


FFQ are frequently used in epidemiological studies because of the relatively low costs and limited efforts involved. Dietary intake estimated with FFQ is similar to dietary intake estimated with other dietary intake instruments subject to measurement errors, which can be both systematic and random. These measurement errors may lead to bias within individuals as well as between individuals(Reference Kipnis, Midthune and Freedman1, Reference Willett2). Using dietary intake in estimates of diet–disease associations can lead to an attenuation of the association, since measurement errors tend to bias the estimate towards zero(Reference Kipnis, Freedman and Brown3).
The Northern Sweden FFQ is used in the Västerbotten Intervention Programme (VIP), which is part of the European Prospective Investigation into Cancer and Nutrition (EPIC), as well as in the Northern Sweden WHO Multinational Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA) studies. The FFQ has been validated against ten repeated 24 h dietary recalls (24-HDR) with regard to intake of foods, energy and macronutrients(Reference Johansson, Hallmans and Wikman4), vitamins and minerals(Reference Johansson, Hallmans and Wikman4, Reference Johansson, Van Guelpen and Hultdin5) and fatty acids(Reference Wennberg, Vessby and Johansson6). The correlation coefficients between the FFQ and 24-HDR for energy, fat and fibre were between 0·45 and 0·61, and the median correlation coefficient for energy, macronutrients and a range of micronutrients was 0·50(Reference Johansson, Hallmans and Wikman4). Thus, the estimated level of validity was similar to that of other FFQ used in prospective cohort studies.
Plant sterols are bioactive compounds occurring in all vegetable foods. The chemical structure of plant sterols is similar to that of cholesterol, and plant sterols play an important role in the structure and function of plant cell membranes(Reference Piironen, Lindsay and Miettinen7). Plant sterols inhibit cholesterol absorption in the gut by competing for space in micelles(Reference Plat and Mensink8). In addition, plant sterols are thought to regulate the proteins implicated in cholesterol metabolism in the enterocytes and hepatocytes, although this action is not yet fully understood(Reference Calpe-Berdiel, Escola-Gil and Blanco-Vaca9). Because of these effects on cholesterol, plant sterol intake reduces serum cholesterol levels. Dietary intake of naturally occurring plant sterols has generally been considered ineffective, since the amounts consumed are relatively low. The daily intake of naturally occurring plant sterols in Europe is approximately 300 mg for men and varies from about 200 to about 300 mg for women(Reference Klingberg, Andersson and Mulligan10–Reference Valsta, Lemstrom and Ovaskainen13). However, two clinical trials have shown that an intake of 300 mg/d reduces cholesterol absorption by 11 % in a 3d trial(Reference Ellegård, Andersson and Bosaeus14) and by 28 % in a test meal trial(Reference Ostlund, Racette and Okeke15). In addition, two large epidemiological studies have shown a significant inverse association between dietary intake of naturally occurring plant sterols and levels of serum cholesterol(Reference Klingberg, Ellegård and Johansson11, Reference Andersson, Skinner and Ellegård16). Therefore, it may be hypothesized that a high intake of naturally occurring plant sterols could reduce the risk of myocardial infarction.
The objective of the present study was to evaluate plant sterol intake estimated with the Northern Sweden FFQ, with repeated 24-HDR as the reference method.
Materials and methods
The Västerbotten Intervention Programme
The population-based VIP invites all inhabitants in Västerbotten county in northern Sweden to a health check-up at their primary health-care centre the year they turn 30, 40, 50 and 60 years of age. The programme has been running since 1985 and, on average, 60 % of those invited participate(Reference Weinehall, Hallgren and Westman17).
Study population
In 1992, a stratified random subsample of individuals participating in the VIP was asked to take part in a validation study(Reference Johansson, Hallmans and Wikman4). A total of 246 individuals were invited, and 102 men and 101 women agreed to participate. This random sample was representative of the total study cohort with respect to smoking, BMI, total serum cholesterol and blood pressure, and the participants were equally distributed between the ages of 30, 40, 50 and 60 years(Reference Johansson, Hallmans and Wikman4). At the start of the validation study the participants completed an FFQ (FFQ1), followed by ten 24-HDR over the subsequent 12-month period. At the end of the study period a second FFQ (FFQ2) was completed. Eight participants were excluded: six did not complete all 24-HDR and two did not return FFQ1. In total, ninety-six men and ninety-nine women completed all ten 24-HDR and FFQ1, and all but two women also completed FFQ2. The Regional Ethical Review Board in Gothenburg, Sweden, has approved the analyses of the data presented here (registration number 622-05).
FFQ (test method)
The semi-quantitative FFQ with eighty-four questions(Reference Johansson, Hallmans and Wikman4) was distributed immediately before the beginning of the 24-HDR period. The frequencies of consumption were reported on a scale of nine levels, ranging from never to four or more times daily. The questionnaire included eight questions on spreads and fats used for cooking; ten on dairy products; ten on bread and cereals; eleven on fruits, berries, vegetables, root vegetables and legumes; five on potatoes; six on cookies and sweets; twenty-one on meat, fish and mixed dishes; twelve on coffee, tea, alcoholic and other beverages; and one on salty snacks. The FFQ included four colour photographs with which the respondents indicated portion sizes of potatoes, rice and pasta; meat and fish; and vegetables. Energy and nutrient intakes were calculated using the food composition database (updated 1994) at the Swedish National Food Administration, Uppsala, Sweden, as previously described(Reference Johansson, Hallmans and Wikman4). A database of the analysed plant sterol content of more than 330 food items held at the Department of Clinical Nutrition at the University of Gothenburg, Sweden, was used to estimate plant sterol intake(Reference Normén, Bryngelsson and Johnsson18–Reference Normen, Johnsson and Andersson20). The plant sterol database comprises data for five individual plant sterols: the unsaturated plant sterols campesterol, stigmasterol and β-sitosterol, and the saturated plant stanols campestanol and β-sitostanol. The sum of the five individual plant sterols constitutes ‘total plant sterol’ and, unless specified otherwise, is referred to as ‘plant sterol intake’ in the present paper. The database and calculation of plant sterol intake from the FFQ have been described in detail elsewhere(Reference Klingberg, Ellegård and Johansson11).
Repeated 24 h dietary recalls (reference method)
The ten repeated 24-HDR were carried out by telephone during the 12-month period between FFQ1 and FFQ2(Reference Johansson, Hallmans and Wikman4). The ten 24-HDR were unannounced, equally dispersed throughout the period and covered all days of the week. The participants were interviewed in a standardized way and asked to report all consumed foods and drinks during the previous 24 h. To help in estimating portion sizes, a booklet with full-size portion pictures was sent in advance to the participants(Reference Bergström21, Reference Håglin, Hagman and Nilsson22). Energy and nutrient intakes were calculated utilizing the database from the Swedish National Food Administration (updated 1994) as previously described(Reference Johansson, Hallmans and Wikman4). To estimate plant sterol intake, each food item consumed was allocated a plant sterol value based on analyses(Reference Normén, Bryngelsson and Johnsson18–Reference Normen, Johnsson and Andersson20) or recipe calculations of analysed ingredients.
Statistical analyses and calculations
All statistical calculations were performed separately for the men and women using the statistical software package PASW Statistics 18 for Windows (SPSS Inc.), except the weighted kappa statistics which were performed using the SAS statistical software package version 9·2 (SAS Institute Inc.). Intakes of plant sterols were normally distributed, and parametric methods were used. All statistical tests were two-sided and P values below 0·05 were considered statistically significant.
To correct correlation coefficients for within-individual variation and between-individual variation an attenuation factor was calculated as  $$-->$<> {{a}_{\rm factor}}\, = \,{{\{ [1\, + \,{{(C{{V}\!_{\rm w}}\,/\,C{{V}\!_{\rm b}})}_x}\,/\,{{n}_x}{\rm{]<$>
<[[$$
$$-->$<> {{a}_{\rm factor}}\, = \,{{\{ [1\, + \,{{(C{{V}\!_{\rm w}}\,/\,C{{V}\!_{\rm b}})}_x}\,/\,{{n}_x}{\rm{]<$>
<[[$$ $$\[-->$<>[}}1\, + \,{{(C{{V}\!_{\rm w}}\,/\,C{{V}\!_{\rm b}})}_y}\,/\,{{n}_y}]\} }^{0 \cdot 5}} <$>
<!--$$, where CV w is within-individual variation, CV b is between-individual variation, n is the number of repeated measurements, x represents the FFQ and y represents the 24-HDR(Reference Willett2).
$$\[-->$<>[}}1\, + \,{{(C{{V}\!_{\rm w}}\,/\,C{{V}\!_{\rm b}})}_y}\,/\,{{n}_y}]\} }^{0 \cdot 5}} <$>
<!--$$, where CV w is within-individual variation, CV b is between-individual variation, n is the number of repeated measurements, x represents the FFQ and y represents the 24-HDR(Reference Willett2).
Energy-adjusted intake of plant sterols was defined as intake per energy unit, i.e. mg/MJ.
Participants were classified into quartiles for absolute (mg/d) and energy-adjusted (mg/MJ) plant sterol intake by ranking the men and women separately according to their reported absolute plant sterol intake (mg/d) and energy-adjusted plant sterol intake (mg/MJ), respectively.
Results
Both the men and women had a mean age of 45 years and the proportions of 30-, 40-, 50- and 60-year-old participants were equal for both sexes. The men had a daily mean (minimum–maximum) energy intake of 9·1 (2·7–21·0) MJ estimated with FFQ1, 8·7 (4·2–16·2) MJ with FFQ2 and 9·1 (4·6–16·0) MJ with 24-HDR. The corresponding estimated intakes for the women were 7·1 (4·0–15·3) MJ, 6·9 (3·6–12·2) MJ and 6·9 (3·1–12·4) MJ, respectively.
The mean (95 % CI) intakes, Pearson correlation coefficients and calibration coefficients of absolute plant sterol intake (mg/d) estimated with FFQ1 and 24-HDR are reported separately for the men and women in Table 1. The corresponding data on energy-adjusted plant sterol intake (mg/MJ) are presented in Table 2.
Table 1 Absolute intake of plant sterols (mg/d) estimated with the first administration of the Northern Sweden FFQ (FFQ1) and ten repeated 24 h dietary recalls (24-HDR) in ninety-six men and ninety-nine women participating in the Västerbotten validation study
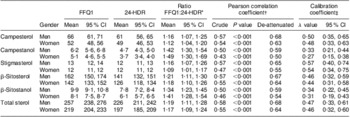
*Mean (95 % CI) of individual ratios between intakes estimated with FFQ1 and 24-HDR.
†The Pearson correlation coefficient between plant sterol intakes estimated with FFQ1 and 24-HDR, crude coefficients and after de-attenuation.
‡The calibration coefficient, with 95 % CI corresponding to the slope of the regression of the plant sterol intake estimated with 24-HDR v. the intake estimated with FFQ1.
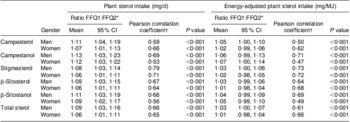
Table 2 Energy-adjusted plant sterol intake (mg/MJ) estimated with the first administration of the Northern Sweden FFQ (FFQ1) and ten repeated 24 h dietary recalls (24-HDR) in ninety-six men and ninety-nine women participating in the Västerbotten validation study
*Mean (95 % CI) of individual ratios between intakes estimated with FFQ1 and 24-HDR.
†The Pearson correlation coefficient between energy-adjusted plant sterol intakes estimated with FFQ1 and 24-HDR, crude coefficients and after de-attenuation.
‡The calibration coefficient, with 95 % CI corresponding to the slope of the regression of energy-adjusted plant sterol intake estimated with 24-HDR v. the energy-adjusted plant sterol intake estimated with FFQ1.
The men had a mean (minimum–maximum) total plant sterol intake of 257 (71–561) mg/d estimated with FFQ1 and 226 (68–496) mg/d estimated with 24-HDR. The women had an intake of 219 (107–446) mg/d and 197 (77–401) mg/d, respectively. The Pearson correlations between absolute intakes of individual plant sterols estimated with FFQ1 and 24-HDR showed crude correlation coefficients between 0·50 and 0·58 for the men and 0·43 and 0·55 for the women (all P < 0·001), while de-attenuated correlation coefficients were between 0·59 and 0·68 for the men and between 0·50 and 0·64 for the women, respectively. Linear regression of total plant sterol intake from 24-HDR v. FFQ1 showed a calibration factor of between 0·33 and 0·57 for the men and between 0·27 and 0·54 for the women.
Mean (minimum–maximum) energy-adjusted plant sterol intake was 28 (15–48) mg/MJ estimated with FFQ1 for the men and 25 (9–48) mg/MJ estimated with 24-HDR. For the women, energy-adjusted plant sterol intake was 31 (18–45) mg/MJ and 29 (12–57) mg/MJ, respectively. The correlation coefficients between the intakes estimated by FFQ1 and 24-HDR ranged from 0·23 to 0·40 for the men and 0·27 to 0·53 for the women (all P < 0·05). After de-attenuation, correlation coefficients ranged between 0·29 and 0·48 for the men and between 0·33 and 0·63 for the women. The calibration coefficients from linear regression of energy-adjusted plant sterol intake from 24-HDR v. FFQ1 were between 0·21 and 0·38 for the men and between 0·18 and 0·54 for the women.
The Pearson correlation coefficients for absolute plant sterol intake and energy-adjusted plant sterol intake estimated with FFQ1 were 0·46 for the men and 0·56 for the women, and 0·48 and 0·63 estimated with 24-HDR for the men and women, respectively (all P < 0·001).
The reproducibility of the FFQ with regard to absolute plant sterol intake (mg/d) and energy-adjusted plant sterol intake (mg/MJ) is shown in Table 3. The mean intake ratios for absolute plant sterol intake (mg/d) ranged between 1·08 and 1·13 for the men, and between 1·06 and 1·12 for the women. The corresponding figures for energy-adjusted plant sterol intake (mg/MJ) were between 1·03 and 1·06 for the men, and between 1·01 and 1·07 for the women. The Pearson correlation coefficients for absolute plant sterol intake (mg/d) ranged from 0·59 to 0·79 for the men, and from 0·53 to 0·71 for the women (all P < 0·001). The correlation coefficients for energy-adjusted plant sterol intake (mg/MJ) ranged from 0·50 to 0·73 for the men, and from 0·47 to 0·72 for the women (all P < 0·001).
Table 3 Reproducibility for absolute plant sterol intake (mg/d) and energy-adjusted plant sterol intake (mg/MJ) estimated with the first and second administration of the Northern Sweden FFQ (FFQ1 and FFQ2) at a 12-month interval, expressed as the ratio between FFQ1 and FFQ2, and the Pearson correlation coefficients in ninety-six men and ninety-seven women participating in the Västerbotten validation study
*Mean (95 % CI) of individual ratios between intakes estimated with FFQ1 and FFQ2.
†The Pearson correlation coefficient between the plant sterol intakes estimated with FFQ1 and FFQ2.
The Bland–Altman plots (Fig. 1(a) to (d)) exhibit the difference between plant sterol intakes estimated with 24-HDR and FFQ1 plotted against the mean intake from the two methods. The plots indicate generally low mean differences and little systematic bias between the two methods.
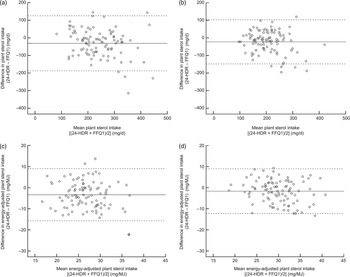
Fig. 1 Bland–Altman plots for (a) absolute total plant sterol intake in ninety-six men, (b) absolute total plant sterol intake in ninety-nine women, (c) energy-adjusted total plant sterol intake in ninety-six men and (d) energy-adjusted total plant sterol intake in ninety-nine women, all participating in the Västerbotten validation study. Differences in intakes estimated with the ten repeated 24 h dietary recalls (24-HDR) and the first administration of the Northern Sweden FFQ (FFQ1) are plotted against the mean intakes estimated with the two methods (——, mean difference; ----, 95 % limits of agreement, i.e. mean difference ± 1.96 sd of the difference between the two methods)
Cross-classification of participants in quartiles of plant sterol intake estimated with 24-HDR v. FFQ1 and with FFQ1 v. FFQ2 is shown in Table 4. Cross-classification of absolute plant sterol intake quartiles estimated with the FFQ1 and 24-HDR revealed that 90 % of the men and 83 % of the women were classified into the same or an adjacent quartile, while 1 % of both the men and women were grossly misclassified. For energy-adjusted plant sterol intake quartiles, 71 % of the men and 74 % of the women were classified into the same or an adjacent quartile. Severe misclassification was observed for 6 % of the men and 4 % of the women. Weighted kappa values for absolute plant sterol intake were over 0·4 for both men and women, while the values for energy-adjusted plant sterol intake were 0·17 for men and 0·25 for women. Cross-classification of absolute plant sterol intake quartiles estimated with FFQ1 and FFQ2 showed that 85 % of the men and 95 % of the women were classified into the same or an adjacent quartile, and that 1 % of the men and none of the women were severely misclassified. Eighty-eight per cent of the men and 90 % of the women were classified into the same or an adjacent quartile of energy-adjusted plant sterol intake (mg/MJ), and 2 % of the men and 1 % of the women were grossly misclassified. Weighted kappa values were about 0·5 for both absolute and energy-adjusted plant sterol intake for both men and women.
Table 4 Percentage agreement within the same or an adjacent quartile and percentage misclassification between extreme quartiles for the mean intake from ten repeated 24 h dietary recalls (24-HDR) and the first administration of the Northern Sweden FFQ (FFQ1) in ninety-six men and ninety-nine women, and between FFQ1 and the second FFQ administration (FFQ2) in ninety-six men and ninety-seven women participating in the Västerbotten validation study

*Weighted κ value.
Discussion
In the present study we investigated the agreement between two dietary assessment methods, namely the Northern Sweden FFQ and ten repeated 24-HDR, with respect to absolute plant sterol intake (mg/d), energy-adjusted plant sterol intake (mg/MJ) and the ability to rank individuals according to their plant sterol intake. Previous publications from this diet database have examined the agreement between these two methods, focusing on the intakes of foods, energy, macronutrients and a selection of micronutrients(Reference Johansson, Hallmans and Wikman4), fatty acids(Reference Wennberg, Vessby and Johansson6), folate and other B vitamins(Reference Johansson, Van Guelpen and Hultdin5). These previous studies have concluded that the validity of the Northern Sweden FFQ is similar to that of other FFQ used in large-scale studies.
The difficulty of dietary assessments in free-living populations is that all methods depend on individuals’ subjective information on their food intake. Hence, these methods are subject to measurement errors of different kinds, which can be both random and systematic(Reference Kipnis, Midthune and Freedman1). The development of biomarkers of nutrient intake is promising as it enables objective validation of dietary assessment methods(Reference Jenab, Slimani and Bictash23). Unfortunately, when it comes to plant sterols no biomarker for free-living individuals exists and probably never will, since very little of the plant sterols are absorbed in the intestine and consequently most are excreted with faeces. Additionally, plant sterols are found in a wide range of foods and with a large variation in each food group, making it impossible to use substitute biomarkers like those for fruit and vegetables (e.g. vitamin C and carotenoids in plasma) or fat (e.g. fatty acids in erythrocyte membranes). Therefore, studies such as the present one are important, i.e. comparisons of two dietary methods where one is presumed to be more accurate, but where the true intake remains uncertain.
The absolute intake of plant sterols estimated with FFQ1 was higher than that estimated with repeated 24-HDR: 19 % higher in the men and 17 % higher in the women. The individual plant stanols (campestanol and β-sitostanol) were overestimated with the FFQ more than the other plant sterols (campesterol, stigmasterol and β-sitosterol). Campestanol was 42 % higher for the men in the FFQ and 49 % higher for the women. For β-sitostanol the figures were 34 % and 41 % higher for men and women, respectively. The higher estimation of absolute plant sterol intake by the FFQ could be explained by the fact that the reported intake of plant sterol-containing foods such as bread, cereals, potatoes/rice/pasta, fruits and vegetables was higher in the FFQ than in the 24-HDR(Reference Johansson, Hallmans and Wikman4). The plant stanols had a higher degree of overestimation by the FFQ than the plant sterols, despite the much lower intake, which could be a result of systematic misreporting. Plant stanols are almost only found in cereals and to a higher extent in wholegrain cereals. One possible explanation could be that the intake of wholegrain bread is overestimated in the FFQ, leading to an overestimation of plant stanol intake. Post hoc analyses support this explanation since consumption frequencies from the FFQ showed almost the same consumption of wholegrain bread and white bread, while data from the 24-HDR showed that wholegrain bread contributed only 25 % of the consumed bread. The correlation coefficients between FFQ1 and the 24-HDR for absolute intakes of the individual plant sterols and total plant sterols were between 0·50 and 0·58 for the men, and between 0·43 and 0·55 for the women, and thus are comparable to those for other nutrients studied within this cohort(Reference Johansson, Hallmans and Wikman4–Reference Wennberg, Vessby and Johansson6). As seen for most other nutrients, the correlation coefficients declined when energy-adjusted plant sterol intake was studied instead. This may be because the energy adjustment was made by dividing the plant sterol intake by the energy intake, and this quotient is dependent on two values that may differ between the two methods. Likewise, the calibration coefficient – showing how well the FFQ can predict the ‘true value’, i.e. the mean of ten 24-HDR – was higher when absolute intakes were studied than when energy-adjusted intakes were studied.
Cross-classification of absolute plant sterol intake quartiles showed good agreement between the two methods, and very few individuals were grossly misclassified. Here too, cross-classification based on energy-adjusted plant sterol intake showed a slightly lower level of agreement, although more than 70 % of the men and women were still classified into the same or an adjacent quartile. This suggests that the FFQ is able to rank individuals with acceptable accuracy according to both their absolute plant sterol intake and their energy-adjusted plant sterol intake. The agreement for cross-classification of FFQ1 and FFQ2 for both absolute plant sterol intake and energy-adjusted plant sterol intake was high, which suggests that the FFQ method is reliable. Intake ratios based on absolute intake revealed slightly higher reported intakes from FFQ1 than from FFQ2, perhaps suggesting an effect of exhaustion or a more pronounced under-reporting due to the repeated 24-HDR preceding the second FFQ. Another possible explanation is that the true intake has decreased. This effect was not seen, however, for energy-adjusted plant sterol intake.
Both the absolute intake of plant sterols(Reference Klingberg, Andersson and Mulligan10, Reference Normen, Brants and Voorrips12, Reference Valsta, Lemstrom and Ovaskainen13, Reference Escurriol, Mari-Dell'Olmo and Rohlfs24) and the energy-adjusted plant sterol intake(Reference Klingberg, Andersson and Mulligan10, Reference Valsta, Lemstrom and Ovaskainen13) in Sweden are slightly lower than those reported from other European countries. One explanation could be differences in dietary assessment methods. For example, the Swedish FFQ used in the present study consists of eighty-four questions compared with 150 questions in the Dutch study(Reference Normen, Brants and Voorrips12) and 130 questions in the UK study(Reference Klingberg, Andersson and Mulligan10); hence, fewer questions could be a reason for the lower estimation of absolute plant sterol intake in Sweden. However, the energy-adjusted plant sterol intake was also lower, indicating a true difference in plant sterol intake between Sweden and the Netherlands as well as the UK.
The random and systematic measurement errors inherent to all dietary assessment methods make nutrient intake data uncertain and a consequence could be that relationships between nutrients and health-related states and diseases remain undetected. A further challenge facing studies investigating the association between plant sterol intake and the risk of future illness is that the dispersion of dietary intakes of plant sterols is narrow: about 75 % of both the men and women in our study had an intake between 150 and 350 mg/d. This may make it difficult to find and show statistical associations between intake and the risk of disease. Here, larger research collaborations like EPIC are important as they represent populations with widely different dietary patterns.
Conclusions
The evaluation has demonstrated that the Northern Sweden FFQ is able to capture absolute plant sterol intake to the same extent as macronutrients and micronutrients. The FFQ is also able to rank individuals according to both their absolute plant sterol intake and their energy-adjusted plant sterol intake. Furthermore, investigation of the reproducibility showed that the agreement between FFQ1 and FFQ2 was good, suggesting that the method is reliable. This makes it possible to use plant sterol intake data from the FFQ in large-scale studies of the association between plant sterol intake and disease.
Acknowledgements
This work was funded by FORMAS, the Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning (grant 22·2/2003-0655); VR, the Swedish Research Council (grants K2005-27VX-15218-02B and K2006-27X-20061-01-3); and the Swedish Nutrition Foundation. The plant sterol analyses were funded by a grant from the Swedish Government under the LUA agreement and the Swedish Cancer Foundation. The Västerbotten Intervention Programme (VIP) was funded by the Swedish Cancer Society, the Europe Against Cancer Programme and Västerbotten County Council. The development and maintenance of the dietary database is funded by grants from the Swedish Council for Working Life and Social Research and the Swedish Research Council. None of the authors have personal or financial conflict of interest. The authors’ responsibilities were as follows. G.H. was the principal investigator in the VIP study; I.J. and A.W. were responsible for the dietary data of the VIP study; I.J. and S.K. prepared the plant sterol data set in the VIP cohort; S.K. was the principal investigator in the present study and wrote the paper with contributions from co-authors. Each author has seen and approved the content of the submitted manuscript. The authors acknowledge Lars Ellegård for insightful comments on the manuscript.





