaire was administered with an instruction to answer only if they knew the answer, and to select the option ‘don’t know’ if they were unsure of the answer. They were also instructed to stop the questionnaire administration if any question was not understood by them, and those questions were repeated and asked until they were understood. The time taken to complete the 132- and eighty-eight-item questionnaires was approximately 30 and 20 min, respectively. On average, six to eight households were visited per day to administer the questionnaire.
Item difficulty
The item difficulty was determined by the total number of correct responses to the test item. Item difficulty index (p) was calculated by using the formula: p=R/T, where R is the number of correct responses and T is the total number of responses. An item was considered difficult or easy when p<0·20 or p>0·80, respectively( Reference Garret and Woodworth 28 ).
Item discrimination
Item discrimination compares the number of high scorers and low scorers who answer an item correctly. It is the extent to which items discriminate among respondents in the high and low scorers. A total test was scored, the scores were rank-ordered, and 25 % of the highest and lowest scorers were selected. The number of correct answers in the highest 25 % was subtracted from the number of correct answers in the lowest 25 %. This result was divided by the number of people in the larger of the two groups; the resulting value was considered the item discrimination index (D)( Reference Kelley 29 , Reference Nunnally 30 ). A value D=0·20–0·29 was considered acceptable, D=0·30–0·39 as good and D≥0·40 was considered excellent as per available literature( Reference Ebel 31 ).
Internal consistency
The rational equivalence method using Cronbach’s α was employed to assess the reliability of the test. Cronbach’s α estimates the reliability of test scores with respect to (i) how well the individual items of the scores fit together and (ii) whether they assess the same construct. It assesses the intercorrelations of the items in the test and the correlations of the items with the test overall. A value α<0·70 is considered low and a value α>0·70 is considered adequate( Reference Cohen 32 ).
Test–retest reliability
The eighty-eight-item KAP questionnaire was administered twice among thirty mothers to test the stability of the questionnaire over time. The mothers were kept unaware of the retest, which was done two weeks after the test. The differences between the two measurements were plotted against the means of the two measurements by the Bland–Altman method( Reference Myles and Cui 33 ).
Scoring
All questions were closed-ended and had multiple choices, except three questions that were open-ended. There was only one correct answer to each question. The responses were scored by awarding a mark of 1 to the correct answer and a mark of 0 to an incorrect answer. The quality of individual items in the questionnaire was measured in terms of item difficulty, item discrimination and internal consistency.
Statistical analysis
Statistical analysis was not done for qualitative data, because those data were analysed based on the majority responses of the respondents. Statistical analyses for quantitative data were done using the statistical software package IBM SPSS Statistics version 24.0. Item analysis (item difficulty index p, item discrimination index D, Cronbach’s α) was done for psychometric validation of the eighty-eight-item questionnaire. The Bland–Altman plots were constructed using the MedCalc statistical program version 12.5.0.0 (MedCalc Software, Acacialaan, Belgium).
Results
Representative responses of the FGD participants are provided in Table 3. The insights from FGD which were used to prepare items in the KAP questionnaire are given in Table 4. In general, rice, milk, sugar and roots were consumed daily; green leafy vegetables and flesh foods were consumed once weekly; pulses, eggs, fruits and tubers were consumed twice weekly; and other vegetables three times weekly. The reasons for not consuming a diversified diet daily were either the respective foods were not available in the village market or dislike by the children in the households. The most prepared breakfast items included idly (fermented steamed rice cake), dosa (fermented pancake), upma (semolina porridge), bread, jam, milk and biscuit. The foods mostly liked by the children included carrot, onion, potato, chicken, fish, apple, banana, grapes, watermelon and mango. The foods purchased most frequently in the weekly market included potato, onion, tomato, ladies’ finger, banana, apple, grapes, papaya, watermelon, mango and all other seasonal fruits.
Table 3 Representative comments of the rural, literate, middle-income mothers of school-age children (6–10 years) on the focus group discussion themes, Ghatkesar sub-district, Medchal district, Telangana state, India (n 44)

Table 4 Insights from the focus group discussions (FGD) that were used to develop items for the knowledge, attitude and practice questionnaire

Quantitative data
Based on the FGD, the 127 KAP questions in the item pool were modified into a 132-item KAP questionnaire, which was subjected to content analysis and further reduced to a 125-item KAP questionnaire (Table 2). About three-quarters (72 %) of the questions from the item pool were based on FGD.
Psychometric validation
Following psychometric validation, the 125-item questionnaire was further reduced to eighty-eight items. The item difficulty index p for knowledge questions ranged from 0·10 to 0·91. There were five relatively easy questions (p=0·81–0·91) and five difficult questions (p=0·07–0·12), with all the rest being in the desirable range of difficulty.
The item discrimination index D for knowledge questions ranged from 0·09 to 0·68. Nineteen questions had D>0·40, five questions had D>0·30 and five questions had D>0·20.
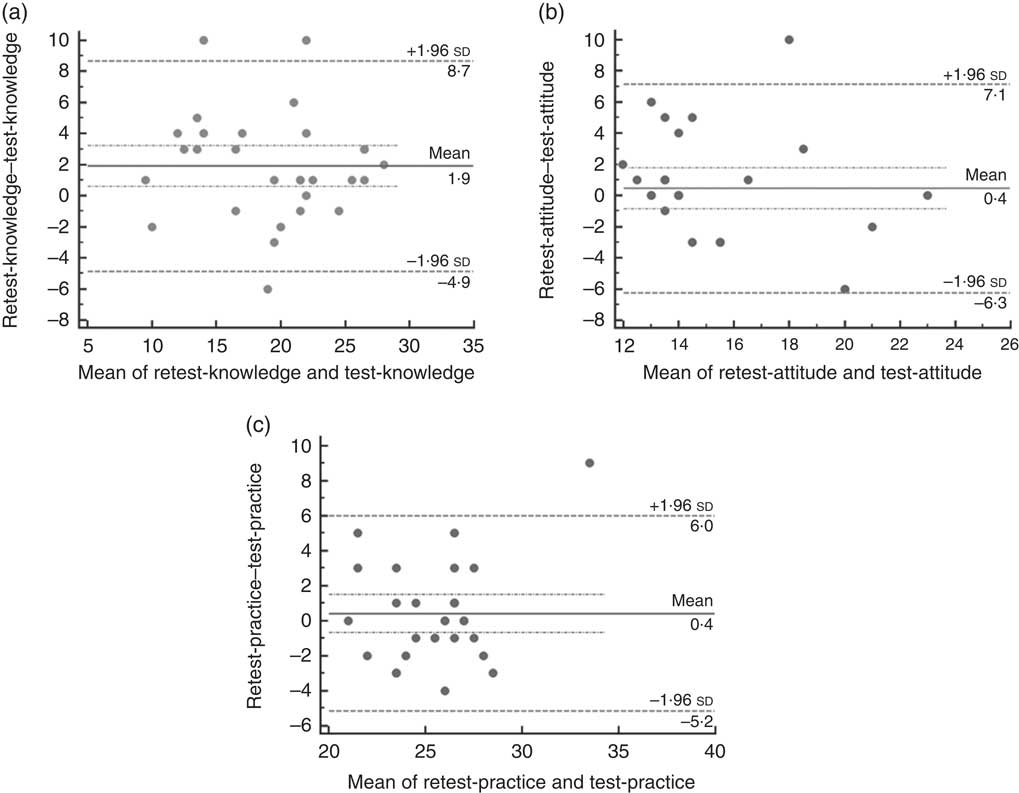
A Cronbach’s α value of 0·78 was obtained for the knowledge and attitude questions, whereas α=0·50 was obtained for practice questions, which are considered adequate and low, respectively. The Bland–Altman plots showed a mean bias of 1·9, 04 and 0·4 for the knowledge, attitude and practice questions, respectively, with few outliers, and had a good agreement between test and retest scores (Fig. 2(a)–(c)). The final questionnaire consisted of eleven, thirty, twenty-two and twenty-five items on diet diversity, micronutrients, cooking/eating practices and sunlight exposure, respectively.
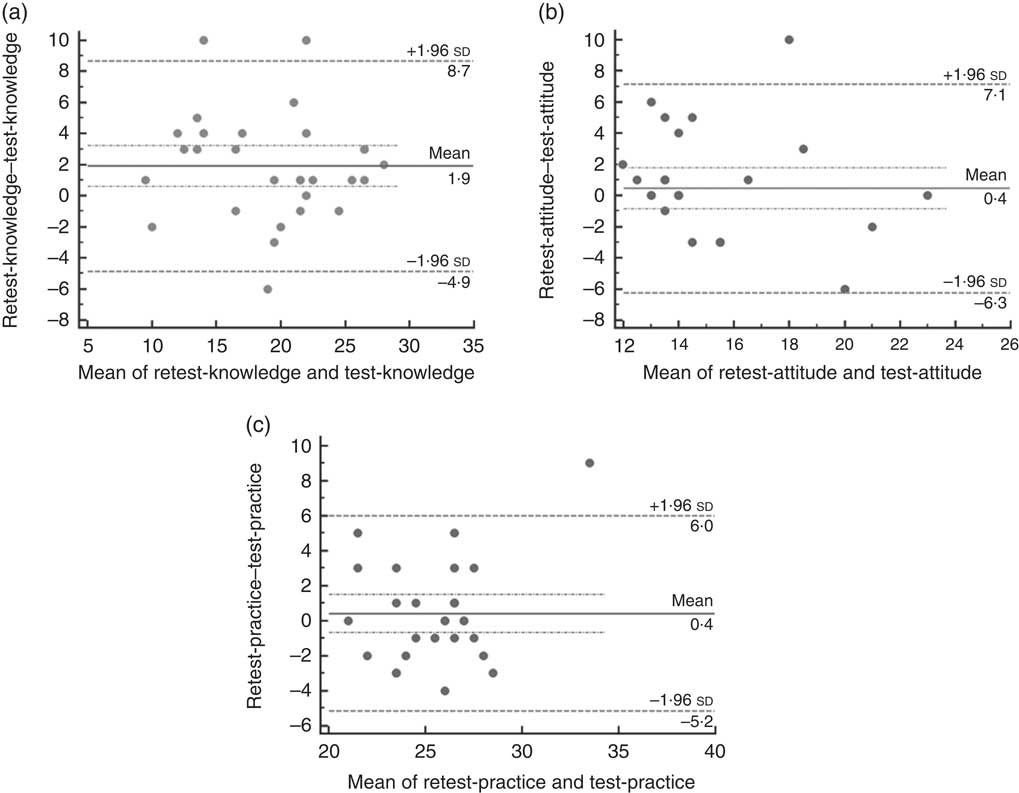
Fig. 2 Bland–Altman plots showing the agreement between test and retest scores on (a) knowledge questions, (b) attitude questions and (c) practice questions of the eighty-eight-item knowledge, attitude and practice questionnaire on micronutrients and factors affecting micronutrient status among rural, literate, middle-income mothers of school-age children (6–10 years), Ghatkesar sub-district, Medchal district, Telangana state, India (n 30). The differences between the retest and test scores were plotted against the means of the two scores and the limits of agreement were calculated. ![]() represents the mean difference between the retest and test (bias);
represents the mean difference between the retest and test (bias); ![]() represent the 95 % CI of the bias;
represent the 95 % CI of the bias; ![]() represent the upper and lower 95 % limits of agreement.
represent the upper and lower 95 % limits of agreement.
Discussion
The present study adopted two-phase exploratory methods to develop a comprehensive KAP questionnaire that captured inherent inabilities of mothers to practise a diversified diet to satisfy the micronutrient status of 6–10-year-old children. First, FGD-based qualitative data provided contextual understanding of the community’s ability to absorb and practise nutrition knowledge. In the second phase, a psychometrically validated KAP questionnaire was developed. This KAP questionnaire can be a valuable assessment tool and can contribute to public health nutrition policy.
The food people consume is affected by a large number of interrelated factors, including food availability, food accessibility and food choice, which in turn are influenced by geography, demography, disposable income, socio-economic status, urbanization, globalization, religion, culture, marketing and consumer attitude. Dietary diversification is considered one of the long-term sustainable strategies to combat micronutrient malnutrition globally. However, due to the lack of understanding of contextual factors that lead to the success of such interventions, there is a need for critical evaluation of (i) the level of awareness/knowledge and perceptions of the target population and (ii) barriers at community and individual level; apart from certain extraneous factors like availability, affordability and accessibility for practising dietary change( Reference Gavaravarapu, Konapur and Saha 34 ). This in turn could be due to a lack of context-specific validated tools that consider all these aspects.
A review of a large number of studies measuring nutrition knowledge revealed that most instruments that have been applied to measure nutrition knowledge have not been validated( Reference Steenhuis, Brug and Van Assema 35 ). Some authors reported a pilot investigation( Reference Petersen and Kies 36 – Reference Kristal, Bowen and Curry 42 ) in which the questionnaire was tested. Several studies have reported using only pre-tested questionnaires for collecting data on nutrition knowledge, but they have avoided mentioning the statistical or methodological steps in developing such questionnaires( Reference Mohapatra, Bulliyya and Kerketta 15 , Reference Bhavesh, Prakash and Shailesh 16 , Reference Lanerolle and Atukorala 43 – Reference Lakshman, Sharp and Ong 46 ). The importance of a structured approach to establishing the validity and reliability of a questionnaire, especially on micronutrients, was emphasized by Augustine et al. ( Reference Augustine, Vazir, Rao and Rao 9 ). The KAP questionnaires used in earlier studies were general nutrition KAP questionnaires focusing on dietary recommendations and diet–disease relationships( Reference Shepherd and Stockley 40 , Reference Anderson, Bell and Adamson 41 , Reference McDougall 47 – Reference Stafleu, van Staveren and de Graaf 49 ) or have concentrated on a specific aspect of nutrition such as fat( Reference Douglas and Douglas 39 ), fat, fibre and cholesterol( Reference Resnicow, Hearn and Delano 50 ), or micronutrients( Reference Augustine, Vazir, Rao and Rao 9 , Reference Bhavesh, Prakash and Shailesh 16 ) alone. These, although useful, may not provide information on KAP in the context in which the target population is situated.
Studies evaluating KAP on nutrition often adapt questionnaires from elsewhere, without conducting formative research in the study area( Reference Bhavesh, Prakash and Shailesh 16 , Reference Choi, Shin and Jung 51 , Reference Shaaban, Nassar and Abd Elhamid 52 ). For framing the questions themselves, formative research was seen to be the most helpful phase in the current study. Although a few studies have used a mixed-methods approach in assessing KAP on nutrition, the questionnaires have not been validated( Reference Choi, Shin and Jung 51 ). The KAP questionnaire in the current study is developed and validated based both on qualitative and quantitative data obtained from formative research. Therefore, unlike the earlier studies which had questions only on micronutrients, fat and food group knowledge, we consider ours is one of the early approaches to have adopted a holistic methodology in developing a comprehensive context-specific questionnaire. Additionally, our study looked not only into context in the formative phase, but also used appropriate quantitative analysis methods to ensure the consistency and reliability after examining the validity.
FGD aided in deleting, retaining, modifying and adding a few questions in the 127 questions in the item pool, resulting in a new 132-item KAP questionnaire which was subjected to content analysis. The basis for deletion of questions from the item pool in each domain was that either they were too basic or the participants had never heard of that particular concept (such as foods rich in vitamin B12, which vitamin helps in cognitive development). The item pool used for the questionnaire development addressed the micronutrients that had an established evidence of dietary deficiency such as iron and vitamin A( 5 ).
The Cronbach’s α for the entire KAP questionnaire was 0·70 (not reported), which is an acceptable value according to Nunnally( Reference Nunnally 53 ). When tested for individual constructs – knowledge, attitude and practice – the Cronbach’s α of knowledge and attitude remained the same (>0·70) but for the practice construct α was 0·50. The low Cronbach’s α for the practice construct could be due to various reasons. The primary reason appears to be due to fewer questions per domain in the practice construct as compared with the overall number of questions in the KAP questionnaire. Cortina( Reference Cortina 54 ) reported that internal consistency is sensitive to the number items in the questionnaire and it is likely to increase with increase in the number of items. Therefore, a low α value of one construct in the questionnaire could end up affecting the internal consistency of the questionnaire as a whole( Reference Cortina 54 , Reference Sijtsma 55 ). Moreover, the questions in the practice construct were diverse and there was scope for a lot of inconsistency in responses as multiple answers were possible. Multidimensionality of answers could have resulted in low Cronbach’s α. Although deleting a few items in the practice construct improved α to 0·65, they were purposely retained because they would be useful to assess the impact of the nutrition education intervention in the next phase of the study. Similar Cronbach’s α was reported in a review conducted by Stone et al. ( Reference Stone, Otten and Engels 56 ), wherein the Strengths and Difficulties Questionnaire (SDQ) had a total Cronbach’s α of 0·81, but the individual α values ranged from 0·53 to 0·81.
There are no cut-off values set for Cronbach’s α for an acceptable reliability. For instance, although Nunnally( Reference Nunnally 53 ) recommended a minimum α value of 0·70 for pilot studies and 0·80 and 0·90 for basic and applied research, respectively, other contemporary researchers characterized reliabilities of 0·60 and 0·70 as good or adequate( Reference Dekovic, Janssens and Gerris 57 , Reference Holden, Fekken and Cotton 58 ). However, for exploratory studies, lower Cronbach’s α values were considered acceptable( Reference Santos 59 ). Considering the multidimensionality of the practice construct in the questionnaire, the authors consider an α value of 0·50 for the practice construct to be acceptable.
A novelty of the questionnaire is the inclusion of the theme on sunlight exposure. Considering the pandemic deficiency of vitamin D and its importance in maintaining bone health, the authors believed that inclusion of questions pertaining to sunlight exposure will be a benefit in the study, as sunlight is the major source of vitamin D. Another novelty of the questionnaire is the inclusion of questions on barriers to diet diversification such as availability, affordability and accessibility, which were essential yet ignored in the earlier questionnaires (see online supplementary material).
A question related to iodine was not included in the questionnaire initially, expecting that the respondents will have awareness regarding iodized salt owing to the universal salt iodization programme which has been in place in the country for decades now. However, the FGD revealed that the majority of mothers were unaware of the health benefits of iodized salt. Hence, a question related to iodine was included in the questionnaire. The questionnaire also covered cooking and eating practices that influence bioavailability of micronutrients, such as washing green leafy vegetable prior to cutting them, consuming tea and coffee within 1 h of food consumption, and consumption of vitamin C-rich foods along with iron-rich foods( 60 ).
The combination of FGD and item pool helped in identifying the most appropriate items for inclusion in the questionnaire. FGD aided in understanding the current knowledge on micronutrients, the food scenario in the community, attitudes towards consumption of a diversified diet, underlying factors preventing consumption of a diversified diet, cooking practices and sunlight exposure. The options provided for each question in the item pool were modified according to the responses given by the participants in FGD.
The selection of questions from the item pool after content validity was difficult. The expertise of the panel regarding the domains tested, the anticipated difficulty level of the item and the essentiality of the information to be obtained for the intervention were considered while selecting questions. Questions that did not fall under an acceptable range of item difficulty were still considered for inclusion based on the qualitative understanding of the context, which was possible through the formative component of the study. Similarly, a few questions related to specific micronutrients that were earlier part of the item pool had to be modified because the FGD revealed that respondents knew more about the foods than the nutrients they contained. The authors felt that the terms ‘vitamins’ and ‘minerals’ would sound more like jargon to the respondents because they were relating food groups to a specific body function without even knowing about the micronutrient content of the same. For instance, when they were asked to identify the vitamin that was responsible for proper vision, most respondents could not specify vitamin A, but had an idea that consuming foods such as green leafy vegetables and carrots would help improve vision although they had no idea that they contained vitamin A. Therefore, the question ‘Can you identify the vitamin that helps in proper vision?’ was modified to ‘Identify foods that help in proper vision’. Likewise, a few questions in the item pool which earlier dealt with food sources and deficiency disorders of vitamin B12, folate, zinc and calcium also had to be modified. Thus, ‘Can you identify the mineral that improves height, weight and cognitive development?’ was replaced by ‘What are the food groups that should be consumed for proper height, weight and cognitive development of children?’. This indeed is a useful observation that would help build appropriate communication tools and messages to create awareness about these nutrients in the intervention phase of the study.
Questions that were felt to be inappropriate were deleted from the item pool and questions that were felt to be ambiguous by the expert panel members were modified. Thus, care was taken to select items which were simple and easily understandable to rural literate mothers of the middle-income group.
Respondents were not practising diet diversity daily at their households. So, based on the results of the FGD, questions related to identification of a balanced diet, such as frequency of variety of foods to be consumed daily, were included in the questionnaire. Questions related to food sources and deficiency symptoms were included in the questionnaire as respondents were not aware of them. Caregivers were also not aware of their family’s micronutrient status and they did not know what to do if they were deficient in some nutrient. So, questions pertaining to attitude towards their micronutrient intake and status were included.
As cooking and eating practices were not properly followed by a few mothers, questions related these were also included in the questionnaire. When probed on availability, accessibility and affordability for a diversified diet, it was revealed that availability of fruits in villages was a major hindrance to practising diversity, so questions related to those were also included in the questionnaire. FGD revealed that children were given importance during distribution of foods in all households, irrespective of food inflation. Further, all middle-income households were selected in the study, expecting a middle-income family to afford a diversified diet; hence, questions related to affordability were not included in the questionnaire.
Mothers had a positive attitude towards sunlight exposure. As the majority of mothers were aware of the importance of sunlight exposure, only questions related to time of day and duration for sun exposure were included in the questionnaire, as none of them were aware of these aspects. Thus, the selected eighty-eight-item questionnaire is a useful tool among rural literate mothers of the middle-income group to test KAP on micronutrients and factors affecting micronutrient status of 6–10-year-old children.
Strengths and limitations
The strength of the current study lies in the fact that all prerequisite steps of a mixed-methods approach were followed. Although the questionnaire deals with micronutrients and diet diversity, it is specific to the context and may not be directly suitable in other contexts and cannot be generalized. We consider that the methods employed and the documentation of the same would be a positive addition to the existing body of literature. The stepwise methodology is replicable in developing questionnaires in other contexts too. The small sample size need not be seen as a limitation because it is appropriate in the context of the study.
Conclusion
The sequential, exploratory, mixed-methods approach assisted in viewing the context of the study from multiple perspectives. Integrating qualitative and quantitative methods enhanced the understanding of knowledge gaps and facilitators and barriers of diet diversification. These findings will have implications for structuring the social behaviour change communication intervention model in the next phase of the study.
Acknowledgements
Acknowledgements: The authors wish to acknowledge the funding received from the Indian Council of Medical Research for carrying out the study. The Fellowship of the first author was supported by University Grants Commission, Government of India. The authors thank the Nutrition Society of India and Elsevier for the opportunity to present part of the results of this study at the 48th Annual Conference held in Bengaluru, India, 4–5 November 2016 and the 3rd International Conference on Global Food Security held in Cape Town, South Africa, 3–6 December 2017. The authors would like to thank the participants for taking part in the study. The authors would also like to acknowledge the assistance rendered by Mr Jawed, Mr Hrusikesh Panda, Ms Kiruthika Selvaraj, Ms Keren Susan Cherian and Ms Alekhya Sabbithi. A special thanks to Dr Little Flower Augustine for her critical comments on the manuscript. Financial support: This work was supported by the Indian Council of Medical Research (grant number 5/9/1138/2014-NUT). The Indian Council of Medical Research had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: All authors have participated in the research and have agreed to be authors of this paper. S.R.M.G. and M.N.K. conceptualized and designed the study, supervised the study and contributed to the preparation of the manuscript. A.K. was responsible for designing the questionnaire, implementation of the study, data collection and manuscript writing. B.N. provided the statistical analysis. All authors have read and approved the contents of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Institutional Ethics Committee, National Institute of Nutrition (Indian Council of Medical Research), Hyderabad, Telangana, India. Written informed consent was obtained from all subjects.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980019000521