


Stroke is one of the leading causes of disabilities and death in both developed and developing countries. For example, stroke was the leading cause of death in China in 2010 (1·7 million deaths)( Reference Yang, Wang and Zeng 1 ). Due to population ageing, stroke, which consumes substantial health resources and leads to a significant economic burden, will become a tremendous burden to the health system in future decades( Reference Meschia, Bushnell and Boden-Albala 2 ). However, stroke has a profound impact not only on the government but also on individuals and their families. Therefore, it is imperative to develop prevention strategies that might reduce the risk of stroke.
Diet is one of the key lifestyle factors involved in the prevention of stroke. Recently, extensive epidemiological studies have focused on the relationship among nutrients, food groups, dietary patterns and stroke. For the general public, specific nutrition is too specialized to understand. Further, changing dietary patterns is also difficult for individuals. Compared with nutrients and dietary patterns, because food groups are more easily understood by and acceptable to the public, the targeted aim of the present overview was food groups. It has been shown that some specific foods are related to the risk of stroke, such as vegetables and fruits( Reference Hu, Huang and Wang 3 ), meat( Reference Kaluza, Wolk and Larsson 4 ) and fish( Reference Xun, Qin and Song 5 ). Summarizing the evidence on the impact of diet at the food level will provide greater insights into the role of food groups in stroke.
An overview of systematic reviews is a relatively new approach to synthesizing a large body of literature in a particular area. Numerous systematic reviews of prospective studies regarding food groups associated with stroke have been published( Reference Zhang, Xu and Wei 6 – Reference Hu, Huang and Wang 8 ). Systematic reviews of prospective studies are considered to provide a high level of evidence and represent a potentially powerful method to evaluate the long-term effects of food groups on stroke risk. Patients and researchers require such evidence to support shared decisions and to set priorities for research. Clinicians and policy makers also require information from systematic reviews to inform clinical practice and policy( Reference Sherzai, Heim and Boothby 9 ). However, to date, there has been no effort to summarize the evidence from these systematic reviews and meta-analyses. As the first review of the evidence across existing systematic reviews of prospective studies, the present study provides an overview of the range and validity of the reported associations of food groups with stroke.
Methods
Literature search
The present systematic review was guided by the PRISMA Statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)( Reference Moher, Liberati and Tetzlaff 10 ). A systematic literature search was conducted in the PubMed, EMBASE and Cochrane Library databases up to September 2015. Search terms included ‘food’, ‘diet’, ‘nutrition’, or one specific food such as ‘nut’, ‘legume’, ‘fruit’, ‘vegetable’, ‘fish’, ‘meat’, ‘egg’ and others, combined with ‘stroke’, ‘cerebral vascular disease’, ‘cerebral infarction’ and ‘systematic review’ and ‘meta-analysis’. These searches included a mixture of MeSH (Medical Subject Headings) terms and text words to attempt to maximize the retrieval of potentially relevant studies (see online supplementary material for the search strategy and terms used). The reference lists of the retrieved articles were also reviewed.
Study selection
The eligibility criteria for including reviews in our overview were that the target review was itself a systematic review or meta-analysis of prospective studies and that it included studies investigating the relationship between a specific food or food groups and stroke outcome (including risk of stroke or stroke mortality). Studies in which CVD outcomes were assessed cumulatively rather than by individual disease risk assessment were not included. When more than one meta-analysis on the same research question was eligible and when the method of these systematic reviews or meta-analyses was similar, the study with the largest number of component studies with data on the individual studies’ effect sizes was retained for the main analysis. When one systematic review or meta-analysis was an updated review of a previous review, we reported the results of the updated study only. Narrative, non-systematic reviews and editorials/commentaries were not eligible for this overview.
Data extraction
The following data were extracted from the selected studies using a standardized data-collection form: the name of the first author; publication year; targeted food; number of included studies; population size; case numbers; and conclusions of the meta-analysis. Two independent reviewers (C.D. and Q.L.) conducted the literature search, study selection and data extraction, removing duplicates or ineligible reviews before proceeding to full-text screening of the eligible articles. Consensus was reached through a third researcher’s opinion (Y.Z.).
Quality assessment
The quality of the studies was assessed by two raters according to the AMSTAR (Assessment of Multiple Systematic Reviews) validated scale. The AMSTAR provides a risk of bias assessment across eleven different domains. The AMSTAR items are scored as ‘yes’, ‘no’, ‘can’t answer’ or ‘not applicable’. It has been shown to be adequately valid and reliable for use in assessing systematic reviews( Reference Shea, Hamel and Wells 11 ). The quality of the studies was categorized as follows according to the number of criteria that were met: excellent, 11; very good, 9 or 10; good, 7 or 8; acceptable, 5 or 6; and deficient, 0 to 4. The AMSTAR criteria include the following:
-
1. a priori design provided;
-
2. duplicate study selection/data extraction;
-
3. comprehensive literature search;
-
4. status of publication as inclusion criterion;
-
5. list of studies (included/excluded) provided;
-
6. characteristics of included studies documented;
-
7. scientific quality assessed and documented;
-
8. appropriate formulation of conclusions;
-
9. appropriate methods of combining studies;
-
10. assessment of publication bias; and
-
11. conflict of interest statement.
Data synthesis
The characteristics of the systematic reviews and statistical pooling of the included articles were summarized descriptively. Evidence tables were produced to synthesize the clinical findings and recommendations of the systematic reviews.
Results
Description of the included studies
The literature search identified 1027 relevant reviews. After duplicates were removed, 926 reviews remained for analysis (479 from PubMed, 401 from EMBASE and forty-six from the Cochrane Library). After screening of the abstracts, 108 reviews were retrieved as full text. In all, fifty-three reviews were identified as potential studies for inclusion in the overview. Ultimately, eighteen reviews fulfilled the inclusion criteria and were included in the overview, all of which were published between 2008 and 2015 (Fig. 1).
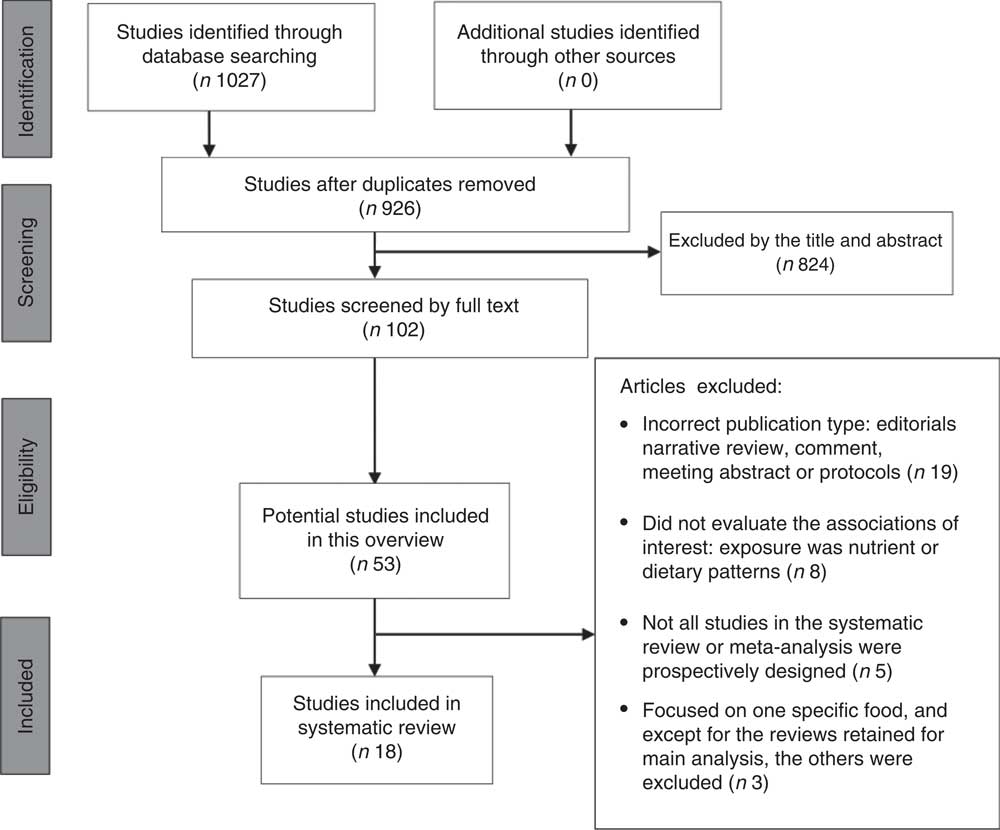
Fig. 1 Flow diagram of study selection for the present overview of systematic reviews and meta analyses on the reported associations of food groups with stroke risk
The characteristics and results of the included reviews are presented in Table 1. The reviews examined the following topics: nuts, legumes, fruits and vegetables, refined grains, whole grains, dairy products, eggs, chocolate, red and/or processed meat, fish, tea, sugar-sweetened beverages and coffee. Regarding the quality of the included reviews, eight were at the ‘very good’ level, six reviews were at the ‘good’ level, and four of the reviews were at the ‘acceptable’ level (Table 2).
Table 1 Characteristics of the systematic reviews on the reported associations of food groups with stroke risk included in the present overview

SSB, sugar-sweetened beverage; NR, not reported.
Table 2 Quality of the systematic reviews on the reported associations of food groups with stroke risk included in the present overview

AMSTAR, Assessment of Multiple Systematic Reviews; Y, yes; N, no, NA, not applicable; C, can’t answer.
Nuts
Two reviews reported on the relationship between nuts and risk of stroke or stroke mortality( Reference Zhang, Xu and Wei 6 , Reference Shi, Tang and Wu 12 ). The method and conclusion of Shi et al.’s( Reference Shi, Tang and Wu 12 ) review were similar to those of Zhang et al.( Reference Zhang, Xu and Wei 6 ); however, because the number of participants included was less than that of Zhang et al.’s, we only reported the results of the Zhang et al. review.
Zhang et al.( Reference Zhang, Xu and Wei 6 ) searched PubMed and EMBASE and reviewed the references of the retrieved articles. Nine prospective studies published from 2000 to 2013 and consisting of 476 181 participants were included in their meta-analysis. Comparing the highest with the lowest nut consumption, the highest nut consumption was associated with a 10 % lower risk of stroke (relative risk (RR)=0·90; 95 % CI 0·83, 0·98). Gender modified the effects of nut consumption with a significant inverse association observed for women (RR=0·88; 95 % CI 0·78, 0·98). Furthermore, although it did not reach significance, they observed a trend towards an inverse association between higher nut consumption and stroke mortality (RR=0·86; 95 % CI 0·69, 1·06).
Legumes
One review reported on the relationship between legumes and stroke risk. Shi et al.( Reference Shi, Tang and Wu 12 ) searched MEDLINE and EMBASE up to January 2014. Six prospective studies published between 2000 and 2012 that included 173 229 participants and 4030 stroke events were identified. The pooled results showed that a diet containing greater amounts of legumes might not be associated with a lower risk of stroke. Comparing the highest v. the lowest level of dietary legume intake, the pooled RR of stroke was 0·95 (95 % CI 0·84, 1·08).
Fruits and vegetables
Three reviews reported on the relationship between fruits and vegetables and stroke risk( Reference Hu, Huang and Wang 3 , Reference He, Nowson and MacGregor 13 , Reference Dauchet, Amouyel and Dallongeville 14 ). Among these three reviews, because Hu et al.’s( Reference Hu, Huang and Wang 3 ) review had the largest number of component studies with data on individual studies’ effect sizes, we reported their results only. Hu et al. searched the PubMed (1947 to January 2014) and EMBASE (1974 to January 2014) databases. Twenty prospective studies, consisting of 760 629 participants with 16 981 stroke events, were included in that meta-analysis. Comparing the highest with the lowest category of total fruit and vegetable consumption, the highest category of total fruit and vegetable consumption was associated with a 21 % lower risk of stroke (RR=0·79; 95 % CI 0·75, 0·84); moreover, fruit consumption was associated with a 23 % lower risk of stroke (RR=0·77; 95 % CI 0·71, 0·84) and vegetable consumption was associated with a 14 % lower risk of stroke (RR=0·86; 95 % CI 0·79, 0·93). The linear dose–response relationship showed that the risk of stroke decreased by 32 % (RR=0·68; 95 % CI 0·56, 0·82) and 11 % (RR=0·89; 95 % CI 0·81, 0·98) for every 200 g/d increment in fruit consumption and vegetable consumption, respectively.
Refined grains
One review reported on the relationship between refined grains and risk of stroke. Wu et al.( Reference Wu, Guan and Lv 15 ) searched the MEDLINE (from 1 January 1966) and EMBASE (from 1 January 1974) databases up to 30 November 2014. Eight prospective studies consisting of 410 821 subjects with 8284 stroke cases were included in the meta-analysis. The pooled results showed that a diet containing greater amounts of refined grains was not associated with risk of stroke (RR=1·02; 95 % CI 0·93, 1·10). In the subgroup analysis, no significant associations between the consumption of refined grains and risk of stroke were found for both women and men, for both haemorrhagic and ischaemic strokes, and for both incident and fatal strokes. Consumption of white rice was not associated with risk of stroke (RR=1·01; 95 % CI 0·93, 1·11). For those consuming 3 servings rice/d, the pooled results showed no significant association between refined grain consumption and total stroke (RR=0·98; 95 % CI 0·73, 1·03).
Whole grains
One review reported on the relationship between whole grains and risk of CVD. The results for stroke were extracted. Mellen et al.( Reference Mellen, Walsh and Herrington 16 ) searched MEDLINE from 1966 to April 2006. In the analysis of four studies, greater whole grain intake (2·5 servings/d v. 0·2 servings/d) was not associated with stroke risk (RR=0·83; 95 % CI 0·69, 1·02).
Dairy products
Two reviews reported on the relationship between dairy products and risk of stroke( Reference Hu, Huang and Wang 8 , Reference Qin, Xu and Han 17 ). Qin et al.( Reference Qin, Xu and Han 17 ) investigated the association between dairy products and the risk of major cardiovascular events. The results from patients with stroke were extracted. They searched the PubMed, EMBASE and Cochrane Library databases up to February 2014. Twenty studies (twelve in stroke) published between 1997 and 2013 and consisting of 504 803 participants with 21 801 stroke cases were included in the meta-analysis. Dairy consumption reduced the risk of stroke by 13 % (RR=0·87; 95 % CI 0·77, 0·99). In the subgroup analysis, stroke risk was reduced by the consumption of low-fat dairy (RR=0·93; 95 % CI 0·88, 0·99) and cheese (RR=0·91; 95 % CI 0·84, 0·98).
Hu et al.( Reference Hu, Huang and Wang 8 ) searched EMBASE (1950 to November 2013), Web of Knowledge (1950 to November 2013) and PubMed (1945 to November 2013). Eighteen separate results from fifteen prospective cohort studies consisting of 764 635 participants with 28 138 stroke events were included in their meta-analysis. Total dairy (RR=0·88; 95 % CI 0·82, 0·94), low-fat dairy (RR=0·91; 95 % CI 0·85, 0·97), fermented milk (RR=0·80; 95 % CI 0·71, 089) and cheese (RR=0·94, 95 % CI 0·89, 0·99) were significantly associated with reduced risk of stroke, whereas whole/high-fat dairy, non-fermented milk, butter and cream were not significantly associated with risk of stroke. No significant association with either ischaemic or haemorrhagic stroke was observed due to limited data. A non-linear dose–response relationship between milk and risk of stroke was found, and the RR (95 % CI) of stroke was 0·88 (0·86, 0·91), 0·82 (0·79, 0·86), 0·83 (0·79, 0·86), 0·85 (0·81, 0·89), 0·86 (0·82, 0·91), 0·91 (0·84, 0·98) and 0·94 (0·86, 1·02) for 100, 200, 300, 400, 500, 600 and 700 ml milk/d, respectively (Fig. 2; extracted from the original review).
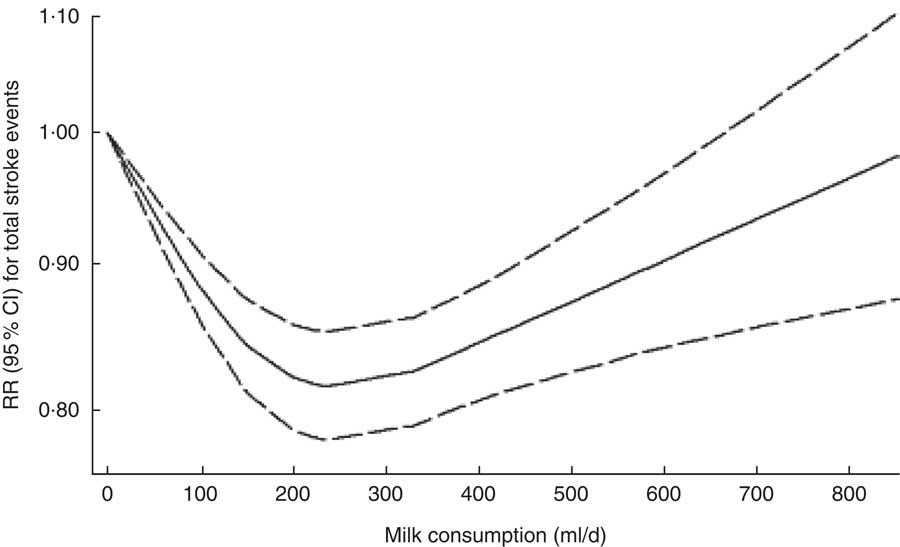
Fig. 2 Dose–response analysis between milk consumption and total stroke events; relative risk (RR; ————) and 95 % CI (— — — —). (From Hu et al.( Reference Hu, Huang and Wang 8 ))
Eggs
One review reported on the relationship between eggs and risk of stroke. Rong et al.( Reference Rong, Chen and Zhu 18 ) searched PubMed and EMBASE from January 1966 through June 2012. Six articles with eight reports consisting of 210 404 patients with 7579 incident cases for stroke were included in their review. They did not observe a curvilinear association between egg consumption and risk of stroke. The pooled RR for increased consumption of 1 egg/d was 0·91 (95 % CI 0·81, 1·02). Higher intake of eggs (up to 1 egg/d) was not associated with risk of stroke. However, those with higher egg consumption had a 25 % lower risk of developing haemorrhagic stroke (RR=0·75; 95 % CI 0·57, 0·99).
Chocolate
One review reported on the relationship between chocolate and risk of stroke. Larsson et al.( Reference Larsson, Virtamo and Wolk 19 ) searched the PubMed and EMBASE databases through 13 January 2012. Five studies consisting of 131 345 participants with 4260 stroke cases were included in their meta-analysis. Comparing the highest v. the lowest category of chocolate consumption, the highest chocolate consumption was associated with a 19 % lower risk of stroke (RR=0·81; 95 % CI 0·73, 0·90). A 50 g/week increment in chocolate consumption was associated with a 14 % lower risk of stroke (RR=0·86; 95 % CI 0·76, 0·97).
Red and processed meat
Two reviews reported on the relationship between red and processed meat and risk of stroke( Reference Kaluza, Wolk and Larsson 4 , Reference Chen, Lv and Pang 20 ). Chen et al.( Reference Chen, Lv and Pang 20 ) performed a literature search in the PubMed database through June 2012. Five studies consisting of 239 251 subjects with 9593 stroke events were identified. Comparing the highest category of consumption with the lowest category, the highest categories of total meat (red and processed meat combined) consumption, red meat consumption and processed meat consumption were associated with a 15 % (RR=1·15; 95 % CI 1·05, 1·25), 9 % (RR=1·09; 95 % CI 1·01, 1·18) and 14 % (RR=1·14; 95 % CI 1·05, 1·25) higher risk of total stroke, respectively. The pooled RR of ischaemic stroke (highest v. lowest quintile) was 1·15 (95 % CI 1·04, 1·28), 1·13 (95 % CI 1·01, 1·25) and 1·19 (95 % CI 1·08, 1·31), respectively. Consumption of red and/or processed meat was not associated with haemorrhagic stroke. In the dose–response analysis, the risk of stroke increased significantly by 10 and 13 % for each 100 g/d increment in total and red meat consumption, respectively, and by 11 % for each 50 g/d increment in processed meat consumption.
Kaluza et al.( Reference Kaluza, Wolk and Larsson 4 ) searched the PubMed database through 26 May 2012. Five articles including the results from six prospective studies published between 2003 and 2012 and consisting of 329 495 participants with 10 630 stroke cases were included in their meta-analysis. Increased consumption of 1 serving/d for fresh red meat, processed meat and total red meat was associated with 11 % (RR=1·11; 95 % CI 1·03, 1·20), 13 % (RR=1·13 95 % CI 1·03, 1·24) and 11 % (RR=1·11; 95 % CI 1·06, 1·16) higher risk of total stroke, respectively. In the subgroup analysis, the risk of ischaemic stroke was positively associated with the consumption of fresh red meat (RR=1·13; 95 % CI 1·00, 1·27), processed meat (RR=1·15; 95 % CI 1·06, 1·24) and total red meat (RR=1·12; 95 % CI 1·05, 1·19); no significant associations were observed for haemorrhagic stroke.
Fish
Three reviews reported on the relationship between fish and risk of stroke( Reference Xun, Qin and Song 5 , Reference He, Song and Daviglus 21 , Reference Larsson and Orsini 22 ). Among these three reviews, Xun et al.’s( Reference Xun, Qin and Song 5 ) had the largest number of component studies with data on the individual studies’ effect sizes; thus, we reported its results only. They searched MEDLINE and EMBASE through April 2012 and reviewed the reference lists of the relevant articles or retrieved additional information through Google. Sixteen eligible studies (nineteen cohorts), consisting of 402 127 individuals with 10 568 incident cases, were included in their meta-analysis. Compared with those who never consumed fish or those who ate <1 fish serving/month, those who consumed 1 fish serving/week, 2–4 fish servings/week and ≥5 fish servings/week had a 14 % (hazard ratio (HR)=0·86; 95 % CI 0·80, 0·93), 9 % (HR=0·91; 95 % CI 0·85, 0·98) and 13 % (HR=0·87; 95 % CI 0·79, 0·96), respectively, lower risk of stroke. In the subgroup analysis, an inverse association between fish intake and stroke incidence was found only by those studies conducted in North America.
Tea
Two reviewers reported on the relationship between tea consumption and risk of stroke or stroke mortality( Reference Zhang, Qin and Wei 23 , Reference Shen, Song and Ma 24 ) . Zhang et al.( Reference Zhang, Qin and Wei 23 ) investigated the association between tea consumption and the risk of major CVD. The results from patients with stroke were extracted. They searched the PubMed, EMBASE and Cochrane Library electronic databases up to July 2014. Twenty-four studies (stroke in eight studies, stroke mortality in five studies) with 10 572 cases of stroke and 2350 stroke deaths among 856 206 individuals were included in their meta-analysis. According to high v. low tea consumption, high tea consumption was associated with a 23 % lower risk of stroke (RR=0·67; 95 % CI 0·53, 0·85) and a 22 % lower risk of cerebral infarction (RR=0·78; 95 % CI 0·67, 0·92), but not with any reduction in stroke mortality, intracerebral haemorrhage or subarachnoid haemorrhage. The dose–response analysis indicated that an increase in tea consumption by 3 cups/d was associated with an 18 % lower risk of stroke (RR=0·82; 95 % CI 0·73, 0·92), a 16 % lower risk of cerebral infarction (RR=0·84; 95 % CI 0·72, 0·98) and an 11 % lower risk of intracerebral haemorrhage (RR=0·79; 95 % CI 0·72, 0·87), albeit with little or no effect on stroke mortality (RR=0·93; 95 % CI 0·83, 1·05). In the subgroup analysis, they found that an increase of 3 cups tea/d was associated with a reduced risk of stroke if the participants were men, Asian, or if they consumed green tea.
Shen et al.( Reference Shen, Song and Ma 24 ) searched the PubMed database from January 1966 to March 2012 and reviewed the reference lists of the retrieved articles to identify relevant studies. Fourteen studies consisting of 513 804 participants with 10 192 stroke cases were included in their meta-analysis. An increase of 3 cups/d in tea consumption was associated with a 13 % lower risk of stroke (RR=0·87; 95 % CI 0·81, 0·94). Tea consumption was also associated with a 24 % lower risk of ischaemic stroke (RR=0·76; 95 % CI 0·69, 0·84) but not with cerebral haemorrhage or subarachnoid haemorrhage.
Sugar-sweetened beverages
One review reported on the relationship between sugar-sweetened beverages (SSB) and risk of stroke. Xi et al.( Reference Xi, Huang and Reilly 25 ) investigated the relationship between SSB and risk of hypertension and CVD. The results from patients with stroke were extracted. They searched the PubMed and EMBASE databases up to 5 May 2014. Four prospective studies consisting of 259 176 participants with 10 011 incident cases of stroke were included in their meta-analysis. For every 1 serving/d increase in SSB consumption, the pooled results showed that no significant association existed between SSB consumption and total stroke (RR=1·06; 95 % CI 0·97, 1·15) Compared with the lowest level, the highest intake level of SSB was marginally associated with the overall risk of stroke (RR=1·10; 95 % CI 1·00, 1·20). In the subgroup analysis, they found no significant associations between SSB intake and the risk of either ischaemic stroke or haemorrhagic stroke. However, SSB intake was associated with a higher risk of stroke in Caucasians (RR=1·17; 95 % CI 1·06, 1·28), although not in East Asians.
Coffee
Three reviews reported on the relationship between coffee and stroke( Reference Zhang, Wang and Song 7 , Reference Ding, Bhupathiraju and Satija 26 , Reference Larsson and Orsini 27 ). Ding et al.( Reference Ding, Bhupathiraju and Satija 26 ) performed a meta-analysis to assess the dose–response relationship between long-term coffee consumption and risk of CVD. The results from patients with stroke were extracted. They searched the PubMed and EMBASE databases from January 1966 to March 2013. Thirty-six studies (seventeen studies on stroke) consisting of 1 283 685 study participants with 2030 stroke cases were included. The categories of coffee consumption in their review were defined as follows: the lowest category (median and mean coffee consumption=0 cups/d), the third highest (median=1·5 cups/d; mean=1·48 cups/d), the second highest (median=3·5 cups/d; mean=3 cups/d) and the highest category (median=5 cups/d; mean=5·5 cups/d). Compared with the lowest category of coffee consumption, the corresponding RR of stroke was 0·89 (95 % CI 0·84, 0·94) for the third highest category, 0·80 (95 % CI 0·75, 0·86) for the second highest category and 0·95 (95 % CI 0·84, 1·07) for the highest category. Additionally, they found that coffee consumption was non-linearly associated with stroke risk (Fig. 3; extracted from the original article).
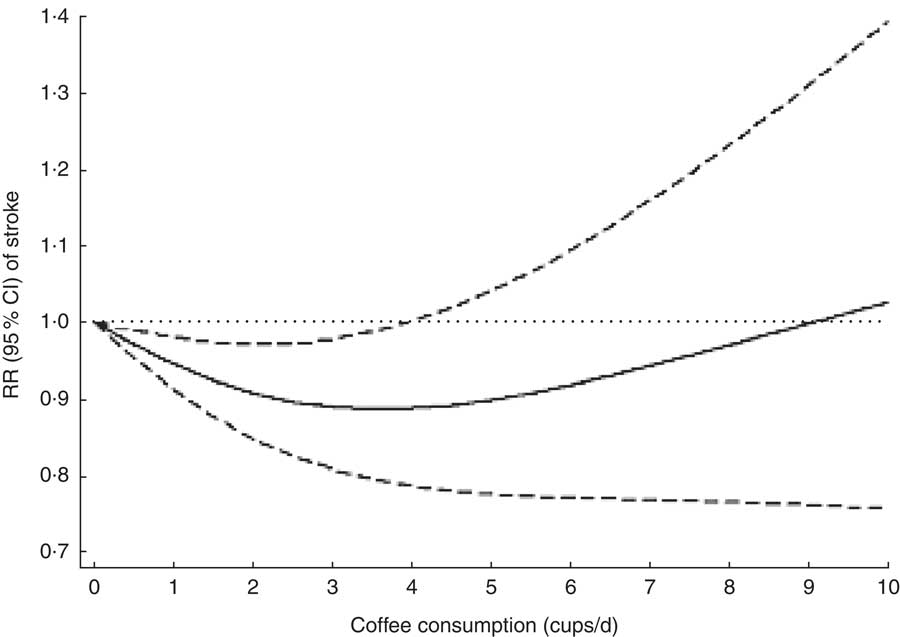
Fig. 3 Coffee consumption and risk of stroke; relative risk (RR; ————) and 95 % CI (— — — —); · · · · · represents no effect; P for heterogeneity=0·007, P for trend <0·001, P for non-linearity <0·001. (From Ding et al.( Reference Ding, Bhupathiraju and Satija 26 ))
Zhang et al.( Reference Zhang, Wang and Song 7 ) searched PubMed and EMBASE up to June 2011. Thirteen studies consisting of 492 760 individuals with 12 414 stroke cases were included in their meta-analysis. They combined coffee consumption of less than 1 cup/week and no coffee consumption into the non-coffee consumption group. Coffee consumption of more than 1 cup/d was further classified into three categories: (i) light consumption: >1 cup/week but ≤1 cup/d in the US and Asian studies and >1 cup/week but ≤2 cups/d in the European studies; (ii) moderate consumption: 1–3 cups/d in the US and Asian studies and 3–4 cups/d in the European studies; and (iii) heavy consumption: ≥4 cups/d in the US and Asian studies and ≥5 cups/d in the European studies. Compared with non-coffee drinking, all coffee consumption reduced total stroke risk by 11 % (RR=0·89; 95 % CI 0·81, 0·97). Coffee consumption reduced stroke risk by 17 % (RR=0·83; 95 % CI 0·79, 0·87) among females. Although lacking significance for men, coffee consumption tended to decrease stroke risk (RR=0·88; 95 % CI 0·72, 1·09). Light, moderate and heavy coffee consumption reduced all-type stroke risk by 10 % (RR=0·90; 95 % CI 0·85, 0·96), 14 % (RR=0·86; 95 % CI 0·76, 0·97) and 17 % (RR=0·83; 95 % CI 0·78, 0·89), respectively.
Larsson and Orsini( Reference Larsson and Orsini 27 ) searched PubMed and EMBASE from January 1966 through May 2011. Eleven studies consisting of 479 689 participants with 10 003 stroke cases were included in their meta-analysis. In their review, coffee consumption was classified into five groups: reference (the lowest category in each study), <3 cups/d, 3–5 cups/d, 5–7 cups/d and >7 cups/d. Compared with no coffee consumption, 2 cups coffee/d reduced stroke risk by 14 % (RR=0·86; 95 % CI 0·78, 0·94), 3–4 cups/d reduced risk of stroke by 17 % (RR=0·83; 95 % CI 0·74, 0·92) and 6 cups/d reduced risk of stroke by 13 % (RR=0·87; 95 % CI 0·77, 0·97), with no significant difference observed between 8 cups/d and stroke risk. The results demonstrated that a non-linear association existed between coffee consumption and risk of stroke (Fig. 4; extracted from the original article). The findings from that meta-analysis indicated that moderate coffee consumption might be weakly inversely associated with stroke risk.

Fig. 4 Adjusted relative risk of stroke associated with coffee consumption in a meta-analysis of published studies, 1966–2011; relative risk (RR; ————) and 95 % CI (— — — —); · · · · · represents no effect. (From Larsson and Orsini( Reference Larsson and Orsini 27 ))
Discussion
We have provided an overview of systematic reviews and meta-analyses relating to a specific food or to food groups that have been associated with stroke outcome. Our overview synthesized the evidence from eighteen reviews. The quality of these systematic reviews or meta-analyses is generally good. Overall, thirteen specific foods were studied for an association with stroke outcome, including nuts, legumes, fruits and vegetables, refined grains, whole grains, dairy products, eggs, chocolate, red and/or processed meat, fish, tea, SSB and coffee. While high consumption of nuts, fruits, vegetables, dairy foods, fish and tea, and moderate consumption of coffee and chocolate demonstrated a protective effect, high consumption of red and/or processed meat was associated with increased stroke risk. Refined grain, SSB, legume, egg and whole grain intake showed no effect on stroke outcome.
There are some common characteristics and nutrition factors for protective foods, which are described as follows. Nuts contain mostly unsaturated fats, which have beneficial effects on blood lipids( Reference Grundy and Denke 28 ). Moreover, nuts are rich in arginine. Arginine is the precursor of nitric oxide, which is an effective vasodilator and may inhibit platelet aggregation and adhesion. Additionally, nuts are rich sources of K, Mg, folate and fibre, and meta-analyses have shown that supplementation with K alone or in combination with other minerals such as Mg and Ca resulted in a reduction in blood pressure( Reference Beyer, Dickinson and Nicolson 29 ). Folate is a crucial regulator of the metabolism of homocysteine, and studies have indicated that dietary supplementation with folate reduced blood levels of homocysteine and was inversely related to the risk of stroke( Reference Wang, Qin and Demirtas 30 ). Studies have also suggested that higher dietary fibre and protein intake might lower blood pressure and were associated with a reduced risk for stroke( Reference Streppel, Arends and van ’t Veer 31 , Reference Zhang, Xu and Liu 32 ).
Complex mechanisms might explain the protective effects of fruits and vegetables on stroke. Studies have shown that increased fruit and vegetable consumption might lower blood pressure, improve microvascular function and have favourable effects on other cardiovascular risk factors, such as those observed for BMI, waist circumference, total cholesterol, LDL cholesterol, inflammation and oxidative stress( Reference Hu, Huang and Wang 3 ). Fruits and vegetables are rich sources of K, folate, antioxidants (e.g. vitamin C, β-carotene, flavonoids) and fibre, which were significantly associated with decreased stroke risk( Reference Dauchet, Amouyel and Dallongeville 14 ).
Several biological mechanisms may be involved in the potentially protective effects of dairy products against CVD. Dairy products are rich in minerals (Ca, K and Mg), protein (casein and whey) and vitamins (riboflavin and vitamin B12). Such components showed beneficial effects on CVD incidence. However, the underlying mechanisms of the effects of dairy products on stroke remain unknown( Reference Hu, Huang and Wang 8 ).
The reason why fish has beneficial attributes in lowering the risk of stroke may be attributed to the antithrombotic activity and anti-inflammatory property of long-chain n-3 PUFA, the key nutrients in fish( Reference He 33 , Reference Calder 34 ). Such marine-derived long-chain n-3 PUFA have been shown to have multiple favourable effects on blood pressure, arrhythmias, lipid profile, platelet aggregation and endothelial function that might reduce the risk of ischaemic stroke( Reference He, Song and Daviglus 21 ).
The beneficial effect of tea consumption on stroke risk has been suggested to be attributable to the presence of polyphenolic compounds, particularly catechins, in green and black tea. Catechins, a major category of polyphenols in tea, exert a wide spectrum of beneficial effects against CVD, including antioxidative, anti-inflammatory, anti-endothelial dysfunction, antihypertensive and lipid-lowering effects( Reference Shen, Song and Ma 24 , Reference Babu and Liu 35 ).
Coffee is a complex mixture of biologically active substances that may have both beneficial and harmful effects on the cardiovascular system. The phenolic compounds in coffee, such as caffeic, ferulic and p-coumaric acids, have strong antioxidant activity and may reduce the oxidation of LDL cholesterol( Reference Larsson and Orsini 27 ). Additionally, habitual coffee consumption has been associated with higher insulin sensitivity, and several studies have found an inverse association between coffee consumption and blood concentrations of some inflammatory markers. Alternatively, caffeine in coffee may increase blood pressure and levels of plasma homocysteine. The non-linear U-shaped relationship between coffee consumption and risk of stroke might be due to a combination of beneficial and detrimental effects.
Chocolate is a source of flavonoids and is particularly rich in epicatechin, catechin and procyanidins (polymers of catechins and epicatechins). The flavonoids may reduce the risk of stroke through several biological mechanisms, including antioxidant, antiplatelet and anti-inflammatory effects, as well as by lowering blood pressure, increasing HDL cholesterol and improving endothelial function( Reference Natsume, Osakabe and Yamagishi 36 ). Chocolate also contains caffeine, and the consumption of coffee, which is a rich source of caffeine, has been inversely associated with risk of stroke( Reference Zhang, Wang and Song 7 ).
Foroughi et al.( Reference Foroughi, Akhavanzanjani and Maghsoudi 37 ) and Sherzai et al.( Reference Sherzai, Heim and Boothby 9 ) summarized the evidence regarding the relationship between nutrition and stroke outcome. However, the type of studies included in their reviews was not limited. Mixed results were demonstrated. Compared with previous reviews of nutrition and stroke, our overview is robust because only systematic reviews and meta-analyses of prospective observational studies were included, which might eliminate selection and recall bias. In addition, the systematic reviews and meta-analyses included in our overview have relatively large sample sizes and long periods of follow-up. The findings from our study are informative because they provide a high-evidence overview of food groups associated with stroke outcome, which researchers and clinicians may use as a basis for strong practice recommendations.
Our overview has some limitations. Because all original studies in the systematic reviews or meta-analyses included in our overview followed an observational design, the possibility that other factors might account for the observed results could not be eliminated. Additionally, most original studies used FFQ to evaluate the levels of food consumption, and measurement error was inevitable. Furthermore, the cut-off values for the food consumption categories were not consistent among the studies. These limitations might have contributed to heterogeneity in the pooled analysis. One cannot conclude convincingly from those data that increasing consumption of some types of foods has a protective effect against stroke outcomes. Future studies should use uniform criteria for food consumption. Dietary patterns differed in different populations, and habitual consumption of foods also differed. For example, green tea consumption is more popular in Asian than in Western countries. However, analyses stratified by ethnicity were not available in most of the systematic reviews included in our overview, which might play an important role in the relationship between food consumption and stroke outcome. Finally, the findings from reviews receiving lower quality ratings and those of small size must be interpreted with caution.
Conclusion
The present study is the first overview of systematic reviews that brings together the evidence relating to food groups associated with stroke outcome. It shows that the quality of these systematic reviews is generally good. Overall, thirteen specific foods have been studied for an association with stroke outcome. Whereas a high consumption of nuts, fruits, vegetables, dairy foods, fish and tea, and moderate consumption of coffee and chocolate demonstrated a protective effect, a high consumption of red and/or processed meat was associated with increased stroke risk. Refined grain, SSB, legume, egg and whole grain intake showed no effect on stroke outcome. Although the current overview provides powerful evidence on food groups associated with stroke risk, its findings require further confirmation by well-designed large randomized clinical trials.
Acknowledgements
Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: The authors declare that they have no conflicts of interest. Authorship: C.D. and Q.L. contributed equally to this work. C.D. and Q.L. designed the study; C.D. and Q.L. searched the databases, checked them according to the eligibility and exclusion criteria and analysed the data; B.G., L.L. and L.C. assisted C.D. and Q.L. in data collection and statistical analysis. C.D. wrote the draft of the paper; C.D., Q.L., B.G., L.L., L.C., Y.Z. and L.F. revised the paper. Y.Z. and L.F. were responsible for the final content. All the authors read and approved the final manuscript. Ethics of human subject participation: Not applicable.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980017003093








