



Food insecurity – having limited or uncertain availability of nutritionally adequate food – is a serious public health concern that is linked with a host of adverse physical and psychological health maladies(Reference Gundersen and Ziliak1). As of 2018, approximately 37 million individuals were living in food insecure households in the USA(Reference Coleman-Jensen, Rabbitt and Gregory2). In the USA, certain segments of the population such as racial/ethnic minorities and lower income households are more likely to be food insecure(Reference Coleman-Jensen, Rabbitt and Gregory2–Reference Gundersen, Kreider and Pepper3). Even so, there has been limited research on food insecurity among lesbian, gay and bisexual (LGB) individuals. This is surprising considering LGB individuals have greater rates of poverty(Reference Badgett4) and experience worse overall health(Reference Bostwick, Hughes and Everett5–Reference Conron, Mimiaga and Landers6) relative to heterosexual people, with especially high rates of hardship and health issues found among bisexual men and women(Reference Badgett4–Reference Mereish, Katz-Wise and Woulfe8).
To date, only a few studies have addressed the topic of food insecurity among LGB individuals. One study using data from the June to December 2012 Gallup Daily Tracking Survey found that 28 % of lesbian, gay, bisexual or transgender individuals compared with 18 % of non-lesbian, gay, bisexual or transgender persons reported that they did not have enough money for food at some time in the past year(Reference Gates9). Furthermore, drawing on data from the 2006–2010 National Survey of Family Growth, this same study found that bisexual individuals (25 %) were more likely than lesbian/gay (14 %) and heterosexual persons (15 %) to report participation in the Supplemental Nutritional Assistance Program, although this survey did not directly assess food insecurity. Another study using data on women from the 2004–2014 National Health and Nutrition Examination Survey examined food insecurity among four categories of females: exclusively heterosexual (i.e., sexually attracted to only men), bisexual (i.e., sexually attracted to men and women), lesbian (i.e., sexually attracted to only women) and heterosexual women who reported sexual activity with women. The current study found elevated rates of food insecurity and severe food insecurity among lesbian (food insecurity = 25·5 %; severe food insecurity = 13·7 %), bisexual (food insecurity = 27·3 %; severe food insecurity = 13·5 %) and heterosexual women who reported sexual activity with women (food insecurity = 20·6 %; severe food insecurity = 11·4 %), compared with exclusively heterosexual women (food insecurity = 13·1 %; severe food insecurity = 5·5 %)(Reference Patterson, Russomanno and Tree10).
While informative, studies on food insecurity among sexual minorities and prior literature remain limited in important ways. For instance, some prior studies use data only on women, thus limiting the generalisability of the findings to the broader LGB population(Reference Patterson, Russomanno and Tree10). Data used in past studies are also somewhat dated (occurring prior to 2015). Using contemporary data is important considering there have been stark changes to public opinion about the LBG community(Reference McCarthy11) and an expansion of rights (i.e., same-sex marriage in June 2015) in recent years. Even so, post-2016 there has been a rollback of many LGB protections at the federal level and nationally(Reference Moreau12). Additionally, while the use of nationally representative data in prior studies is informative for generalisability, it remains unclear whether LGB individuals face higher rates of food insecurity in contexts with greater LGB rights and support. Indeed, past research finds discrimination to be a risk factor for food insecurity(Reference Phojanakong and Brown Weida13). Moreover, there is significant geographic variation in public support for LGB rights, with rural areas and states in the South and Midwest offering less public support compared with metropolitan areas and states in the Northeast and West(14). In particular, New York City has long been a centre of a progressive LGB movement, and New York has been at the forefront of passing laws barring discrimination based on sexual orientation in employment, housing and public accommodations(15). It remains possible that findings from prior studies with broad national samples detecting higher food insecurity among LGB individuals could be driven by contexts with less LGB support.
The current study aims to extend this literature by examining the association between sexual orientation and food insecurity using a recent data from New York City. Specifically, we assess whether in recent years individuals identifying as LGB were more likely to experience food insecurity relative to heterosexual individuals.
Data
Data for the current study are pooled from the 2017 and 2018 New York City Community Health Survey (CHS). The CHS is an annual survey that uses a stratified random sampling technique to produce a cross-sectional survey that is representative of non-institutionalised New York City residents aged 18 or older who have a cellular phone or live in a household with a landline phone. The sampling frame was constructed via a list of telephone numbers provided by a commercial vendor, and one adult is randomly selected from the household to complete the interview. The CHS is conducted by the New York City Department of Health and Mental Hygiene using a computer-assisted landline and cellular telephone survey(16).
Dependent variable
Food insecurity is measured using an item asking respondents: ‘In the past six months, which of the following best describes the food eaten in your household:’ no food insecurity (had enough of the kinds of food they wanted to eat), mild food insecurity (had enough but not always the kinds of food they wanted to eat) and moderate-to-severe food insecurity (sometimes there was not enough to eat, or often there was not enough to eat)(Reference Jackson, Chilton and Johnson17). Prior research documents that health problems tend to worsen as food insecurity levels become more severe(Reference Gregory and Coleman-Jensen18).
Independent variable
Sexual orientation is a categorical variable from a question asking respondents to describe their sexual identity. Responses include heterosexual, gay/lesbian, bisexual or something else. A separate gender identity question was also available to further classify individuals into categories including cisgender (non-transgender), transgender, gender non-conforming, something else and other gender identity. There were too few responses to reliably analyse the subgroups based on gender identity. Therefore, we opted to remove the something else sexual orientation category and the following gender identities: transgender, gender non-conforming, something else and other gender identity.
Covariates
Control variables include race/ethnicity (White, Black, Hispanic, other race/ethnicity), sex (1 = male, 0 = female), age (18–24, 25–29, 30–44, 45–64, 65+), education level (less than high school, high school graduate, some college, college graduate), the number of persons living in a household (adults and children under the age of 18 (range 1–7)), married/coupled (1 = yes, 0 = no), whether a child was living in the home (1 = yes, 0 = no), whether a respondent is a home owner (1 = owner, 0 = renter), currently employed (1 = currently employed; 0 = unemployed/out of the labor force) and if a respondent is living at < 200 % federal poverty line (1 = yes, 0 = no). Models include a binary variable for survey year (1 = 2018; 0 = 2017) and a categorical indicator controlling for borough for residence (Brooklyn, Bronx, Manhattan, Queens, Staten Island).
Method
Multinomial logistic regression was used to examine the association between sexual orientation and food insecurity, net of covariates. All models are adjusted for survey weights using the SVY command in Stata 16.1. An analysis of variance inflation factors revealed no serious concerns with multicollinearity(Reference Allison19). Patterns of missing data are reported in Appendix A.
Results
The summary statistics of the sample stratified by sexual orientation presented in Table 1 reveal that bisexual respondents were the least likely to report no food insecurity (52·8 %) and had the highest rates of mild food insecurity (35·0 %) and moderate-to-severe food insecurity (12·2 %). The results of the multinomial logistic regression in Table 2 show that bisexual individuals were more likely to experience both mild (relative risk ratio (RRR) = 1·719, 95 % CI 1·148, 2·573) and moderate-to-severe food insecurity (RRR = 1·851, 95 % CI 1·097, 3·122) relative to heterosexual individuals. The predicted probabilities using the marginal standardised technique(Reference Muller and MacLehose20) shown in Fig. 1 demonstrate 12·3 % of bisexual individuals were predicted to have experienced moderate-to-severe food insecurity, compared with 8·6 % of heterosexual individuals. Conversely, 58·0 % of bisexual individuals were predicted to be food secure compared with 69·7 % of heterosexual individuals.
Table 1 Weighted summary statistics stratified by sexual orientation†
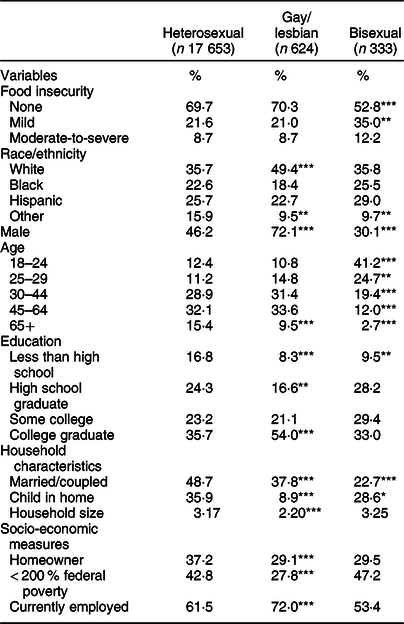
* P < 0·05, **P < 0·01, ***P < 0·001.
† P-values represent differences in mean t test compared with heterosexual respondents.
Table 2 Results of multinomial logistic regression of food insecurity on sexual orientation (n 18 610)

*P < 0·05, **P < 0·01, ***P < 0·001.

Fig. 1 Predicted probabilities of food insecurity by sexual orientation. ![]() , No food insecurity;
, No food insecurity; ![]() , Mild food insecurity;
, Mild food insecurity; ![]() , Moderate-to-severe food insecurity
, Moderate-to-severe food insecurity
Supplemental analyses
Supplemental analyses were conducted using a stratified sample of males and females. Appendix B documents that bisexual females had the highest levels of mild food insecurity (40·7 %), which was nearly double the level of bisexual males (21·7 %). However, bisexual males reported the highest levels of moderate-to-severe food insecurity (15·9 %). Multinomial logistic regression analyses stratified by biological sex in Appendix C reveal generally positive but non-significant associations between LGB sexual orientation and food insecurity. The large CI indicate that when the sample is stratified by sex, the estimates become unstable due to small sample size and thus should be interpreted cautiously. Still, findings indicate that bisexual females experience mild-food insecurity (relative to no food insecurity) at approximately twice the rate as heterosexual females (RRR = 2·152, 95 % CI 1·313, 3527).
Discussion
The findings demonstrated that bisexual individuals in New York City are more likely to experience both mild and moderate-to-severe food insecurity compared with heterosexual individuals. These findings confirm the results of earlier research, which suggest that sexual minorities are at an elevated risk for food insecurity even after adjusting for markers of socio-economic status(Reference Gates9–Reference Patterson, Russomanno and Tree10). Moreover, the study finding showing that bisexual individuals are at the greatest risk for food insecurity is also consistent with recent research that has found among the LGB community, bisexual individuals experience the greatest rates of economic hardship and worse health outcomes(Reference Badgett4–Reference Mereish, Katz-Wise and Woulfe8). Analyses stratified by sex demonstrated mild food insecurity is particularly elevated among bisexual females. Taken together, the current study extends prior literature which has been conducted on a national scale and finds that the risk for food insecurity remains even in LGB supportive contexts such as New York City.
The results suggest that expanding efforts by government agencies (i.e., NYC Human Resources Administration) and non-profit organisations (i.e., Food Bank for New York City) to provide information and resources to help connect LGB individuals to public assistance programmes such as Supplemental Nutritional Assistance Program may be a promising avenue given research indicating the benefit of Supplemental Nutritional Assistance Program for alleviating food insecurity(Reference Bartfeld, Gundersen and Smeeding21–Reference Ratcliffe, McKernan and Zhang22). Another option may be through providing information and connections to food assistance through local LGBTQ community centres, as well as government and non-profit agencies. Because fear of bias and discrimination may inhibit attending religiously affiliated food pantries(Reference Russomanno, Patterson and Jabson23), expanding food pantry resources into LGBTQ community centres may a beneficial approach. Third, the expansion of mobile feeding programmes to areas with larger LGB communities may also provide benefits as such programmes offer the benefit of bringing food to individuals, rather than requiring individuals to travel to retailers to access food(24).
The current study also points to areas of future research. It would be useful for future work to further explore the mechanisms that may explain greater hardship among bisexual individuals. For example, recent research suggests that bisexual individuals may face particularly heightened levels of discrimination(Reference Van, Mereish and Woulfe25), social exclusion(Reference Hayfield, Clarke and Halliwell26–Reference Kertzner, Meyer and Frost27) and loneliness(Reference Mereish, Katz-Wise and Woulfe8), all of which can serve as risk factors for food insecurity(Reference Phojanakong and Brown Weida13,Reference Burris, Kihlstrom and Arce28) . Research also shows that LGB individuals are more prone to experiencing adverse childhood experiences compared with heterosexual individuals(Reference Austin, Herrick and Proescholdbell29–Reference Andersen and Blosnich30). Considering emerging research detailing a link between adverse childhood experiences s and food insecurity(Reference Jackson, Chilton and Johnson17,Reference Testa and Jackson31) , it is important for future research to explore whether adversities from earlier in life may underpin this association.
Limitations
There are a few limitations in the current study. First, the question measuring food insecurity references the prior 6 months, rather than past year as measured by the United States Department of Agriculture; therefore, food insecurity rates may be lower compared with studies that use longer reference periods. Second, the measure of food insecurity relies on a single-item measure rather than the multi-item United States Department of Agriculture scale. While the measure in the NYS CHS data offers a valid proxy for levels of food insecurity(Reference Jackson, Chilton and Johnson17,Reference Alaimo, Briefel and Frongillo32) , it would be useful for future research to evaluate the questions in the current study using the full United States Department of Agriculture scale in order to tap into additional factors such as the sufficiency of access to food and food consumption (i.e., quality, quantity, desirability). Relatedly, there is a lack of research assessing the relationship between sexual orientation and dietary quality. Accordingly, a vital area of future research is to investigate the association between sexual orientation and the quality of nutritional intake, as well as assess how food insecurity may moderate the association between sexual orientation and diet. Third, the NYC CHS study identifies sexual orientation and gender identity with two separate questions. There were too few responses tapping into gender identities (transgender, gender non-conforming, something else) to reliably analyse in the current study. Therefore, the sample was limited to non-transgender individuals. Still, future research that examines food insecurity across varying gender identities would be useful in expanding knowledge in this important area. Fourth, while we were able to control for several measures of socio-economic status, the NYC CHS data do not include information on participation in public assistance programmes such as Supplemental Nutritional Assistance Program. Fifth, the current study did not include health-related covariates because the reference period was typically after food insecurity. However, it would be beneficial for future research to investigate whether physical or psychological health confounds the association between sexual orientation and food insecurity. Finally, the study was drawn from New York City and therefore results are not generalisable to broader populations outside of this context.
Conclusions
Among New York City residents, bisexual individuals were found to have significantly higher rates of mild and moderate-to-severe food insecurity compared with heterosexual individuals. The results suggest that bisexual individuals are a group at an elevated risk of food insecurity. Study findings suggest medical and public health practitioners, as well as community organisations should collaborate to develop efforts to connect LGB individuals with resources that can help alleviate food insecurity and promote greater health equity among this population.
Acknowledgements
Acknowledgements: None. Financial support: This research received no funding or financial support. Conflict of interest: The authors do not have any conflicts of interest including financial interests or relationships or affiliations relevant to the subject of the manuscript. Authorship: A.T. conceptualised the study, conducted the data analysis and contributed to the writing. D.B.J. helped conceptualise the study and contributed to the writing. All authors reviewed, commented and revised drafts of the manuscript. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the University of Texas at San Antonio. Verbal informed consent was witnessed and formally recorded from all subjects/patients.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020005157





