Worldwide trends of increasing weight gain and obesity are reported in children( 1 , 2 ). In South Africa the combined overweight and obesity prevalence in children aged 2–19 years is 18·8 and 26·3 % for boys and girls, respectively( Reference Ng, Fleming and Robinson 3 ). The consequences of overweight and obesity include non-communicable diseases such as CVD, type 2 diabetes mellitus, fatty liver disease, musculoskeletal disorders and some cancers( 4 ). To prevent the development of overweight and obesity a need is recognised for early intervention strategies during childhood, while children are still developing eating habits( 1 , Reference Vereecken, Bobelijn and Maes 5 ).
The implementation of health promotion and nutrition interventions at schools may offer the opportunity to influence the nutrition-related perceptions of students from an early age and also promote healthy eating behaviours of young students( Reference Vereecken, Bobelijn and Maes 5 – Reference Wang and Stewart 7 ). In recent years, the types of food, snack and beverage items supplied by school tuck shops has become a focus point for intervention in view of the fact that meals and snacks consumed by students during school hours provide a large percentage of their daily nutrient intakes( Reference Temple, Steyn and Myburgh 8 – Reference Conway, Sallis and Pelletier 10 ). Schools tuck shops are usually profit driven and offer unhealthy items that are high in energy, with a high saturated fat and/or sugar content and low content of vitamins, minerals and dietary fibre( Reference Briefel, Wilson and Gleason 6 , Reference Temple, Steyn and Myburgh 8 , Reference Wiles, Green and Veldman 11 ). Healthy food items with a high nutrient density that are high in fibre, low in saturated fat, contain no added sugar and are low in sodium are often not as popular and thus less profitable for tuck shops to sell( 1 , Reference Temple, Steyn and Myburgh 8 , Reference Kakarala, Keast and Hoeer 12 ).
The availability and composition of unhealthy foods offered by tuck shops often have a negative influence on students’ eating habits and may limit their ability to make healthy choices( Reference Utter, Schaaf and Mhurchu 9 , Reference Gosliner, Madsen and Woodward-Lopez 13 ). In addition to the availability and popularity of tuck shop items, parents often see school tuck shops as an opportunity to ‘treat’ their children, thus encouraging poor eating habits( Reference Bell and Swinburn 14 ). Furthermore, the content of lunchbox items brought to school can also contribute to the unhealthy food intake of students during school hours( Reference Kubik, Lytle and Hannan 15 , Reference Sangiorski, Bell and Kremer 16 ). In South Africa, Temple et al. reported that even though 50 % of students brought food to school in their lunchboxes, the lunchboxes contained unhealthy food items and students bought additional unhealthy food items at school( Reference Temple, Steyn and Myburgh 8 ).
Tuck shops that regulate the types of foods and beverages that are available, and sell mostly healthy items to students (nutritionally regulated tuck shops), may help to limit access to unhealthy foods and beverages during school hours( 1 , Reference Temple, Steyn and Myburgh 8 , Reference Kakarala, Keast and Hoeer 12 ). A paucity of data exists in the current literature describing the influence of a nutritionally regulated school tuck shop on the perceptions, attitudes and behaviours of South African primary-school students towards healthy eating. Therefore the aim of the current study was to determine if the presence of such a nutritionally regulated tuck shop in the primary-school environment could have an influence on students’ perceptions and attitudes towards healthy eating, and also if students in a school with a nutritionally regulated tuck shop would be encouraged to buy healthier tuck shop items and to bring more healthy items to school in their lunchboxes.
Methods
The study population consisted of primary-school students attending well-resourced, co-education primary schools in the urban city area of Bloemfontein, with Afrikaans language as the teaching medium. For the present purposes, a primary school with an established (and fairly unique) nutritionally regulated tuck shop was included in the study (school A). For comparison purposes, two other well-resourced primary schools with similar student profiles and conventional tuck shops were randomly selected for the study (school B and school C). School B was included in the main study and the pilot study was held at school C. In order to ensure that participating schools fell into the same socio-economic area of the city, the region of Bloemfontein, south of Nelson Mandela Drive, within a radius of 4 km from school A, was considered for selecting schools B and C. To limit possible bias of the study results, none of the participating schools had to be part of any educational programmes offered by external stakeholders. Four schools qualified for selection and two of these schools were selected by means of random sampling by drawing the schools’ names from a hat.
A mixed-methods research approach was used. A cross-sectional survey with an analytical component as well as focus group discussions were conducted. Fifteen boys and fifteen girls from grades 2 to 7 (ages 7 to 14 years) were randomly selected by means of interval sampling in each of the participating schools to complete a self-administered questionnaire. A list with the exact number of students per grade, also indicating gender, was obtained from each school. The class lists were combined for each grade and these lists were used for interval sampling. Selection took place in the form of random sampling per school grade and gender to include equal numbers of students from each year group and gender. A study sample was obtained from the school lists by selecting every third male and female until fifteen males and fifteen females were selected in each participating grade of schools A and B. From this study sample, six students per grade (three boys and three girls) in each of the schools were randomly selected to participate in focus group discussions. The first six students selected for the focus group discussions who gave written assent were included in the focus groups.
The self-administered questionnaire was developed by the principal researcher and questions were based on the research objectives of the study and current literature( Reference Briefel, Wilson and Gleason 6 , Reference Temple, Steyn and Myburgh 8 – Reference Conway, Sallis and Pelletier 10 , Reference Kakarala, Keast and Hoeer 12 , Reference Bell and Swinburn 14 – Reference Sangiorski, Bell and Kremer 16 ). The questionnaire aimed to assess students’ perceptions, attitudes and behaviours towards healthy eating. The questions were written in easily understandable language to be suitable for self-completion by primary-school students. The first section of the questionnaire consisted of eight close-ended questions regarding sociodemographic information, the amount of money spent at the tuck shop and the frequency per week that items were bought from the tuck shop. The second section contained three close-ended questions about lunchbox contents. The third section consisted of four open-ended questions regarding the items bought at the tuck shop on the day of data collection and items sold by the tuck shop that the student liked and disliked. There was also a question asking which other items the student would like to have available in the tuck shop. The last part of the questionnaire had a section with nine questions that evaluated perceptions and attitudes by means of three-point Likert scales with smiley faces. The questionnaire ended with two games where the student was asked to mark pictures of food, beverage and snack items he/she would pack into his/her own lunchbox, and then to mark all the pictures of the fruits and vegetables that he/she liked.
To ensure content validity, two primary-school teachers and two registered dietitians scrutinised the content of the questionnaire to determine its validity for measuring the perceptions, attitudes and behaviours of primary-school students towards healthy eating. Face validity was determined by the subjective judgement of the researcher. The researcher assessed the readability, feasibility, clarity of wording, layout and style of the questionnaire, as well as the results obtained from the pilot study, to determine that each item in the questionnaire provided answers to the research questions. To test the reliability of the questionnaire, a pilot study was conducted in a randomly selected primacy school (school C) in Bloemfontein with a similar student profile to the other two schools selected for the study. To further evaluate reliability, the questionnaire was re-administered to the same sample of students in school C after two weeks. The internal reliability of the questionnaire was evaluated statistically per construct by calculating Cronbach’s α using the data obtained from the pilot study. A coefficient close to +1·00 reflects a high internal reliability of a questionnaire. The Cronbach’s α value (+0·92) indicated that the questionnaire was reliable. A few questions with a low internal reliability score and negatively worded questions were omitted from the final questionnaire and questions that were misunderstood by students, based on notes kept by the researcher and trained research assistant during the pilot study, were adapted.
Questionnaire administration took place at the respective school after the school interval when students could remember best what they had eaten from their lunchbox and/or bought from the tuck shop. The older students completed the questionnaire in approximately 10 min, while the younger students took about 20 min. The researcher assisted the students by reading out each question and allowing time for completion. Any queries were clarified and where necessary students were assisted without influencing their responses to the questions. Questionnaire information was treated as confidential and filled out anonymously.
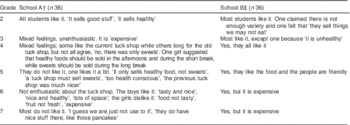
Focus group discussions were conducted in each grade with six students per group to further explore the perceptions, attitudes and behaviours of students towards healthy eating. The first questions on the discussion guide were general questions which allowed students to relax and understand the procedure (Table 1). The focus group discussions were held during school hours in a room where students could sit around a table and discuss the relevant topics. Students could communicate freely, since there were no interruptions. Each focus group discussion lasted between 15 and 20 min. The discussions were facilitated by the principal researcher while a trained research assistant took notes of the students’ interactions and their contributions to the discussion. An audio recorder was set up to record the discussions. The researcher followed the discussion guide and helped students to stay focused on a specific topic by asking exploratory questions without leading them.
Table 1 Example of questions in the discussion guide
Statistical analysis
Data from the questionnaires were captured using Microsoft® Excel 2007 and the statistical software package STATISTICA version 10 was used to analyse the data. A statistician analysed the quantitative data by making comparisons between the school with the nutritionally regulated tuck shop and the school with the conventional tuck shop. Relationships between two continuous variables were analysed with regression analysis and the strength of the relationship measured by Pearson correlation or Spearman correlation when continuous variables were not normally distributed. Analyses for each grade were also done, where every grade in the school with the nutritionally regulated tuck shop was compared with the same grade in the school with the conventional tuck shop. The relationship between nominal variables was investigated with contingency tables and the likelihood ratio maximum likelihood χ 2 test. P<0·05 was taken to represent statistical significance in hypothesis testing and 95 % confidence intervals were used to describe the estimation of some unknown parameters.
Students’ responses to open-ended questions in the questionnaire were sorted into categories by making use of inductive coding, whereby the researcher used categories as they emerged from the data( Reference Creswell and Plano Clark 17 ). The results of the open-ended questions were summarised in a Microsoft Excel spreadsheet in order to calculate the percentage of units that fell into each category( Reference Norton 18 ).
Content analysis of focus group discussions
The principal researcher transcribed audio recordings, notes made by the research assistant during focus group discussions, as well as non-verbal cues. The researcher then performed a content analysis of the transcripts. The researcher read and re-read each transcript until she became familiar with the content. Thereafter the complete transcripts were summarised, question by question, for each focus group, with emphasis on identified perceptions, attitudes and behaviours. Meaningful segments of data were coded using predetermined or deductive coding( Reference Niewenhuis 19 ).
Results
A total of 116 students (boys n 44, girls n 72) in school A and 141 students (boys n 56, girls n 85) in school B completed the questionnaire, while six students from grade 2 to 7 in each school took part in focus group discussions (n 72). The current paper focuses on results concerning students’ perceptions and attitudes towards the school’s tuck shop, their tuck shop buying behaviour and the types of food items in their lunchboxes.
Perceptions and attitudes of students towards their school tuck shop
To determine the perceptions and attitudes of students about their particular school’s tuck shop, the students were asked to indicate whether they ‘agree’, ‘disagree’ or ‘don’t know’ when given two statements. In both schools the majority of students did not agree with the statement that the tuck shop must not sell sweets and cold drinks (Fig. 1). During the focus group discussions, students from both schools said that they would like to have a combination of healthy and unhealthy items available in their respective school’s tuck shop.
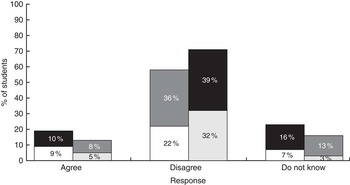
Fig. 1 Grade 2 to 7 students’ responses to the statement: ‘The tuck shop must not sell sweets and cold drinks’ (n 257) by school and gender (![]() , school A boys;
, school A boys; ![]() , school A girls;
, school A girls; ![]() , school B boys;
, school B boys; ![]() , school B girls), Bloemfontein, South Africa (school A has a nutritionally regulated tuck shop, school B has a conventional tuck shop)
, school B girls), Bloemfontein, South Africa (school A has a nutritionally regulated tuck shop, school B has a conventional tuck shop)
In response to the second statement, the majority of students in both schools indicated that they would rather buy fresh fruit than sweets at the tuck shop (Fig. 2), but none of the students at either school bought fresh fruit from their respective school’s tuck shop on the day of data collection (Table 2).

Fig. 2 Grade 2 to 7 students’ responses to the statement: ‘I will rather buy fresh fruit than sweets at the tuck shop’ (n 257) by school and gender (![]() , school A boys;
, school A boys; ![]() , school A girls;
, school A girls; ![]() , school B boys;
, school B boys; ![]() , school B girls), Bloemfontein, South Africa (school A has a nutritionally regulated tuck shop, school B has a conventional tuck shop)
, school B girls), Bloemfontein, South Africa (school A has a nutritionally regulated tuck shop, school B has a conventional tuck shop)
Table 2 Tuck shop items bought by grade 2 to 7 students on the day of data collection (n 257), Bloemfontein, South Africa
† School with a nutritionally regulated tuck shop.
‡ School with a conventional tuck shop.
§ These items are regarded as healthy items since recipes were adapted to have a lower fat and sugar content. Muffin: 556 kJ (133 kcal), 2·8 g fat; sugar-free sweets, packet: 88 kJ (21 kcal), 0 g fat; pancake/brownie: 544 kJ (130 kcal), 3·5 g fat; samoosa: 276 kJ (66 kcal), 2 g fat; hamburger: 761 kJ (182 kcal), 3·7 g fat.
When students at school A were asked if they like their tuck shop, mixed feelings were detected among the focus group participants regarding the nutritionally regulated tuck shop (Table 3). The younger students (grade 2 in particular) were clearly more positive than the older students (grades 5 to 7). Several liked it ‘a little bit’ or ‘not a lot’ and the groups gave several opinions to state why they did or did not like the tuck shop. They were all aware that healthy food items were sold. The reasons for the positive attitude (‘liking it’) were based on perceptions that ‘it sells healthy good stuff’, the food is ‘tasty and nice’, the venue is appealing (‘lots of space’), and the shop sells ‘nice stuff’ – ‘like those pancakes’. There were also conversations (grades 4 and 5) about the previous ‘old’ conventional tuck shop at the school; some wanted it back and some preferred a combination of both tuck shops. Some perceptions underlying the negative attitudes towards the nutritionally regulated tuck shop in the grade 5 to 7 groups include feelings like ‘it only sells healthy food, not sweets – a tuck shop must sell sweets’, ‘too health conscious’, ‘too expensive’, ‘the food not nice and tasty’, ‘fruit not always fresh’. In the grade 7 group most students did not like the tuck shop, but they also admitted that the healthy tuck shop concept is still new to them: ‘I guess we are just not used to it’.
Table 3 Grade 2 to 7 students’ responses to the question: ‘Do you like your school’s tuck shop?’ (n 72) by grade and school, Bloemfontein, South Africa
† School with a nutritionally regulated tuck shop.
‡ School with a conventional tuck shop.
In contrast to school A, the students in school B were in general very positive towards their conventional tuck shop and the question did not trigger them to elaborate and voice their opinions as experienced in the case of the discussions at school A. They liked the tuck shop because they ‘like the food’ and ‘the people are friendly’. In the younger groups (grades 2 and 3) some students were conscious of the fact that the foods were not always healthy (‘they sell things we should not eat’, ‘it is unhealthy’), while the older students (grades 6 and 7) mentioned that they did not like the prices (‘expensive’).
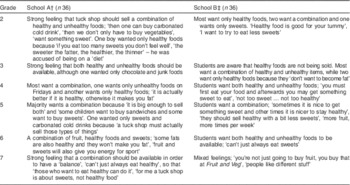
The focus group participants were also asked if, in their opinion, ‘Tuck shops should only sell healthy foods or only sweets?’ In all age groups at both schools the students had strong feelings that a combination of healthy and unhealthy items should be available in the school tuck shops (Table 4). Reasons for having a combination of tuck shop items at school A ranged from feelings that they will then not be forced to buy only healthy items from the nutritionally regulated tuck shop (‘then one can buy carbonated cold drinks’, ‘then we don’t only have to buy vegetables’, ‘some children want to buy sandwiches and some want to buy sweets’) to perceptions about what a tuck shop should sell (‘a tuck shop is about sweets, not healthy food’) and that moderation and a ‘balance’ between healthy foods and sweet intake is necessary (‘if you eat too many sweets you don’t feel well’, ‘it’s actually better if it is healthy, otherwise it makes you fat’, ‘can’t just always eat healthy’, ‘fruit and sweets will give you energy for sport’).
Table 4 Grade 2 to 7 students’ responses to the question: ‘Do you think tuck shops should only sell healthy foods or only sweets?’ (n 72) by grade and school, Bloemfontein, South Africa
† School with a nutritionally regulated tuck shop.
‡ School with a conventional tuck shop.
Although students suggested that their tuck shop should sell a combination of healthy and unhealthy items, the younger students in school B (grades 2 and 3) liked the idea of a healthy tuck shop (‘I want to try to eat less sweets’, ‘don’t want to become fat’). Similar to students in school A, the older students in school B wanted to have a ‘balance’ and a choice between healthy and unhealthy items (‘you must first eat your food and afterwards you may get something sweet’, ‘sometimes it is nice to get something sweet and other times it is nicer to stay healthy’, ‘more fruit, more times per week’, ‘can’t just always eat sweets’).
Tuck shop buying behaviour of students
Only a small percentage of students indicated that they bought items from the tuck shop on a daily basis (school A: 4 %, n 5; school B: 6 %, n 9). Students in both schools indicated that they receive pocket money of ‘R100 or more’ (approximately $US 6·89 or more) per month. Students in school A spent ‘between R6 and R10’ (approximately $US 0·41–0·69) per visit to the nutritionally regulated tuck shop, while students in school B spent ‘between R11 and R20’ (approximately $US 0·76–1·38) per visit to the conventional tuck shop.
In school A the students’ favourite items were the tuck shop’s slushy (fruit juice with crushed ice), iced lollies (frozen diluted fruit juice), fruit juice (unsweetened) and also the hot dogsFootnote * that were available once weekly on Friday. On the day of data collection, students in school A mostly bought a slushy (8 %, n 9), iced lollies (7 %, n 8) and oven-baked samoosas* (5 %, n 6) from the nutritionally regulated tuck shop. The students in school B mostly bought sweets (13 %, n 18), crisps (9 %, n 13) and carbonated cold drinks (6 %, n 8) from the conventional tuck shop (Table 2).
During the discussions some students had a negative attitude towards their nutritionally regulated tuck shop and the adjusted recipes which allowed items to have a lower fat and sugar content (‘I want a real chocolate muffin, not with carrots in it’ and ‘I do not buy there. My own food is much nicer’). The same was found in the focus group discussions where some of the students were longing for the conventional tuck shop the school used to have (‘Yes, I want that tuck shop!’, ‘energy bars and Energade are necessary before sport games’). There were, however, also suggestions for fresh fruit and a variety of salads (although one said, ‘I don’t like salad’). Other requests included cooked meals like lasagne, macaroni and cheese and meatballs. Despite negative attitudes towards the nutritionally regulated tuck shop, all groups except the grade 2 group mentioned that they sometimes also liked to buy fruit from their nutritionally regulated tuck shop.
During the discussions several students in school B indicated that they liked ‘everything’ in the conventional tuck shop. Sweets (‘ooo … sweeties!’), pies, hot dogs and crisps with cold drinks seemed to be very popular in all grades. When asked to make suggestions, the students indicated that they were mostly satisfied with their conventional tuck shop, but had suggestions for a larger variety of beverages (coffee, tea, Milo and milk), snacks (other types of sweets and chocolates) and traditional foods like boerewors (type of traditional sausage), braaivleis (barbequed meat) and hot dogs were mentioned, as well as takeaways food like potato chips, pizza and traditional desserts like koeksisters (syrup-infused type of doughnut).
Students’ lunchbox contents
Most students brought a lunchbox to school on a daily basis (school A: 81 %, n 94; school B: 83 % n 117). The majority of students in both schools had a sandwich in their lunchbox (Fig. 3), mostly made with white bread (school A: 56 %, n 65; school B: 58 %, n 82), while fewer had a brown bread sandwich (school A: 22 %, n 25; school B, 15 %, n 22). In the focus group discussions students mentioned that sandwiches with spreads and fillings such as syrup, jam, peanut butter, cheese, biltong (beef jerky) and processed meat (polony and ham) and vegetables were their favourite lunchbox items. When lunchbox contents were compared between the groups in the two schools, significant differences were found: students in school A with the nutritionally regulated tuck shop had significantly more fruit (41 %, n 47; P<0·001), muffins (10 %, n 12; P<0·05) and water (43 %, n 50; P<0·05) in their lunchboxes (Fig. 3). The students in this school interestingly also had significantly more unhealthy items such as sweets (20 %, n 23; P<0·05) and crisps (16 %, n 19; P<0·05) in their lunchboxes. During the focus group discussions students in school A mentioned that their lunchboxes contained a combination of food (hot dogs or sandwiches), fruit (fresh or dried) and also a treat (sweets, chocolates, crisps or cupcakes). Students in school B also mentioned having a ‘treat’ in their lunchbox together with their food (sandwich or hot dogs), but only two groups mentioned bringing fruit to school.
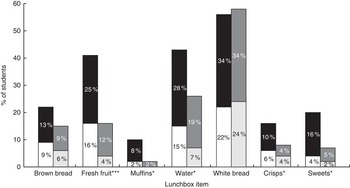
Fig. 3 Lunchbox contents of grade 2 to 7 students (n 257) by school and gender (![]() , school A boys;
, school A boys; ![]() , school A girls;
, school A girls; ![]() , school B boys;
, school B boys; ![]() , school B girls), Bloemfontein, South Africa (school A has a nutritionally regulated tuck shop, school B has a conventional tuck shop). *P<0·05, ***P<0·001 for difference between school A and school B
, school B girls), Bloemfontein, South Africa (school A has a nutritionally regulated tuck shop, school B has a conventional tuck shop). *P<0·05, ***P<0·001 for difference between school A and school B
Discussion
Based on the current study results, the presence of the nutritionally regulated tuck shop had a positive influence on certain perceptions, attitudes and behaviours of students, but some unwanted eating behaviours and negative perceptions and attitudes were also found.
The younger students in school A were more positive and accepting towards their ‘healthy’ tuck shop, while the older students (grades 4–7) showed some resistance towards the concept of having a nutritionally regulated tuck shop at their school. The WHO recommends that early intervention strategies are needed to target children while they are still developing their food habits( 4 ). Since the nutritionally regulated tuck shop was in operation for only 2 years at the time of the study, the positive attitudes of the younger students might be an indication that exposure to mostly healthy foods in the school environment can influence the eating habits of students from a young age. To ensure that these positive attitudes and behaviours will persist into adolescence further studies are needed.
Despite the negative perceptions and attitudes towards the nutritionally regulated tuck shop shown by some of the older students in school, students in all age groups bought healthy items from the tuck shop. In a study by Wiles et al., primary-school students in Pietermaritzburg, South Africa spent a mean amount of R7·09 (approximately $US 0·49) at the first school break and R9·14 (approximately $US 0·63) at the second school break( Reference Wiles, Green and Veldman 11 ). In the present study students in school A spent less money at the tuck shop, compared with students in school B. Although students at school A spent less money at the nutritionally regulated tuck shop, they had more treats in their lunchboxes. It can therefore be argued that without involving and educating parents and students, the impact of the nutritionally regulated tuck shop on the school food environment and students’ health behaviours is not significant. On the other hand, the popularity and variety of the items that were available in the conventional tuck shop at school B could also have encouraged students to spend more money.
Through the focus group discussions it became evident that in both schools the majority of students wanted a balance between healthy and unhealthy foods to be made available in their school tuck shops. Unfortunately, access to competitive food items such as sweets, crisps and sweetened beverages in the school environment promotes unhealthy food choices, since children have a greater preference for these popular items than for healthy items such as fruit, vegetables and water( Reference Utter, Schaaf and Mhurchu 9 , Reference Gosliner, Madsen and Woodward-Lopez 13 , Reference Kubik, Lytle and Hannan 15 ). In South Africa, Wiles et al. and Temple et al. also studied the types of items that school students bought from school tuck shops( Reference Temple, Steyn and Myburgh 8 , Reference Wiles, Green and Veldman 11 ). Temple et al. found that the majority of adolescents attending schools in Cape Town bought unhealthy items such as sweets, chocolate, soft drinks, French fries and potato chips from the schools’ tuck shops( Reference Temple, Steyn and Myburgh 8 ); similarly as found for the school with the conventional tuck shop in the present study. As reported by Wiles et al., the most popular items sold in tuck shops in primary schools in Pietermaritzburg, South Africa were savoury pies (similar to the school with the conventional tuck shop in the present study) and iced popsicles (like the iced lollies in the present study). Only a few school tuck shops had bananas available and these sold the least number of units( Reference Wiles, Green and Veldman 11 ). An observation can therefore be made, based on the current research study and supported by Wiles et al., that purchase is not only based on the availability of healthy items, but is also influenced by the variety offered by the tuck shop, as well as the availability of other popular unhealthy items. Researchers have recommended that unhealthy tuck shop items should be limited, while the number and variety of healthy items in school tuck shops should be increased, displayed better and marketed effectively among school students( 1 , Reference Wiles, Green and Veldman 11 ).
In the present study, more than 80 % of students in both schools brought a lunchbox to school on a daily basis. Faber et al. reported that in poorly resourced schools in South Africa, only about 24 % of students brought a lunchbox to school( Reference Faber, Laurie and Maduna 20 ) and Temple et al. found that students who attended secondary schools in Cape Town with a high socio-economic status were twice as likely to bring a lunchbox to school( Reference Temple, Steyn and Myburgh 8 ). In Temple et al.’s study only about 50 % of adolescents took a lunchbox to school( Reference Temple, Steyn and Myburgh 8 ). Abrahams et al. reported that younger students in schools in the Western Cape, South Africa were more likely to bring a lunchbox to school than older students; it was also found that students who brought a lunchbox to school were more likely to consume a diet adequate in nutrients and were less likely to be overweight or obese, whereas students who did not bring a lunchbox to school were more likely to buy unhealthy snack foods from tuck shops or vendors( Reference Abrahams, de Villiers and Steyn 21 ).
Students in school A with a nutritionally regulated tuck shop had significantly more fruit, muffins and water in their lunchboxes but, interestingly, also significantly more unhealthy items such as sweets and crisps. Thus, on the one hand, the presence of the nutritionally regulated tuck shop at school A had a positive influence on the health behaviour of students because they brought more healthy items to school in their lunchboxes; however, on the one hand, they also brought more unhealthy items from home probably because they could not buy them at school. It is therefore recommended that students should be encouraged through a school food policy to bring healthy items to school in their lunchboxes, similar to the items that are being sold at the nutritionally regulated tuck shop( Reference Temple, Steyn and Myburgh 8 ). The habit of taking a lunchbox to school should be reinforced in an attempt for this behaviour to continue throughout the school career. Greater awareness also needs to be created among parents regarding the impact of unhealthy items in lunchboxes and the influence it has on students’ daily nutrient intakes. Schools should thus collaborate with parents as their involvement can play an important role in the development of their children’s dietary behaviour( 1 , Reference Skouteris, McCabe and Swinburn 22 ).
Successful health and nutrition interventions at schools, such as the Health Promoting Schools concept, require a holistic multi-pronged approach involving parents, students, school personnel and the community who should work together with the aim of creating a healthy school environment( Reference Wang and Stewart 7 ). Although managing the availability of unhealthy food items at schools is just one component that is necessary for successful health interventions at schools, there is value in regulating the types of foods, snacks and beverages made available for purchase during school hours.
Limitations of the study
The sample used for the present study was relatively small (n 257) and included only well-resourced schools in an urban area with Afrikaans as the language of instruction. The results of the study can therefore not be extrapolated to South African students who attend poorer resourced schools or schools in rural areas, or students of other cultural groups or who do not attend Afrikaans-medium schools.
Conclusion
In the current study it was found that by offering mainly healthy foods and beverages in a school tuck shop, the types of food items available to purchase during school hours were not only regulated, but also the presence of a nutritionally regulated tuck shop in this primary-school environment also led to other positive attitudes, good eating behaviours and healthy lunchbox choices of students. Young students in school A showed a positive attitude towards the nutritionally regulated tuck shop, while students in all age groups demonstrated positive health behaviours by buying healthy items from the school tuck shop and by bringing significantly more healthy items to school in their lunchboxes. The study showed that the potential value of controlling the types of items available for purchase at school A might have been counteracted by: (i) unhealthy lunchbox items, as was found in the case of students in school A bringing more sweets and crisps to school in their lunchboxes; (ii) perceptions of students about the types of foods tuck shops should sell; (iii) negative attitudes of the older students towards the nutritionally regulated tuck shop; (iv) and previous exposure of the older students in school A to a conventional tuck shop. It can be concluded that a single intervention such as the presence of a nutritionally regulated tuck shop cannot advance the healthy school food environment in its totality. As recommended by previous studies and discussed earlier, a multi-pronged approach is recommended and awareness must be created among all role players. As in the case of the present study, the impact of a nutritionally regulated tuck shop will be insignificant unless students and parents are educated to make better food choices and pack healthier lunchboxes.
Acknowledgements
Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: None. Authorship: The principal researcher, F.B., developed the idea and the protocol for this research study, planned the research, undertook data collection (with the assistance of a trained research assistant), captured the data for analyses, analysed the data with the assistance of a statistician, interpreted the data and drafted the research thesis and article. Fellow researchers, M.M. and N.K. (supervisors), provided input at all stages and revised the protocol, thesis and article. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures were approved by the Health Research Ethics Committee at the Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa (ethics reference number N10/08/246). Permission was also obtained from the Department of Education in the Free State Province, the principals of the three primary schools and the tuck shop managers. Participation was voluntary and only students with a signed consent form from a parent/guardian and students who also gave written assent participated in the study. The consent form provided a separate section on voice recording of the focus group discussions.