


Vitamin A deficiency (VAD) is a public health problem affecting many pregnant women and children in Africa and South-East Asia( 1 ). In children, VAD is associated with an increased risk of morbidity and mortality due to xerophthalmia, diarrhoea, acute respiratory disorders and impaired cognitive function( Reference Rice, West and Black 2 ). In pregnant women, VAD is associated with fetal loss, preterm birth, all-cause infant mortality, and maternal morbidity and mortality( Reference Rice, West and Black 2 ).
According to the Tanzania Demographic and Health Survey (DHS), in 2010, 33 % of children aged 6–59 months and 37 % of women aged 15–49 years in Tanzania were vitamin A deficient( 3 ). Most VAD in Tanzania is due to low dietary intake (although inflammation and infection also reduce measured serum retinol-binding protein, a biochemical indicator of VAD used in the DHS( 3 )). The majority of the complementary foods given to children are made from grains that lack vitamin A( 3 ). To improve vitamin A intake, increasing dietary diversity, supplementation and food fortification could be adopted. In 1987, vitamin A supplementation was provided to children aged 6–59 months suffering from VAD-related diseases in government-run primary health-care facilities( Reference Mullins and Ehrlick 4 , 5 ). In 1997, vitamin A supplementation was introduced into the routine WHO Expanded Programme on Immunization for children aged 6–24 months and postpartum mothers( 5 ). Although coverage of vitamin A supplementation to improve vitamin A intake for children aged <5 years and postpartum women has improved significantly in the country since 2005( 6 ), increasing coverage to reach all children and postpartum women is expensive( Reference Horton, Begin and Greig 7 ). Moreover, high doses of vitamin A increase the risk of teratogenesis during the first trimester of pregnancy when women may not know that they are pregnant. Compared with supplementation, food fortification is usually less costly as it utilizes the existing food product market( Reference Allen, de Benoist and Dary 8 ). Fortified foods are also safe for consumption by pregnant women due to the much lower dose of vitamin A. The fortification process is simple to implement and could have a quick and significant impact without involving substantial change in consumer behaviour that is needed for dietary diversification( Reference Allen, de Benoist and Dary 8 ). Although vitamin A supplementation is recommended by WHO for reducing vitamin A deficiency in children aged <5 years( 9 ), several studies have shown that compared with supplementation, food fortification is more effective in reducing VAD( Reference Mason, Ramirez and Fernandez 10 , Reference Solon, Fernandez and Latham 11 ).
To reduce the prevalence of micronutrient deficiencies, in 2011, the Government of Tanzania mandated all businesses to fortify wheat flour, maize flour and vegetable oil with vitamin A, Fe and/or Zn( 12 ). Such legislation is, however, usually met only by large-scale producers that focus mainly on urban markets. The legislation is difficult to implement in remote areas which are predominantly served by local small and medium-sized enterprises that often do not have sufficient knowledge or the necessary resources that are required for fortification. Hence, the Masava project was implemented from November 2015 to June 2017 to support small and medium-sized enterprises to fortify unrefined sunflower cooking oil with vitamin A and distribute it in Manyara and Shinyanga regions, where the prevalence of VAD is among the highest in the country( 3 ). According to the Tanzania 2010 DHS survey( 3 ), in Manyara, 44 % of children aged 6–59 months and 54 % of women aged 15–49 years were vitamin A deficient, and in Shinyanga, 37 % of children and 43 % of women were deficient( 3 ). To promote consumption of the fortified oil, the oil was initially made available by the Masava project with a subsidy which offset the higher fortification and packaging costs required, through a mobile phone-based electronic voucher (e-Voucher) system.
To ensure that fortified foods are consumed in the right amounts by individuals who most need them, fortification programmes benefit from being implemented alongside communication interventions that are targeted towards behaviour change, at the population, community and individual levels consistently and simultaneously( Reference Michie 13 ). Social marketing provides a framework for designing interventions that aim to promote a specific behaviour of a target audience in order to improve their personal welfare and that of the society by offering benefits that they want, reducing barriers that they are concerned about and using persuasion to create motivation to participate in the programme( Reference Kotler and Roberto 14 ). To improve consumption of vitamin A-fortified sunflower oil, under the Masava project, a social marketing intervention was implemented. The intervention promoted consumption of vitamin A-fortified sunflower oil, at the household level, by conveying messages concerning the health benefits of fortified oil and the availability of the oil at a subsidized price in six districts in Manyara and Shinyanga.
Many theories have been proposed across multiple disciplines that attempt to explain the process of behaviour change. Many of these theories have overlapping constructs but are named differently( 6 ). For instance, social norms have been incorporated as a determinant of behaviour in a number of behaviour change theories such as the Theory of Planned Behaviour( Reference Montano and Kasprzyk 15 ) and Social Cognitive Theory( Reference McAlister, Perry and Parcel 16 ). To address the multitude of different but overlapping theories, the Theoretical Domains Framework (TDF) was developed which provides an approach that, rather than relying on a single behaviour change theory, integrates frameworks for change based on synthesis of 128 theoretical constructs from thirty-three psychological behaviour change theories( Reference Michie, Johnston and Abraham 17 ). The TDF developed by Michie et al. ( Reference Michie, Johnston and Abraham 17 ) identifies fourteen domains of behaviour change constructs: (i) knowledge; (ii) skills; (iii) social/professional role and identity; (iv) beliefs about capabilities; (v) optimism; (vi) beliefs about consequences; (vii) reinforcement; (viii) intentions; (ix) goals; (x) memory, attention and decision processes; (xi) environmental context and resources; (xii) social influences; (xiii) emotion; and (xiv) behavioural regulation( Reference Michie, Johnston and Abraham 17 ). The TDF has been used to develop and evaluate interventions( Reference French, Green and O’Connor 18 , Reference Thomas and Mackintosh 19 ), as well as identify facilitators and barriers to implementation practices and behaviours( Reference Yamada, Potestio and Cave 20 – Reference Grady, Seward and Finch 22 ). To date, to the best of our knowledge, the TDF has not been used to evaluate social marketing interventions to identify facilitators and barriers to the uptake of fortified foods.
The present paper reports on an evaluation of the effectiveness of a social marketing intervention in improving knowledge and attitudes, as predictors of behaviour change, and household consumption of vitamin A-fortified oil in Manyara and Shinyanga regions in Tanzania.
Methods
Setting
The study was conducted in two regions in Tanzania. In the Manyara region, four districts were involved: Babati Urban, Babati Rural, Hanang and Mbulu. In the Shinyanga region, involved districts were Shinyanga Urban, Shinyanga Rural, Kahama Urban and Kishapu.
Study design
The study employed a quasi-experimental non-equivalent control group study design, in which three of the four districts in each region were non-randomly assigned to the intervention group and one district served as the control group. The intervention districts were selected based on the desire of the enterprises that produce the fortified oil to distribute to the region, the researchers’ desire to include a mix of urban and peri-urban districts, and the availability of good cell phone network connectivity that is required for redemption of e-Vouchers.
Intervention
The intervention was implemented in the six intervention districts from February 2016 to March 2017. The desired behaviour change was to substitute traditional unfortified cooking oil with vitamin A-fortified sunflower oil in household cooking. The target population was lactating women with children aged <5 years. The fortified oil was made available through retailers who were recruited under the Masava project in the intervention districts. With the discount provided through the e-Voucher technology, on average, one litre of the fortified oil cost about Tsh 2900, which is comparable to the price of the regular unfortified oil, about Tsh 3000; although both these prices varied considerably depending on the season. To inform the intervention strategy for promoting consumption of the fortified oil, a formative survey, comprising thirty-six key informant interviews and twelve focus group discussions, was conducted in November–December 2014 to identify current levels of knowledge, attitudes and practice (KAP) regarding vitamin A and fortified foods, household decision making and determinants of food purchasing behaviour (Tanzania Communication and Development Center, unpublished results).
The intervention took a deliberate approach to blend classic marketing strategies, such as brand awareness and price discounts, with behaviour change communication and education through trusted sources of information such as health professionals, community health workers (CHW) and religious leaders. To promote consumption of the fortified oil among households, the social marketing approach identified and worked from the values and desires of the target audience; the campaign sought to build awareness of health benefits of vitamin A for their children, as well as of its affordability and accessibility. The intervention highlighted messages of the health benefits of vitamin A, availability of vitamin A-fortified sunflower oil at a discounted price, and how to identify fortified oil from the fortification logo, through community events and community mobilization activities. The events and activities included: (i) clinic shows conducted by nurses to encourage people to associate using fortified oil with healthier families, as health workers were reported as the most trusted sources of information according to the formative survey; (ii) cooking shows to demonstrate that no additional skills are required in cooking with fortified oil compared with traditional unfortified oil, emphasize the equivalence in cost of fortified oil and offer free food-tasting after the show; (iii) road shows and cultural dances to also address false beliefs about fortified foods; and (iv) distribution of information, exchange and communication (IEC) materials such as flyers and pamphlets at health clinics and during promotional events.
As health workers were identified as the most trusted sources of information, CHW were recruited to provide education at the community level as well as through home visits. Religious and community leaders were involved in implementing the community activities. It was important to involve religious leaders in the Masava activities to address any religious misconceptions regarding consumption of fortified foods. To involve men, messages were disseminated through bicycle races and football matches that were implemented in Shinyanga, where household spending on food was dominated by men, according to the formative research. A live radio talk show was conducted after the endline survey to prevent contamination between the intervention and control districts.
In terms of planning and intervention design criteria that have been put forward as exemplary of social marketing projects( 23 ), the Masava project met these benchmarks (Table 1). However, the social marketing benchmarks convey that we rely on the procedures and principles of a social marketing project. On the other hand, the TDF is a tool that can be used to explore the theoretical domains that were important in mediating the behaviour change, if observed. Therefore, we used the TDF to inform the intervention evaluation, although the interventions did not initially apply the TDF in its design. The intervention addressed twelve of the fourteen domains of the TDF as barriers to and enablers of behaviour change, at the design and implementation levels. The domains addressed were: knowledge; skills; social/professional role and identity; beliefs about capabilities; optimism; beliefs about consequences; reinforcement; intentions; memory, attention and decision processes; environmental context and resources; social influences; and emotion. Table 2 shows the fourteen domains of the TDF along with their definitions and how the intervention design and implementation addressed twelve of the fourteen domains( Reference Cane, O’Connor and Michie 24 ).
Table 1 Social marketing benchmark criteria and how each benchmark was met in the Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017
Table 2 Domains of the Theoretical Domains Framework (TDF) and domains addressed in the design and implementation of the Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017
CHW, community health worker; IEC, information, exchange and communication.
Sample size calculation
Assuming maximum variability in the population (P = 0·50), 5 % margin of error and 95 % CI, the minimum required sample size was 385. To account for non-response rate, the minimum sample size was increased by 5 % to 404.
Sample size
During the baseline survey, 568 mothers were interviewed in the intervention (n 366) and the control (n 202) groups. Of these, 494 (309 in the intervention and 185 in the control group) were followed up after 9 months of intervention, giving an attrition rate of 13 %.
Sample selection
From each intervention and control district, lactating mothers with children aged <5 years were identified by personnel from health centres. The list of mothers was then stratified based on age group, geographic location and income level. From each stratum, mothers were randomly selected to obtain a representative sample.
Data collection
Data on predictors of behaviour change (knowledge of vitamin A and fortification) and self-reported fortified oil consumption were collected in June–July 2015 before the implementation of the intervention and in November 2016–January 2017 after about 9 months of intervention. The KAP data were collected as part of a larger survey that collected information on household characteristics, sociodemographic characteristics, maternal and child diet, maternal and child health, and household oil-purchasing patterns, which is being studied elsewhere( Reference Walters 25 ). The KAP questionnaire is based on a KAP survey on the use of fortified oil in West Africa from Hellen Keller International( 26 ). The KAP questionnaire collected information on knowledge of vitamin A and its health benefits, source of information on vitamin A and methods that could be taken to improve vitamin A intake. Four additional questions were added to the endline survey to test knowledge of fortification and to get information on self-reported consumption of fortified oil. The KAP questionnaire is given in the online supplementary material. The questionnaire was translated from English into Swahili. All mothers were interviewed in Swahili through home visits by CHW and researchers from the Sokoine University of Agriculture in Tanzania who were trained to conduct the survey. Oil samples were collected during the endline survey from each household to test for retinol content which is used as an indicator of actual fortified oil consumption. Consent was obtained from all mothers prior to data collection. A paper-based survey was used at baseline; and tablets, using the iFormBuilder application (2017), were used at endline.
Data processing
All data were entered into spreadsheets in Microsoft® Excel 2013. Knowledge of vitamin A was examined based on responses of ‘yes’ or ‘no’ when asked, ‘Have you heard information about vitamin A?’ Knowledge of health benefits of vitamin A was considered a ‘yes’ if the respondent mentioned at least one correct health benefit of vitamin A. Correct health benefits of vitamin A include helps with child growth, strengthens immunity to illness, improves vision, improves health/reduces illness, avoids night-blindness and reduces mortality. Knowledge of fortification was coded as ‘yes’ if the respondent noted ‘additional nutrients added to food’. Respondents were considered to be using fortified sunflower oil only if they knew the oil was fortified from the fortification logo or from the retailer. ‘Don’t know’ responses were considered not using fortified oil. Oil samples were analysed for retinol content by the Tanzania Food and Nutrition Centre using HPLC. In the data analysis step, the retinol content was divided into three categories: inadequately fortified, adequately fortified and overfortified, based on the range recommended by the Tanzania Bureau of Standards for fortification with retinyl palmitate of 20·0–40·0 mg/kg which converts to 36·6–73·3 mg retinol/kg( Reference Horton, Saleh and Mosha 27 ).
Statistical analysis
Baseline differences in age, setting, education level, and knowledge of vitamin A and methods that could be used to improve vitamin A intake between the intervention and control districts were compared using the χ 2 test. The McNemar test was used to compare changes in knowledge of vitamin A, health benefits of vitamin A, methods that could be used to improve vitamin A intake and fortification, and self-reported consumption of vitamin A-fortified oil before and after the intervention. To compare the differences in knowledge, attitudes, self-reported use of fortified oil and distribution of retinol content of oil samples between the intervention and control districts, the χ 2 test was used. For all tests, a P value of <0·05 was considered significant. All statistical analyses were carried out on R version 3.3.1.
Ethics approval
The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Office of Research Ethics of the University of Waterloo (ORE file number 20501) and the National Institute for Medical Research of Tanzania (NIMR/HQ/R.8/VOLIX/1299). Verbal consent was obtained from all subjects. Verbal consent was witnessed and formally recorded.
Results
Sociodemographic characteristics
Table 3 shows sociodemographic characteristics of the mothers in the intervention and control groups at baseline. There was no statistically significant difference in age and education level between mothers in the two groups. Attrition rates were low enough not to cause concerns about bias in the endline survey. Reasons for attrition included migration and unavailability of the mothers at the time of the endline survey. The only difference that was significant between the attrited households and those that were followed up was that mothers from the attrited households were younger (by 2 years) than those who were followed up( Reference Walters 25 ).
Table 3 Sociodemographic characteristics of mothers in intervention and control districts at baseline of the Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017 (n 568)
No significant difference between mothers in the intervention and control districts.
Change in knowledge, attitudes and practice
Table 4 shows findings on knowledge of vitamin A, health benefits of vitamin A and use of fortified foods to improve vitamin A intake, before and after 9 months of intervention, in the intervention and control districts. At baseline, there was no significant difference in any of the knowledge items between the intervention and control districts. After 9 months of intervention, intervention districts showed no significant improvement in knowledge of vitamin A compared with before the intervention as well as compared with control districts. Knowledge of using fortified foods to improve vitamin A intake decreased, although insignificantly, from pre- to post-intervention in both the intervention and control districts. However, knowledge of health benefits of vitamin A increased significantly from 33 to 45 % in the intervention districts (P = 0·002) and from 32 to 45 % in the control districts (P = 0·012). Knowledge of fortification was significantly higher in the intervention districts after the intervention than in the control districts (16 v. 7 %, P = 0·003).
Table 4 Knowledge and attitudes towards vitamin A among mothers in intervention and control districts at baseline and endline of the Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017 (n 494)
NA, not available.
* Significantly different from baseline (95 % CI).
† Significantly different from control districts (95 % CI).
Table 5 shows the self-reported use of fortified oil among those who had heard of vitamin A and the source of information that the oil is fortified among those who reported using fortified oil after the intervention. Among 392 women who had heard of vitamin A, five women reported using the fortified oil. All five women belonged to the intervention districts. There was no significant difference in self-reported fortified oil use between the intervention and control districts. Among the five women who reported using the fortified oil, four reported knowing that the oil was fortified from the fortification logo and one mentioned that she was told by the retailer.
Table 5 Self-reported use of fortified oil among those who heard about vitamin A and source of information that the oil is fortified among those who reported using fortified oil after the intervention, Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017 (n 392)
No significant difference between intervention and control districts.
Out of 494 households interviewed at endline, oil samples could not be obtained from thirteen households. Table 6 shows the distribution of the 481 household oil samples in the inadequately fortified, adequately fortified and overfortified categories. At endline, the proportion of households consuming inadequately fortified oil was significantly lower and the proportions consuming adequately fortified and overfortified oil were significantly higher in the intervention districts compared with the control districts.
Table 6 Retinol level in oil consumed by households after the intervention, Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017 (n 481)
† Significantly different from control districts (95 % CI).
We also examined differences in sociodemographic characteristics between mothers who could not be followed up and those who were followed up (data not shown). Between those two groups, there was no significant difference in the number of years of education (6·9 years among those who were followed up v. 7·5 years among those who attritted, P = 0·06, t test at 95 % CI) and knowledge of vitamin A at baseline (70·2 v. 75·5 %, P = 0·33, χ 2 test at 95 % CI). However, mothers who were followed up were significantly older than those who were not followed up (mean of 30·3 v. 26·5 years, P <0·05, t test at 95 % CI).
Sources of vitamin A information
Figure 1 shows that among those who had heard of vitamin A in both the intervention and control districts, health clinics were the major source of information, reported by 81·5 % of the respondents who heard about vitamin A. Other sources were CHW (19·0 %), radio (7·7 %), neighbours (1·8 %), television (1·5 %) and others (9·7 %). Sources reported under ‘others’ included school, community events, IEC materials, church and project field staff.
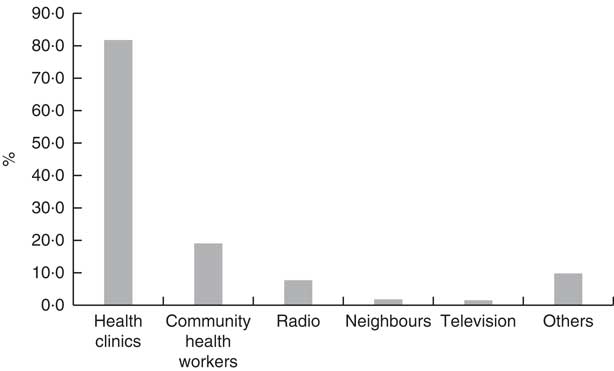
Fig. 1 Sources of vitamin A information among women who had heard of vitamin A in the intervention and control districts of the Masava project conducted in Manyara and Shinyanga regions of Tanzania, February 2016–March 2017 (n 392)
Discussion
To date, to the best of our knowledge, very few studies have evaluated the effectiveness of social marketing interventions in improving consumption of fortified foods based on the TDF. The current intervention, which employed a social marketing framework and addressed twelve out of the fourteen domains of the TDF from an evaluation standpoint, had some influence on KAP regarding consumption of vitamin A-fortified oil after 9 months. At endline, two of the outcome measures were significantly higher in the intervention group v. the control group: knowledge of fortification and actual consumption of adequately fortified oil. Unfortunately, data on knowledge of fortification was not collected in the baseline survey; hence, comparison could not be made on the level of knowledge of fortification in the intervention and control districts before and after the intervention. However, it may be mentioned that although fortification was made mandatory in the country since 2011, it is unlikely that many households in the rural and peri-urban regions where the study was conducted would be aware of fortification, as government campaigns to promote awareness of the fortification logo have not been well funded and this information has not been incorporated into the CHW curriculum. Regarding knowledge at baseline of vitamin A of mothers who were followed up v. not followed up post-intervention, there was no significant difference. Neither were there significant changes in knowledge of vitamin A or using fortified foods to improve vitamin A intake pre- and post-intervention in the intervention districts or when comparing intervention and control groups. Knowledge of the health benefits of vitamin A improved significantly after the intervention in the intervention districts; improvement was, however, also found in the control districts.
The non-significant change in knowledge of vitamin A after the intervention could, in part, be explained by survey fatigue. We found that there were forty-three women who reported knowing about vitamin A at baseline but reported not knowing about it at endline, while fifty-five women reported not knowing about it at baseline and knowing about it at endline. As mentioned earlier, the KAP questionnaire was part of a larger survey that consists of six modules which required about 90 min to complete. As the module on KAP was the last module in the survey, it is possible that some of the respondents, although they knew about vitamin A, reported not knowing about it in order to conclude the survey early. Based on this and the significant improvement in actual consumption of adequately fortified oil, as indicated by the oil retinol content, the social marketing intervention was effective in improving knowledge about and consumption of the fortified sunflower oil.
The results from the current study affirm the findings from several studies on the effectiveness of social marketing in promoting fortified food consumption. In China, Sun et al. ( Reference Sun, Guo and Wang 28 ) found that social marketing through educational activities, newspapers and television, designed based on the 4Ps of the marketing mix (product, price, place and promotion; described in Table 7 ( Reference French, Blair-Stevens and McVey 29 )), significantly improved knowledge, perception and consumption of Fe-fortified soya sauce in rural areas. Another study in Kazakhstan found that a communication campaign consisting of education provided through medical workers, along with social mobilization and marketing activities through television, newspapers, radio, posters and brochures, significantly increased knowledge of the health benefits of Fe-fortified wheat flour and reduced the prevalence of anaemia and Fe deficiency in women and children( Reference Baizhumanova, Nishimura and Ito 30 ). Positive results were also reported in the Philippines, where use of Fe-fortified rice was promoted through social marketing activities involving education in health centres, distribution and display of IEC materials in public areas, and songs based on Fe-fortified rice played when a vehicle delivered the Fe-fortified rice( Reference Angeles-Agdeppa, Saises and Capanzana 31 ).
Table 7 The 4Ps of social marketing( Reference French, Blair-Stevens and McVey 29 )
A wide range of intervention strategies have been used to communicate messages that aimed to promote healthy behaviours. They include educational sessions, group discussions, community activities such as folk dances and road shows, and mass media such as IEC materials, radio, television, newspaper, text messaging and the Internet. The present study found that in Tanzania, health centres and CHW are important sources of health information for women. One of the limitations of the present household survey is that the survey did not examine the effects of the radio show which was implemented only after the endline survey was completed and which is expected to be more far-reaching than the other in-person programmes implemented. The radio show and four additional months of social marketing activities were implemented after the endline survey was completed because, for ethical purposes, the control districts must also be permitted to benefit from the fortified oil sales. It is worth mentioning that in addition to the present household survey, a separate survey on KAP was also conducted by the organization overseeing the social marketing activities before and after 14 months of intervention.Footnote * The latter survey found that female respondents most frequently mentioned hearing the messages from clinic shows and radio, whereas men heard them primarily from the radio, followed by clinic shows and IEC materials. From the results of the two surveys, it might be inferred that health clinics, CHW and radio are the major source of information for women, and radio, health clinics and IEC materials are important for men. This finding, in part, supports that of an earlier study in Kenya, a neighbour to Tanzania, which found that churches, media such as radio and television, and health-care providers are the major sources of information about family planning for women( Reference Naanyu, Baliddawa and Peca 32 ). Our study emphasizes the importance of CHW in reaching and providing health education to women in Africa, providing useful evidence to inform future health communication interventions in Tanzania and East Africa.
Another limitation of our study concerns the validation of the KAP questionnaire. Although the questionnaire was validated for use in francophone countries, it was not validated in translation to Swahili. A third limitation of our present evaluation is that the social marketing intervention did not employ the TDF as a framework for promoting behaviour change in its design and implementation, although the intervention addressed most of the TDF domains from an evaluation standpoint. The KAP questionnaire also was not designed to specifically test changes in the domains of the TDF. However, information on the levels of these domains from the respondents pre- and post-intervention could confirm if these domains were mediators of the observed behaviour change. This information should be collected in future evaluation studies to inform future behaviour change interventions which TDF domains should be prioritized based on the country setting. Our study also did not examine whether households or caregivers simply need to know that a fortified product is better for their families, or whether detail highlighting vitamin A is necessary. To inform future studies and implementation, future research should also assess this question. If detail highlighting of vitamin A adds to an effect, knowledge translation efforts should advocate for enhanced training of CHW as key channels for informed choice, and social marketing messages should be tailored accordingly.
Acknowledgements
Acknowledgments: The authors would like to acknowledge Edna Ndau and Mennonite Economic Development Associates of Canada for carrying out the data collection; Dylan Walters for processing some of the data; and the Tanzania Communication and Development Center for conducting the social marketing intervention. Financial support: The Masava project was supported through a research grant from the International Development Research Centre (IDRC) and Global Affairs Canada (grant number 107790-001). The funding organizations had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: D.C.N.W. performed the statistical analysis, interpreted the data and wrote the paper; K.C. provided the theoretical background of social marketing and critically revised the evaluation from a social marketing perspective; T.C.E.M. and S.H. contributed to the study concept and design; N.S. coordinated the study; S.H. and N.S. revised the accuracy of the information presented in the article; and S.H. and K.C. approved the final version of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Office of Research Ethics of the University of Waterloo (ORE file number 20501) and the National Institute for Medical Research of Tanzania (NIMR/HQ/R.8/VOLIX/1299). Verbal consent was obtained from all subjects. Verbal consent was witnessed and formally recorded.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980018003373









