


The prevalence of overweight and obesity is rising in all countries(Reference Yoon, Lee and Kim1–Reference Fezeu, Assah and Balkau4), including Germany(5, Reference Mensink, Lampert and Bergmann6). The WHO has declared overweight as one of the top ten risk conditions in the world and one of the top five in developed countries(7). According to data from the Telephone Health Survey 2003, approximately 70 % of adult men and 50 % of women in Germany are currently overweight or obese(Reference Mensink, Lampert and Bergmann6). Various studies have shown that excess weight contributes to CVD, some cancers and type 2 diabetes(Reference Bergström, Pisani and Tenet8, 9). The current epidemic reflects a long-term upward shift in the distribution of BMI across all populations(Reference Flegal, Carroll and Ogden10, Reference Dixon and Waters11). One explanation for the development of obesity is an energy imbalance caused by a combination of more sedentary lifestyles and an increase in consumption of energy (rich foods)(Reference Hill and Peters12–Reference French, Story and Jeffery14).
National surveys conducted in Germany between 1985 and 2002 showed an increase in the prevalence of obesity in both genders(Reference Helmert and Strube18), and according to the German National Health Interview and Examination Survey(15) only 13 % of the German adult population met the German guideline of being physically active three times per week for at least 30 min in 1998. A study conducted in Bavaria, Germany, revealed that fewer than a third of the 893 participants met the recommended physical activity levels and, in addition to reduced sports activities, obesity was also linked to increased television viewing and use of computers(Reference Schaller, Seiler and Himmerich16). Furthermore, food consumption in the German population has changed over the years. Although there has been a positive increase in fish, poultry, vegetable and fruit consumption, there has also been an increase in sweets and fried potato dishes(17).
The first study to introduce the idea of a population-wide energy gap and its estimation model was that of Hill et al.(Reference Hill, Wyatt and Reed19). Using data from the National Health and Nutrition Examination Survey and the Coronary Artery Risk Development in Young Adults study(Reference Lewis, Smith and Wallace20), they estimated the distribution of the rate of weight gain within the population over a period of 8 years. With the assumption of a gradual/linear rate of gain and that each pound of body weight equals 14 644 kJ (3500 kcal), they calculated the annual energy accumulated. The estimated energy accumulation for 90 % of the population was approximately 209 kJ (50 kcal)/d. Thus, it was hypothesized that by some combination of increasing energy expenditure and reducing energy intake by 419 kJ (100 kcal)/d, most of the weight gain in the US population could be prevented. In China, the estimated energy gap for the population was 188 kJ (45 kcal)/d(Reference Zhai, Wang and Wang21). In Australia, using data from the Australian Longitudinal Study on Women’s Health, an average weight gain of approximately 0·5 kg/year for women aged 45–55 years was found, which equates to an energy imbalance of only approximately 42 kJ (10 kcal)/d(Reference Brown, Williams and Ford22). In Swedish adults, the estimated energy gap was 34 kJ (8·2 kcal)/d for men and 52 kJ (12·4 kcal)/d for women(Reference Berg, Rosengren and Aires23).
Müller and his colleagues(Reference Plachta-Danielzik, Landsberg and Bosy-Westphal24) used the same approach to calculate the energy gap in German children using actual measures of fat mass and fat-free mass to calculate energy gain. They found mean daily energy increases of 89 kJ (21·2 kcal)/d in boys and 194 kJ (46·4 kcal)/d in girls aged 10–14 years. The 90th percentile of energy gap in these children who became overweight was 301 kJ (72 kcal)/d for girls and 223 kJ (53·2 kcal)/d in boys. The authors estimated that reductions in energy intakes of 419–586 kJ (100–140 kcal)/d should prevent overweight in German children.
The objective of the present study is to estimate the energy gap of the German adult population using results from national health surveys conducted between 1985 and 2003 by using the average weight gain over the 17-year period and translating the kg (fat) into kJ (kcal) in order to calculate the estimated energy accumulation per year (and per day).
Methods
The published results from four national health surveys conducted between 1985 and 1998 (1984–1986, 1987–1988, 1990–1992 and 1998)(Reference Forschungsverbund25, 26) were used for the analysis. Each cohort included between 2300 and 3700 participants, with a total of 22 807 participants (11 248 men and 11 559 women). The German national health surveys (Bundesgesundheitssurvey, ‘Federal Health Survey’) were used to determine the health status of the German adult population. The surveys were conducted by the Robert Koch-Institute on behalf of the German Ministry of Health. The data from the first two health surveys only include West Germany, and body weight and height were individually measured in a laboratory setting.
In addition, three surveys of the ‘Bertelsmann Health Monitor’ in 2002–2003 (Spring 2002, Fall 2002 and Spring 2003)(Reference Böcken, Braun and Schnee27) with a total of 3707 participants (1736 men and 2071 women) were used. For data collection of the ‘Bertelsmann Health Monitor’, at each data point, approximately 50 000 households across Germany were contacted and the three surveys were merged to report mean height and weight for 2002. The survey was used to obtain information and trends about the existing German health-care sector. Body weight and height were assessed using self-reported measures. Given the existing bias with regard to self-reported height and weight, both measures were adjusted accordingly using results from the national health survey 1984–1986, in which both direct and self-reported measures of height and weight were collected. More details about the adjustments can be found in Helmert and Strube(Reference Helmert and Strube18). All included samples were representative for the German population aged 25–69 years.
For the analysis, the published body weight data, separated by gender, of the seven health surveys reported in Helmert and Strube(Reference Helmert and Strube18) were used to estimate the energy gap in the German population.
Results
Men and women aged 25–65 years using the population-based data from the surveys mentioned above were included to estimate the energy gap in the German population. Table 1 shows the body height, weight and BMI in men and women aged 25–69 years between 1985 and 2002.
Table 1 Mean body height, weight and BMI of German adults (aged 25–69 years) by gender using national health surveys (1985–2002; n 26 614)Footnote *
* Retrieved and modified from Helmert and Strube(Reference Helmert and Strube18).
† Pooled means from all three ‘Bertelsmann Health Monitor’ surveys.
Given these data and assuming a linear rate of gain, the average annual weight gain among men was 0·22 kg and 0·32 kg among women over the 17-year period. Assuming weight gain is normally distributed, 90 % of the population gained < 0·54 kg/year (for men = 0·49 kg/year; for women = 0·54 kg/year).
Assuming that each kilogram of weight gained represents 32 238 kJ (7700 kcal), the estimated average energy accumulation is 19 kJ (4·64 kcal)/d in men and 28 kJ (6·75 kcal)/d in women aged 25–69 years. The distribution of estimated energy accumulation for 90 % of the German population is < 50 kJ (12 kcal)/d; men = 43 kJ (10·33 kcal)/d; women = 48 kJ (11·40 kcal)/d.
Since direct measures of energy cannot be used in large population studies, we used estimations of energy efficiency by Hill et al.(Reference Hill, Wyatt and Reed19) and Brown et al.(Reference Brown, Williams and Ford22). The authors assumed an energy efficiency of at least 50 %; meaning for every excess 419 kJ (100 kcal) consumed, at least 209 kJ (50 kcal) of energy are deposited in energy stores. With an energy efficiency of approximately 50 %, the yearly weight gain in the German population could be prevented with < 100 kJ (24 kcal) reduction in energy intake or increase in energy expenditure per day in 90 % of the population. Figure 1 shows the hypothetical weight gain projection for men and women in Germany with and without the 100 kJ (24 kcal)/d energy gap.
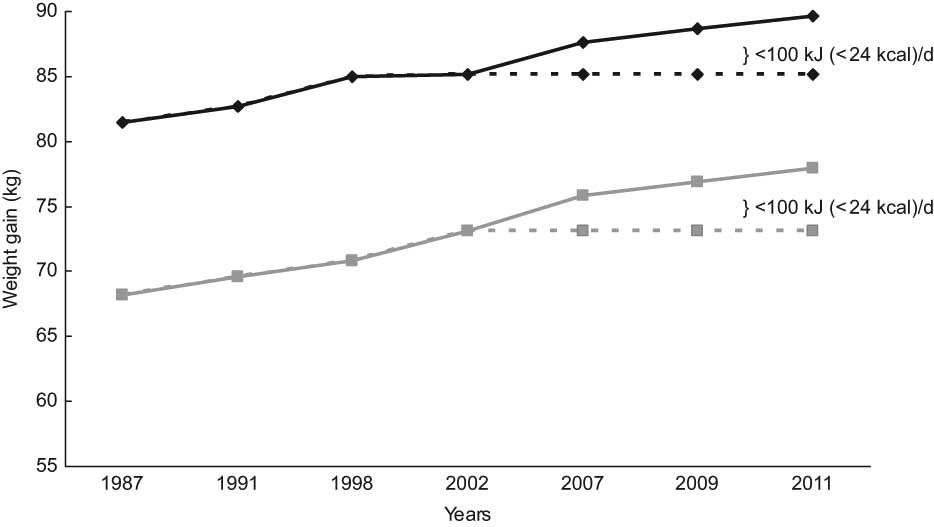
Fig. 1 Hypothetical weight projection by gender with and without the 100 kJ (24 kcal)/d energy gap. The solid lines indicate the projected weight gain in the population without any changes, whereas the dotted lines indicate weight maintenance with an energy gap of <100 kJ (24 kcal)/d (
![]() , men;
, men; ![]() , women)
, women)
Discussion
In the present analysis, we estimated the annual energy accumulation of the German adult population using cross-sectional population-based data from several representative surveys. We determined that by a combination of reducing energy intake minimally and increasing energy expenditure modestly further weight gain could be prevented in Germany.
Thus, the magnitude of this daily imbalance between energy intake and energy expenditure is estimated to be relatively small, with energy accumulations of approximately 63 kJ (15 kcal)/d accounting for weight gain in US population studies(Reference Hill, Wyatt and Reed19) and even less for children(Reference Plachta-Danielzik, Landsberg and Bosy-Westphal24, Reference Wang, Gortmaker and Sobol28). However, this gap can lead to an annual weight gain of at least 2 pounds per year and 20 pounds in 10 years(Reference Hill, Wyatt and Reed19).
Given the current prevalence of overweight and obesity in Germany and its rather notable increase in incidence per year, it is surprising that 90 % Germans appear to gain only an estimated ≤ 50 kJ (≤ 12 kcal)/d, compared to approximately 209 kJ (50 kcal)/d in 90 % of the US population. German children (10–14 years) appear to be gaining more than adults(Reference Plachta-Danielzik, Landsberg and Bosy-Westphal24). For the German adult population, an approach that reduces energy intake by 100 kJ (24 kcal)/d could potentially prevent further weight gain in approximately 90 % of the population and thus at least stabilize obesity rates. This equals < 100 g of fat-reduced yoghurt or approximately 5 min of fast walking.
The use of population-based data collected by others limits the extent of the present analysis, and in general self-reported information is inferior to actual weight measurements. Given our lack of access to original data sets, we could not adjust for possible confounders such as changes in smoking status or socio-economic characteristics. In addition, using existing aggregated data does not allow for the adjustment of possible age or gender differences over the years. Since original data were not available, it was not possible to determine whether changes in age or gender distribution might exist and whether they might have influenced the changes in weight over the years.
However, we assume that the data used in the reference study adequately adjusted for potential confounders and sample distribution changes. It is also not the intention of the authors to calculate the precise caloric differences and weight changes of the German population over the years, but rather to point out that the estimated energy imbalance of this magnitude is in all likelihood a result of the increase in overweight and obesity in the population.
The energy gap concept of Hill et al.(Reference Hill, Wyatt and Reed19) has been criticized as not accounting for the fact that obese individuals have accumulated more stored energy than lean individuals(Reference Swinburn, Sacks and Lo29). Hill et al.(Reference Hill, Peters and Wyatt30) clarify this by distinguishing between the energy gap for prevention of additional weight gain (which does not depend on stored energy) and the energy gap for maintenance of weight loss. The energy gap for the treatment of obesity is much larger due to the reduction in energy requirements after weight loss(Reference Hill, Peters and Wyatt30). It is not suggested that this approach can restore the population to normal weight, but rather that it can stabilize obesity rates and prevent further weight gain.
It should be noted that in calculating the energy gap, Hill et al.(Reference Hill, Wyatt and Reed19) used an energy efficiency of 50 % for storage of excess energy in order to model the most conservative case. In reality, excess energy may be stored with greater efficiency under most conditions. If one assumes that the efficiency of storage of excess energy is > 50 %, the energy gap would be reduced.
Even though the energy gap is based on theoretical estimations and assumptions and empirical results are urgently necessary, we believe that the energy gap in the German population is still small and further weight gain could be prevented using the small-changes approach. This method emphasizes the importance of small increases in physical activity, as well as small decreases in food intake(Reference Hill, Wyatt and Reed19, Reference Hill31). Both changes can be achieved with relatively minimal effort, for example walking approximately 1 km/d, which equals approximately 167 kJ (40 kcal) of energy expenditure or by reducing portion size modestly with each meal every day. There is already existing evidence that the small-changes approach can be effective. Dolan et al.(Reference Dolan, Weiss and Lewis32) and Bravata et al.(Reference Bravata, Smith-Spangler and Sundaram33) show the feasibility and effectiveness of making small changes to increase physical activity. School and family programmes using the small-changes approach have also shown promising results(Reference Stewart, Dennison and Lohl34–Reference Rodearmel, Wyatt and Stroebele36). In regard to dietary behaviour, Rolls et al.(Reference Roll, Drewnowski and Lediwke37) have consistently shown that decreases in energy density produce small reductions in energy intake. With the use of the small-changes approach, we believe that it might be possible to stabilize obesity rates in most populations.
We believe that making small changes to everyday living is more feasible and sustainable than big changes such as complete diet alterations or the transformation from a sedentary to a highly active lifestyle. In addition, our current environment does not support an active lifestyle. Small environmental changes could include various improvements such as more bike paths in cities, better public transportation systems or easier access to healthy foods in public places such as schools and cafeterias. In the United States, there are already initiatives by various entities such as the American Society of Nutrition, the Institute of Food Technology and the International Food Information Council, which support the small-changes approach and are ready to contribute to the goal of changing people’s lifestyle behaviour in collaboration with the private sector and the government(Reference Hill31). Given the rise in obesity rates in Germany, creating a German initiative with similar goals supported by various private and governmental institutions and stakeholders of different industries such as food supply or sporting goods is urgently needed. It is crucial that the public and private sector work together in order to create an environment that encourages people to make small changes towards a healthier lifestyle.
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. There are no conflicts of interest. N.S. and J.O.H. analysed the data and drafted and revised the manuscript. N.S. wrote the first draft of the manuscript. J.O.H. and S.N.W. made substantial contributions to the interpretation and writing of the manuscript and its revision.


