


In Europe, CVD, diabetes and cancer are some of the leading causes of death and account for a large proportion of the disease burden in the region( 1 ). Still, these conditions are all largely preventable by tackling modifiable risk factors, including unhealthy diet( Reference Benziger, Roth and Moran 2 , 3 ). More recently, the emerging field of ‘chrono-nutrition’ has been emphasized as research suggests that eating at the ‘wrong time’ may impair metabolism and that misalignment between timing of eating and endogenous circadian systems is associated with increased inflammation and adverse health outcomes( Reference Garaulet and Gomez-Abellan 4 – Reference Almoosawi, Vingeliene and Karagounis 8 ). For example, observational studies have shown that later-night eaters have an increased risk of CHD( Reference Cahill, Chiuve and Mekary 9 ) and that shift workers have a higher risk of developing type 2 diabetes compared with day workers, which is believed to reflect greater consumption of energy intake during the night( Reference Pan, Schernhammer and Sun 10 , Reference Parkes 11 ). Furthermore, high evening relative to morning energy intake has been positively associated with BMI( Reference Aljuraiban, Chan and Oude Griep 12 ) and individuals consuming a larger proportion of daily energy at dinner (≥48 % of total energy intake) have been found to have an increased risk of obesity, metabolic syndrome and non-alcoholic fatty liver disease, even after adjusting for a set of covariates including breakfast skipping, total energy intake and dietary fibre( Reference Bo, Musso and Beccuti 13 ). Thus, not only the amount and content of food intake, but also elements such as timing of food intake need to be considered as potential risk factors for diet-related chronic diseases.
In the USA, the American Dietetic Association states that greater consumption of energy intake during the day may be preferable to evening consumption for weight management( Reference Seagle, Strain and Makris 14 ). In the European guidelines for obesity management in adults, general advice is given to avoid breakfast skipping and eating at night( Reference Yumuk, Tsigos and Fried 15 ). However, despite the potential health implications of timing of eating, associated individual characteristics and their variation among different populations, cultures and geographical regions have rarely been investigated. This is likely due to the inconsistent approaches used to examine meal patterns, including a lack of standardized terminology, heterogeneity in how meal patterns are analysed and the wide range of assessment methods used, making interpretation and comparability between studies and countries problematic( Reference Leech, Worsley and Timperio 16 , Reference Bellisle 17 ). Nevertheless, from a public health perspective, information on sociodemographic, sociocultural and lifestyle characteristics associated with timing of eating is needed to guide the development of evidence-based dietary recommendations and identify at-risk groups for preventive actions.
In a recent report, we utilized the standardized and homogeneous methodology used in the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study to characterize meal patterns across ten European countries. We found distinct differences in meals patterns across Europe, with marked diversity for intake frequency and proportional energy contribution from meals and snacks between Mediterranean and Central/Northern European countries( Reference Huseinovic, Winkvist and Slimani 18 ). However, differences in timing of eating were not covered in that report. Such analyses have the potential to further map geographical differences in meal patterns and provide a valuable resource and benchmark for Europe. Hence, the aim of the present paper was to describe meal timetables and to examine the timing of eating and its association with sociodemographic, lifestyle and health-related characteristics in women and men from ten European countries.
Methods
Study population
The present paper is based on data collected within the EPIC calibration study, a nested study within EPIC undertaken during 1995–2000. Details of the rationale, design and populations of EPIC, and of the calibration study, have been described elsewhere( Reference Riboli, Hunt and Slimani 19 , Reference Slimani, Kaaks and Ferrari 20 ). In short, EPIC is a multicentre cohort study aimed at investigating the association between dietary, biological, lifestyle and environmental factors in the aetiology of cancer and other chronic diseases. The EPIC project began in 1992 and includes 520 000 participants recruited from twenty-three administrative centres (reclassified into twenty-seven centres according to geographical region) in ten Western European countries: Greece, Spain, Italy, France, Germany, the Netherlands, the UK, Denmark, Sweden and Norway. Participants were mostly recruited from the general population, with some exceptions: women attending mammography screening (one centre in the Netherlands and one in Italy), women members of a health insurance for employees of the National Education System (France) and blood donors (some centres in Italy and Spain). Hence, nineteen of the twenty-seven EPIC regions recruited both women and men while eight regions recruited women only. In Oxford (UK), most participants were vegetarians or vegans and/or had a special interest in health, and are therefore evaluated separately (the ‘UK Health-conscious’ in contrast to the ‘UK General population’). The EPIC project was approved by the ethical review boards of the International Agency for Research on Cancer (Lyon, France) and from all local centres. Written informed consent was obtained from all participants.
The calibration study was designed to account for random and systematic errors from food frequency-derived dietary data in EPIC and to enable examination of dietary data according to the same reference scale. The calibration study population was an age- and sex-stratified random sample of 36 994 participants from the total EPIC cohort (~8 %) and involved a single 24 h diet recall to be used as reference calibration method( Reference Slimani, Kaaks and Ferrari 20 – Reference Ferrari, Day and Boshuizen 22 ). The results in the present paper are based on dietary data from the standardized 24 h diet recalls.
Dietary assessment
The 24 h diet recalls were collected using the standardized and computerized software EPIC-SOFT (now renamed GloboDiet). The structure and functions of the software program have been described in detail elsewhere( Reference Slimani, Kaaks and Ferrari 20 , Reference Slimani, Deharveng and Charrondiere 23 ). In short, EPIC-SOFT was administered by trained interviewers through face-to-face interviews in all countries except in Norway, where telephone interviews were performed. The interviews were structured into two steps: a first step where participants were asked to recall all foods and drinks consumed during the previous day; and a second step where they were asked to quantify and describe their intake. To standardize the memory aids used by the interviewers during the recall, eleven predefined food consumption occasions (FCO) were asked for, and information on all foods and drinks consumed were entered as one of the following FCO according to the participants’ description: (i) before breakfast, (ii) breakfast, (iii) during morning, (iv) before lunch, (v) lunch, (vi) after lunch, (vii) during afternoon, (viii) before dinner, (ix) dinner, (x) after dinner and (xi) during evening. These FCO were defined to chronologically cover the different occasions of consumption during the day and consider the different food habits among the participating countries. Hence, a FCO could consist of single or combined food/s and/or drink/s. For each FCO, time of consumption was indicated per hour as integer values (e.g. 08.00, 09.00 hours, etc.) and each FCO, except for breakfast, lunch and dinner, could be selected several times during the day because of intakes in different hours (e.g. FCO ‘during afternoon’ consumed at both 14.00 and 17.00 hours). During the interview, participants were asked to list all foods and drinks consumed between waking up on the recall day and waking up on the next day, usually the interview day. However, interviews with regard to diet on Saturdays were conducted on Mondays in most countries for logistical reasons. The mean duration of the recalled day was always about 24 h( Reference Slimani, Kaaks and Ferrari 20 ) and interviews were conducted over various seasons and days of the week. For calculation of energy intake, the EPIC Nutrient Database, developed to standardize the national nutrient databases across the ten EPIC countries, was used( Reference Deharveng, Charrondiere and Slimani 24 , Reference Slimani, Deharveng and Unwin 25 ).
Non-dietary variables
The baseline examination in EPIC was performed during 1992–1998 and included detailed self-administered questionnaires on diet, medical history and lifestyle, which have been described elsewhere( Reference Riboli, Hunt and Slimani 19 , Reference Haftenberger, Schuit and Tormo 26 , Reference Friedenreich, Cust and Lahmann 27 ). Through these questionnaires, data were collected on education level (none, primary, technical/professional, secondary, university), marital status (single, married/living together, divorced/separated and widowed), smoking (never, former, current), physical activity (inactive, moderately inactive, moderately active, active), diabetes (yes, no) and hyperlipidaemia (yes, no). To assess physical activity, the Cambridge physical activity index with four categories was used, which has been validated within the EPIC study and showed no significant heterogeneity by country( Reference Peters, Brage and Westgate 28 ). For the calibration study, information on age, body weight and height were self-reported during the 24 h diet recall, and BMI was calculated as weight divided by the square of height. The mean time interval between the baseline examination and the 24 h diet recall varied between countries, from 1d to 3 years( Reference Slimani, Kaaks and Ferrari 20 ).
Meal timetables and temporal distribution of food consumption occasions
Meal timetables across the countries are displayed to illustrate time of consumption of meals (breakfast, lunch and dinner) and snacks (all other FCO) during the 24 h diet recall. Likewise, the proportion of FCO per hour for all EPIC countries are displayed in Fig. 1 to demonstrate temporal distribution. In line with our previous publication( Reference Huseinovic, Winkvist and Slimani 18 ), we included all FCO in the analyses except for FCO consisting of water only (tap or mineral water), which were excluded. In addition, we also present Supplemental Fig. 1 (see online supplementary material) where only FCO containing ≥209·2 kJ (≥50 kcal) are included to enable comparison with other studies using an energy content criterion to define an intake occasion( Reference Leech, Worsley and Timperio 16 ).
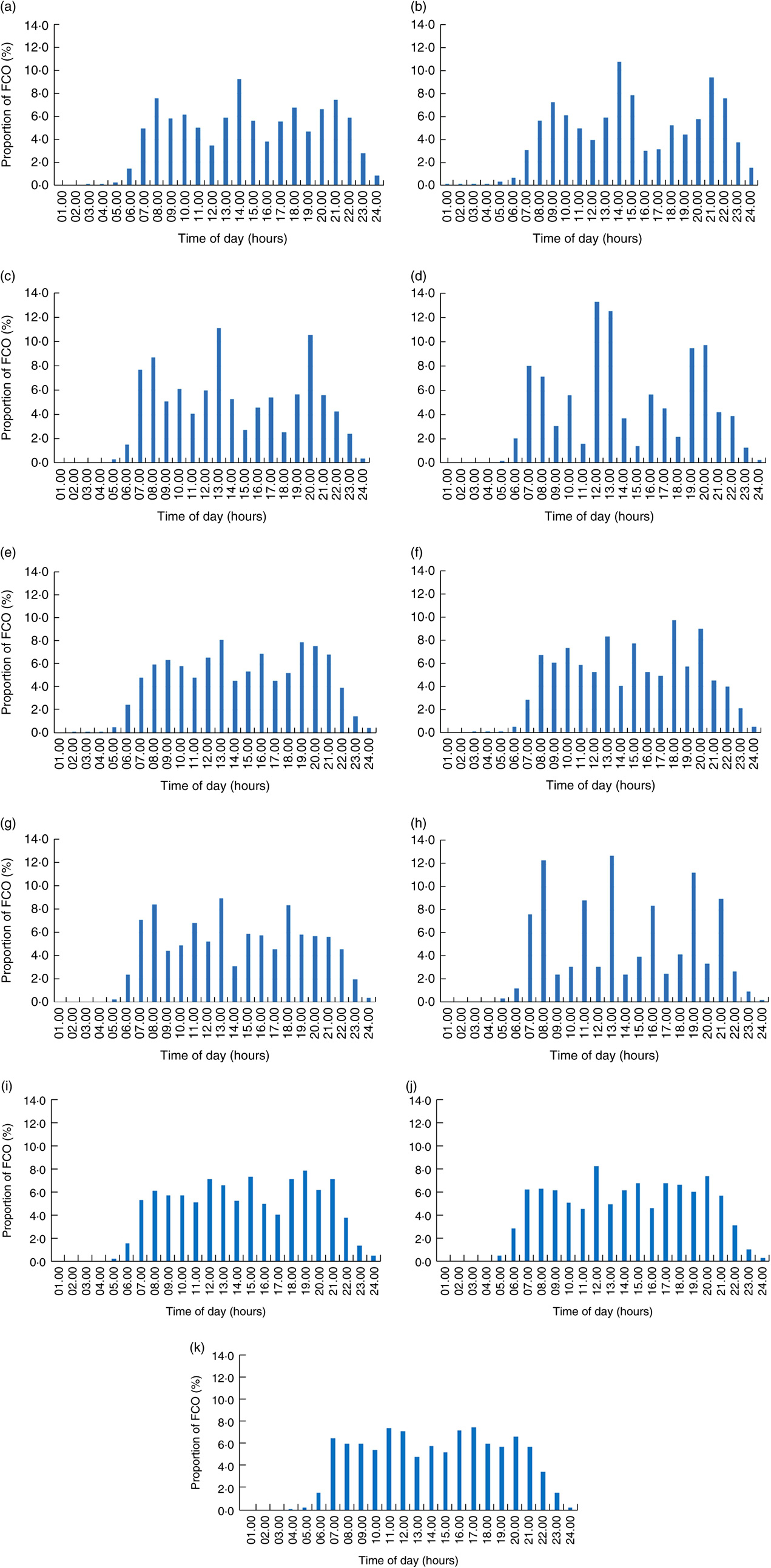
Fig. 1 Proportion of food consumption occasions (FCO) reported per hour throughout the day for the ten countries in the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study: (a) Greece (n 2692); (b) Spain (n 3220); (c) Italy (n 3952); (d) France (n 4735); (e) Germany (n 4414); (f) the Netherlands (n 3966); (g) UK General population (n 977); (h) UK Health-conscious (n 309); (i) Denmark (n 3917); (j) Sweden (n 6041); (k) Norway (n 1797). All FCO except for FCO consisting of water only are included
Later:earlier energy intake ratio
Timing of eating was examined as the later:earlier energy intake ratio, in line with previous research( Reference Aljuraiban, Chan and Oude Griep 12 ). Earlier intakes were defined as 06.00–14.00 hours, and later intakes as 15.00–24.00 hours. These time points were selected after studying the distribution of FCO and time of consumption of meals (Fig. 1 and Table 1) with the aim to produce two time periods that could be compared across a broad geographical span. This cut-off has previously been used to distinguish later v. earlier energy consumers( Reference Kaczmarek, Musaad and Holscher 29 ). Hence, a ratio of <1·0 indicates greater energy load earlier during the day (06.00–14.00 hours) and a ratio of >1·0 indicates greater energy load later during the day (15.00–24.00 hours). To enable calculation of the ratio among all participants, earlier energy intakes that equalled 0 kcal (i.e. the denominator) were replaced with 1 kcal.
Table 1 Time (hours) of consumption of food consumption occasions across ten European countries in the European Prospective Investigation into Cancer (EPIC) calibration study

Values are mode; similar results were observed for medians, see online supplementary material, Supplemental Table 1.
Statistical analysis
Data are presented as mean, range, median, 1st–3rd quartile and mode. Type III tests of the generalized linear model procedure were used to evaluate associations between a priori selected variables (based on previous research and available data) and the later:earlier energy intake ratio, given all covariates in the model. The variables evaluated were country, age, educational level, marital status, smoking status, physical activity, BMI, prevalence of hyperlipidaemia and diabetes, day of recall and season. All variables were entered into the model as categorical variables except for age and BMI. The ratio was log-transformed before being entered into the model to correct for positive skewness. Adjusted R 2 is presented to display the variation in the ratio explained by the model, given all entered variables. Only data on participants who had complete covariate information were used in the model. All analyses are stratified by sex. Data were analysed using the statistical software package IBM SPSS Statistics version 21.0. Statistical significance was considered at P<0·05.
Results
Study participants
A total of 36 020 participants (22 985 women and 13 035 men) with dietary data from the 24 h diet recall were included after exclusion of participants aged under 35 years or over 74 years due to low participation in these age groups (n 960) and of individuals with incomplete information (n 14). Mean (range) age for women and men ranged from 49·0 (35·0–65·5) and 50·0 (35·2–65·2) years (Bilthoven, the Netherlands) to 61·4 (45·3–74·2) and 64·1 (50·5–74·3) years (Malmö, Sweden), respectively. Mean BMI of women ranged from 22·9 (14·4–37·6) kg/m2 (South of France, France) to 29·3 (17·9–48·8) kg/m2 (Granada, Spain), and from 23·9 (18·2–31·8) kg/m2 (UK Health-conscious) to 29·3 (20·9–46·2) kg/m2 (Granada, Spain) for men. For the Type III tests evaluating the association between the ratio and selected variables, 13 132 women and 5680 men had complete covariate information.
Meal timetables
Overall, time of consumption of meals and snacks varied across the countries according to a south–north gradient (Table 1 and online supplementary material, Supplemental Table 1). As for breakfast, this was most often consumed at 07.00 hours in Sweden, Norway and France compared with 09.00 hours in Spain (Table 1). Following the time of breakfast, lunch was consumed earlier in the Nordic countries (12.00 hours) compared with Spain and Greece (14.00 hours). The greatest heterogeneity was observed for dinner, which was most frequently consumed between 16.00 and 19.00 hours in the Nordic countries compared with 20.00–21.00 hours in the Mediterranean countries. As for snacks, the largest difference was observed for the FCO ‘during afternoon’, where the most common time of consumption ranged from 14.00 hours in Norway to 18.00 hours in Spain and Greece, and for the FCO ‘during evening’, which ranged from 20.00 hours in Sweden to 24.00 hours in Spain.
Temporal distribution of food consumption occasions
In general, more distinct peak times for temporal distribution of FCO were observed in Mediterranean countries compared with Central/Northern European countries (Fig. 1). This was particularly prominent in France and Italy, where three peak times emerged at 07.00–08.00, 12.00–13.00 and 19.00–20.00 hours. In contrast, less pronounced peaks were observed in e.g. the Nordic countries, where FCO were more evenly spread across the day. Across all countries, the most defined peak time appeared at lunch time, with most countries displaying high frequency of FCO at 12.00–14.00 h. Similar patterns were observed when only FCO consisting of ≥209·2 kJ (≥50 kcal) were included (see online supplementary material, Supplemental Fig. 1), although the peak times appeared more distinct after removal of small energy intakes. Temporal distribution of energy intake is presented in Supplemental Fig. 2.
Later:earlier energy intake ratio
A south–north gradient for the later:earlier energy intake ratio emerged, with Mediterranean countries (median ratio of 0·76) demonstrating a lower ratio compared with Central and Northern European countries (median ratio of 1·13 and 1·15, respectively). For women, the median ratio ranged from 0·68 in France to 1·39 in Norway (Table 2), and for men from 0·71 in Greece to 1·35 in the Netherlands (Table 3). In addition, geographical differences for the ratio were observed within countries, with the ratio ranging from e.g. 0·66 (Navarra) to 2·04 (Granada) among women and from 0·72 (Navarra) to 2·58 (Granada) among men in Spain. In contrast, smaller within-country variations were observed for e.g. women in France (range 0·63–0·72) and men in Italy (range 0·73–0·88; see online supplementary material, Supplemental Tables 2 and 3).
Table 2 Later:earlier energy intake ratio across sociodemographic, lifestyle and health variables for women in the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study*
*Type III tests of the generalized linear model procedure were used to evaluate associations between a priori selected variables and the ratio, given all covariates in the model. The ratio was log-transformed before entered into the model to correct for positive skewness. In total, the following number of women were missing covariate information: 381 women for educational status, 3960 women for marital status, 398 women for smoking status, 1808 women for physical activity, 6503 women for hyperlipidaemia status and 841 women for diabetes status. Only data on participants who had complete covariate information were used in the model (n 13 132).
Table 3 Later:earlier energy intake ratio across sociodemographic, lifestyle and health variables for men in the European Prospective Investigation into Cancer and Nutrition (EPIC) calibration study*

*Type III tests of the generalized linear model procedure were used to evaluate associations between a priori selected variables and the ratio, given all covariates in the model. The ratio was log-transformed before entered into the model to correct for positive skewness. In total, the following number of men were missing covariate information: 133 men for educational status, 3929 men for marital status, 142 men for smoking status, 1354 men for physical activity, 3860 men for hyperlipidaemia status and 392 men for diabetes status. Only data on participants who had complete covariate information were used in the model (n 5680).
Among women, the following variables were associated with the ratio: country (P<0·001), age (P<0·001), education (P<0·001), marital status (P=0·021), smoking (P<0·001), day of recall (P<0·001) and season (P=0·024; Table 2). Importantly, female later energy consumers (i.e. ratio >1·0) tended to be from Central/Northern Europe, younger, have higher educational level, be current smokers, and to have captured a weekend day (i.e. Saturday–Sunday) and the summer season during the recall interview. For men, statistically significant associations with the ratio were found for: country (P<0·001), age (P<0·001), education (P<0·001), smoking (P<0·001), physical activity (P=0·020), BMI (P<0·001) and day of recall (P<0·001; Table 3). Hence, importantly, male later energy consumers were more likely to be from Central/Northern Europe, younger, to have higher educational level, be current smokers, physically inactive and to have captured a weekend day during the recall interview. However, the models explained only 12·9 and 8·3 % of the variation in the ratio among women and men, respectively.
Discussion
We set out to examine meal timetables and timing of eating across ten European countries. We found pronounced geographical differences across the countries, with later timing of meals and snacks but higher energy load earlier during the day in Mediterranean countries compared with Central/Northern European countries. Furthermore, among both women and men, we found that higher later compared with earlier energy load was associated with Central/Northern European countries, weekend days, and being younger, more educated and current smoker.
These results add to our previous report where we demonstrated that lunch provides 38–45 % of daily energy intake in Mediterranean countries and 16–27 % in Central/Northern European countries( Reference Huseinovic, Winkvist and Slimani 18 ). In the current paper, we found that main meals are consumed later in most Mediterranean countries than in Central/Northern Europe (e.g. 09.00, 14.00 and 21.00 hours in Spain compared with 07.00, 12.00 and 16.00 hours in Norway, respectively). Still, within the Mediterranean countries, breakfast and lunch are consumed earlier in France than in Spain, Italy and Greece. This is in line with previous research demonstrating main meals to be consumed at 07.00, 12.00 and 20.00 hours in France( Reference Park, Freisling and Huseinovic 30 ), compared with 09.00, 15.00 and 22.30 hours in Spain( Reference Garaulet, Gomez-Abellan and Alburquerque-Bejar 31 ). Furthermore, meal pattern analyses within the European Food Consumption Validation (EFCOVAL) study, conducted during 2007–2008, confirm our findings of more distinct peak times of eating in Mediterranean countries (represented by France in the EFCOVAL study) than in Central/Northern European countries (represented by the Netherlands, Norway, Belgium and the Czech Republic), where eating times were more spread throughout the day( Reference Park, Freisling and Huseinovic 30 ). This finding is also in agreement with our previous report, where we found daily energy intake provided by snacks to be 10–20 % v. 23–35 % in the two regions, respectively, and the mean intake frequency to range from 4·9–5·0 (Greece and Italy) to 6·8–7·0 (the Netherlands) FCO per day( Reference Huseinovic, Winkvist and Slimani 18 ), indicating more eating occasions between the main meals in Central/Northern European than in Mediterranean countries.
Eating behaviour is a complex process influenced by social, cultural, biological and personal factors( Reference De Castro 32 , Reference Chiva 33 ). Historically, social constraints have determined the daily number of eating occasions and culture has dictated when eating is, or is not, appropriate( Reference Bellisle 17 ). In the present study, we found a near doubling of the later:earlier energy intake ratio from lowest to highest between the EPIC countries. This suggests that cultural habits within a country are stronger predictors of temporal eating than any of our measured individual-level characteristics. Likewise, in the EFCOVAL study, country was found to be independently associated with all examined meal pattern aspects and to contribute the most to the variability in meal patterns( Reference Park, Freisling and Huseinovic 30 ). Still, in the EPIC data, considerable variation in the ratio was observed across centres within the same country, e.g. in Spain. This indicates both between- and within-country variation in timing of eating. Nevertheless, for the two UK centres, General population and Health-conscious, similar results were found for both timing of eating and the later:earlier energy intake ratio, although dinner was consumed somewhat later in the UK Health-conscious population. Furthermore, meal patterns have been reported to have seasonal and weekly variations, and to be influenced by age. For example, meals have been found to be shifted to the later part of the day on weekends compared with weekdays( Reference McCarthy 34 , Reference McHill, Phillips and Czeisler 35 ), and the elderly have been reported to eat earlier in the day than younger individuals( Reference de Castro 36 ). In addition, Leech et al. recently reported that individuals with a ‘grazing’ meal pattern, characterized by later and less distinct peak times of eating, were younger, had higher education (women) and were less likely to be married (men), compared with individuals with a ‘conventional’ or ‘later lunch’ pattern( Reference Leech, Worsley and Timperio 37 ). This is in agreement with our findings demonstrating a higher later:earlier energy intake ratio on weekends and among younger and higher educated individuals. Finally, and interestingly, we found that countries with later meal timetables (e.g. Mediterranean countries) had lower later:earlier energy intake ratio compared with countries with earlier meal timetables. This indicates that later timing of meals and snacks does not necessarily translate into greater energy load later during the day. However, the suggested misalignment between timing of eating and endogenous circadian systems( Reference Marinac, Sears and Natarajan 6 , Reference Morris, Purvis and Mistretta 7 ) may still apply, irrespective of temporal energy load. Future studies should evaluate how timing of eating, energy load across the day and irregularity in temporal distribution of eating affect metabolic circadian rhythm and diet-related disease risk.
We could not distinguish a clear and/or strong association between timing of eating and BMI, hyperlipidaemia or diabetes. Although eating behaviours are highly interrelated, consuming a greater proportion of daily energy intake at dinner and breakfast skipping have both been independently associated with obesity and the metabolic syndrome, also after adjusting for total energy intake( Reference Bo, Musso and Beccuti 13 ). For example, Aljuraiban et al. found that individuals who ate more frequently and consumed most of their energy intake earlier in the day (evening:morning energy intake ratio of ≤1·8) had lower energy density and total energy intake, and higher nutrient quality, compared with participants with lower eating frequency and who consumed most of their energy intake later in the day (ratio of >1·8). In addition, they found a positive association between BMI and evening:morning energy intake ratio also after adjusting for total energy intake( Reference Aljuraiban, Chan and Oude Griep 12 ). Furthermore, in a 12-week weight-loss trial among ninety women with metabolic syndrome, a high-energy breakfast was found to reduce weight, fasting glucose, insulin and TAG, and to increase satiety scores, more than a high-energy dinner under isoenergetic conditions( Reference Jakubowicz, Barnea and Wainstein 38 ). Also, others have shown that later Spanish lunch eaters (after 15.00 hours), compared with earlier lunch eaters, lose less weight and have slower weight-loss trajectory( Reference Garaulet, Gomez-Abellan and Alburquerque-Bejar 31 ), and that eating a later lunch or snack is associated with impaired metabolism and decreased resting energy expenditure and diet-induced thermogenesis( Reference Bandin, Scheer and Luque 39 , Reference Romon, Edme and Boulenguez 40 ). Thus, this suggests that a high energy intake earlier in the day may influence health more favourably than corresponding energy consumed later during the day. Even though high evening intake might reflect other lifestyle habits and/or food choices compared with high morning intake, a growing body of evidence indicates that circadian timing of eating affects body weight irrespective of total energy intake and may be a modifiable risk factor for diet-induced chronic disease.
The strengths of the present study include a large and diverse population sampled across several European countries concurrent with standardized and homogeneous dietary assessment methodology, which enabled an objective comparison of timing of eating across a broad geographical span. As for the limitations, the data herein were collected during 1995–2000 and are not nationally representative samples of the European general populations. However, the results may still demonstrate significant geographical differences between the countries due to the harmonized methodology used. In addition, our findings are confirmed by more recent analyses of meal patterns in adult European populations( Reference Park, Freisling and Huseinovic 30 , Reference Garaulet, Gomez-Abellan and Alburquerque-Bejar 31 ). Second, the results are restricted to the methodology and definitions used through the earlier–later dichotomy approach, with earlier intakes defined as 06.00–14.00 hours. This cut-off was chosen as it encompasses the time of lunch for most countries and has been used previously to define earlier energy consumers( Reference Kaczmarek, Musaad and Holscher 29 ). Nevertheless, for some Mediterranean countries such as Spain, the cut-off was drawn during lunch hours, resulting in a higher ratio than if a later cut-off had been used. Still, the biological and metabolic implications of consuming a large proportion of daily energy intake later in the day should be the same irrespective of whether the energy load is labelled later lunch or earlier dinner. Third, participants missing complete covariate information were excluded. Fourth, the large sample size might have increased the number of statistically significant findings and the models explained only a small proportion of the variance in the ratio. Fifth, due to the use of single 24 h diet recalls and the cross-sectional design, we can only draw conclusions at the group level and interpret the results as hypothesis-generating that need to be evaluated in longitudinal and experimental settings. Finally, future research should examine what, and how, specific dietary factors relate to timing of eating, and could consider using data-driven approaches( Reference Leech, Worsley and Timperio 37 ) to examine patterns in timing of eating across meals and snacks.
Conclusion
We found pronounced differences in timing of eating across Europe, with later meal timetables and greater energy load earlier during the day in Mediterranean countries compared with Central and Northern European countries. More research is needed within the emerging field of chrono-nutrition to improve our understanding of the health implications of timing and patterning of eating throughout the day.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980018002288
Acknowledgements
Financial support: This study was carried out with the financial support of the European Commission: Public Health and Consumer Protection Directorate 1993–2004; Research Directorate-General 2005, Ligue contre le Cancer (France); Société 3M (France); Mutuelle Générale de l’Education Nationale; Institut National de la Santé et de la Recherche Médicale (INSERM); Institute Gustave Roussy; German Cancer Aid; German Cancer Research Center; German Federal Ministry of Education and Research; Danish Cancer Society; Health Research Fund (FIS) of the Spanish Ministry of Health; Spanish Regional Governments of Andalucía, Asturias, Basque Country, Murcia (no. 6236) and Navarra and the Catalan Institute of Oncology; and ISCIII RETIC (RD06/0020), Spain; Cancer Research UK; Medical Research Council, UK; the Stroke Association, UK; British Heart Foundation; Department of Health, UK; Food Standards Agency, UK; the Wellcome Trust, UK; Greek Ministry of Health; Hellenic Health Foundation; Italian Association for Research on Cancer; Italian National Research Council, Regione Sicilia (Sicilian government); Associazione Italiana per la Ricerca sul Cancro-AIRC-Italy – ONLUS (Hyblean association for epidemiological research, NPO); Dutch Ministry of Health, Welfare and Sport; Dutch Prevention Funds; LK Research Funds; Dutch ZON (Zorg Onderzoek Nederland); World Cancer Research Fund (WCRF); Swedish Cancer Society; Swedish Research Council; Regional Government of Skane and the County Council of Vasterbotten, Sweden. The funders had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: A.W. and H.B.F. initiated the study. E.H., A.W. and H.B.F. formulated the research questions, performed the analysis and wrote the manuscript taking into account comments from all co-authors. H.F., N.S, H.B., G.B., L.S. and E.W. contributed to the conception, analysis and interpretation of the data and drafting of the manuscript. All other co-authors were local EPIC collaborators involved in the collection of dietary data and other data. All authors read and approved the final version. Ethics of human subject participation: The EPIC project was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects was approved by the ethical review boards of the International Agency for Research on Cancer (Lyon, France) and from all local centres. Written informed consent was obtained from all subjects.







