



Burkina Faso is a landlocked and low-income country situated in West Africa. The country is among the poorest in the world with 44 % of its population below the international poverty line of US$1·90 per day(1). The mortality rate of children under-five in Burkina Faso is also one of the highest in the world (85 %), 35 % of which is attributed to malnutrition(2). The country’s 2016 National Nutritional Survey revealed that 27·3 % of children under-five were stunted, 7·6 % were severely wasted and 19·2 % underweight(3). Concurrently, overweight and obesity among women increased from 7·7 % in 1980 to 28·8 % in 2016(4). The country has implemented some important changes in nutrition policy during recent years, which has resulted in progress which includes reduced rates of stunting and wasting in the under-fives, but which do not yet put the country on track to meet the World Health Assembly targets in 2025(Reference Vanderkooy, Verstraeten and Becquey5). Recent security issues in the northern and eastern parts of the country are jeopardising the sustainability of this progress.
Burkina Faso National Nutrition Policy suggests that child malnutrition and micronutrient deficiencies are due primarily to poor breast-feeding and complementary feeding practices, accompanied by high prevalence of infectious diseases and limited health services(6). The 2019 Nutrition Policy in Burkina Faso recommended that these gaps be addressed through prioritising investment in multi-sectoral programmes, which mainly benefit women and children(Reference Vanderkooy, Verstraeten and Becquey5). Previous research in Burkina Faso and other low-and-middle income countries has shown that improvements in maternal and child nutrition are held back by deep-seated, cultural and socially defined gender inequities, which contribute to women’s lack of empowerment and their limited capacity to influence household decision-making(Reference Shiwakoti and Paudel7–Reference Heise, Greene and Opper9). Women are also expected to carry heavy workloads, are subject to restrictive gender norms and to a lack of access to health-promoting resources(3). Gender is becoming increasingly recognised as an underlying determinant of health and nutrition and an increasing number of interventions focus on women’s empowerment with positive effect(Reference Heise, Greene and Opper9–Reference Olney, Pedehombga and Ruel14). A multi-sectoral intervention, which provided dedicated land to women in Burkina Faso and trained them in agricultural production and income generation, led to significant reductions in child wasting(Reference Olney, Pedehombga and Ruel14) and to improvements in mothers’ nutrition and empowerment outcomes(Reference Olney, Bliznashka and Pedehombga15).
Simultaneously, there is a growing recognition of the importance of men’s involvement in ensuring adequate maternal and child nutrition(Reference Ochieng, Afari-Sefa and Lukumay16–Reference Barker, Dombrowski and Colbourn18). Men play an important role in providing instrumental and emotional support to mothers and children(Reference Kansiime, Atwine and Nuwamanya17). For interventions to be effective, however, it is important to involve communities in their development; effective interventions tend to be embedded in the social life and ecology of the community which includes the men(Reference McCloskey, McDonald and Cook19).
The objective of this study was to carry out discussions with women and men in a rural community in Burkina Faso in order to collect context-specific insights into maternal and child health and nutrition issues. The intention was also to explore options for contextually appropriate interventions to improve maternal and child health and nutrition in the ‘first 1000 d plus’ period, this term describing the period from before conception up to a child’s second birthday. This study is embedded in a larger, multicentre study entitled INPreP (Improved Nutrition Preconception, Pregnancy and Post-Delivery), which aims to understand how and where best to engage with community and relevant stakeholders to optimise nutrition in the 1000 d plus period in Burkina Faso, Ghana and South Africa(20). The qualitative findings from the other INPreP countries are presented in other papers in this special issue(Reference Erzse, Goldstein and Norris21–Reference Watson, Kehoe and Erzse23).
Research methods
Study site and population
The study took place within the Nanoro Health and Demographic Surveillance System (HDSS) catchment area of the Nanoro Health district. The HDSS covers two counties including Nanoro (fifteen villages) and Soaw (nine villages). The HDSS is located in the Center-West region of Burkina Faso, 90 km from the capital city, Ouagadougou(Reference Derra, Rouamba and Kazienga24). Seven peripheral health facilities and one referral hospital provide health care to the population within the HDSS. It is a poor, rural region with a population estimated in 2017 at 171 119 inhabitants(Reference Derra, Rouamba and Kazienga24), where approximately 55 % of people live on <0·70 US$/d(Reference Zida and Kambou25).
The population comprises farmers who produce food crops (sorghum, millet and maize) and cash crops (peanuts, beans, sesame and cotton) on lateritic soils. It is an area with irregular and poor distribution of rains, rudimentary cultivation techniques and soil degradation. Rearing livestock is the second economic activity in this population, particularly cattle, goats, sheep, pigs, donkeys and poultry, much of which is sold(Reference Zida and Kambou25).
Diseases caused by inadequate potable water utilisation and poor sanitation are the main health problems(26). Malaria, acute respiratory infections and fever of unknown origin are the leading causes of mortality among adults and under-five children in this area(Reference Tinto, Valea and Sorgho27,Reference Maltha, Guiraud and Berenger28) .
Study design and data collection
A qualitative methodology was adopted for this study because of its utility in obtaining culturally specific information about the values, opinions, behaviours, relationships and social contexts of particular populations. Focus group discussions (FGD) were chosen as the method of data collection because they allow discussion on a research topic where a specified population or group’s opinions are given, and the meanings behind those perceptions are explored(Reference Nyumba, Wilson and Derrick29).
Discussions were conducted to explore the community’s maternal and child health and nutrition priorities. Therefore, a topic guide (Appendix A and B) with standardised questions for the three INPreP sites was generated. Questions explored participants’ views of the major health issues for women and children and of specific nutritional issues. Participants were invited to suggest interventions which might address these issues. Flexibility was built into the topic guide to allow for some probing where it was required for clarity.
Study participants were purposively recruited from ten of the twenty-four villages of the HDSS and from different households. Villages were selected in order to ensure that FGD were distributed across the study area (Fig. 1). Community informants facilitated the recruitment of participants for the FGD who represented age groups across the reproductive life course. Potential participants were given a Participant Information Sheet outlining the study purpose and procedures and those who agreed were invited to attend the FGD at a convenient location within the community. On the day of the FGD, participants’ characteristics were confirmed and they were checked against the eligibility criteria. Written informed consent was obtained by a research assistant. Non-literate participants signed their consent form in the presence of a witness.
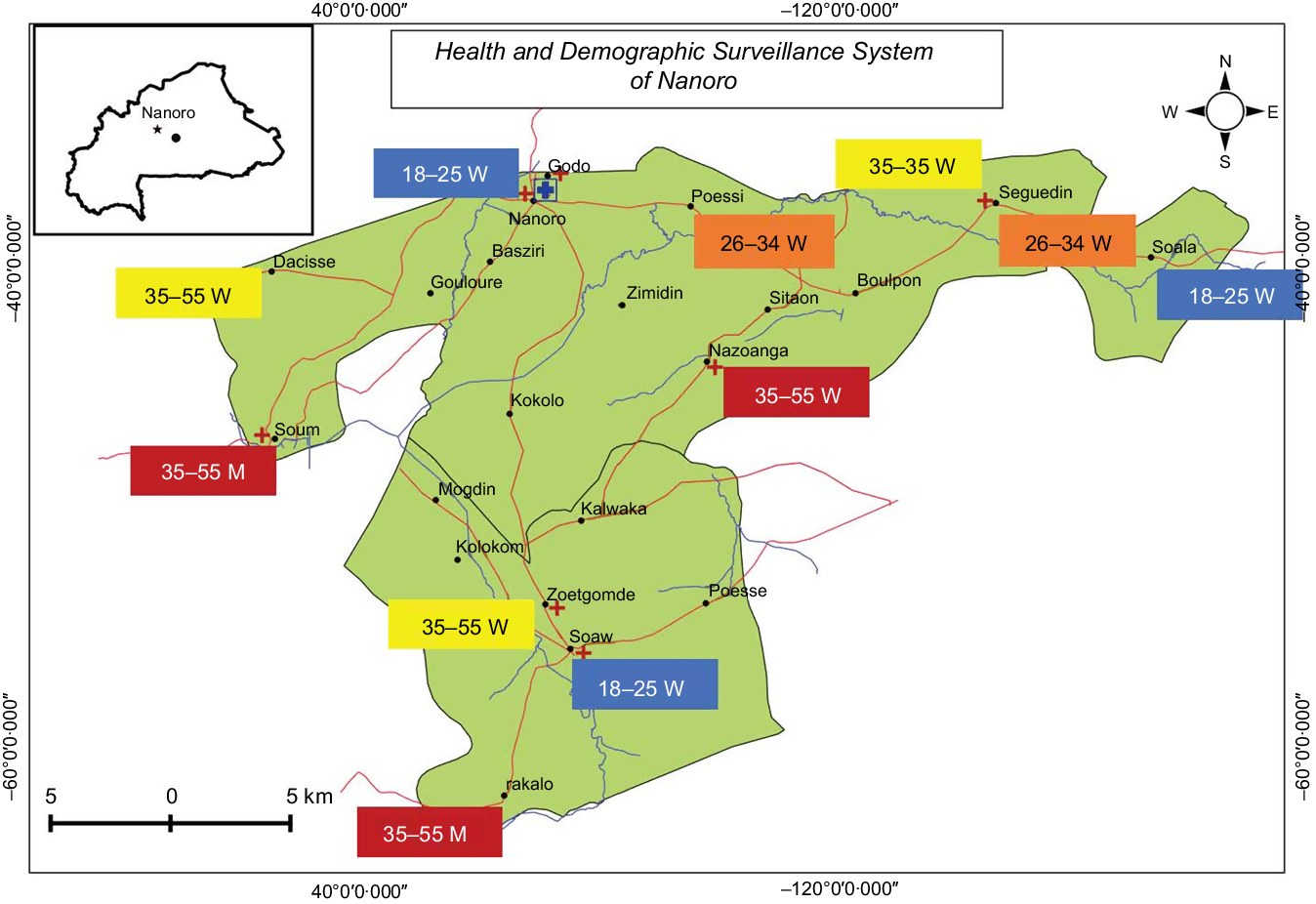
Fig. 1 Map of the study area and distribution of focus group discussion per age group. W: women; M: men. ![]() , Village;
, Village; ![]() , referral hospital;
, referral hospital; ![]() , health facility;
, health facility; ![]() , river;
, river; ![]() , departmental road;
, departmental road; ![]() , Health and Demographic Surveillance System area
, Health and Demographic Surveillance System area
Participants were grouped by age and gender to enable them to freely express themselves. The research team felt that older women might inhibit younger women from speaking freely and that women might feel uncomfortable in joint meetings with men. Therefore, the groups were formed as follows: men aged 18–55 years, women aged 18–25 years; women aged 26–34 years and women aged 35–55 years.
FGD were conducted in the local language (Moore) by a moderator and an observer who took notes, these roles being taken by field assistants with a background in social research. Discussions were audio recorded.
Data analysis
Audio recordings from the FGD were simultaneously translated and transcribed verbatim from the local language into French and then into English by a social scientist. The study coordinator and the field assistant coded the transcripts independently in NVivo 12 qualitative analysis software (QSR International Pty Ltd), then inductively identified and agreed on key emerging themes through discussion. A consensus forming workshop was held with the four INPreP research teams to thematically analyse the initial codes. Thematic analysis was used to organise and produce rich descriptions of the data following established guidelines(Reference Nyumba, Wilson and Derrick29). A code book was developed based on the topic guide, research objectives and the thematic grouping of the transcripts. The final set of codes was agreed by the research team, and definitions for each code were developed. Field notes taken during the data collection were used to supplement data from the transcripts.
Results
Participants characteristics
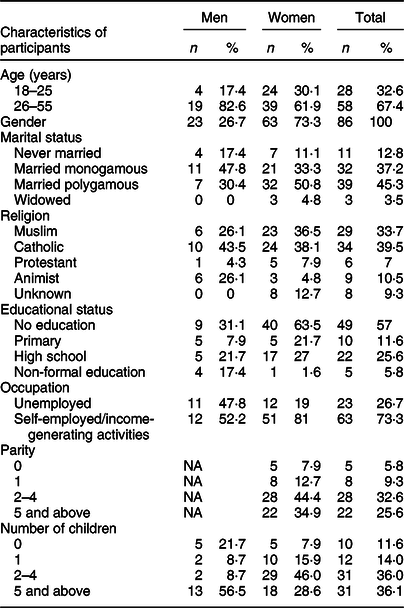
A total of eighty-six men and women participated in eleven FGD (Table 1). Of the participants, 73 % were women, 57 % had received no education and 27 % were unemployed. Five women had never given birth (Table 2). Data are presented below as they relate to the study objectives to (i) understand context-specific issues which affected maternal and child health and nutrition and (ii) explore options for contextually appropriate interventions to improve maternal and child health and nutrition.
Table 1 Composition of focus groups
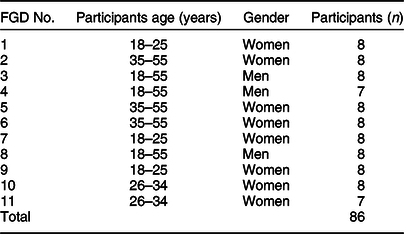
Table 2 Socio-demographic characteristics of participants
Obstacles to good maternal and child nutrition
Participants reported a number of barriers to optimal nutrition of mothers and children in their communities. Two major themes emerged: (1) poverty and (2) challenges generated by socially and culturally determined gender roles. Sub-themes related to access to health care and farming infrastructure to enhance food production and women lacking access to food whilst pregnant. Themes and sub-themes are described below, supported by verbatim quotes from the FGD (Table 3).
Table 3 Additional illustrative quotes from research in Burkina Faso
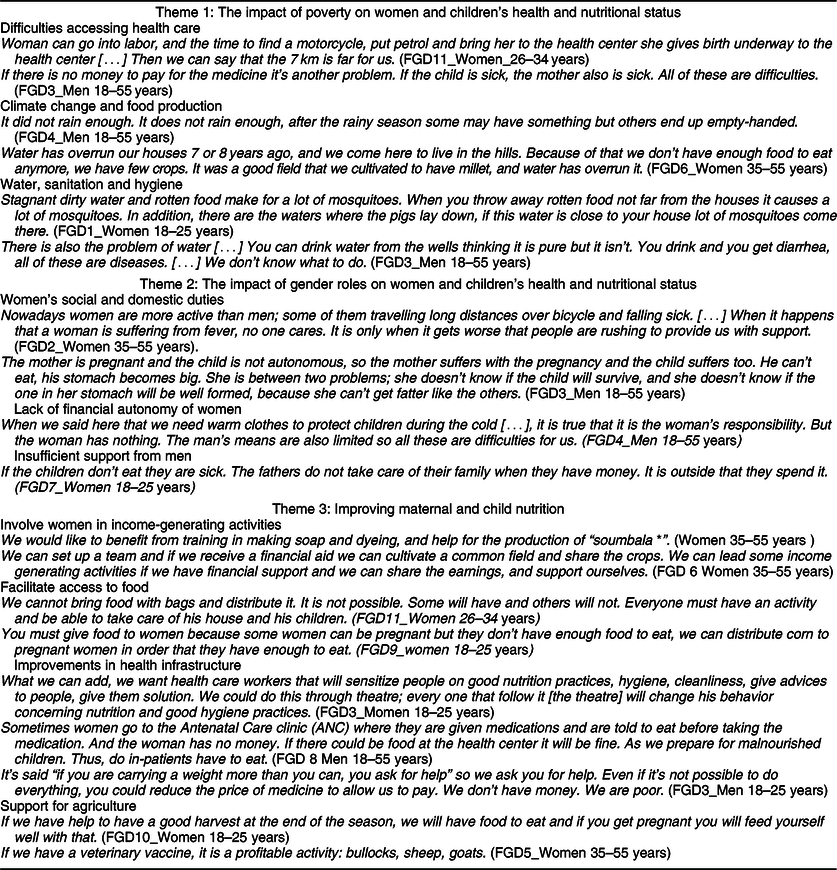
* Soumbala is the fermented seeds of Parkia biglobosa, also known as the African locust bean.
Theme 1: The impact of poverty on women and children’s health and nutritional status
Difficulties accessing health care
Despite free universal health coverage for pregnant women and children under-five years of age implemented in Burkina Faso from 2017, poverty affected access to health care facilities. Poverty-related issues described by participants included distances between the household and the health care facility, the low quality of the free health care services and lack of availability and affordability of drugs.
After the consultation there are no drugs to buy. You can come back on next day and there is still no drug. (FGD7_Women 18–25 years)
Difficulty prioritising money for food
Lack of money also led to having to make choices between paying for health care or paying for food. Available money was in these cases often used for health care.
You can have money and you tell yourself that you are going to pay for a bag of rice, and when you get home, someone is sick and you use that money to go to the health center. There is no more bag of rice. (FGD8_Men 18–55 years)
This led to various coping mechanisms that often prioritised money spent on health care instead on nutrition.
If the child is sick, you can sell some part of your crops to pay for drugs. (FGD2_Women 35–55 years)
Climate change and food production
Both too much and too little rain reduced the crop yield for farmers and had an impact on their ability to feed themselves and their families. They described how some parts of the study area are now regularly flooded during the rainy season. This has led to displacement of some communities to places where they have to start a new life, build new houses and cultivate new, less fertile land.
Lack of rain also leads to low crop productivity and food shortages. In addition, some of the soil was poor quality and required fertilizer to grow millet, the staple food. This was challenging when farmers could not afford fertilizer or other farming inputs.
One year is not enough to solve one bad year’s harvest. The year that it hadn’t rained enough you manage to get through it. And the next year if you have good harvest you have to solve the old problems you get when you didn’t have food to eat with the new harvest. So, if the granary becomes your box and you take grain out of there to eat and sell you are finished. (FGD3_Men 18–55 years)
Water, sanitation and hygiene
Lack of sanitation was also identified as a cause of poor maternal and child health. Access to potable water was limited by the presence of polluted and dirty wells. Polluted water caused nutritional problems because it is often the only source of water for drinking and cooking.
Even though the food is clean if you put it in a dirty dish it gives diseases. (FGD2_Women 35–55 years)
Men and women also reported difficulties in keeping the environment clean. Lack of facilities to dispose waste water and trash in a hygienic way meant that households were often surrounded by rubbish, which they worried caused the spread of disease.
Theme 2: The impact of gender roles on women and children’s health and nutritional status
Women’s social and domestic duties
The need to fulfil gender-specific social and domestic roles was perceived as a barrier to improving maternal and child nutrition by both men and women. Discussions reflected the fact that women were responsible for running the household, looking after the family and working the land. Participants, particularly older women, explained that prioritising such responsibilities often came at the cost of maternal and child health.
When you leave for the purchase of the goods there is no one to look after the children. While you went out of the house early […] you did a job for which your body does not have health, and your child who stayed at home is not well taken care of. (FGD2_Women 35–55 years)
Women found it difficult to adequately fulfil their maternal role and ensure financial security.
If you’re pregnant and you have a baby and you want to pedal the bike to carry out activities it’s hard, and your kids will cry and people will make fun of you… (FDG11_Women 26–35 years)
Men seemed critical of women who juggled both economic activity and child care.
Some women do not take good care of children. They can put the child in the sand at the market and the child has fun with the sand while it can make him sick… (FGD4_Men 18–55 years)
Men were also critical of women’s birth spacing, remarking on how pregnancy might negatively influence the mother and child’s well-being. They suggested, for example, that women may not be able to properly breastfeed while pregnant. Participants said that giving birth to many children was a determinant of household food insecurity and was difficult at times of food shortages.
There are women who get children in a close way. [.]While the other one has not had enough food, he already has a little brother or sister […] (FGD6_Men 18–55 years)
According to women, men acknowledged the burden pregnancy placed on mothers and children but were sometimes reluctant to use family planning.
There are women, if they adopt a contraceptive method, the husband can reject her… (FGD2_Women 35–55 years)
Lack of financial autonomy of women
Lack of money was a major problem for many women; they had to rely on their husband’s income and lacked opportunities to generate their own money.
Women do not have any activity that generates income. If they had some, if they have a problem they can manage until the husband arrives… (FGD5_Women 35–55 years)
Insufficient support from men
The lack of male involvement in the household was widely discussed by women. Women felt overloaded with domestic duties and saw the support they received from men in their households to be insufficient in a number of ways including nutritionally. First, women felt that men no longer took care of important needs such as paying for their children’s schooling, clothing or health care.
The woman has to do her best to allow the child to wear clothes and eat. The man is going to drink his alcohol and come back late at night. He doesn’t know what is going on with the woman and the children. (FGD5_Women 35–55 years)
Women felt that they were left with sole responsibility for farming and food production for their families in increasingly difficult conditions.
They have created a plough for women, and women tract themselves instead of the donkey. Women pay the price and use themselves. We call it ‘I am my own donkey’. Nowadays […] you can’t even pull 10 lines and sow. (FGD6_Women 35–55 years)
Theme 3: Improving maternal and child nutrition
Participants suggested a range of solutions to the nutritional problems of women and their children in ways that were both nutrition-specific and nutrition-sensitive.
Facilitating access to food
Since poverty is a major problem and prevents access to food, participants said they would like to see food subsidies or receive these products for free.
If they could sell the food to us at ‘social’ prices it will be good, because nowadays you cannot expect one to come and give you free food like that. This is not possible. (FGD8_Men 18–55 years)
Participants also recognised that free or subsidised food provision was not a sustainable option nor going to solve root causes. Therefore, others felt that they needed training in skills that would help them improve their ability to grow food.
If you distribute food to everybody that will certainly bring issues; you have to train us on activities that will help us have food. Otherwise if they give you 30 bags of food you will eat all and will finish. (FGD3_Men 18–55 years)
Supporting agriculture
The community was aware of strategies for the development of resilience in agriculture and consequently wanted technical assistance and financial support to develop this sector.
If we can have ploughs and donkeys to pull them during the rainy season it will facilitate field work. If we also put fertilizer this will allow us to have good crops and our food will improve. (FGD11_Women 26–34 years)
They not only wished for help in raising livestock for breeding and for producing manure to fertilize the soil but also asked for support in keeping their animals healthy.
There is a lot to do. [ …] If we can also breed in addition and you have natural fertilizer to enrich the ground, you will have a better harvest than someone that hasn’t done the same. (FGD2_Women 35–55 years)
Involving women in income-generating activities
Women across all age groups said they would like to be employed in order to guarantee a livelihood for themselves and their families. They saw this as benefiting the whole community.
If they find us employment it will improve our living conditions and it will also develop the village. (FGD7_Women 18–25 years)
Woman asked for support to build their capacity to start businesses and acquire skills that would enable them to make their own money and take care of their families. They also talked about working their land collectively to benefit them all.
Women were clear about the connection between their ability to generate wealth and improved health.
In the other villages, women have income generating activities that they lead but here in Seguedin we do not have any. It is only us that have nothing. If we had activities with income our health would improve. (FGD10_Women 26–34 years)
Increasing men’s commitment to caring for their families
Men’s involvement was considered to be an essential factor in facilitating good maternal and child nutrition, especially their involvement in the decision to use family planning. Women wanted men to be made aware of the need for and benefits of family planning, even though they were not convinced that this would change men’s behaviour.
One must raise men’s consciousness to take care of their wives … But you cannot change all men. (Laughter)…. They will not all change. There are some for whom it is not possible, you cannot change them. Some men, it is their friends who teach them to behave badly. (FGD11_Women 26–34 years)
Improving health infrastructure
The community, younger members in particular, suggested that a range of investments should be made to improve health infrastructure. These included making medications more affordable and accessible, employing more and better trained health care staff, increasing awareness of the importance of good nutrition and making food available at health care centres for in-patients.
We also want advice. When we come for consultation they can show us the food which is suitable for the children of six months, for example. It will also help us. (FGD7_Women 18–25 years)
Participants felt that making food available at health care centres would help women coming for consultation and for in-patient stays. Currently, food for patients is only available at the market which takes place only every 3 d and the food bought there can be unsuitable. Patients have to bring food from home or go back home to eat, sometimes about 7 km from the health care centre.
They should recruit people to cook in the health centre because someone brings his patient and there is no food. […] He is obliged to pay for dry bread for the patient. (FGD7_Women, 18–25 years)
Discussion
This study was carried out to explore the perspectives of men and women living in rural Burkina Faso on issues concerning maternal and child nutrition and how best to improve them. The community members in this study described factors influencing maternal and child nutrition such as income and resources, household food insecurity, lack of health services and unhealthy environments. Gender roles were widely perceived to impact nutrition; participants spoke of men limiting women’s ability to control food production, and how men had become distanced from household responsibilities and care of women and children. This led to women asking for support with establishing income-generating activities to provide food for themselves and their families.
The causes of malnutrition discussed in the focus groups included changing gender roles, structural political responses and increasing vulnerability to climate change. Participants described the gender roles in their community, which they saw as affecting women and children’s health and therefore their nutritional status. They spoke of the need for women to carry out their traditional domestic duties in addition to tasks outside of traditional gender roles such as farming the family’s land(Reference Lantara30,Reference Spurling31) . In Nanoro, there is a long standing history of men migrating to Côte d’Ivoire in order to look for jobs and more financial stability(32). In these circumstances, women have to take on responsibilities to compensate for the loss of men’s labour(Reference Lantara30,Reference Spurling31) . Women in this study explained, however, that they had limited financial autonomy and insufficient support from their husbands to carry out these tasks in the most effective way. Women described themselves as unable to purchase the food they needed and so consequently had to rely on men allocating them resources which were often insufficient to cover household needs. There is evidence that women’s autonomy is positively linked to health care seeking behaviour for their children as well as themselves(Reference Mkandawire and Hendriks33,Reference Ebot34) . Likewise, women’s participation in household decision-making and their ability to purchase food is significantly associated with increased diversity in the household diet(Reference Amugsi, Lartey and Kimani35). Participants in this study argued that improving women’s financial autonomy was key to addressing malnutrition but required increased income-generating opportunities. There is evidence that empowering women improves women’s health and has a positive impact on their nutritional status and that of their children(Reference Shiwakoti and Paudel7,Reference Heckert, Olney and Ruel12) . An intervention in Burkina Faso that gave women autonomy by providing them with land and agricultural training reported increased women’s empowerment and nutritional status as well as significant reductions in child wasting(Reference Olney, Pedehombga and Ruel14,Reference Olney, Bliznashka and Pedehombga15) . The same intervention, however, not only had unintended consequences for women such as reduced time for child feeding and care, but also exposed them and their children to risks associated with livestock and chicken faeces(Reference Ruel, Quisumbing and Balagamwala36).
The study described in this paper also reported women being too busy working at markets to take care of their children and provided more evidence that household chores and agricultural tasks can be detrimental to women’s health and nutrition(Reference Nti, Inkumsah and Fleischer37). Evidence from Ghana suggests that 70 % of women had only two meals a day because needing to leave home early for work gave them too little time to eat(Reference Kadiyala, Harris and Headey38). Difficult decisions regarding prioritisation of household and agricultural tasks over nutrition-related activities have to be made; time spent working on the land reduced time to gather firewood for cooking, for example, to go to the market to acquire a variety of foods and to prepare healthy and nutritious meals. All of this may affect dietary diversity of both child and mother(Reference Komatsu, Malapit and Theis39,40) . Men’s involvement has actually been considered an important element in supporting good maternal and child nutrition, since they have a double responsibility both as household decision-makers(Reference Singh, Lample and Earnest41) and as support to women and children(Reference Daniele, Sarrassat and Cousens44,Reference Ibrahim, Polcher and Karambiri45) . Both men and women described the heavy workload that women bear and their limited financial opportunities, which were believed to damage their health and well-being and that of their children. Although research has shown the positive effect of male support on postpartum birth spacing practices(Reference Daniele, Sarrassat and Cousens44), challenges remain. Further research exploring male perspectives on their roles in women’s reproductive health management needs to be conducted in order to identify enablers to this and therefore helps define context and culturally specific solutions.
In addition to the debate on shifting gender roles, climate change and access to quality health care were discussed as having real impact on the quantity and quality of food for mothers and children in the communities in this study. Agriculture provides occupation for 86 % of the rural population in Burkina Faso, but practices remain largely traditional and production relies on dependable climatic conditions, particularly the right amount of rainfall(Reference Ibrahim, Polcher and Karambiri45). Participants reported that inadequate or excessive annual rainfall was now more common. There is documentary evidence that these conditions are leading to a drop-in crop yields and a deficit of food(Reference Moursi, Moura and Martin-Prevel46). The effect of changes to patterns of the seasons on food intake has been described in resource-poor settings and linked with high rates of malnutrition in parts of Africa(Reference Ibrahim, Polcher and Karambiri45–Reference van Cooten, Bilal and Gebremedhin48). Because of this, the community suggested solutions to the nutrition problems that included social, economic and structural components. They would like their government to distribute free or subsidised food, in particular for the most vulnerable. Food donation or subsidisation is indeed a solution to malnutrition. In Burkina Faso, the ‘Société Nationale de Gestion du Stock de Sécurité Alimentaire’ supports vulnerable people to buy cereals at subsidised prices(49). These initiatives have faced considerable challenges with, and therefore criticism of, processes for identifying and targeting those in need and avoiding abuse of the system by those who are not in need(50). Similar feelings of distrust were also expressed by community members towards health services in this study; they did not trust the quality of the free health care.
Participant also discussed causes of malnutrition which included lack of care for women and children, and household food insecurity linked to access to health services and medicines. It was perceived in the FGD that the burden of women’s responsibilities is made heavier by the expectation that they will bear many children on top of their other roles already discussed. In Burkina Faso, the fertility rate remains high at 5·3 children per woman with low use of contraception (32 %) among women aged 15–49 years(51,Reference Naik and Smith52) . Men are sometimes resistant to the use of contraception, constrained by their belief that children are bestowed by God, and by the value they place on them as a source of financial security(Reference Kabagenyi, Jennings and Reid53). Uncontrolled fertility among women leading to inadequate birth spacing and frequent births is likely to reduce the time mothers have to provide optimum care to each child and for them to recuperate from the previous birth. This low autonomy in decision-making has been linked to sub-optimal usage of maternal health care services(Reference Tiruneh, Chuang and Chuang54).
Other topics discussed by participants that affect maternal and child health and nutrition were access the health care infrastructures and inadequate water, sanitation and hygiene. The most important contributing factor to low utilisation of health services by the poorest population groups was the expenditure it required in terms of payments for medicine, consultations and hospitalisation as well as indirect costs such as lost working time and transportation(Reference Samuelsen55,Reference Nguyen, Hai Khuat and Ma56) . Therefore, short-term coping strategies were described to finance health care which, in the long term, prevented people from feeding themselves appropriately(Reference Murphy, McGowan and McKee57,Reference Sauerborn, Adams and Hien58) . These sometimes included selling crops and farm animals or reducing food consumption in order to pay for catastrophic expenses. A previous study in the field of health economics conducted in 1996 in Burkina Faso showed how animals were used as ‘ambulatory savings-banks’ in order to pay for treatment(Reference Hausmann-Muela59), which was a concept indirectly described by community members. As in previous studies, participants in this study described selling crops grown for food to buy medicine, when necessary(Reference Su, Kouyaté and Flessa60,Reference Somé and Jones61) .
Study strengths and limitations
An advantage of this study is that it was conducted in the context of multicentre research involving researchers from different backgrounds including public health, anthropology, nutrition and psychology. The thematic analysis was conducted during a consensus forming workshop where the four INPreP research teams gather to share their data and agree themes and a set of codes from each site, thus enhancing the rigor of the analysis and interpretation. Another strength is that participants gathered in the FGD included men and women of different age groups allowing for diversity of experience and opinion. One limitation of the study, however, was that the interviews were conducted in the local languages, transcribed into French and then translated into English. Consequently, some statements may have lost their primary meanings through this process. To counteract this possibility, transcripts were shared between researchers and the representation of quotes and themes discussed and checked.
Conclusion
This paper offers context-specific insights into local maternal and child health and nutrition issues and identifies potential interventions suggested by community members as being appropriate and helpful for this population in Burkina Faso. The study highlights the importance of gender issues and of women’s empowerment in addressing maternal and child nutrition in Burkina Faso. Findings reported in this paper make some fundamental points about the need for multi-sectorial interventions to address the nutrition environment in a way that is sustainable and that go beyond supplemental provision of food or nutrients.
Acknowledgements
Acknowledgements: We are most grateful to all community members for their time and efforts while participating in the study and their confidence in our research. Financial support: This research was funded by the National Institute for Health Research (NIHR) (17/63/154) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care. Conflict of interest: The authors declare that they have no competing interests. Authorship: M.L.N., H.S., P.R.B., H.T., A.C. and M.B. designed the WP4 study. H.S., P.R.B., H.T. and M.B. supervised the implementation of the study and guided the manuscript conception. KO collected, transcribed and translated the data in English. A.C. checked and confirmed the accuracy of transcription and translation. A.C. and K.O. analysed the data. A.C. carried out the literature review and drafted the paper. All authors reviewed and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki. This anthropological study was approved by the National Health Ethics Committee in Burkina Faso, number 2018-12-156 and the University of Southampton Faculty of Medicine Ethics Committee, number 47290. All interviewees were informed before the start of the interview about project goals, the topic as well as their right to decline participation or to interrupt the conversation at any time. Anonymity was guaranteed and confidentiality of interviewees assured by assigning a unique code number to each informant. Written informed consent was obtained from all participants.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980020003365






