


Obesity is a major risk factor for several serious chronic diseases, including CVD and type 2 diabetes mellitus (T2DM)(Reference Poirier, Giles and Bray1). In addition, obesity is associated with some cancers, gallbladder disease, hypertension and osteoarthritis(Reference Poirier, Giles and Bray1–Reference Weiss, Dziura and Burgert8). The measurement of obesity in children and adolescents, as in adults, is an important first step in the recognition and reduction of CVD and T2DM and their potential consequences(Reference Poirier, Giles and Bray1–Reference Weiss, Dziura and Burgert8), as obesity has been shown to track into adulthood(Reference Freedman, Khan and Serdula5).
Simple reliable methods for measuring overall obesity exist and include measuring weight (kg) and dividing it by the square of the height (m2) to obtain the BMI. An alternative and increasingly used measure of obesity is waist circumference (WC), which reflects abdominal fat accumulation. Recent studies show that WC in adults(Reference Janssen, Katzmarzyk and Ross2, Reference Carr, Utzschneider and Hull3) and children(Reference Zimmet, Alberti and George4–Reference Weiss, Dziura and Burgert8) may be a more sensitive indicator of future cardiovascular risk than BMI. Consequently, most researchers and expert organizations now assert that WC should be used in screening for metabolic syndrome (MS). Two such organizations, the National Cholesterol Education Program (NCEP) of the USA and the International Diabetes Federation (IDF), both use WC as one of the five indicators of MS, a condition that is associated with increased risk of CVD and T2DM(Reference Carr, Utzschneider and Hull3, Reference Zimmet, Alberti and George4). The five indicators that indicate high risk for MS are elevated blood pressure, large WC, hyperglycaemia, high TAG levels and low levels of HDL cholesterol.
In the IDF definition, a large WC (along with any two additional indicators) is central to the diagnosis of MS, while with the NCEP definition, possession by an individual of any three of the five indicators constitutes the presence of MS(Reference Zimmet, Alberti and George4, Reference Savva, Tornaritis and Savva7).
On account of lifestyle changes associated with the transition in nutrition in the Arabian Gulf, resulting principally from rising incomes associated with the discovery and production of oil over the past few decades, obesity has increased dramatically(Reference Musaiger9, Reference Jackson, Al-Mousa and Al-Raqua10). El Bayoumy et al.(Reference El Bayoumy, Shady and Lofty11) found that the overall prevalence of overweight and obesity among men was 29·3 % and 14·9 %, respectively, (P < 0·001) and the prevalence of overweight and obesity among women was 32·1 % and 14·2 %, respectively (P < 0·001). Studies have shown that with new affluence has come increased availability of fast-food restaurants and ready availability of other semi-fast food establishments in all Gulf countries, including Kuwait(Reference Musaiger9, Reference Mabry, Reeves and Eakin12). In addition to the ready availability of energy-dense fast foods, many Kuwaiti citizens are less physically active than their predecessors(Reference Mabry, Reeves and Eakin12). Of the over 2·6 million total population of Kuwait, about one-half of the population is of ‘migrant’ workers who perform much of the manual labour done in Kuwait. The increased availability of energy-dense foods and the concomitant decrease in activity has been documented in the Gulf (which includes Kuwait) and is believed to be the main reason why diseases such as T2DM and CVD(Reference El Bayoumy, Shady and Lofty11–Reference Al-Adsani, Moussa and Al-Jasem14) have increased dramatically over the past several years. Of great concern is the finding that chronic diseases are also increasing among children and adolescents(Reference El Bayoumy, Shady and Lofty11, Reference Moussa, Alsaeid and Abdella15).
Virtually all studies of obesity in adults and children in Kuwait have measured BMI(Reference Jackson, Al-Mousa and Al-Raqua10, Reference Al Isa and Thalib16–Reference Al Isa and Thalib18) as the yardstick to measure obesity. No large-scale epidemiological studies have examined WC, despite the fact that WC is thought to be more reliably related to MS than is BMI(Reference Janssen, Katzmarzyk and Ross2, Reference Carr, Utzschneider and Hull3, Reference Savva, Tornaritis and Savva7, Reference Zannolli and Morgese19).
The objective of the present study was to develop smoothed WC percentiles for Kuwaiti children and adolescents between 5·0 and 18·9 years of age that could be used to inform public health practice. We also sought to examine the percentages of Kuwaiti children, at each age, who had WC that exceeded the 90th percentile, a value that is commonly said to indicate elevated risk for MS(Reference Lee, Davis and Woolford6, Reference Weiss, Dziura and Burgert8). Finally, we sought to examine the correlation between overall obesity (defined by BMI values) and abdominal obesity (measured by WC values) in this child and adolescent population.
Subjects and methods
The study included 9593 healthy male and female students who were interviewed and measured in primary, intermediate and secondary schools in Kuwait. The sample included 5014 children (5·0–9·9 years) and 4579 adolescents (10·0–18·9 years). The data were collected as part of the Kuwait National Nutrition Surveillance System (KNNS). The KNNS system has been described elsewhere(Reference Jackson, Al-Mousa and Al-Raqua10, Reference Jackson, Al-Mousa and Al-Raqua20); however, in brief, it includes children and adults from all geographical locations (governorates) of Kuwait. It includes measurements of weight and height, WC and cholesterol values in some subgroups. It also includes several sociodemographic variables. It is designed to continuously monitor the nutritional health status of different Kuwaiti population groups and to provide data as an instrument of policy formulation and health intervention evaluation for health workers and decision makers. In the present study, adolescents are children who are between 10 and 19 years of age.
A structured questionnaire was used to elicit a variety of information including age, gender, location of residence and school grade level of pupils.
Non-fasting cholesterol levels were measured in a subsample of 1497 children who were more than 10 years of age. Cholesterol was measured from capillary blood taken from the finger in adolescents who were in a sitting position. Cholesterol was analysed using a Reflotron (Boehringer Mannheim, Germany); this device meets the performance standards of the American NCEP Laboratory Standardization Panel.
Weight, height and WC were also measured. Weight was measured to the nearest 0·1 kg and height was measured to the nearest 0·1 cm. WC was measured to the nearest 0·1 cm mid-way between the inferior margin of the lower rib and the top of the iliac crest. BMI was calculated as the weight (kg) divided by the square of height (m2). We used WC ≥90th percentile as evidence of elevated risk for obesity-related cardiovascular disorders(Reference Lee, Davis and Woolford6, Reference Weiss, Dziura and Burgert8). Thus, we dichotomized the population into those children and adolescents who were <90th percentile (lower risk) and those who were ≥90th percentile (higher risk). The basic prevalence estimates of higher risk were generated by examining the number of children with WC ≥ 90th least median square (LMS) regression percentile values for each age and sex category (see Tables 2 and 3). LMS regression resulted in cut-off values at each selected percentile (e.g. 75th, 90th, etc.). We then found the percentage of children in each age and sex category whose WC value was same or more.
Statistical analysis was carried out using descriptive statistics, including means and frequencies and inferential statistics that included correlation coefficients and independent sample t tests. To produce smoothed WC percentile graphs and tables, the software program Chartmaker Pro (Institute of Child Health, London, UK) was used to carry out LMS regression using the method developed by Cole and Green(Reference Cole and Green21). The LMS procedure resulted in a WC cut-off for male children and another for female children at each percentile (3rd, 10th, 25th, 50th, 75th, 90th and 97th percentiles) for each age category. Graph and table percentiles calculated were the 3rd, 10th, 25th, 50th, 75th, 90th and 97th percentiles. The LMS method involved summarizing the percentiles at each age (separately for male and female children in the present study) on the basis of the Box–Cox power transformations, which are used to normalize the data. The final percentile curves were the result of smoothing three age-specific curves, termed lambda (L), mu (M) and sigma (S). The L, M and S curves describe the skewness, median and CV of the distribution of WC at each age(Reference Cole and Green21). Statistical analyses were carried out with the Statistical Package for Social Sciences statistical software package version 17·0 (SPSS Inc., Chicago, IL, USA). Significance was defined as P ≤ 0·05.
Results
The sample of 9593 included 4843 (50·5 %) male and 4750 (49·5 %) female children. The overall age range of the sample was 5·0–18·9 years. The mean (sd) age of male children was 11·0 (sd 3·9) years, whereas it was 10·9 (sd 3·9) years for female children.
Table 1 shows the number, mean and sd of WC and BMI values of Kuwaiti children and adolescents aged 5·0–18·9 years by sex. The mean WC generally increased with age for both male and female children. The BMI values of male and female children also generally increase with age. However, the BMI means for ages 8, 9 and 10 years are higher than at other ages. From the age of 10 years, male children have higher WC values than do female children, as is evident from Table 1. The mean BMI values of male children are generally higher than those of female children at most ages.
Table 1 Mean WC and BMI of Kuwait children aged 5·0–18·9 years by sex
WC, waist circumference.
*Percentage with WC values ≥90th percentile.
Tables 2 and 3 show the smoothed WC percentile values for male and female children at various percentiles (3rd, 10th, 25th, 50th, 75th, 90th and 97th), respectively. They also show that waist percentiles increase with age for both male and female children. The tables also show the percentage of male and female children at each age who had WC ≥ 90th percentile. The tables indicate that between 7·9–16·7 % and 1·8–13·4 % of male and female children, respectively, had a WC ≥ 90th percentile, a value frequently considered to be evidence of elevated risk for MS(Reference Lee, Davis and Woolford6, Reference Weiss, Dziura and Burgert8). As can be seen from Table 1, the percentage of male children exceeding the 90th percentile was larger than the percentage of female children exceeding that value at every age ≥6 years. The smoothed percentile curves for female and male children are shown in Figs 1 and 2, respectively.
Table 2 Smoothed WC percentiles (in cm) for Kuwaiti male children
WC, waist circumference.
*Percentage with WC values ≥90th percentile.
Table 3 Smoothed WC percentiles (in cm) for Kuwaiti female children
WC, waist circumference.
*Percentage with WC values ≥90th percentile.
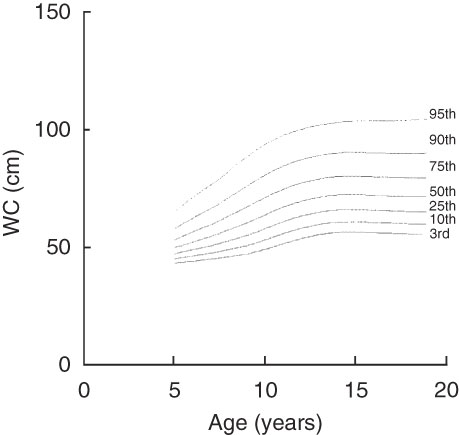
Fig. 1 Smoothed waist circumference (WC) percentiles for female Kuwaiti children aged 5–19 years
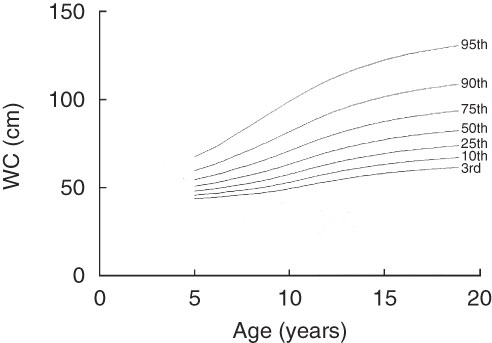
Fig. 2 Smoothed waist circumference (WC) percentiles for male Kuwaiti children aged 5–19 years
Above the age of 7 years, male children have higher WC percentiles than female children at the 50th, 75th, 90th and 97th percentiles. Thus, it seems that the dramatic increase in WC is established in male children starting as early as at the age of 7 years. Before the 7th year, female children have higher WC percentiles at these four percentile levels (50th, 75th, 90th and 97th).
For primary school-aged children the mean BMI of female (n 2497) and male children (n 2517) was 27·6 (sd 9·1) kg/m2 and 27·7 (sd 9·1) kg/m2, respectively. The mean WC of female children was 58·1 (sd 9·6) cm, whereas the mean WC of male children was 58·4 (sd 9·8) cm.
The mean BMI of female (n 2253) and male adolescents (n 2326) was 25·2 (sd 8·1) kg/m2 and 25·3 (sd 8·7) kg/m2, respectively. The mean WC of female adolescents was 72·6 (sd 11·9) cm, whereas the mean WC of male adolescents was 78·5 (sd 15·7) cm. Male adolescents maintained a slightly higher mean BMI than did female adolescents. However, the mean WC of male adolescents was significantly higher (P < 0·01) than that of female adolescents.
A WC ≥ 90th percentile is thought to confer increased risk of developing MS(Reference Lee, Davis and Woolford6, Reference Weiss, Dziura and Burgert8). When we dichotomized our sample by gender into those with WC ≥ 90th percentile and those with WC < 90th percentile, we found that the mean BMI of male and female children, whose WC was ≥90th percentile, was significantly greater (P < 0·01) at every age than those who had WC <90th percentile.
The Pearson correlation (r) of WC and BMI in primary school-aged female children was 0·879 (n 2497, P < 0·01), whereas the correlation in primary school-aged male children was slightly higher (r = 0·896, n 2517, P ≤ 0·01). The correlation of WC and BMI in female adolescents was 0·595 (n 2253, P < 0·01), whereas it was slightly higher in male adolescents (r = 0·656, n 2326, P ≤ 0·01).
For male children, the partial correlations (controlling for age) between cholesterol values and WC (r = 0·218, n 761, P = 0·001) and between cholesterol and BMI (r = 0·217, n 761, P = 0·001) were both highly significant. For female children, the correlations between cholesterol values and WC (r = 0·099, n 728, P = 0·007) and between cholesterol and BMI (r = 0·080, n 728, P = 0·030) were also significant.
Discussion
Obesity is increasing worldwide among adults and among children and adolescents(Reference Poirier, Giles and Bray1–Reference Weiss, Dziura and Burgert8, 22). There is growing evidence that abdominal obesity is associated with increased risk for T2DM, dyslipidaemia (elevated TAG and lowered HDL cholesterol levels), hypertension and CVD(Reference Freedman, Serdula and Srinivasan23). WC is a sensitive measure of abdominal fat(Reference Janssen, Katzmarzyk and Ross2, Reference Carr, Utzschneider and Hull3, Reference Savva, Tornaritis and Savva7). Several experts recommend that WC should be used for children and adults when screening for potential CVD and T2DM risk(Reference Lee, Davis and Woolford6–Reference Weiss, Dziura and Burgert8, Reference Moussa, Alsaeid and Abdella15, Reference Zannolli and Morgese19, Reference Freedman, Serdula and Srinivasan23).
WC cut-off values have been proposed for children and adolescents of several Western countries (e.g. Italy(Reference Zannolli and Morgese19), Spain(Reference Moreno, Fleta and Mur24), Britain(Reference McCarthy, Jarrett and Crawley25), USA(Reference Fernández, Redden and Pietrobelli26), Canada(Reference Katzmarzyk27), etc.); however, waist cut-off values do not exist for Kuwaitis or for most other Gulf Arab children and adolescents. We know from adult studies that body fat distributions vary across ethnic groups, leading NCEP and IDF to call for the application of different WC cut-offs for some non-Western populations. Given the high rate and growing trend towards obesity worldwide(22), including in Kuwait and other Gulf countries, the development of age- and gender-specific WC cut-offs is needed.
These are the first age- and gender-specific comprehensive smoothed WC growth curves developed for Kuwaiti children and adolescents. Given the precipitous increase in overweight and obesity in Kuwait(Reference Moussa, Alsaeid and Abdella15–Reference Al Isa and Thalib18), the use of these curves and tables can provide early identification of children who may be at higher risk for future CVD and T2DM(Reference Lee, Davis and Woolford6, Reference Weiss, Dziura and Burgert8).
We found that male children had higher WC percentiles than female children at most of the ages that were studied. These results are similar to those found from other adolescent populations, in which e.g. Fernandez et al.(Reference Fernández, Redden and Pietrobelli26) in Americans and Katzmarzyk(Reference Katzmarzyk27) in Canadians also found that male children had higher WC percentiles than female children for most of the ages they studied. Thus, our Kuwait results can be seen as a part of a larger worldwide trend towards greater overall and abdominal obesity, particularly among male children.
The 90th percentile is commonly suggested(Reference Lee, Davis and Woolford6, Reference Weiss, Dziura and Burgert8) as a cut-off percentile at and above which the risk for MS and CVD increases substantially. Of male children 8·0–16·7 % (for an average of 12 %) over the entire 5·0–18·9-year age range in our study had WC percentiles ≥90th percentile. In female children, between 2·0 % and 13·0 % (for an average of 7·6 %) over the entire age range had values ≥90th percentile. In fact, male children had a greater percentage of individuals above the 90th percentile at nearly every age (>6 years of age) in our study.
The percentage of male children who exceed the 90th percentile was more or less constant (averaging about 12 %) over the 5·0–18·9-year age range. However, the percentage of girls exceeding the 90th percentile declined after the age of 10 years. Thus, for this sample, the age of 11 years seems to be a transition age, with ages ≥11 years showing substantial decreases in the percentage of girls with WC ≥90th percentile. Our cross-sectional study cannot answer why this observed difference occurs or what causes it. Additional studies are needed to ascertain why this dramatic gender-related decrement occurs in percentages exceeding the 90th percentile in female children. It may be related to gender-related maturational or possibly to cultural differences in exercise patterns between male and female children.
The age of 10 years is the age that represents the transition age between primary and intermediate schools in Kuwait. The mean BMI values at the age of 9 and 10 years were inexplicably high. Perhaps, the diet or exercise regimes differ between the two school levels. In 2003, Al Isa(Reference Al Isa17) reported that obesity increased in Kuwaiti men and women between 1980–1981 and 1993–1994, but that the increase in obesity was slightly greater in men than in women. In a later study, in adolescents, Al Isa and Thalib(Reference Al Isa and Thalib16) studied BMI in 10–14-year-old Kuwait children and found that the percentage of obesity was higher in male children, particularly at the higher percentiles (75th through the 95th) of the BMI distribution. Therefore, these studies using BMI as a measure of overall fatness show that male adolescents and adults have greater obesity than do female adolescents. Al Isa(Reference Al Isa17) pointed to changes in the levels of affluence, excessive food consumption and sedentary behaviour to explain the increasing obesity rates and gender differences in obesity in this age group. Mabry et al.(Reference Mabry, Reeves and Eakin12) also indicate that changing exercise patterns may account for the increases in obesity in Gulf countries(Reference Mabry, Reeves and Eakin12).
In a later study, Al Isa and Thalib(Reference Al Isa and Thalib18) found that the BMI values of Kuwaiti boys aged 3–9 years exceeded those of girls at those ages. Those results are similar to the results that we found for the WC values of boys and girls. In our study, there was no consistent pattern in the mean BMI between male and female children at 5–14 years of age. However, the mean BMI values of older male adolescents (15–18 years) were larger than those of older female adolescents. The correlation between WC and cholesterol values was stronger and more highly significant in male than in female children. This supports the finding that men are at greater risk due to their larger WC values.
Thus, our results show clearly that males are at greater risk and that intervention in this group is urgently required to understand and reverse this finding. Child and adolescent overweight and obesity have been shown to track into adulthood(Reference Freedman, Khan and Serdula5, Reference Whitaker, Wright and Pepe28), thus increasing the risk for later development of CVD and T2DM.
Above the age of 10 years, male children have higher WC percentiles than female children at the 50th, 75th, 90th and 97th percentiles. Further research is needed to explain why this clear trend towards bigger WC occurs in male children between 11·0 and 18·9 years of age and why this age seems to be the transition age. However, this suggests that starting at the age of 10 years, WC should be measured in male and female children as after this age the correlation of BMI and WC is low and expert groups(Reference Zimmet, Alberti and George4) have found WC to be a better indicator of CVD risk than BMI. Moreover, the correlation of WC with cholesterol values was more significant than that of BMI and cholesterol values, indicating that WC is more highly related to metabolic risk than is the current measure of obesity and BMI.
As relatively few health-care professionals routinely measure WC, efforts are needed to promote the measurement of this anthropometric indicator as an important tool in paediatric primary care practice. It is clear that these age- and gender-specific WC percentiles can be used as a tool to impact public health recommendations and practice vis-à-vis children and adolescents in Kuwait and other Gulf countries.
These are the first age- and gender-specific comprehensive smoothed WC growth curves developed for Kuwaiti children and adolescents. Owing to the genetic and ethnic similarities of Gulf Arab children(Reference Al Isa and Thalib18), these WC percentiles might be able to be used in other Gulf populations where WC percentiles do not currently exist. The comparison of observed values of other Gulf children and adolescents to the 90th or 95th percentiles of these tables may be particularly helpful. Second, this is a large representative study of both sexes over a wide age range. Thus, the present study can be used as a basis for comparison for children of similar ages performed in different countries outside the Arabian Gulf.
The cross-sectional nature precludes us drawing conclusions about the associations we observed in the present study. Only longitudinal studies that track anthropometric indicators and other metabolic indicators of risk can definitively answer questions about the relationship of WC to proven cardiovascular risk. Other indicators of the MS (e.g. blood lipids, blood glucose and blood pressure) were not measured in the present study. The direct correlation of these indicators with WC would have given a stronger indication of risk.
Acknowledgements
The present study received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. The authors have no conflict of interest to declare. R.T.J. analysed the data and prepared the draft and final manuscript; N.A.H. planned the research and contributed to writing and editing the manuscript; P.P. read various drafts of the manuscript and also cleaned and did preliminary analyses of the data; M.A.S. oversaw the field research team, helped to develop the questionnaire for the research and also contributed to editing the final manuscript.





