


International health guidelines recommend adolescents to engage in 60 min or more of moderate-to-vigorous physical activity (MVPA) each day(1). Regular physical activity (PA) in adolescents is related to beneficial health outcomes during adolescence(1, Reference Biddle, Gorely and Stensel2) and adulthood(1). However, previous studies using objective and subjective assessment methods revealed that the majority of adolescents are not sufficiently active(Reference Pearson, Atkin and Biddle3, Reference Currie, Nic Gabhainn and Godeau4). As a result, the promotion of PA in adolescent populations has become an international health concern.
Recent reviews have revealed socio-economic inequalities in PA, showing that adolescents with lower socio-economic status (SES) are less physically active than those with higher SES(Reference Hanson and Chen5, Reference Stalsberg and Pedersen6). In order to overcome these socio-economic differences, information is needed about the factors influencing the relationship between SES and PA in adolescents. At present, little is known about the underlying mechanisms of this association. One Canadian study, using focus groups, revealed that environmental factors are very important for adolescents with low SES to engage in PA, while intrapersonal and social factors are essential among both high- and low-SES adolescents(Reference Humbert, Chad and Spink7). To our knowledge, no other qualitative or quantitative studies have investigated the factors influencing socio-economic differences in adolescents’ levels of PA. Therefore, the aim of the present study was to conduct an in-depth analysis of the SES–PA association in adolescents.
Data collected during the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study(Reference Moreno, González-Gross and Kersting8) provide the opportunity to examine the SES–PA association more thoroughly. The HELENA cross-sectional study, conducted in ten European cities in nine different countries, revealed different self-reported PA patterns according to gender, age, weight status and SES in adolescents aged 12·5 to 17·5 years(Reference De Cocker, Ottevaere and Sjöström9). As well as these demographic and biological variables, other traditional correlates of physical activity, i.e. psychosocial factors(Reference Sallis, Prochaska and Taylor10, Reference Van Der Horst, Paw and Twisk11) including stage of change, attitudes, awareness, modelling, social support, self-efficacy, benefits and barriers, and environmental correlates of PA, were also investigated. The present study examined to what extent SES differences in these theoretical psychosocial factors account for SES variations in PA. SES was already found to be associated with attitudes and beliefs about healthy lifestyles(Reference Wardle and Steptoe12). Therefore it is hypothesized that SES may contribute to inequalities in psychosocial correlates of physical activity, which in turn influence physical activity levels. In addition, previous research in Australian adolescents regarding another health behaviour, namely diet, already revealed that individual, social and environmental factors were strong mediators of SES inequalities in eating behaviour(Reference Ball, MacFarlane and Crawford13). Consequently, the objective of the present study was to investigate the potential mediating role of psychosocial correlates of PA on the relationship between SES and PA in European adolescents participating in the HELENA Study.
Methods
Study design, procedure and participants
The original objective of the HELENA Study was to collect data on nutritional status and lifestyle across a random sample of European adolescents using the same methodology (i.e. strict standardization of the fieldwork) in ten city centres(Reference De Henauw, Gottrand and De Bourdeaudhuij14, Reference Moreno, De Henauw and González-Gross15). Details on the study design and sampling procedures can be found elsewhere(Reference Moreno, De Henauw and González-Gross15).
In brief, adolescent boys and girls aged 12·5 to 17·49 years in ten European cities (see Table 1) formed the basis for a random cluster sampling of adolescents stratified by geographical location, age and SES. Adolescents were recruited through schools and questionnaires were handed out during classes and filled in immediately. A signed informed consent form was obtained from both the adolescents and the parents. Study protocols were approved by the Ethical Committee of each centre involved(Reference Béghin, Castera and Manios16).
Table 1 Sample size by gender, age category and city/country used in the weighted analyses, and the prevalence of low SES indicators; the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study
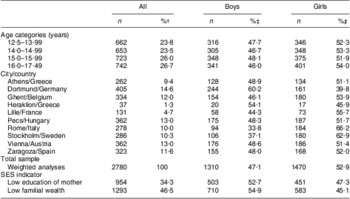
SES, socio-economic status.
†Percentage values expressed in relation to the total sample.
‡Percentage values expressed in relation to each age category, city or SES group.
A total of 3051 adolescents completed at least 75 % of the PA questionnaire (= inclusion criterion in the HELENA Study)(Reference Moreno, De Henauw and González-Gross15), 3390 completed at least 75 % of the SES questions and 3241 completed at least 75 % of the questionnaire concerning correlates of PA. The sample providing sufficient information on all three measures (PA, SES and correlates of PA) consisted of 2780 adolescents (79 % of originally recruited adolescents). During analyses, the data were adjusted by a weighting factor to balance the sample according to the theoretical age and gender distribution of the European adolescent population. The weighted sample size by gender, age category and city of this final adolescent group can be found in Table 1.
Measures
Outcome measure: physical activity
To assess PA of the last 7 d, an adolescent-adapted version (IPAQ-A) of the International Physical Activity Questionnaire (IPAQ), self-administered and long version, was used. The original valid and reliable questionnaire was developed for adults aged 18–65 years, assessing PA in four different domains (work; transport; house and garden; leisure time)(Reference Craig, Marshall and Sjöström17). To adapt the questionnaire to an adolescent study population, questions about PA at work were replaced by questions about PA at school, namely physical education, walking and moderate and vigorous PA at school. Furthermore, the item relating to domestic and gardening PA was reduced to one question. A validation study on this instrument showed significant modest correlations (≅0·20) between activities of different intensities and total PA reported in the questionnaire and PA measured by accelerometry(Reference Hagströmer, Bergman and De Bourdeaudhuij18). Following methods of a previous study(Reference De Cocker, Ottevaere and Sjöström9), min/week were computed for total PA (summation of PA at school, during transport, at home and during leisure time) and MVPA (summation of moderate and vigorous PA). It was decided to use these two outcome variables as the correlates concerned PA and sports in general, and not domain-specific PA.
Predictor measures: education of mother and Family Affluence Scale
Health-related aspects are commonly affected by the mother's level of education. Adolescents reported the educational level of their mother by indicating whether their mother had a lower, lower secondary, higher secondary or higher/university education. This 4-point scale was re-coded into a dichotomized 2-point scale(Reference Von Rueden, Gosch and Rajmil19): ‘0 = low education’ (lower and lower secondary); ‘1 = high education’ (higher secondary and higher/university degree; see Table 1).
A modified version of the Family Affluence Scale (FAS) index of Currie et al., used in the Health Behaviour in School-aged Children Study(Reference Currie, Molcho and Boyce20), was used in the present study. The original FAS index (family car ownership, having one's own bedroom, family holidays and family computer ownership) was found to be a valid indicator of adolescents’ SES and material circumstances(Reference Currie, Molcho and Boyce20). However, as a cross-sectional child–parent validation study of the original FAS later showed low percentage agreement for family holidays and suggested to replace the family holiday item(Reference Andersen, Krolner and Currie21), it was decided to include Internet availability instead of family holidays. Internet use considers current technological developments and was found to be closely related to SES(Reference Wangberg, Andreassen and Prokosch22). Consequently, in the present study, adolescents reported on their personal and sociodemographic variables, including family car ownership, whether the adolescent has his/her own bedroom, whether Internet is available at home and the family's computer ownership. The scale ranged from 0 to 8 and was re-coded and dichotomized into a 2-point scale: ‘0 = low familial wealth’ (index score = 0–4); ‘1 = high familial wealth’ (index score = 5–8; see Table 1).
A pilot HELENA cross-sectional study showed that the socio-economic and parental questionnaire items caused no problems and were completed by at least 85 % of the adolescents(Reference Iliescu, Béghin and Maes23).
Potential mediators: psychosocial correlates of physical activity
Different correlates of PA were assessed using forty-one items. Questions were selected and adopted from previous studies with adolescents(Reference De Bourdeaudhuij, Philiippaerts and Crombez24) and adults(Reference De Bourdeaudhuij and Sallis25). Stage of change (two items: ‘Are you physically active for at least one hour each day?’ and ‘Do you have the intention to do at least one hour of PA each day?’) towards PA was measured and expressed as: ‘1 = not physically active and no intention to become active’; ‘2 = not physically active, but having the intention to become active within six months’; ‘3 = not physically active, but having the intention to become active within one month’; ‘4 = being physically active, but no longer than six months’; and ‘5 = physically active for more than six months’. Attitudes (two items) towards PA (‘I like to do sports and PA’ and ‘Being physically active is healthy’) were measured using a 5-point ordered response scale (‘completely disagree’ to ‘strongly agree’). To assess awareness (two items), adolescents completed the questions ‘Do you think you are very physically active or not?’ (5-point scale: ‘very little’ to ‘very much’) and ‘Do you think that you should be physically active for one hour each day?’ (5-point scale: ‘certainly not’ to ‘certainly yes’). Modelling (five items) from the adolescent's mother and father, brothers and sisters, and best friend was measured by asking adolescents how regularly these relatives were physically active (5-point scale: ‘never’ to ‘(almost) daily’). Social support (five items) was assessed by asking adolescents how often their parents, siblings and best friend encouraged them to be physically active (5-point scale: ‘not at all’ to ‘very often’). Self-efficacy (four items) was measured by asking adolescents how hard it is to be active for at least one hour each day, how hard it is to be active at home, in their neighbourhood and during school breaks (5-point scale: ‘very hard’ to ‘not hard at all’). Perceived benefits (eight items) and barriers (six items) with regard to PA were investigated by asking adolescents to rate their agreement (5-point scale: ‘completely disagree’ to ‘strongly agree’) with possible benefits of PA (physical appearance, weight, fitness and health, social interaction, competition, stress and depression, admiration of others, relaxation from schoolwork) and barriers preventing them from being physically active (lack of time, lack of discipline, not skilled enough, too expensive, no transportation, fear of being laughed at). Finally, the agreement (‘completely disagree’ to ‘strongly agree’) with different environment correlates (seven items: possibility to be active at school during recess and lunch break, safeness to bike and walk to school, neighbourhood's traffic, availability of shops and facilities within walking distance, sports facilities, and open spaces) were investigated using a 5-point scale.
All different items were (re)coded in the same direction so that the highest scores were the most positive answers on each item (re-coding was necessary for the item about neighbourhood's traffic). Pearson correlation coefficients were calculated to test the reliability of scales with only two items (stage, attitude, awareness), while Cronbach's α coefficients of internal consistency were calculated for the other mediating variables’ scales with more than two items (see Table 2). Per potential mediator, the average of the different items (scores 1–5) was calculated and consequently expressed into the original 5-point ordered response scales.
Table 2 Main association tests, action theory tests and conceptual theory tests (controlled for age, gender, BMI and region); the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study
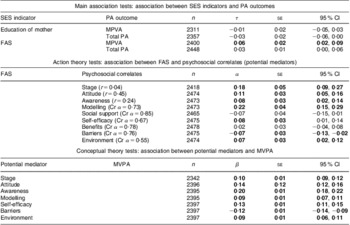
SES, socio-economic status; PA, physical activity; τ, estimate of unstandardized regression coefficient of association between SES indicator and PA outcome before adjustment for mediator; α, estimate of unstandardized regression coefficient of association between FAS and psychosocial determinants; β, estimate of unstandardized regression coefficient of association between potential mediators and MVPA; FAS, Family Affluence Scale; MVPA, moderate-to-vigorous physical activity; r, Pearson correlation coefficient; Cr α, Cronbach's α coefficient.
Boldface indicates statistically significant associations.
Anthropometric measures
As explained previously(Reference De Cocker, Ottevaere and Sjöström9), height and weight were measured in order to calculate the BMI of the adolescents.
Data analysis
Analyses were conducted using the SPSS for Windows statistical software package version 15·0 (SPSS Inc., Chicago, IL, USA). The data were adjusted by a weighting factor, according to the HELENA consortium, to ensure true representation of each of the stratified groups and to keep methods consistent through all HELENA study papers. Furthermore, clustering at the school level was taken into account by conducting multilevel analyses. Based on previous research with other(Reference Haerens, Deforche and Maes26) and the present(Reference De Cocker, Ottevaere and Sjöström9) adolescent samples using comparable questionnaires, the PA scores were truncated at reasonable and realistic levels (all values of 2540 min/week or more were replaced by 2540 min/week) to limit unrealistic high values. Next, the skewed scores of both total PA and MVPA were log-transformed (after changing 0 min into 0·1 min) to obtain normal distributions.
In the first stage of the analyses, the main associations between the SES indicator and the PA outcomes were tested using linear mixed-models analyses (main associations). When the SES indicator was shown to be a significant predictor of PA (total PA and MVPA), the second stage of the analyses was conducted for that particular SES indicator. In that second stage, the mediating role of the correlates of PA on the SES–PA association were tested using the product-of-coefficients test of MacKinnon(Reference MacKinnon, Fairchild and Fritz27). This test consists of different stages: (i) the action theory tests(Reference MacKinnon, Fairchild and Fritz27) which estimate the association between the SES indicators and the potential mediators (the different correlates of PA), resulting in α coefficients; (ii) the conceptual theory tests(Reference MacKinnon, Fairchild and Fritz27) which estimate the association between the potential mediators and the PA outcome, resulting in β coefficients for the mediators; (iii) the calculation of the product of the two coefficients (αβ), representing the mediating effect; and (iv) the calculation of dividing αβ by its standard error to assess the statistical significance of the mediating role. For the calculation of the standard error, the Sobel test(Reference Wangberg, Andreassen and Prokosch22, Reference Sobel28) was used: seαβ = √(α 2seβ 2+β 2seα 2). The obtained value of αβ/seαβ was then compared to a standard normal distribution(Reference MacKinnon, Fairchild and Fritz27).
Furthermore, the proportion mediating the association between the SES indicators and PA outcomes was estimated by dividing the product of coefficients (αβ) by the τ coefficient (regression coefficient for the association between SES indicators and PA before adjustment for the mediators). Finally, as well as single-mediator models, multiple-mediator models were assessed when several mediators influenced the SES indicator–PA association and when the summation of the proportion mediated of the single-mediator models exceeded 100 %.
As in the present HELENA adolescent sample PA levels were related to age, gender and BMI(Reference De Cocker, Ottevaere and Sjöström9), all analyses were adjusted for these variables. Region (two categories: north Europe with Sweden, Germany, Belgium, Austria and France; and south Europe with Hungary, Greece, Italy and Spain) was also included as a covariate in the linear regression models, as the data were collected in ten different cities throughout Europe. An α level of P < 0·05 was used to decide upon statistical significance.
Results
Main associations
The first stage of the analyses showed that the FAS was significantly and positively associated with MVPA (see Table 2). No significant association was found between the FAS and total PA. The education of the mother was not significantly associated with total PA or MVPA. As a result, only the mediating role of psychosocial correlates on the association between the FAS and MVPA was investigated.
Action theory tests
The associations between the FAS and the separate potential mediators are presented in Table 2. A significant and positive association was found between the FAS and stage of change, attitude, awareness, modelling and self-efficacy with regard to PA and environmental correlates of PA. A negative association was found between FAS and barriers of PA. Therefore, only these seven correlates were included as potential mediators in the following single-mediator models. The FAS was not significantly associated with social support and benefits with regard to PA.
Conceptual theory tests
When the potential mediators were included individually as additional predictor in the models examining the association between the FAS and MVPA, each correlate was shown to have a positive and significant association with MVPA, except barriers which were negatively associated with MVPA (see Table 2).
Mediating role
Results (product-of-coefficient estimate; statistical significance; proportion mediation) of the single-mediator models are presented in Table 3. Each psychosocial correlate, except attitude, had a significant mediating role on the FAS and MVPA association (see Table 3). This means that the FAS–MVPA association was mediated by these single correlates.
Table 3 Mediating role (controlled for age, gender, BMI and region) of psychosocial correlates on the association between FAS and MVPA; the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

FAS, Family Affluence Scale; MVPA, moderate-to-vigorous physical activity; SES, socio-economic status; αβ, product-of-coefficient estimate, mediated role.
Boldface indicates statistically significant mediation.
*0·01<P ≤ 0·05, **0·001<P ≤ 0·01, ***P ≤ 0·001.
The proportion mediated by the individual mediators ranged between 10·5 % and 33·0 % (see Table 3). The summation of these separate proportions exceeded 100 %. Consequently, a multiple-mediator model including all correlates simultaneously was conducted. The product-of-coefficients (αβ), representing the multiple-mediated role, was 0·031 (se 0·005, t = 6·2, P < 0·001) with a 95 % CI of 0·005, 0·021. The proportion mediated in this multiple-mediator model was 51·7 %.
The independent mediating role of each mediator resulting from the multiple-mediation models is represented in Table 4. Stage of change, awareness and modelling had a unique contribution to the explanation of the FAS–MVPA relationship.
Table 4 Independent mediating role (controlled for age, gender, BMI and region) of each mediator resulting from multiple-mediation models on the association between FAS and MVPA; the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study

FAS, Family Affluence Scale; MVPA, moderate-to-vigorous physical activity; SES, socio-economic status; αβ, product-of-coefficient estimate, mediated role.
Boldface indicates statistically significant mediation.
*0·01<P ≤ 0·05, ***P ≤ 0·001.
Some authors(Reference Cerin and MacKinnon29) suggest to examine potential mediating effects even in the absence of a significant association between the independent and outcome variable. These analyses (data not fully shown) revealed three potential mediators of the (non-significant negative) association between education of the mother and MVPA, namely self-efficacy (α = –0·11, se 0·04; 95 % CI −0·18, −0·04), attitude (α = 0·07, se 0·03; 95 % CI 0·01, 0·13) and benefits (α = 0·15, se 0·03; 95 % CI 0·08, 0·21). Self-efficacy (αβ = −0·014, se 0·005; 95 % CI −0·025, −0·004) was a significant mediator of the association between education of the mother and MVPA, while attitude (αβ = 0·010, se 0·004; 95 % CI 0·001, 0·018) and benefits (αβ = 0·015, se 0·003; 95 % CI 0·008, 0·022) had a suppressor effect.
Discussion
The present study aimed to explore the mechanisms through which SES differences in PA in European adolescents remain. Current results showed that FAS-related social inequalities in MVPA are mediated by certain correlates of PA, namely stage of change, awareness, modelling, self-efficacy, barriers and environmental factors. This means that adolescents with low family wealth scored lower (higher for barriers) on these correlates of PA, which in turn resulted in lower levels of MVPA. This information is useful for the development of PA interventions in low-SES adolescent populations. The current findings suggest that targeting stage of change, awareness, modelling, self-efficacy, barriers and environmental factors will be a good approach to promote MVPA in adolescents with low family wealth.
Future interventions should include strategies that target both individual and environmental correlates of PA. For example, low-SES adolescents’ awareness of their PA level should be increased. Self-monitoring, for example by using a step counter, can be a strategy to increase awareness. Besides, a recent review showed that use of a step counter is an effective strategy to promote PA in this age group(Reference Lubans, Morgan and Tudor-Locke30). The role of family members (parents and siblings) and best friend of the adolescent is important too. Present results suggest that the role modelling is significant. As a result, the involvement of these individuals is recommended in future interventions. In contrast, the social support from parents, siblings and best friend was not significant. Another individual construct that should be targeted in low-SES adolescents is their self-efficacy. Strategies should increase the belief of adolescents in their own competence to be physically active each day, at home, in the neighbourhood and during school breaks. Finally, by offering certain types of PA, some barriers preventing low-SES adolescents from doing PA might be overcome; for example, activities that require no specific skills, which are inexpensive or can be done at home or school so that no transportation is needed. Cost and time were previously also found to be essential for low-SES adolescents to engage in PA(Reference Humbert, Chad and Spink7).
A second group of constructs that was found to be important are the environmental correlates of PA. Results suggest that adolescents should have the possibility to be active at school and walk or bike to school safely, that neighbourhood traffic should be limited, and that adolescents should have access to shops and facilities within walking distance and access to sports facilities and open spaces. Focus groups in adolescents of the same age already revealed that environmental factors are important among low-SES adolescents(Reference Humbert, Chad and Spink7). Agreement exists between the latter study and our research findings on proximity, facilities and safety.
A final construct which was found to be an important mediator was stage of change towards PA or the intention to become physically active. This construct is influenced by the previously mentioned individual and environmental correlates, so when interventions focus on these correlates, the intention to become physically active can also be affected. Additionally, future interventions can include specific strategies, e.g. by enhancing motivation, that increase the stage of change of low-SES adolescents.
An appropriate setting to address the individual and environmental factors found to be significant in the present study is the (community) school. Schools can organize the (health) educational part of the intervention, provide opportunities to be active at school, and promote active transport to and from school. Some might argue that school-based interventions will widen inequalities due to a higher effectiveness in higher-SES groups(Reference De Bourdeaudhuij, Simon and De Meester31). In contrast, it has recently been shown that European school-based interventions, combining educational and environmental interventions to promote PA, reached similar effects in low- and high-SES adolescents(Reference De Bourdeaudhuij, Simon and De Meester31). Moreover, if future interventions focus on the individual and environmental constructs found to be significant in the present study, social disparities might be narrowed. As modelling (next to stage of change and awareness) is a unique contributor to the SES–PA association, an additional family component could strengthen school-based interventions.
Current results suggested that it is less relevant to focus on social support when trying to diminish social inequalities in PA among adolescents, as SES was not associated with this construct here. However, in the focus groups of Humbert et al., low-SES adolescents reported that social support was essential to engage in PA(Reference Humbert, Chad and Spink7). Comparison with other studies was not possible as no other study has investigated the possible mechanisms through which SES differences in PA remain. This advocates for more research investigating the mediating role of psychosocial correlates of PA or other determining factors on the relationship between SES and PA in adolescents.
The current study has some limitations that need to be mentioned. First, data on the outcome measures were self-reported by the adolescents. The validity of the self-reports on PA can be threatened by cognitive (e.g. recall bias) and situational (e.g. social desirability bias) factors(Reference Brener, Billy and Grady32). However, the IPAQ-A has reasonable validity properties for assessing activities in different intensities and for total PA in this sample(Reference Hagströmer, Bergman and De Bourdeaudhuij18). A second point that needs attention is the choice of the SES indicator. As there is no consensus on SES indication, a variety of different measures of adolescent SES have been used in the literature; for example, education, occupation and income of the parents, neighbourhood-related measures or family's available material resources(Reference Stalsberg and Pedersen6, Reference Currie, Molcho and Boyce20, Reference Federico, Falese and Capelli33, Reference Gracia-Marco, Tomas and Vicente-Rodriguez34). Here, it was chosen to use education of the mother and the FAS, as was done in another recent European study in adolescents(Reference Von Rueden, Gosch and Rajmil19). In the present study, the FAS was associated with MVPA, but the education of the mother showed no significant relationship with PA. This latter result could be expected, as a previous study in this European adolescent sample found only trivial differences in school-based, home-based, leisure-time, moderate and vigorous PA between adolescents whose mother had a low and high education(Reference De Cocker, Ottevaere and Sjöström9). However, also mediation analyses were conducted for this non-significant negative association(Reference Cerin and MacKinnon29). The association between education of the mother and self-efficacy was negative, which was not the case for the FAS. However, as the main association between education of the mother and MVPA was also negative, self-efficacy was found to be a significant mediator, which is similar to the other SES variable. Furthermore, two suppressors of the maternal education–MVPA association were found: education of the mother had an indirect positive ‘impact’ on MVPA through attitudes and benefits. These two latter constructs were of no significance in the FAS–MVPA association. Third, also the precise data on PA should be taken in mind, i.e. type, contexts or domains, frequency, duration and intensity of activity(Reference Stalsberg and Pedersen6, Reference Gracia-Marco, Tomas and Vicente-Rodriguez34, Reference Salmon, Timperio and Cleland35). Here for example, the FAS was significantly associated with MVPA but not with total PA. The fact that the FAS was negatively associated with walking in the present study sample(Reference De Cocker, Ottevaere and Sjöström9) probably explains why no association was found here between the FAS and total PA, including walking. In an adult population, individuals living in low-SES areas were also less likely to undertake vigorous activity, while they were more likely to walk for transport(Reference Giles-Corti and Donovan36). In addition, a potential selection bias should be considered as only healthy adolescents were considered to be eligible during the HELENA Study. Furthermore, only those completing questions about PA, correlates of PA and SES were included for the present analysis, which could also lead to over- or under-sampling of specific groups. Finally, reliability or validity estimates are missing for some variables. No information is available on the reliability of the SES indicators, and the scale constructs (potential mediators) were tested rather for reliability and not for validity. For some scales’, reliability levels were low; however, this did not systematically affect the potential mediating role of the construct.
The main strength of the present paper is the fact that this is probably the first quantitative study examining the underlying mechanisms of the SES–PA association among adolescents. As the interest in the effect of SES on health (behaviours) is high, and the reduction and prevention of socio-economic inequalities in health behaviours, including PA, are among the main concerns of public health policy in Europe today(Reference van Lenthe, De Bourdeaudhuij and Klepp37, Reference Richter, Erhart and Vereecken38), the present results are useful to reduce social inequalities in PA. Future studies might consider similar analyses to examine the association between SES and other health behaviours, such as eating habits, smoking, sedentary behaviour (e.g. television viewing) or alcohol consumption(Reference van Lenthe, De Bourdeaudhuij and Klepp37, Reference Richter, Erhart and Vereecken38). Other strengths are the large sample size and inclusion of up to ten cities in nine different countries in the present study.
Conclusion
The present results showed that the association between SES and MVPA in European adolescents is mediated by both individual and environmental correlates of PA. Consequently, interventions should focus on these constructs, in order to overcome social inequalities in PA behaviours among adolescents.
Acknowledgements
Sources of funding: The HELENA Study took place with the financial support of the European Community Sixth RTD Framework Programme (Contract FOOD-CT: 2005-007034). The ALPHA-project in the framework of the Public Health Programme (2006120) also supported this study. The content of this paper reflects the authors’ views only and the European Community is not liable for any use that may be made of the information contained herein. Conflict of interest: There are no potential, perceived or real conflicts of interest related to the research reported in the manuscript. All authors agree with the content of the manuscript and no author has interest that might be interpreted as influencing the research. Authors’ contributions: K.D.C. wrote the first draft of the manuscript and led the writing of the paper. K.D.C. and I.D.B. contributed to the conception and designing of the study, the statistical analyses and interpretation of the data. E.G.A., S.D.H., S.D., F.G., L.B., M.H., M.S., M.P., Y.M., B.M., D.M., L.M., C.O., J.V., L.M. and I.D.B. contributed to the study conception and provided substantial feedback on the manuscript.
Appendix
HELENA Study Group
Co-ordinator: Luis A. Moreno.
Core Group members: Luis A. Moreno, Frédéric Gottrand, Stefaan De Henauw, Marcela González-Gross, Chantal Gilbert.
Steering Committee: Anthony Kafatos (President), Luis A. Moreno, Christian Libersa, Stefaan De Henauw, Jackie Sánchez, Fréderic Gottrand, Mathilde Kersting, Michael Sjöstrom, Dénes Molnár, Marcela González-Gross, Jean Dallongeville, Chantal Gilbert, Gunnar Hall, Lea Maes, Luca Scalfi.
Project Manager: Pilar Meléndez.
Universidad de Zaragoza (Spain): Luis A. Moreno, Jesús Fleta, José A. Casajús, Gerardo Rodríguez, Concepción Tomás, María I.Mesana, Germán Vicente-Rodríguez, Adoración Villarroya, Carlos M. Gil, Ignacio Ara, Juan Revenga, Carmen Lachen, Juan Fernández Alvira, Gloria Bueno, Aurora Lázaro, Olga Bueno, Juan F. León, Jesús Ma Garagorri, Manuel Bueno, Juan Pablo Rey López, Iris Iglesia, Paula Velasco, Silvia Bel.
Consejo Superior de Investigaciones Científicas (Spain): Ascensión Marcos, Julia Wärnberg, Esther Nova, Sonia Gómez, Esperanza Ligia Díaz, Javier Romeo, Ana Veses, Mari Angeles Puertollano, Belén Zapatera, Tamara Pozo.
Université de Lille 2 (France): Laurent Béghin, Christian Libersa, Frédéric Gottrand, Catalina Iliescu, Juliana Von Berlepsch.
Research Institute of Child Nutrition Dortmund, Rheinische Friedrich-Wilhelms-Universität Bonn (Germany): Mathilde Kersting, Wolfgang Sichert-Hellert, Ellen Koeppen.
Pécsi Tudományegyetem (University of Pécs) (Hungary): Dénes Molnar, Eva Erhardt, Katalin Csernus, Katalin Török, Szilvia Bokor, Mrs Angster, Enikö Nagy, Orsolya Kovács, Judit Répasi.
University of Crete School of Medicine (Greece): Anthony Kafatos, Caroline Codrington, María Plada, Angeliki Papadaki, Katerina Sarri, Anna Viskadourou, Christos Hatzis, Michael Kiriakakis, George Tsibinos, Constantine, Vardavas Manolis Sbokos, Eva Protoyeraki, Maria Fasoulaki.
Institut für Ernährungs- und Lebensmittelwissenschaften – Ernährungphysiologie, Rheinische Friedrich Wilhelms Universität (Germany): Peter Stehle, Klaus Pietrzik, Marcela González-Gross, Christina Breidenassel, Andre Spinneker, Jasmin Al-Tahan, Miriam Segoviano, Anke Berchtold, Christine Bierschbach, Erika Blatzheim, Adelheid Schuch, Petra Pickert.
University of Granada (Spain): Manuel J. Castillo, Ángel Gutiérrez, Francisco B. Ortega, Jonatan R. Ruiz, Enrique G. Artero, Vanesa España Romero, David Jiménez Pavón, Palma Chillón.
Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione (Italy): Davide Arcella, Elena Azzini, Emma Barrison, Noemi Bevilacqua, Pasquale Buonocore, Giovina Catasta, Laura Censi, Donatella Ciarapica, Paola D'Acapito, Marika Ferrari, Myriam Galfo, Cinzia Le Donne, Catherine Leclercq, Giuseppe Maiani, Beatrice Mauro, Lorenza Mistura, Antonella Pasquali, Raffaela Piccinelli, Angela Polito, Raffaella Spada, Stefania Sette, Maria Zaccaria.
University of Napoli ‘Federico II’ Department of Food Science (Italy): Luca Scalfi, Paola Vitaglione, Concetta Montagnese.
Ghent University (Belgium): Ilse De Bourdeaudhuij, Stefaan De Henauw, Tineke De Vriendt, Lea Maes, Carine Vereecken, Mieke de Maeyer, Charlene Ottevaere, Inge Huybrechts.
Medical University of Vienna (Austria): Kurt Widhalm, Katharina Phillipp, Sabine Dietrich, Birgit Kubelka, Marion Boriss-Riedl.
Harokopio University (Greece): Yannis Manios, Evangelia Grammatikaki, Zoi Bouloubasi, Tina Louisa Cook, Sofia Eleutheriou, Orsalia Consta, Elpida Papadantonaki, George Moschonis, Ioanna Katsaroli, George Kraniou, Stalo Papoutsou, Despoina Keke, Ioanna Petraki, Elena Bellou, Sofia Tanagra, Kostalenia Kallianoti, Dionysia Argyropoulou, Katerina Kondaki, Stamatoula Tsikrika, Christos Karaiskos.
Institut Pasteur de Lille (France): Jean Dallongeville, Aline Meirhaeghe.
Karolinska Institutet (Sweden): Michael Sjöstrom, Patrick Bergman, María Hagströmer, Lena Hallström, Mårten Hallberg, Eric Poortvliet, Julia Wärnberg, Nico Rizzo, Linda Beckman, Anita Hurtig Wennlöf, Emma Patterson, Lydia Kwak, Lars Cernerud, Per Tillgren, Stefaan Sörensen.
Asociación de Investigación de la Industria Agroali mentaria (Spain): Jackie Sánchez-Molero, Elena Picó, Maite Navarro, Blanca Viadel, José Enrique Carreres, Gema Merino, Rosa Sanjuán, María Lorente, María José Sánchez, Sara Castelló.
Campden & Chorleywood Food Research Association (United Kingdom): Chantal Gilbert, Sarah Thomas, Elaine Allchurch, Peter Burguess.
SIK – Institutet foer Livsmedel och Bioteknik (Sweden): Gunnar Hall, Annika Astrom, Anna Sverkén, Agneta Broberg.
Meurice Recherche & Development asbl (Belgium): Annick Masson, Claire Lehoux, Pascal Brabant, Philippe Pate, Laurence Fontaine.
Campden & Chorleywood Food Development Institute (Hungary): Andras Sebok, Tunde Kuti, Adrienn Hegyi.
Productos Aditivos SA (Spain): Cristina Maldonado, Ana Llorente.
Cárnicas Serrano SL (Spain): Emilio García.
Cederroth International AB (Sweden): Holger von Fircks, Marianne Lilja Hallberg, Maria Messerer.
Lantmännen Food R&D (Sweden): Mats Larsson, Helena Fredriksson, Viola Adamsson, Ingmar Börjesson.
European Food Information Council (Belgium): Laura Fernández, Laura Smillie, Josephine Wills.
Universidad Politécnica de Madrid (Spain): Marcela González-Gross, Jara Valtueña, David Jiménez-Pavón, Ulrike Albers, Raquel Pedrero, Agustín Meléndez, Pedro J. Benito, Juan José Gómez Lorente, David Cañada, Alejandro Urzanqui, Rosa María Torres, Paloma Navarro.




