


The Mediterranean diet (MD) was defined as the dietary pattern found in the olive-oil-growing areas of the Mediterranean region in the late 1950s and early 1960s by Ancel Keys( Reference Trichopoulou 1 ). This dietary pattern varies between coastal and inland areas of the Mediterranean and depends on cultural differences, traditions, geographic location and food availability( Reference Willett, Sacks and Trichopoulou 2 , Reference Vareiro, Bach-Faig and Raidó Quintana 3 ), but generally the traditional MD is characterized by high consumption of legumes, cereals (in the past unrefined), fruits and vegetables, moderate to high consumption of fish (depending on proximity to the sea), moderate consumption of milk and dairy products (mainly in the form of yoghurt and cheese), moderate consumption of alcohol (mainly wine and preferably during meals), and low consumption of meat and meat products( Reference Trichopoulou, Costacou and Christina 4 ). High ratio of monounsaturated to saturated dietary fat is another characteristic of the MD, because of the abundant use of oil olive and the low intake of saturated dietary fats( Reference Trichopoulou 1 ). In addition to their healthy diet, Mediterranean people had regular physical activity, usually required for field or kitchen work and outdoor leisure activities( Reference Willett, Sacks and Trichopoulou 2 , Reference Contaldo, Pasanisi and Mancini 5 ).
The great richness and diversity of plants in the Mediterranean region provide numerous functional foods (FF) that improve state of health and/or provide a reduction in the risk of disease( Reference Diplock, Aggett and Ashwell 6 ), like olive oil, yoghurt, garlic, tomato, wine, condiments, herbs, spices and nuts( Reference Ortega 7 ). In addition to FF, the MD is rich in functional dietary components like phenols, flavonoids, isoflavonoids, phytosterols, phytic acid and n-3 fatty acids( Reference Ortega 7 ). As a whole, the MD is a good example of a functional diet( Reference Contaldo, Pasanisi and Mancini 5 ).
The functionality and disease-preventing effect of the ‘traditional’ MD has been proved by several studies in the literature( Reference Trichopoulou, Costacou and Christina 4 , Reference Biesalski 8 – Reference Valls-Pedret, Lamuela-Raventós and Medina-Remón 12 ). The MD has been related to reduced risk of CVD, certain cancers and overall mortality( Reference Trichopoulou, Costacou and Christina 4 , Reference Bondia-Pons, Serra-Majem and Castellote 10 , Reference Sofi, Cesari and Abbate 11 ). Furthermore, this dietary pattern has a protective effect on weight gain( Reference Schröder, Marrugat and Vila 13 , Reference Schröder 14 ) and the development of type 2 diabetes( Reference Biesalski 8 , Reference Schröder 14 , Reference Baldini, Pasqui and Bordoni 15 ).
Despite the health benefits of the MD, several studies have reported that dietary pattern in the Mediterranean areas has been changing and switching to a more Westernized diet( Reference Baldini, Pasqui and Bordoni 15 – Reference Bibiloni, Martínez and Llull 20 ). Increased prevalence of diet-related diseases such as overweight and obesity among children in Greece( Reference Kontogianni, Vidra and Farmaki 19 , Reference Farajian, Risvas and Karasouli 21 ), Spain( Reference Schröder, Marrugat and Vila 13 , Reference Moreno, Sarría and Popkin 22 ) and Italy( Reference Bellisle 23 , Reference Bonaccio, Di Castelnuovo and Costanzo 24 ) support the findings of these studies.
Adherence to the MD among the Mediterranean population was examined by several authors( Reference Baldini, Pasqui and Bordoni 15 – Reference Kontogianni, Vidra and Farmaki 19 ); however, studies evaluating the MD adherence of FF consumers, who are more health-oriented than non-consumers( Reference Bech-Larsen and Scholderer 25 ), are missing. Thus, in the present study we aimed to assess differences in adherence to the MD between consumers and non-consumers of FF among the Balearic Islands’ adolescent population.
Methods
Study design
The study is a population-based cross-sectional nutritional survey carried out (2007–2008) in the Balearic Islands (Spain), a Mediterranean region.
Study population
A multi-centre study was performed on Balearic Islands’ adolescents aged 12–17 years. The population was selected by means of a multiple-step, simple random sampling, taking into account first the location (Palma de Mallorca, Calvià, Inca, Manacor, Maó, Eivissa, Llucmajor, Santa Margalida, S’Arenal and Sant Jordi de Ses Salines) and then, by random assignment, the schools within each city. Sample size was stratified by age and sex. The socio-economic variable was considered to be associated with geographical location and type of school. As the selection of schools was done by random selection and fulfilling quota, this variable was also considered to be randomly assigned.
To calculate the number of adolescents to be included in the study in order to guarantee a representative sample of the whole Balearic Islands, we selected the variable with the greatest variance for this age group from data published in the literature at the time the study was planned; that was BMI( Reference Moreno, Fleta and Mur 26 ). The sampling was determined for the distribution of this variable; the confidence interval was established at 95 % with an error of ±0·25. The established number of subjects was 2400. The total number of subjects was uniformly distributed in the cities and proportionally distributed by sex and age group. Exclusion criteria were type 2 diabetes, pregnancy, alcohol or drug abuse, and non-directly related nutritional medical conditions.
The sample was oversized to prevent loss of information and as necessary to do the fieldwork in complete classrooms. In each school, classrooms were randomly selected among those of the same grade or level, and all of the adolescents of one classroom were proposed to participate in the survey. A letter about the nature and purpose of the study informed parents or legal tutors. After receiving their written consent, the adolescents were considered for inclusion in the study. All responses to questionnaires were filled in by adolescents. After finishing the field study, the adolescents who did not fulfil the inclusion criteria were excluded. Finally, the sample was adjusted by a weight factor in order to balance the sample in accordance with the distribution of the Balearic Islands’ population and to guarantee the representativeness of each of the groups, already defined by the previously mentioned factors (age and sex). The final number of adolescents included in the study was 1961 (82 % participation). The reasons to not participate were (i) the adolescent declined to be interviewed and (ii) the parents did not authorize the interview.
The study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Balearic Islands’ Ethics Committee (Palma de Mallorca, Spain).
General questionnaire
A questionnaire incorporating the following questions was used: age group; father’s and mother’s education level (grouped according to years of education: low, <6 years at school; medium, 6–12 years of education; high, >12 years of education); and father’s and mother’s socio-economic level, based on the occupation of parents and classified as low, medium and high, according to the methodology described by the Spanish Society of Epidemiology( Reference Alvarez, Alonso and Domingo 27 ).
Anthropometric measurements were also obtained. Height was determined using a mobile anthropometer (Kawe 44444, Asperg, Germany) and measured to the nearest millimetre, with the participant’s head in the Frankfurt plane. Body weight was determined to the nearest 100 g using a digital scale (Tefal sc9210, Rumilly, France); participants were weighed in bare feet and light underwear. BMI was computed as weight/height2. Study participants were categorized as underweight (≤5th percentile), normal weight (>5th to ≤85th percentile), overweight (>85th percentile) and obese (≥95th percentile) according to the WHO growth standards for children and adolescents( Reference De Onis, Onyango and Borghi 28 ).
Physical activity was evaluated according to the guidelines for data processing and analysis of the International Physical Activity Questionnaire( 29 ) in the short form and its specific modification for adolescents (International Physical Activity Questionnaire-A)( Reference Hagströmer, Manios and Gilbert 30 ). The specific types of activity assessed were walking, moderate-intensity activities (i.e. physical activity at school) and vigorous-intensity activities (i.e. sport practice), and an additional question about sitting time was used as an indicator variable of time spent in sedentary activity. On the basis of their total daily time of physical activity, the participants were divided into two groups: <60 and ≥60 min/d, according to the current physical activity recommendations( Reference Andersen, Harro and Sardinha 31 ).
Dietary questionnaire
Dietary intake was assessed with dietary questionnaires including two non-consecutive 24 h recalls and a validated semi-quantitative FFQ( Reference Moreno, Sarría and Popkin 22 ). The FFQ, which asked the participant to recall average intake over the past year, consisted of 145 items (118 items of the original validated FFQ, plus the most characteristic Balearic Islands foods in order to make easy it for the interviewees to answer) and was arranged by food type and meal pattern. Frequency of food consumption was based on times that food items were consumed (per day, week or month). Consumption <1/month was considered no consumption. Daily consumption (g) was determined by dividing the reported amount of the intake by the frequency (d). The period of consumption of seasonal items was also considered. To avoid bias resulting from day-to-day intake variability, the questionnaires were administered homogeneously from Monday to Sunday. Well-trained dietitians administered the recalls and verified and quantified the food records. Volumes and portion sizes were reported in natural units, in household measures or with the aid of a manual of sets of photographs( Reference Gómez, Kohen and Nogueira 32 ). Total energy and nutrient intakes were calculated using a computer program (ALIMENTA®; NUCOX, Palma, Spain) based on Spanish( Reference Mataix, Mañas and Llopis 33 – Reference Ortega, López and Marcos 35 ) and European food composition tables( Reference Feinberg, Favier and Ireland-Ripert 36 ) and complemented with food composition data available for Balearic food items( Reference Ripoll 37 ). The nutritional density of each functional dietary component was calculated by dividing the average intake of these nutrients by the total energy intake (MJ) in order to avoid bias caused by different intakes of energy. Adequacy of intakes of functional dietary components was calculated as a percentage of the age-specific Recommended Dietary Reference Intake (RDI) for Spanish adolescents( Reference Ortega, López and Marcos 35 ) and the RDI for Europeans( 38 ) when no reference data were given for Spanish adolescents.
Misreporters were determined by using Black’s modification( Reference Black 39 ) of the Goldberg cut-off for energy intake. To define under-reporting, the lower cut-off value for the ratio between energy intake and BMR (EI:BMR) was calculated for boys and girls separately as 3 sd below the mean of the ratio between total energy expenditure( 40 ) and basal metabolic rate (TEE:BMR) for the 99 % lower confidence limit. With this calculation, the variations of energy intake, BMR and energy requirements are taken into account. In large studies (n>500) the number of days of dietary assessment has a negligible effect on the cut-off values, and for measured BMR and 2 d of assessment, the CV used was 28·74 %( 38 ). Identification of misreporters was done based on EI:BMR: values <0·92 (boys) and <0·85 (girls) were considered to represent under-reporters and values ≥2·40 were considered to represent over-reporters( Reference Black 39 , Reference Johansson, Solvoll and Bjørneboe 41 ).
Assessment of functional food consumption
FF, which were selected according to a list( Reference Hasler 42 ), were taken from the FFQ. Moreover, modified milk (milk with low/reduced fat, milk with added n-3), infusions (coffee and tea) and soya milk were considered as FF in this review, due to various studies that reported these foods might reduce the risk of some diseases( Reference Shu, Jin and Dai 43 – Reference Bouchard, Ross and Janssen 49 ).
Adherence to the Mediterranean diet
A Mediterranean diet score (MDS) was defined according to a previously defined score indicating the degree of adherence to the traditional MD( Reference Trichopoulou, Costacou and Christina 4 , Reference Tur, Romaguera and Pons 16 , Reference Martínez, Llull and Bibiloni 18 , Reference Trichopoulou, Kouris-Blazos and Wahlqvist 50 ). The MDS was converted to relative percentage of adherence using a previously described method( Reference Sanchez-Villegas, Martinez and De Irala 51 ). An energy-adjusted value was obtained for each individual for the daily consumption of legumes, cereals and roots (including bread and potatoes), fruit (including nuts), vegetables, fish, meat (and meat products) and milk (and milk products). The alcohol consumption in adolescents must be null and values above the reference indicate consumption of alcohol on the part of adolescents. Information about the consumption of all the food items was obtained from the FFQ.
All the values were standardized as a Z value. A Z-score expresses the difference between the individual’s measurement and the mean value of the reference population (in this case, the study population) as a proportion of the standard deviation of the reference population ((observed intake minus energy-adjusted intake)/sd).
The total MDS was computed by adding up all the Z-scores obtained for the favourable or ‘more Mediterranean’ dietary components (legumes, cereals and roots, fruit, vegetables, fish and MUFA:SFA) and subtracting the Z-scores obtained from the consumption of meat, whole milk (mainly high in fat) and alcohol (in adolescents):
 $$\eqalign{\mathop{\sum}{Z_{{i}} = Z_{{{\rm legumes}}} } {\plus}Z_{{{\rm fruit}}} {\plus}Z_{{{\rm vegetables}}} {\plus}Z_{{{\rm cereals and roots}}} {\plus}Z_{{{\rm fish}}} \cr {\plus}Z_{{{\rm MUFA:SFA}}} {\minus}Z_{{{\rm milk}}} {\minus}Z_{{{\rm meat}}} {\minus}Z_{{{\rm alcohol}}} .$$
$$\eqalign{\mathop{\sum}{Z_{{i}} = Z_{{{\rm legumes}}} } {\plus}Z_{{{\rm fruit}}} {\plus}Z_{{{\rm vegetables}}} {\plus}Z_{{{\rm cereals and roots}}} {\plus}Z_{{{\rm fish}}} \cr {\plus}Z_{{{\rm MUFA:SFA}}} {\minus}Z_{{{\rm milk}}} {\minus}Z_{{{\rm meat}}} {\minus}Z_{{{\rm alcohol}}} .$$
The MDS was converted to relative percentage of adherence using the range of values of the sample. This percentage ranged from 100 (maximum adherence) to 0 (minimum adherence):
 $${\rm Adherence}\,({\rm percentage}_{{i}} )={{\left( {\mathop{\sum}{Z_{{i}} {\minus}} {\sum}\,Z_{{\min }} } \right)} \over {\left( {\mathop{\sum}{Z_{{{\rm max}}} {\minus}} {\sum}\, Z_{{\min }} } \right)}}{\times}100.$$
$${\rm Adherence}\,({\rm percentage}_{{i}} )={{\left( {\mathop{\sum}{Z_{{i}} {\minus}} {\sum}\,Z_{{\min }} } \right)} \over {\left( {\mathop{\sum}{Z_{{{\rm max}}} {\minus}} {\sum}\, Z_{{\min }} } \right)}}{\times}100.$$
Once the percentage of adherence to the MD was calculated, the variables that could determine a higher or lower adherence were assessed.
Statistics
Statistical analyses were performed using the statistical software package IBM SPSS Statistics for Windows, version 21·0. Mean adherence and its standard deviation were calculated. Quintile values of adherence to the MD were calculated, as previously described( Reference Bibiloni, Martínez and Llull 20 ), in order to find the group of the population with the lowest adherence percentage (percentage below the lower quintile value: <52·1 % among FF consumers and <51·5 % among FF non-consumers) and those with the highest adherence percentage (percentage above the upper quintile value: >61·0 % among FF consumers and >59·7 % among FF non-consumers). Differences in mean adherence between FF consumers and non-consumers, and in mean intakes of FF and functional dietary components by FF consumers according to low and high adherence to the MD, were tested by ANOVA. Logistic regression models were used to calculate differences in the sociodemographic and lifestyle variables between the groups with lowest and highest adherence (in order to assess which variables better determined a high or low adherence), among consumers and non-consumers of FF. Crude and adjusted odds ratios and 95 % confidence intervals were calculated. To adjust the odds ratios all variables were entered simultaneously into the model in order to account for the effects of all other covariates. Spearman’s rank correlation coefficient (ρ) was used to study the correlation between consumption of FF and functional dietary component intakes. The level of significance was established at P<0·05.
Results
Under-reporters (n 246) and over-reporters (n 24) were excluded from the analysis of dietary patterns in order to avoid respondent bias usually present in recall dietary methods. A total of 992 adolescents (59 %) reported FF consumption and 699 adolescents (41 %) consumed none of the FF.
Figure 1(a) shows the distribution of percentage adherence to the MD among FF consumers. The mean adherence of FF consumers was 56·42 (sd 6·05) % and the median adherence of FF consumers was 56·07 %. Figure 1(b) shows the distribution of percentage adherence to the MD among FF non-consumers. The mean adherence of FF non-consumers was 55·76 (sd 5·41) % and the median adherence of FF non-consumers was 55·17 %.
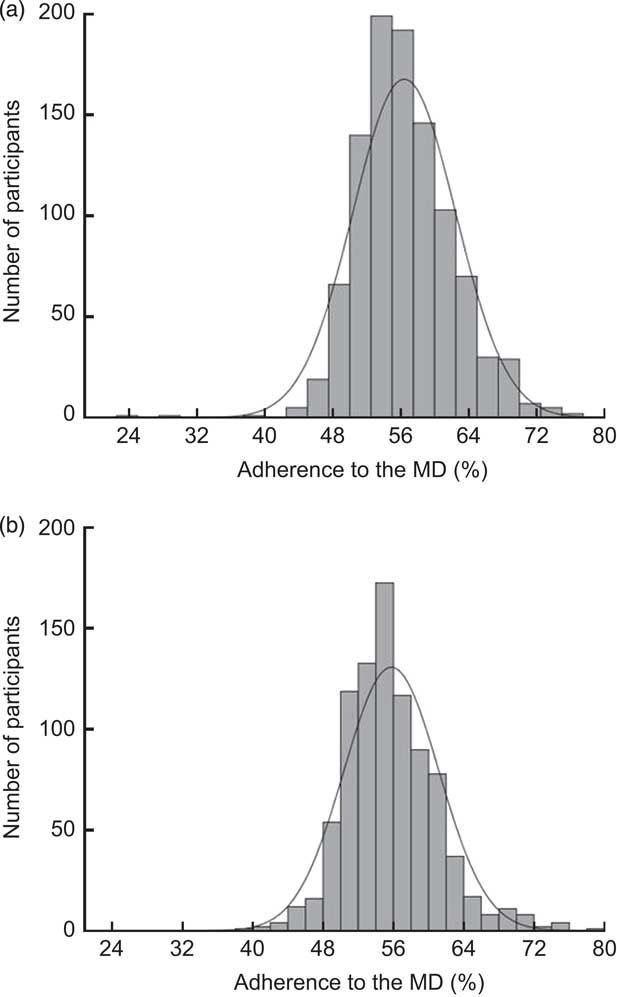
Fig. 1 Distribution of percentage adherence to the Mediterranean diet (MD) according to consumption of functional foods, (a) consumers (n 992) and (b) non-consumers (n 699), among a representative sample of Balearic Islands’ adolescents aged 12–17 years, 2007–2008
Means and standard deviations of percentage adherence to the MD according to sociodemographic and lifestyle factors of FF consumers and non-consumers are shown in Table 1. Among FF consumers and also non-consumers, girls had a significantly higher percentage adherence to the MD than did boys. In the comparison of girls, girls who consumed FF had a significantly higher percentage MD adherence than did non-consumer girls. While percentage of adherence to the MD increased significantly with age among FF consumers, among non-consumers adherence to the MD was not significantly associated with age. Education level of the mother was found to be associated with MD adherence in FF consumers and non-consumers. Non-consumers of FF whose mother had a low level of education had a significantly higher risk to have low adherence to the MD. Percentage adherence to the MD of FF consumers whose father had a medium education level was significantly higher than that of non-consumers whose father had medium level of education. Lower work status of the father and mother was associated with lower adherence to the MD among FF non-consumers. While underweight adolescents who consumed FF had a higher risk to have low MD adherence, the opposite trend was observed among FF non-consumers. High physical activity and having a chronic disease were not significantly associated with low risk of adherence to the MD in FF consumers and non-consumers.
Table 1 Percentage of adherence to the Mediterranean diet (MD) and risk of a low adherence according to sociodemographic and lifestyle variables and consumption of functional foods (FF) among a representative sample of Balearic Islands’ adolescents aged 12–17 years, 2007–2008

Ref., reference category.
* Odds ratio was significantly different from 1·00 (P<0·05).
† Low adherence was defined as a percentage of MD adherence below the lower quintile (52·1 %); high adherence was defined as a percentage of MD adherence above the upper quintile (61·0 %).
‡ Low adherence was defined as a percentage of MD adherence below the lower quintile (51·5 %); high adherence was defined as a percentage of MD adherence above the upper quintile (59·7 %).
§ Odds ratios were adjusted for age and sex.
|| Differences between FF consumers and non-consumers.
¶ Education level of parents: low, <6 years, medium, 6–12 years, high, >12 years.
†† Chronic diseases include diabetes, overweight, cholesterol, coeliac disease, lactose intolerance and other chronic diseases.
FF consumption (g/d) and intakes of functional dietary components of FF consumers according to low and high adherence to the MD are shown in Table 2. As expected, consumption of fruit juice, fibre-rich bread/cookies, cereal bars, fish and soya milk was higher in adolescents with high adherence to the MD, while consumption of modified milk (skimmed/semi-skimmed milk, milk with added n-3), probiotics, breakfast cereals and infusions was higher in adolescents with low adherence to the MD. Moreover, daily mean intakes of functional dietary components from plant-origin foods, like dietary fibre, vitamin C, vitamin E, carotene and folic acid, were significantly higher in adolescents with high adherence to the MD. The average intakes of Se, vitamin C, K, niacin and pantothenic acid met the RDI in both groups, whereas intake of vitamin E met the RDI only in FF consumers who had high MD adherence. While adequate intakes of Zn and n-3 fatty acids were observed among FF consumers with low adherence to the MD, intakes of other functional components were lower than the RDI value in both groups.
Table 2 Average daily intakes of functional foods (FF) and functional dietary components by FF consumers (n 992) according to low and high adherence to the Mediterranean diet (MD) in a representative sample of Balearic Islands’ adolescents aged 12–17 years, 2007–2008

nc, no consumption.
Mean values were significantly different from those of FF consumers with low MD adherence (one-way ANOVA): *P<0·05, **P<0·01, ***P<0·001.
† High adherence was defined as a percentage of MD adherence above the upper quintile (61·0 %).
‡ Low adherence was defined as a percentage of MD adherence below the lower quintile (52·1 %).
§ Skimmed/semi-skimmed milk, milk with added n-3.
|| Coffee and tea.
¶ RDI, Recommended Dietary Intake( Reference Ortega, López and Marcos 35 , 38 ).
The Spearman correlation analysis between the consumption of FF and intakes of functional dietary components is shown in Table 3. Consumption of FF except modified milk, infusions, cereal bars and soya milk were found to be positively associated with the intake of many functional components. Especially, statistically significant positive associations were observed between consumption of fruit juice and intakes of dietary fibre, Se, vitamin E, vitamin C, carotene, n-3 and n-6 fatty acids, and K.
Table 3 Spearman correlation coefficients (ρ) between the intakes of functional foods (FF) and functional dietary components among FF consumers (n 992) in a representative sample of Balearic Islands’ adolescents aged 12–17 years, 2007–2008

Correlation was significant: *P<0·05; ** P<0·01.
As expected, there was a positive correlation between the consumption of modified milk and probiotics and Ca intake. Besides this, consumption of modified milk was negatively associated with intakes of n-3 and n-6 fatty acids, whereas consumption of probiotics was positively related with intakes of these fatty acids. Intake of dietary fibre was found to be inversely associated with the consumption of breakfast cereals and also cereal bars, while the consumption of fibre-rich bread/cookies was positively associated with the intake of dietary fibre.
Discussion
In the present study we assessed differences in adherence to the MD between FF consumers and non-consumers and then represented the intakes of FF foods and functional dietary components by FF consumers according to low and high adherence to the MD.
The traditional MD has been identified as a healthy diet( Reference Trichopoulou, Kouris-Blazos and Wahlqvist 50 , Reference Belahsen and Rguibi 52 ) and consumption of FF is related to a healthy diet. We observed that both populations (FF consumers and non-consumers) had moderate adherence to the MD, but FF consumers showed a slightly higher MD adherence than non-consumers.
Gender was a significant factor that affected the risk of low adherence to the MD; boys had higher risk to have low adherence to the MD than did girls. These findings are in agreement with previous studies that showed higher adherence to the MD among girls than among boys( Reference Martínez, Llull and Bibiloni 18 , Reference Kontogianni, Vidra and Farmaki 19 ). Female adults are usually more interested in healthy eating( Reference Johansson, Thelle and Solvoll 53 ); however, what healthy eating means for female adolescents (weight loss and appearance) should be also considered( Reference Croll, Neumark-Sztainer and Story 54 ).
Age was found as another important factor for adherence to the MD in FF consumers: the youngest adolescents had significantly higher risk to have lower MD adherence than did older adolescents. Similarly, it was reported using KIDMED( Reference Kontogianni, Vidra and Farmaki 19 ) that Greek children had lower adherence to the MD than did Greek adolescents.
Parental education level was found not to be associated with MD adherence in FF consumers, while low education level of parents, especially the mother, was related with low adherence to the MD in FF non-consumers. Positive associations between parents’ education level and healthy diet quality of children and adolescents were previously reported( Reference Xie, Gilliland and Li 55 , Reference Patrick and Nicklas 56 ). Similarly, socio-economic status of parents was also an important parameter that affected the diet quality( Reference Patrick and Nicklas 56 ). While in FF consumers parents’ socio-economic status was not associated with adherence to the MD, in FF non-consumers low adherence to the MD was associated with medium and low level of parental socio-economic status. Moreover, many of the components of the MD cost more than components of a Western diet, which caused Spanish university students to switch to a Westernized diet( Reference Lopez, Martinez-Gonzalez and Sanchez-Villegas 57 ).
We found that underweight adolescents who consumed FF had lower adherence to the MD; however, in non-FF consumers, overweight adolescents were more likely to have lower adherence to the MD. Normal-weight, overweight or obese adolescents who consumed FF had similar adherence to the MD. Similar to our results, others have also observed( Reference Farajian, Risvas and Karasouli 21 ) no difference in adherence between normal-weight and overweight children to the MD; however, some other studies reported an inverse association between BMI and adherence to the MD in children( Reference Lazarou, Panagiotakos and Matalas 58 ) and also adults( Reference Schröder, Marrugat and Vila 13 , Reference Rossi, Negri and Bosetti 59 ). It was previously reported( Reference Schröder, Marrugat and Vila 13 ) that a higher BMI was associated with a lower MD adherence in adults. On the other hand, because the MD is a carbohydrate-rich diet, researchers have questioned that it might be a cause of obesity, the metabolic syndrome and its complications( Reference Contaldo, Scalfi and Pasanisi 60 ); however, the important point is that in the traditional MD unrefined cereals and cereal products rich in dietary fibre are the main source of carbohydrate and sugar consumption is very low( Reference Trichopoulou, Costacou and Christina 4 ). Moreover, many studies have reported that a Mediterranean dietary pattern is not associated with overweight and weight gain( Reference Schröder, Marrugat and Vila 13 , Reference Rossi, Negri and Bosetti 59 ).
Physical activity along with a healthy diet plays an important role in health status( Reference Astrup 61 ) and physically active Greek children were found have higher adherence to the MD( Reference Bibiloni, Martínez and Llull 20 , Reference Lazarou, Panagiotakos and Matalas 58 ); however, we did not observe any association between physical activity status and MD adherence in our population of Balearic Islands’ adolescents.
Average daily intakes of many FF and functional dietary components were found to be higher among adolescents with high adherence to the MD than among those with low MD adherence. The traditional Balearic diet is one of the examples of an MD( Reference Tur, Romaguera and Pons 16 , Reference Martínez, Llull and Bibiloni 18 ) and offers several unprocessed FF and functional dietary components like unrefined cereals and cereal products, fruits and vegetables rich in antioxidants, vitamins, minerals and phytochemicals( Reference Gaskins, Rovner and Mumford 62 , Reference Kavouras, Panagiotakos and Pitsavos 63 ). Wholegrain cereals and cereal products were considered as FF in the current study due to the high dietary fibre content of wholegrain cereal( Reference Schröder 14 ). Both soluble and insoluble dietary fibre play an important role in satiety and energy metabolism( Reference Schröder 14 ), and it was reported that high intake of wholegrain foods might reduce the risk of heart disease, type 2 diabetes and various types of cancer( Reference Schröder 14 , Reference de Munter, Hu and Spiegelman 64 – Reference La Vecchia 66 ). Moreover, whole grains contain bran and germ, which are rich in micronutrients and phytochemicals( Reference de Munter, Hu and Spiegelman 64 ). Fruit juices were also considered as FF due to their high content of vitamins and also dietary fibre. Diets rich in fruits and vegetables are associated with a reduced risk of heart disease and a lower risk of obesity( Reference Tamers, Agurs-Collins and Dodd 67 , Reference Riediger, Shooshtari and Moghadasian 68 ). Bes-Rastrollo et al.( Reference Bes-Rastrollo, Martínez-González and Sánchez-Villegas 69 ) indicated that fruit and vegetable consumption helps to avoid weight gain due to the high fibre content of these foods. Also the US Food and Drug Administration reported that consumption of fibre-rich foods like cereals or fruits and vegetables with a low-fat diet might reduce the risk of some types of cancer and furthermore that the intake of soluble fibre might reduce the risk of heart disease( Reference Hasler 42 ). Moreover, fruits and vegetables provide micronutrients such as carotenoids, vitamin E, ascorbic acid and polyphenols, known for their antioxidant effect( Reference Kavouras, Panagiotakos and Pitsavos 63 , Reference La Vecchia 66 ).
As expected, consumption of FF such as low-fat or skimmed milk and probiotics was higher among adolescents with low adherence to the MD, due to low to moderate intake of milk and milk products being characteristic of a traditional MD( Reference Trichopoulou, Costacou and Christina 4 ).
Intakes of functional dietary components like vitamin E, vitamin C, carotene and dietary fibre were significantly higher among adolescents with high adherence to the MD. Similarly, it was reported( Reference Bach-Faig, Geleva and Carrasco 70 ) that higher adherence to the MD was positively associated with plasma concentrations of β-carotene, folate, vitamin C and α-tocopherol. On the other hand, inadequate intakes of many functional dietary components were observed among FF consumers with low and high adherence to the MD in the Balearic Islands. Inadequate intakes of Zn and carotene also among the adult population in the Balearic Islands was reported; nevertheless, intakes of Se, vitamin E and vitamin C – which act as antioxidants – were above recommendations( Reference Tur, Serra-Majem and Romaguera 71 ).
In the MD the main source of fat intake is olive oil, which is low in saturated and n-6 fatty acids but high in plant monounsaturated fat( Reference Simopoulos 72 ). In line with this, we found that intake of n-6 fatty acids was low in FF consumers with low and also high adherence to the MD; however, intake was lower than RDI value( Reference Llull, Bibiloni and Martínez 73 ). In addition to n-6 fatty acids, intake of n-3 fatty acids was inadequate in FF consumers with high adherence to the MD. It should be considered that the intake of n-3 fatty acids in the present study represented only the intake of linolenic acid, which is an ‘essential fatty acid’ because the human body cannot synthesize it( Reference Hasler 42 , Reference La Vecchia 66 ), and we did not represent intakes of other n-3 fatty acids (EPA and DHA) of which fish is the main source. Daily amount of fish consumption in Spain is one of the highest in the world( Reference Serra-Majem, de la Cruz and Ribas 74 ) and in our study we observed that adolescents consumed about 30 g of fish daily. So, total n-3 fatty acid intake might meet the RDI value by accounting for daily fish consumption.
While consumption of most of the FF had a positive association with the intake of many functional dietary components, consumption of cereal bars and soya milk was found to be inversely associated with many functional dietary component intakes. Cereal bars are sweetened with sugar and also contain a high amount of fat( Reference Woods and Walker 75 ); they might be consumed as snacks and thus might increase energy intake.
As is seen in the correlations between consumption of FF and intakes of functional dietary components, food and nutrient intakes have complex interactions and instead of examining the role of single nutrients or foods in disease risk, investigation of the whole diet accounts for the synergistic and antagonistic effects of foods and nutrients on health( Reference Martinez-Gonzalez and Estruch 9 ). Although FF offer a new kind of health message by promising specific effects caused by particular food components( Reference Doyon and Labrecque 76 ), the MD as a complex dietary pattern with a large variety of food choice provides several FF without recurring to food industry products; however, intakes of many functional dietary components like carotene, Zn, n-3 fatty acids and dietary fibre, which are important components of the MD, were found to be inadequate. High adherence of adolescents to the MD might improve the intakes of these nutrients. Parents should be aware of this and follow the MD to serve as a model for their children.
Finally, it is interesting to note that the adolescent population is particularly difficult to investigate and susceptible to mistakes in eating habits. The results obtained may be relevant to this topic and also deepen understanding of adolescents’ food-based dietary patterns.
Conclusions
The population of adolescents in the Balearic Islands had moderate adherence to the MD and higher adherence was observed among FF consumers. Average daily intakes of FF and functional dietary components were higher among adolescents with high adherence to the MD than among those with low MD adherence. Gender, age and low parental education were risk factors of low adherence to the MD, mainly among FF non-consumers.
Acknowledgements
Financial support: The study was supported by the Spanish Ministry of Health and Consumption Affairs (Programme of Promotion of Biomedical Research and Health Sciences, Projects 05/1276, 08/1259 and 11/01791, Red Predimed-RETIC RD06/0045/1004 and CIBERobn CB12/03/30038); Grant of support to research groups no. 35/2011 (Balearic Islands Government and EU FEDER funds); and the Spanish Ministry of Education and Science (FPU Programme, PhD fellowship to M.d.M.B.). The Research Group on Community Nutrition and Oxidative Stress, University of Balearic Islands belongs to the Centre Català de la Nutrició (IEC) and Exernet Network. The funders had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: A.E.O. and J.A.T. conceived, designed and devised the study; M.d.M.B. collected and supervised the samples; A.E.O., M.d.M.B., M.M.A. and J.A.T. analysed the data and wrote the manuscript; J.A.T. supervised the study; A.P. and J.A.T. obtained funding. All authors read and approved the final manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Balearic Islands’ Ethics Committee (Palma de Mallorca, Spain).




