


Obesity develops from a chronic energy imbalance, with intake exceeding expenditure over time. The obesogenic environment has increased the likelihood of expressing relatively-poor regulation of short-term intake. Certainly, the increase in childhood obesity suggests that overeating in response to environmental cues is becoming more common. The tendency to express poor intake control and to overeat has been characterized as part of the “hyperphagic genotype” ( Footnote 1 ), page 1338). Individuals with this genotype may be identified early in development using behavioural markers such as the compensation index (COMPX) and eating in the absence of hunger (EAH). COMPX reflects the child's ability to adjust intake at a meal in proportion to the energy content of a fixed load, with scores of 100% indicating perfect control( Footnote 2 ). EAH reflects the child's inability to resist eating despite having just consumed a meal and this variable has been linked with risk of overweight and obesity( Footnote 3 ). However, these measures indicate short-term control and positive energy balance occurs over time. Thus, children at risk of developing obesity may show low COMPX and high EAH as enduring attributes. The present study was conducted to assess whether COMPX and EAH were associated with weight change in preschool children and whether these variables were stable over time. In addition, parental characteristics that may predict short-term-intake control were measured.
To test COMPX ad libitum lunch intake after a high- (HE) and low-energy (LE) drink was compared on three occasions (T1, T2, T3). EAH was measured by providing a meal to children then providing snacks or colouring-in to do on three separate occasions (T1, T2, T3). Measurements were spread across a period of 27 weeks. In total twenty-five children enrolled for the study from 5 nurseries in Glasgow city, but complete data for all time points were obtained for thirteen preschool children (3–5.5 years). Parents completed questionnaires relevant to their feeding style; the child's eating behaviour, dietary intake, their BMI and history of overweight and obesity.
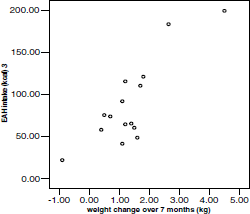
Children significantly adjusted intake at lunch in proportion to the energy content of the drinks at all three time points (COMPX: 48%, 25% and 68%), although correlations between the variables were weak. In contrast, EAH intakes were highly correlated for T1 and T2, but not T3, possibly due to the fall in numbers between T2 and 3, (205, 314 and 326 kJ (49, 75 and 78 kcal) for T1, T2 and T3 respectively). Overall, no correlation was found between COMPX and EAH in all three phases of the study. Children grew on average 0.005 m and gained 1.35 kg in weight over time, with children who gained the greatest amount of weight being more likely to have higher EAH intakes at T3 (r 0.83, P<0.0001; Figure).
Parental and child BMI did not correlate with COMPX or EAH; however, restriction measured by the child feeding questionnaire and concern for the child becoming overweight negatively correlated with the amount of fruit and vegetables consumed at home (r −0.67, P=0.02 and r −0.57, P=0.03 respectively). Change in BMI z score over the course of the study correlated with both monitoring (r 0.77, P=0.03) and parental feeding responsibility (r 0.58, P=0.04). Overall, EAH may be a better predictor than COMPX to identify risk for overweight and obesity and may be a potentially useful marker in characterising the “hyperphagic genotype”.
