


Consumption of sugar-sweetened beverages (SSB) has increased both in the UK and internationally in recent decades( Reference Ng, Ni Mhurchu and Jebb 1 – Reference Bleich, Wang and Wang 3 ). SSB are a major source of added sugars and their frequent consumption has been linked to weight gain and obesity( Reference Malik, Popkin and Bray 4 – Reference Malik, Schulze and Hu 6 ) and risks of diabetes mellitus( Reference Malik, Popkin and Bray 4 , 7 – Reference Imamura, O’Connor and Ye 9 ), dental caries( Reference Bernabe, Vehkalahti and Sheiham 10 , Reference Park, Lin and Onufrak 11 ) and other health problems( Reference de Koning, Malik and Kellogg 12 – Reference Choi and Curhan 16 ). Globally, SSB have been identified as a single, modifiable component of diet that can impact on preventable death and disability in adults( Reference Singh, Micha and Khatibzadeh 17 ). The importance of reducing sugar intake from SSB has been highlighted in national and international public health guidance( 18 – 20 ). Preventive actions have been initiated at a population level in the UK to begin to address the challenge, including awareness campaigns, food labelling recommendations and a commitment by government to introduce an SSB industry levy as a fiscal measure.
The consumption of artificially sweetened beverages (ASB) has also increased in recent years in the UK and elsewhere( Reference Ng, Ni Mhurchu and Jebb 1 , Reference Fakhouri, Kit and Ogden 21 , Reference Duffey and Popkin 22 ). Although ASB are unlikely to offer any nutritional benefit they are promoted as a substitute for SSB for weight control( Reference Tate, Turner-McGrievy and Lyons 23 ). ASB are considered a less harmful alternative to SSB, although little is known about the long-term consequences of habitual ASB consumption.
There is a need to identify social and behavioural determinants of SSB and ASB consumption. Understanding consumers’ characteristics can help identify the groups most likely to benefit from public health interventions. Much of the existing research on social and behavioural correlates with sweetened beverage consumption has been conducted in North America and has focused on consumption of SSB only, particularly among children and adolescents( Reference Kit, Fakhouri and Park 24 – Reference Danyliw, Vatanparast and Nikpartow 27 ). Less is known about social and behavioural factors underlying sweetened beverage consumption in adults in European settings, particularly ASB consumption. To fill this knowledge gap, we aimed to identify the sociodemographic and behavioural factors associated with consumption of SSB and ASB in adults in a population-based cohort in the UK.
Methods
Study design
We conducted cross-sectional analyses in the Fenland Study, a population-based prospective cohort of adults born between 1950 and 1975 in Cambridgeshire, UK. The study was initiated to investigate the influence of lifestyle and genetic factors on the development of cardiometabolic disorders (http://www.mrc-epid.cam.ac.uk/research/studies/fenland/)( Reference Burgoine, Forouhi and Griffin 28 ). Briefly, baseline recruitment and assessment were conducted over 2005–2013 for 10 452 adults, after contacting residents listed with a participating general practice surgery in the Cambridge, Ely and Wisbech areas (27 % response rate). As UK adults are registered with a general practitioner, these registers formed a population-based sampling frame. Adults were not invited if they had a known diagnosis of diabetes since the purpose of the cohort was to examine the risk of cardiometabolic disorders. The other exclusion criteria included: terminal illness with a prognosis of less than 1 year, psychotic illness, or being pregnant, lactating or unable to walk unaided. Participants gave written informed consent.
The current study sample included data on 9991 participants aged 30–64 years. Participants were excluded for the following reasons: missing data on consumption of SSB or ASB (n 355), missing data related to nutrient intake (n 6) or implausible data related to nutrient intake based on responses to an FFQ (n 100). Implausible responses were defined by <0·5th percentile or ≥99·5th percentile of a ratio of total energy intake to BMR( Reference Welch, Luben and Khaw 29 ).
Assessment of dietary intake
Data on consumption of SSB and ASB were collected at baseline visit using a previously validated FFQ( Reference Bingham, Welch and McTaggart 30 ). For each of 130 food/beverage items, participants were asked to report frequency of consumption over the previous year by selecting one of nine categories: never or less than once/month, 1–3/month, once/week, 2–4/week, 5–6/week, once/d, 2–3/d, 4–5/d and ≥6/d. SSB consumption was based on the sum of frequency of consuming two items: ‘fizzy soft drinks (e.g. Coca cola, lemonade)’ and ‘fruit squash or cordial’. ASB consumption was based on responses to one item: ‘low calorie or diet fizzy soft drinks’.
Diet quality, a potential determinant of SSB or ASB consumption, was assessed by a score representing the degree of adherence to the Mediterranean diet (possible range 0 to 18). The score was created using responses to the FFQ and cut-offs described by Sofi et al.( Reference Sofi, Macchi and Abbate 31 ). A higher score was assigned if participants reported higher consumption of fruits, vegetables, cereals, legumes and fish, and lower consumption of dairy products, meat and meat products, moderate consumption of alcohol, and more regular use of olive oil( Reference Sofi, Macchi and Abbate 31 ).
Assessment of lifestyle and eating behaviours
The Fenland Study General Questionnaire was used to assess smoking status (current, former, never) and the frequency of the following seven eating behaviours: eating breakfast, home-delivery/takeaway meals, ready-made meals, home-cooked meals, meals outside the home, meals while watching television and snack foods while watching television. Different frequency categories were used for each of the eating behaviours. Information was also collected on daily intake of alcoholic beverages. Data relating to intake of beer, cider, wine, spirits (e.g. whisky, vodka) and other alcoholic beverages (e.g. port, sherry) were collected using the FFQ, and responses were summed to calculate total daily servings of alcoholic beverages.
Assessment of sociodemographic factors
Demographic variables (age, sex) and socio-economic variables were collected by questionnaire. Seventeen categories of ethnic origin were assessed and collapsed into two groups: white (97·6 %) and non-white ethnicity. Education level, income and other social factors were evaluated as indicators of socio-economic conditions which relate to dietary habits, including daily consumption of SSB or ASB. These included age finishing education, current work status (full-time, part-time, keeping house, not currently working), employment type (employee, self-employed), total combined annual household income (<£20 000, £20 000–£40 000, >£40 000), marital status (single, married, separated/widowed/divorced), number of people in household, car ownership (yes, no) and home ownership (yes, no). Eight occupation types were collapsed to lower, middle or higher socio-economic class in concordance with the National Statistics Socio-Economic Classification (NSSEC)( 32 ). Individuals with occupations in NSSEC I/II were considered to be in the higher socio-economic class; in NSSEC III/IV, the middle socio-economic class; and in NSSEC V/VI/VII, the lower socio-economic class.
Anthropometry and physical activity
Body weight and height were measured objectively by trained research staff and used to compute BMI as weight/height2 (kg/m2). Physical activity was objectively measured for 6 d with a combined heart-rate and acceleration sensor (Actiheart; CamNTech, Cambridge, UK). A treadmill test was used for individual calibration of these data to model energy expenditure due to physical activity, expressed as metabolic equivalents of task (MET) and summarised as average hours per day spent in sedentary or resting time (<1·5 MET), light physical activity (≥1·5 and <3·0 MET) or moderate/vigorous physical activity (≥3·0 MET)( Reference Brage, Westgate and Franks 33 ).
Statistical analysis
All analyses were undertaken using the statistical software package Stata version 13.1 (α two-sided=0·05). For each of SSB and ASB, participants were classified to daily consumers (≥1 drink/d) and non-daily consumers (<1 drink/d, including non-consumers) based on their responses to frequency of consumption. The association between sociodemographic factors and lifestyle/behavioural factors and daily or non-daily consumption of each of SSB and ASB was evaluated using logistic regression, in line with previous approaches( Reference Mullie, Aerenhouts and Clarys 34 – Reference Rehm, Matte and Van Wye 36 ). OR and 95 % CI were estimated by exponentiating regression coefficients, followed by calculating P values based on Wald tests.
Multivariable-adjusted logistic regression models were built sequentially. All models included age, sex and test site (Cambridge, Ely or Wisbech). In analysis of sociodemographic factors as independent variables, the model included other sociodemographic factors simultaneously for mutual adjustment. Individual behaviour factors were not adjusted for in these models, as they may be intermediate factors in the associations between sociodemographic factors and sweetened beverage consumption. For example, watching television may mediate the association between socio-economic status and SSB consumption. In analysis of lifestyle factors and eating behaviours as independent variables, sociodemographic variables were included in the logistic regression models as potential confounders. The seven eating behaviours and BMI were evaluated categorically and also continuously in logistic regression models to examine a linear relationship of each of the variables with the odds of daily SSB and ASB consumption.
To account for correlations between SSB and ASB consumption, logistic regression models were additionally evaluated after including both variables together in the same model (one as the outcome and the other as a covariate). We adjusted for calendar year and date of baseline visit, and medication use for hypertension or dyslipidaemia, to assess their influence on results because calendar time and co-morbid status may have influenced errors in responses to questionnaires and distorted true associations of interest. Total energy intake reflects consumption of foods and beverages overall, and was thus adjusted for in the most adjusted model to obtain results independent of the total amount of foods consumed. To account for missing information on independent variables we created dummy variables indicating missing information and included the indicator variables in all logistic regression models. The χ 2 test was used to examine whether the presence of missing data was associated with daily consumption of sweetened beverages.
As sensitivity analysis, we repeated analyses by classifying consumers as those consuming SSB and ASB ≥3 servings/d, respectively; and by defining only fizzy drinks as SSB, because fruit squash/cordial may be consumed after being diluted to contain low sugars. We also repeated analysis by evaluating consumers of both SSB and ASB (≥1 serving/d for both beverage types) to characterise adults who did not consider how soft drinks were sweetened.
Results
Of 9991 participants, 54·0 % were women. The mean age was 47·8 (sd 7·4) years. The prevalence of obesity (BMI ≥30 kg/m2) was 21·1 %; of overweight (BMI=25·0–29·9 kg/m2), 39·7 %; of current smoking, 12·9 %; and of former smokers, 32·3 %. SSB and ASB consumption was skewed to the right (see online supplementary material, Supplementary Fig. 1). Daily consumption of SSB and ASB was reported by 20·4 and 8·9 % of participants, respectively. Among daily consumers, mean SSB consumption and mean ASB consumption were 2·2 (sd 1·4) servings/d and 2·0 (sd 1·3) servings/d, respectively.
In unadjusted analysis (Tables 1 and 2), daily SSB consumption was positively associated with being male, whereas daily ASB consumption was positively associated with being female (P<0·001). SSB and ASB consumption was each similarly associated with younger age, white ethnicity and all eating behaviours (P<0·001 each), apart from eating outside the home (P > 0·1). Mean BMI was higher among daily SSB consumers than SSB non-consumers (27·6 (sd 5·0) v. 26·6 (sd 4·7) kg/m2, respectively) and among daily ASB consumers than ASB non-consumers (29·5 (sd 5·6) v. 26·6 (sd 4·6) kg/m2).
Table 1 Sociodemographic characteristics, stratified by daily consumption of sugar-sweetened beverages (SSB) and artificially sweetened beverages (ASB), of adults (n 9991) aged 30–64 years in the Fenland Study, Cambridgeshire, UK, 2005–2013

* Values are percentage of each characteristic among daily consumers or non-daily consumers, except age (years). P values were computed by logistic regression analysis in which daily consumption (yes or no) was an outcome and each characteristic was a predictor.
† Missing information among <5 % of adults is not presented.
‡ Marital status was not assessed among 28·0 % of the study population because a questionnaire for those participants did not include the question about marital status, but was revised to include the question for the rest of the participants.
Table 2 Lifestyle/behavioural characteristics, stratified by daily consumption of sugar-sweetened beverages (SSB) and artificially sweetened beverages (ASB), of adults (n 9991) aged 30–64 years in the Fenland Study, Cambridgeshire, UK, 2005–2013
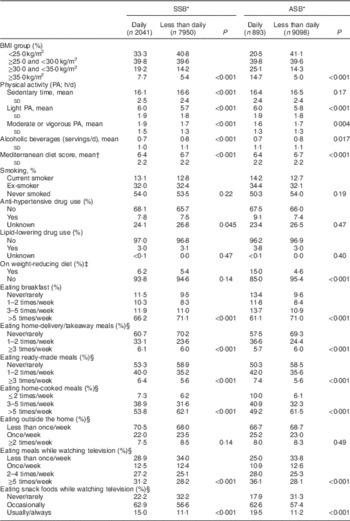
* Values are mean and sd for continuous variables and proportions for categorical variables. P values were computed by crude logistic regression analysis relating daily consumption of SSB or ASB (yes or no) to each characteristic.
† Mediterranean diet score was an 18-point scale representing adherence to the Mediterranean diet, used as a marker of diet quality.
‡ Participants were considered to be on a weight-reducing diet if they responded that they were on any of the following diets: ‘Weight Watchers’, ‘Slimming World’, low-fat diet, low-carbohydrate diet (e.g. ‘Atkins diet’).
§ Missing information among <5 % of adults is not presented.
In multivariable-adjusted analysis (Table 3), daily SSB consumers were significantly more likely to be men, of lower socio-economic class and have a younger age of finishing education. They were less likely to own their home and more likely to have lower household income and live in a larger household. Daily consumption of ASB showed significant associations with age of finishing full-time education, but not with socio-economic class and home ownership. Longer duration of education was associated with lesser SSB and ASB consumption (OR=0·52 and 0·43, respectively, in comparison between extreme categories). Significant trends in an opposing direction for SSB and ASB were observed for sex and household income. Comparing men with women, OR for daily consumption of ASB was 0·66 (95 % CI 0·56, 0·79); and of SSB, 1·33 (95 % CI 1·17, 1·50). Comparing those with higher income with those with lower income, OR for daily consumption of SSB and of ASB were 0·76 (95 % CI 0·63, 0·91) and 1·53 (95 % CI 1·16, 2·00), respectively.
Table 3 Associations of sociodemographic characteristics with daily consumption of sugar-sweetened beverages (SSB) and artificially sweetened beverages among adults (n 9991) aged 30–64 years in the Fenland Study, Cambridgeshire, UK, 2005–2013
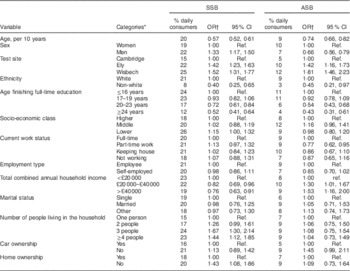
Ref., reference category.
* A category listed at the top of each variable was used as a reference in logistic regression models for daily v. non-daily consumers of SSB and ASB. A category for missing information was included in each model, but not presented. Adjustment for missing data had little influence on the results.
† Adjusted for age, sex, site (Cambridge, Ely, Wisbech) and all sociodemographic variables shown at the first column.
Results for lifestyle characteristics are presented in Table 4. Obese or overweight adults were more likely to consume SSB and ASB than normal-weight adults. Current smoking was associated with lesser likelihood of consuming SSB daily, with OR=0·79 (95 % CI 0·66, 0·93), compared with non-smokers. Those on a weight-loss diet were more likely to consume ASB daily, with OR=2·58 (95 % CI 2·05, 3·24), compared with those not on a weight-loss diet. Among eating behaviours (Figs 1 and 2), skipping breakfast and having meals or snacks while watching television were associated with daily consumption of SSB or ASB (P<0·02).
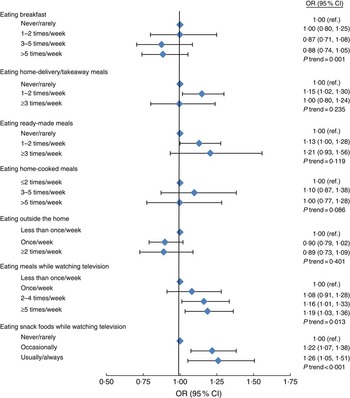
Fig. 1 Associations of dietary habits with daily consumption of sugar-sweetened beverages among adults (n 9991) aged 30–64 years in the Fenland Study, Cambridgeshire, UK, 2005–2013. OR (![]() ) and 95 % CI (represented by horizontal bars) were adjusted for demographic and socio-economic factors and mutually adjusted for different dietary habits presented here (ref., reference category)
) and 95 % CI (represented by horizontal bars) were adjusted for demographic and socio-economic factors and mutually adjusted for different dietary habits presented here (ref., reference category)

Fig. 2 Associations of dietary habits with daily consumption of artificially sweetened beverages among adults (n 9991) aged 30–64 years in the Fenland Study, Cambridgeshire, UK, 2005–2013. OR (![]() ) and 95 % CI (represented by horizontal bars) were adjusted for demographic and socio-economic factors and mutually adjusted for different dietary habits presented here (ref., reference category)
) and 95 % CI (represented by horizontal bars) were adjusted for demographic and socio-economic factors and mutually adjusted for different dietary habits presented here (ref., reference category)
Table 4 Associations of lifestyle characteristics with daily consumption of sugar-sweetened beverages (SSB) and artificially sweetened beverages (ASB) among adults (n 9991) aged 30–64 years in the Fenland Study, Cambridgeshire, UK, 2005–2013

PA, physical activity; Ref., reference category.
* For categorical variables, levels are shown. For continuous variables, scale for interpretation of OR is shown.
† Adjusted for age, sex, test site, and sociodemographic and lifestyle/behavioural variables together. See Tables 1 and 2 for the variables. The associations of eating behaviours are shown in Figs 1 and 2.
‡ Intensity of PA was modelled isotemporarily; with time estimates denoting substitution from light PA into either sedentary or moderate/vigorous PA.
§ Mediterranean diet score was an 18-point scale representing adherence to the Mediterranean diet, used as a marker of diet quality.
║ P values for trend are presented, for which an ordinal variable was included as a continuous term in a logistic regression model.
After adjustment for sociodemographic factors, ASB consumption and SSB consumption were modestly correlated (r=0·13). In additional analyses including SSB or ASB consumption as a covariate, results changed little. Results were not altered materially after adjustment for total energy intake, calendar year or date of baseline visit, or medications for hypertension or dyslipidaemia.
Having missing information (i.e. at least one exposure variable missing) was not significantly associated with daily consumption of SSB (χ 2=0·02; P=0·88) or ASB (χ 2=3·32; P=0·07). Not adjusting for the missing variable indicator had little influence on the main results. Evaluating ≥3 servings/d as a cut-point for SSB and ASB consumption or excluding fruit squash/cordial from SSB definition, estimates became imprecise, but were generally similar to those in the primary analysis (see online supplementary material, Supplemental Tables 1 and 2). As exceptions, by contrast to the primary findings, ≥3 servings ASB/d was significantly associated with former smoking history, lower alcohol drinking and lower diet quality (Mediterranean diet score; P<0·05). Evaluating ≥1 servings/d of both SSB and ASB as an outcome (n 307, 3·1 %), one-third of daily consumers of ASB (n 893) reported daily SSB consumption, while approximately 15 % of SSB consumers reported daily ASB consumption, and trends of associations were generally similar to the findings for ASB with wide confidence intervals (Supplemental Tables 1 and 2).
Discussion
In the current study of 9991 adults in Cambridgeshire, UK, one in five adults reported daily consumption of SSB and one in ten adults reported daily consumption of ASB. Although daily consumers of SSB and ASB shared many sociodemographic characteristics, a key difference between groups was the finding that having a lower household income was associated with higher SSB consumption, but with lower ASB consumption. In addition to sociodemographic factors such as age and education, modifiable factors were significantly associated with higher consumption of both SSB and ASB, including being overweight or obese, eating meals or snack foods while watching television, and skipping breakfast.
Sugar-sweetened beverage consumption
Some of our findings relating to SSB consumption were consistent with existing studies which reported positive associations with younger age, male sex, a lower level of education and a lower household income( Reference Bleich, Wang and Wang 3 , Reference Mullie, Aerenhouts and Clarys 34 , Reference Park, Pan and Sherry 35 , Reference Nikpartow, Danyliw and Whiting 37 – Reference Paulsen, Myhre and Andersen 40 ). Our study was consistent with previous studies that reported positive associations of frequent SSB consumption with higher BMI( Reference Malik, Popkin and Bray 4 – Reference Malik, Schulze and Hu 6 , Reference Malik, Pan and Willett 41 ), less frequent alcohol consumption( Reference Park, Pan and Sherry 35 ), and eating meals or snack foods in front of the television( Reference Park, Blanck and Sherry 26 , Reference Rehm, Matte and Van Wye 36 , Reference Grontved and Hu 42 , Reference Vereecken, Todd and Roberts 43 ). Habitual SSB consumption exerts adverse health effects and its association with lower household income may therefore worsen health outcomes for disadvantaged groups.
Some of the current findings were not consistent with the existing literature, which might reflect differences in population and methodology. We did not observe a significant association of SSB consumption with socio-economic classes after adjustment for other demographic variables, whereas other European studies reported higher SSB consumption among those of lower socio-economic groups( Reference McCartney, Younger and Walsh 44 – Reference Laitinen, Rasanen and Viikari 46 ). This could be partly explained by the differences in the definitions of socio-economic class that were used across studies( Reference Hulshof, Brussaard and Kruizinga 45 , Reference Laitinen, Rasanen and Viikari 46 ), or it may be because the current study controlled for more covariates. We identified home ownership and the number of household members as significant determinants of SSB consumption in our study, independent of socio-economic class. Home ownership may act as a proxy for relative affluence and has not been explored as an independent covariate in similar studies. The positive association with household size suggests that adults living with children may be more frequent consumers of SSB. Since children consume more SSB than any other age group in the UK( 47 ), parents living with children may purchase and consume more SSB than those who are not living with children, as supported by a UK national survey( 39 ) and previous American studies( Reference Berge, Larson and Bauer 48 , Reference Sharkey, Johnson and Dean 49 ). This finding highlights the potential benefit of considering family-based interventions to reduce SSB consumption.
Previous evidence suggests that SSB consumers tend to have generally unhealthy lifestyles( Reference Park, Pan and Sherry 35 , Reference Nikpartow, Danyliw and Whiting 37 , Reference Duffey, Gordon-Larsen and Steffen 50 , Reference Park, Sherry and Foti 51 ). This was not observed in our study, where daily SSB consumption was associated with greater physical activity and lesser alcohol consumption. The finding for physical activity might reflect that physically active adults consume more sports/energy drinks, which are SSB. The lower consumption of alcoholic beverages may be due to a substitution effect. This might be influenced by the type of alcoholic beverages consumed, as some people who consume spirits may also consume SSB as mixers. Further research on the details of such substitution effects will be valuable.
Our finding of an inverse association between current smoking and daily SSB consumption also contrasts with previous studies( Reference Mullie, Aerenhouts and Clarys 34 , Reference Park, Pan and Sherry 35 , Reference Park, Sherry and Foti 51 – Reference Kvaavik, Andersen and Klepp 53 ). Our study supports that smokers have less appetite to consume caloric beverages and foods( Reference Hughes 54 ) and may avoid consuming SSB and other perceived unhealthy products to ‘compensate’ for their smoking. Although such mechanisms are not proven, our findings indicate the need for population-specific monitoring and intervention to reduce SSB consumption among adults, particularly when they are trying to make other lifestyle changes such as quitting smoking or starting an exercise programme.
Eating meals or snacking while watching television was each related to SSB consumption, while eating takeaway meals or eating outside the home was not significantly related, inconsistent with previous studies( Reference Park, Blanck and Sherry 26 , Reference Ayala, Rogers and Arredondo 55 – Reference Myhre, Loken and Wandel 58 ). As discussed above, the inconsistency may reflect differences in available variables for statistical adjustment and population demographics. Additional research is warranted in different populations, evaluating socio-economic and behavioural variables that were previously understudied, but identified in our study to be important as potential determinants of SSB consumption.
Artificially sweetened beverage consumption
There have been fewer studies on determinants of ASB consumption than SSB consumption, but despite limited literature, our study and previous work consistently found that ASB consumption was higher among women and younger adults( Reference Fakhouri, Kit and Ogden 21 , Reference Mullie, Aerenhouts and Clarys 34 , Reference Storey, Forshee and Anderson 38 – Reference Paulsen, Myhre and Andersen 40 , Reference Duffey and Popkin 59 ), those of white ethnicity and higher household income( Reference Fakhouri, Kit and Ogden 21 , Reference Bleich, Wolfson and Vine 60 ), and was more common among adults with higher BMI and those on weight-loss diets( Reference Bleich, Wang and Wang 3 , Reference Mullie, Aerenhouts and Clarys 34 , Reference Bleich, Wolfson and Vine 60 ).
Lower educational attainment (younger age of finishing education) was associated with higher ASB consumption in the present study, similar to SSB consumption. This finding was opposite to two previous studies in Belgium and the UK( Reference Mullie, Aerenhouts and Clarys 34 , 39 ), possibly reflecting the difference in education attainment between the study populations. Whereas our study population had longer duration of education than the national average( Reference Kay, Jacobs and Katan 61 ), the prior UK study, the Low Income Diet and Nutrition Survey (LIDNS), examined the nation’s most socially deprived households( 39 ) and the Belgian study recruited men who were less educated than the Belgian average( 62 ). We found no significant association of ASB consumption with household size. This was inconsistent with the finding from the LIDNS of high ASB consumption in households without children( 39 ). These observations indicate heterogeneity in determinants of beverage consumption across sociodemographic characteristics and indicate the challenges in designing potential interventions which account for this heterogeneity.
ASB consumption was strongly associated with overweight or obesity, skipping breakfast and being on a weight-loss diet, but not associated with physical activity levels, consistent with findings previously reported in non-UK settings( Reference Mullie, Aerenhouts and Clarys 34 , Reference Bleich, Wolfson and Vine 60 ). Consumption of ≥3 servings ASB/d was associated with former smoking and lower diet quality; and one-third of ASB consumers reported daily SSB consumption. This suggests that individuals may habitually consume ASB for weight management or general health after quitting smoking, but without regard for improvement in diet quality and physical activity levels. While confirmation of this finding in a general population is needed, this has potential implications for dietary or weight-loss programmes which aim to improve health outcomes through delivery of information and health promotion interventions.
Eating behaviours such as consuming meals or snacks while watching television were related to ASB consumption, in line with a previous US-based study which reported that persons who purchased the most ASB also purchased the largest amount of snack foods( Reference Binkley and Golub 63 ). Another American study reported that about 20 % of total energy intake among ASB consumers was from snack foods( Reference Bleich, Wolfson and Vine 60 ). This supports that, independent of any direct health effects, ASB consumers may need to be recognised as those with clustering of potentially unhealthy dietary behaviours.
Strengths and limitations
The large size of the current study provided adequate precision in our estimates. The study included a larger number of potential confounders than previous similar studies( Reference Mullie, Aerenhouts and Clarys 34 – Reference Rehm, Matte and Van Wye 36 ). This allowed a more thorough statistical adjustment and provided detailed insight into the characteristics of SSB and ASB consumers, including important behavioural factors in addition to sociodemographic factors. No previous literature was identified for some of the associations in the present study, particularly relating to ASB consumption. For these and other characteristics, the study helps to fill a gap in the existing evidence.
There are a number of limitations to our study. As it was cross-sectional, causality is limited in our findings of associations. Therefore, we cannot rule out that current social factors (e.g. income), for example, were driven by habitual, long-term dietary habit with high SSB consumption and obesity. Moreover, appreciable changes in the pattern of sweetened beverage consumption over time may not have been discerned. Although statistical adjustment might partly reduce measurement errors of dietary exposure, there might be errors in measurements of beverage consumption due to participants’ interpretation of a serving size and habitual consumption, including possible underestimation. Participants may not have thought to report their consumption of some sweetened beverages (e.g. sports drinks) as the FFQ might have prompted respondents to mostly consider carbonated soft drinks and fruit cordials. Pure fruit juices were not included in the study and it is possible that respondents misclassified some SSB as fruit juice. We could not rule out bias due to missing data, but the use of modelled indicator variables did not suggest discernible differences in characteristics. Seasonality of beverage consumption, as well as of lifestyle and dietary behaviours, was not interrogated in the study. Although the FFQ was intended to reflect average habitual dietary consumption over a year, the accuracy of responses is limited by participants’ memory and may be influenced by recall of recent beverage intake, which may in turn be affected by recent weather. This may have led to additional variability in measurements. The differences in SSB consumption across sites in the study may reflect unmeasured societal factors, including area-level characteristics. Wisbech has a higher area-specific Index of Multiple Deprivation score compared with Ely and Cambridge( 64 ). All sociodemographic variables evaluated in the present study were at the individual level and this may have led to residual confounding in our findings.
Generalisability may be limited as the participation rate was low (27 %). The study population did not include people younger than 30 years old where the consumption of sweetened beverages is higher, people with diabetes were excluded, and overall the recruited study participants might be healthier than the general population, being less likely to be current smokers (12·9 %) and overweight/obese (60·8 %) than the general population in Cambridgeshire (16·4 and 63·6 %, respectively)( 64 ). Although the study population might be healthier than the general population, unhealthy behaviours were nevertheless detected. For example, more than two-thirds of participants reported eating meals or snacks while watching television at least once weekly, and more than 30 % skipped breakfast at least twice weekly. Given the relatively high prevalence of sweetened beverage consumption observed, our study is unlikely to overstate needs for future interventions on such eating behaviours related to beverage consumption in the general population.
Implications
Our findings may help to inform strategies aiming to reduce consumption of sweetened beverages among adults. Population-based interventions, such as nutrition labelling, menu labelling and health warnings, need to allow for the lower level of education of frequent consumers of SSB and ASB. Labelling needs to be intelligible to all consumers, as those with lower education may have lesser comprehension of nutrition labels( Reference Cowburn and Stockley 65 ). Restricting television advertising of sweetened beverages may help to reduce consumption in the home, particularly given the higher levels of consumption among those who eat in front of the television.
Our findings support that while SSB taxation may be regressive, disproportionately affecting lower-income groups, the health benefits would be progressive in these groups given their higher levels of consumption and given that these groups were more likely to be obese in our study. However, taxation may not influence the other unhealthy eating behaviours observed among frequent sweetened beverage consumers.
Conclusions
The present study provides the first detailed insight into social and behavioural determinants of SSB and ASB consumption in a UK population. The findings help to clarify those who stand to benefit most from further public health interventions and support that future efforts to reduce sweetened beverage consumption warrant targeting of individuals’ behaviours as well as environmental influences.
Acknowledgements
Acknowledgements: The authors thank all participants and staff of the Fenland Study including the Fenland Study Coordination, Field Epidemiology and Data Management teams. They thank Dr Laura O’Connor at Medical Research Council Epidemiology Unit, University of Cambridge, for inputs at the planning stage of analysis. Financial support: The Fenland Study was funded by the Medical Research Council and the Wellcome Trust. This work was supported by MRC Epidemiology Unit core funding (grant numbers MC_UU_12015/1 and MC_UU_12015/5). The funders had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: P.B. and F.I. contributed equally to this study. P.B., F.I. and N.G.F. designed the study question. P.B. and F.I. conducted data analysis. P.B. drafted the manuscript with input from F.I. and N.G.F. N.J.W., N.G.F., S.J.G. and S.B. coordinated the Fenland Study as study principal investigators and N.J.W. is the study chief investigator. All authors provided critical inputs to revise the manuscript. All authors approved the final manuscript. Ethics of human subject participation: This study was approved by the Cambridge Local Ethics Committee.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S136898001700177X








