


In recent years, smartphone technology has emerged as a promising way to collect more accurate dietary intake data than more traditional methods, such as 24 h recalls, through reduced omission of intake and better quantification of portion size( Reference Arab, Estrin and Kim 1 , Reference Wang, Kogashiwa and Ohta 2 ). Using smartphones, participants can easily record intake in real time by using videos or photographs to record images prior to consumption, which can be used to prompt memory during 24 h recalls( Reference Winter and Boushey 3 , Reference Matthiessen, Steinberg and Kaiser 4 ). In particular, videos can provide more details about food and beverage intakes than traditional written-assisted recall methods by utilizing voice annotations to capture information about place, time and estimated amounts, aiding in quantification and reducing omissions during later 24 h recalls( Reference Winter and Boushey 3 , Reference Matthiessen, Steinberg and Kaiser 4 ). Smartphone technology may be particularly useful in China, where the shift in stages of the nutrition transition is rapid, resulting in a rapid shift towards greater away-from-home eating, snacking and intake of an array of sugar-sweetened beverages( Reference Zhai, Du and Wang 5 – Reference Kleiman, Ng and Popkin 7 ), along with a marked increase in a vast array of packaged food purchases( Reference Popkin 8 ), making it increasingly difficult to accurately capture changing intake patterns using traditional recall methods.
In fact, disparities between sugar-sweetened beverage sales and intake from Chinese national nutrition surveys suggest that current methods of assessing dietary intake may not be accurately capturing these emergent food and beverage trends( Reference Kleiman, Ng and Popkin 7 , 9 ). Increases in obesity and related chronic diseases resulting from the way Chinese people eat and move have coincided with the rapid economic development in China( Reference Zhai, Wang and Du 10 – Reference Du, Wang and Zhang 13 ). It is important to develop a more accurate quantification method of food and beverage intakes.
To test whether smartphones provide a more accurate method for estimating dietary intake, we developed a 3 d smartphone-assisted 24 h recall (SA-24R; three continuous days of 24 h recall using voice-annotated video records recorded on a smartphone) method for assessing beverage intake in a sample of 110 Chinese adults in Shanghai in 2013. We compared beverage intake thus obtained with the current method used in the China Health and Nutrition Survey, a 3 d written-assisted 24 h recall (WA-24R; three continuous days of 24 h recall using written record)( Reference Smith, Hua and Seto 14 ). While we found that smartphone-assisted 24 h recalls were more valid as compared with 24 h urine samples relative to written-assisted 24 h recalls, we also found evidence of decreased reporting and consumption of beverages with the 24 h recall. Thus, one key question is whether respondents reduced their consumption or reporting due to difficulty using or dislike of the smartphone method.
Given that smartphone-assisted recall methods have shown increased accuracy in estimating energy and macronutrient intakes compared with traditional 24 h recalls in other populations( Reference Stumbo 15 – Reference Gemming, Doherty and Kelly 18 ), more understanding is needed to evaluate why the smartphone method did not perform better in the Chinese population and how it might be improved in the future. In particular, the present study’s objectives were to utilize additional questionnaire and other data to: (i) examine the acceptability and feasibility of using smartphone technology to assess beverage intake; and (ii) examine whether the feasibility of smartphone use is greater among key sub-populations, including males and females, rural residents and overweight individuals.
Methods
Methodological detail on the beverage validation study has been published previously( Reference Smith, Hua and Seto 14 ). In brief, 120 healthy adult volunteers aged 25–40 years (50 % urban, 50 % rural) were recruited from neighbourhoods in and proximal to Shanghai, China. Seven participants did not complete the study and three did not meet eligibility criteria for age and lack of chronic disease, resulting in a final analytical sample of 110. At the initial visit, trained interviewers administered a demographic survey and measured the height and weight of all participants( Reference Zhang, Zhai and Du 19 ). On two consecutive weeks, participants completed a 3 d SA-24R and a 3 d WA-24R (more detailed information on the study design can be found in the online supplementary material).
Participants were randomized as to the order in which they completed the SA-24R or the WA-24R first. During the SA-24R, participants used a Samsung Galaxy smartphone to take voice-annotated videos of everything they ate and drank, noting the time, location, and estimating amounts of foods and beverages. One set of recalls was conducted during one week and the other in the subsequent week. For both the SA-24R and WA-24R, three consecutive 24 h recalls were conducted. Each recall lasted 3 d (24 h/d).
At the final visit, interviewers administered a questionnaire about the feasibility and acceptability of using the smartphone to record dietary intake. The feasibility questionnaire was developed based on previous feasibility questionnaires for smartphone diet assessment( Reference Arab, Estrin and Kim 1 , Reference Welch, Dowell and Johnson 20 ) and in consultation with a panel of nutrition experts at the Shanghai Center for Disease Control and the University of North Carolina at Chapel Hill. Using a Likert scale, participants were asked to record how much they agreed with fourteen statements. Each statement was give a score of ranging from 1=‘totally disagree’ to 5=‘totally agree’, with 3=‘neither agree nor disagree’.
We further combined the fourteen questions into a total score; when items were negative, we reverse scored so that a higher score reflected a more positive experience with the smartphone (i.e. a 4 or 5 represents agreement or total agreement with a positive statement about the smartphone). We calculated the proportion of respondents who responded favourably (i.e. mean response of 4 or 5 overall or in a specific domain).
We used the SAS statistical software package version 9·2 with statistical significance at two-sided P<0·05. We presented the baseline characteristics for categorical variables. We used the χ 2 test to determine if the proportion of favourable responders differed between sexes, rural v. urban residents and overweight/obese (BMI≥25·0 kg/m2)( 21 ) v. normal-weight participants.
Results
Demographic characteristics of the participants are presented in Table 1.
Table 1 Baseline characteristics of participants in the China beverage validation study: healthy adults (n 110) aged 20–40 years, Shanghai, China, 2013

Acceptability
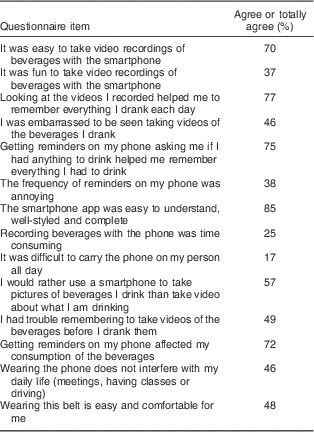
Most participants reported that the phone was acceptable in most aspects, including that videos were easy to use (70 %) and helped with recalls (77 %), ecological momentary assessment (EMA) reminders helped them record intake (75 %) and apps were easy to understand (85 %; Table 2). However, almost half of the participants reported that they had trouble remembering to take videos of the beverages before they consumed them (49 %) or felt embarrassed taking videos in front of other people (46 %). Moreover, most participants (72 %) reported that the EMA reminders affected their consumption.
Table 2 Agreement with items on the China beverage validation study smartphone acceptability questionnaire among healthy adults (n 110) aged 20–40 years, Shanghai, China, 2013
When we assessed overall acceptability of using the smartphone, 72 % of the participants were favourable responders (Table 3).
Table 3 Comparison of favourable responders in the China beverage validation study by overweight status, urbanicity and sex; healthy adults (n 110) aged 20–40 years, Shanghai, China, 2013
* Favourable responders are those who responded 4 or 5 (i.e. ‘agree’ or ‘totally agree’) to positive items, or who responded 1 or 2 (i.e. ‘totally disagree’ or ‘disagree’) for negative items.
† P value of χ 2 test.
‡ Overall acceptability was calculated by combining all the statements together and taking the average of the individual scores; if the average score was equal to 4 or more then the participant was denoted a favourable responder (items were reverse scored if the question was negative question).
Subgroup analysis
There were no statistically significant differences in overall acceptability for overweight v. normal-weight participants or for rural v. urban residents (Table 3). However, we did find that the overall acceptability was slightly but statistically significantly higher for male participants (81 %) than female participants (61 %, P=0·017).
Discussion
To our knowledge, the present study is the first to evaluate the acceptability and feasibility of using smartphones for dietary assessment in a Chinese population. Among a population of 25- to 40-year-old urban and rural residents in Shanghai, China, we found that smartphones were moderately acceptable. Overall, 72 % were favourable responders to the SA-24R.
Looking more closely at different aspects of smartphone acceptability, we found that the majority of participants reported that the phones were fun and the software was easy to use. Additionally, nearly 80 % reported that the phones and the EMA reminders helped them recall beverage intake during the 24 h recall. Overall, these results were consistent with studies evaluating smartphones for collecting dietary intake data in a variety of populations( Reference El-Gayar, Timsina and Nawar 22 – Reference Arab and Winter 26 ). For example, in a study of American diabetes patients, Sevick et al. found 88 % of participants reported that Personal Digital Assistants (a small hand-held system which was used to perform dietary and disease self-monitoring) were a useful tool in monitoring diet and physical activity( Reference Sevick, Zickmund and Korytkowski 16 ).
However, participants also reported that taking videos was time consuming and difficult to remember. These results are similar to those of Arab et al., who found that 71 % of American participants reported a phone-based automated image-capture method somewhat or very burdensome( Reference Arab, Estrin and Kim 1 ). The increased burden of taking videos coupled with the difficulty of remembering to take videos may explain findings from our validation study, in which we found that participants reported consuming fewer beverages on the SA-24R compared with the WA-24R, primarily due to decreased reporting of traditional zero-energy beverages (i.e. water, tea) in the smartphone-assisted method. In addition to the issue of burden, another key concern is that about one-third of the men and over half of the women reported feeling embarrassed taking videos in front of others. The process of displaying, shooting and vocally describing all foods and beverages may be overly burdensome while consuming meals in public. Women in particular may feel especially embarrassed, as cultural norms indicate that they should exhibit more discreet behaviours than men( Reference Croll 27 ).
One option to reduce respondents’ burden and also reduce embarrassment would be to use photographs instead of videos to record foods and beverages to enhance 24 h dietary recalls. Because the participant will still go over each item in detail with an interviewer, the extra detail provided by the voice-annotated video may outweigh perceptions of embarrassment and the time burden imposed by the video. As the majority of respondents indicated that they would have preferred to use photographs instead of videos to document food and beverage intakes, future research should explore whether a smartphone-assisted recall using photographs would provide a more acceptable and more accurate method.
Perhaps more alarming than the increased burden of the SA-24R was that the majority of respondents reported that EMA reminders affected their beverage consumption. These results are not necessarily surprising, considering previous studies have found that the self-consciousness of food intake caused by the process of intentional imaging can dramatically impact normal eating behaviour, usually resulting in decreased food intake relative to usual intake( Reference Wang, Kogashiwa and Ohta 2 , Reference Wang, Kogashiwa and Kira 28 , Reference Kikunaga, Tin and Ishibashi 29 ). A study on using EMA to regulate recommended postoperative eating and activity behaviours in previously obese patients found that EMA did affect the behaviours of eating and physical activity to some extent. EMA prompt the respondents to monitor their food intake, so they consume less( Reference Thomas, Bond and Ryder 30 ). However, if the goal of the diet assessment is to capture usual intake, the consequences of behaviour modification induced by the EMA, or by taking the video record, may outweigh its benefits as a memory enhancer.
Surprisingly, we found that there were no differences in the acceptability of the smartphones between overweight and normal-weight participants. We expected that overweight respondents might report higher difficulty or higher burden with the smartphone because, in our previous study, we found that decreased beverage reporting was greater among overweight participants relative to the normal-weight participants( Reference Smith, Hua and Seto 14 ). We would expect that taking videos of unhealthy beverages like sugar-sweetened beverages would further exacerbate this bias if overweight or obese participants were more embarrassed to show videos of the foods they have consumed, resulting in decreased reporting of sugar-sweetened beverages on the SA-24R relative to the WA-24R. One possibility is that we were not able to fully ascertain potential differences in the acceptability of the SA-24R due to small sample size.
In addition, we found no difference in the number of those reporting difficulties with the phones between urban and rural participants. The main reason might be that the incomes of rural residents are increasing with economic development, and smartphones and other modern technologies are highly prevalent even in rural areas, especially along China’s eastern coast, which tends to be more modernized( Reference Zhai, Du and Wang 5 , Reference Wang and Li 31 , Reference Zhu, Ioannidis and Li 32 ). For example, only four participants from both rural and urban areas had no smartphone experience prior to our study, indicating that this population appeared well prepared to use smartphones to collect dietary data.
However, the study focused only on rural populations close to Shanghai and more work is needed to understand whether rural populations in other parts of the country respond similarly to the smartphone-assisted dietary collection. Another key limitation of the study is that we did not administer the same questionnaire with regard to the written record, which would have provided useful information on whether the moderate acceptability of the smartphone is worse than or on a par with traditional written diet records.
Conclusion
Although respondents did not report difficulty using this methodology, our study did not find smartphone technology helped with dietary assessments in a Chinese population. However, simpler approaches, such as using photographs instead of videos, may be more feasible for enhancing 24 h dietary recalls.
Acknowledgements
Acknowledgements: The authors thank the staff at the Shanghai Municipal Center for Disease Control and Prevention (SCDC), the Songjiang Center for Disease Control and Prevention (CDC) and the Putuo district CDC and Community Health Center for their help in the data design and collection process. Financial support: This study was supported by the Carolina Population Center (grant number 5 R24 HD050924) of the University of North Carolina at Chapel Hill; the National Institutes of Health (NIH; grant numbers R01-HD30880, DK056350, R24 HD050924 and R01-HD38700); the Fogarty International Center, NIH (grant number 5 D43 TW009077); the China Health Fields Specific Research Grant (grant number 201202012); and research grants of the Shanghai Municipal Bureau of Health (number 20134053) and the Shanghai Yangfan Talented Person Plan Grant (number 2015111). The funders had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: J.Z. and J.S. contributed equally to this work. J.Z., J.S. and S.Z. designed the study and wrote the manuscript; Z.W. C.Y., J.M., C.H. and Z.Z. collected the data; L.P.S., S.D. and J.H. analysed the data; E.S. and B.M.P. reviewed the manuscript drafts. Ethics of human subject participation: This study was approved by the ethics committee of both the University of North Carolina at Chapel Hill and the Shanghai Municipal Center for Disease Control and Prevention.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1368980015000907





