



The period of adolescence is characterized by many biological, psychosocial and cognitive changes that can influence nutritional needs and dietary behaviours(Reference Stang, Story, Stang and Story1). Diet patterns of adolescents today are characterized by skipping meals, snacking and eating out, which are compounded by a diet poor in healthy foods (e.g. fruits, vegetables and whole grains) and rich in unhealthy foods and beverages (e.g. processed foods; foods high in saturated fats, salt or added sugar; increased portion sizes; sugar-sweetened beverages)(2–Reference Scharf and DeBoer4). Unhealthy dietary behaviours have been associated with many nutrition-related health problems, the most important of which are obesity and chronic diseases(Reference Ford, Patel and Narayan5,Reference Lim, Vos and Flaxman6) . In 2010, unhealthy diets accounted for about 10 million deaths globally(Reference Lim, Vos and Flaxman6).
Despite the many negative health outcomes with unhealthy diets, more adolescents are engaging in these behaviours. In the most recent Health Behaviour in School-aged Children survey, which was conducted in forty-two European and North American mostly developed countries, 36 % of adolescents skipped breakfast, nearly one in five adolescents consumed soft drinks daily and only 37 % ate two or more servings of fruits every day(Reference Inchley, Currie and Young7). In developing countries the situation is even more alarming, according to data from the Global School-based Student Health Survey (GSHS)(8). Results of the GSHS revealed that more than half (54·3 %) of adolescents consumed carbonated soft drinks and over 70 % did not consume enough fruits and vegetables (F&V)(Reference Yang, Bovet and Liu9,Reference Darfour-Oduro, Buchner and Andrade10) . The transition in these developing countries to poor nutritional habits, confirmed by the GSHS, has led to rising rates of adolescent obesity(Reference Lim, Vos and Flaxman6,Reference Popkin, Adair and Ng11) .
Given the above results on unhealthy diets and the fact that dietary behaviours adopted during adolescence can track into adulthood(Reference Craigie, Lake and Kelly12), strategies to promote adolescent healthy dietary behaviours are needed. To develop a tailored strategy, it is first necessary to better understand the various factors that influence adolescent dietary behaviours, especially those that are modifiable(Reference Sallis, Owen and Fotheringham13,Reference Story, Neumark-Sztainer and French14) . To characterize these influences, a social-ecological framework is particularly useful(Reference Sallis, Cervero and Ascher15,Reference Story, Kaphingst and Robinson-O’Brien16) . This framework is a comprehensive approach that emphasizes connections between people and their environment. Dietary behaviours are thus seen as a function of multiple personal and environmental influences(Reference Sallis, Cervero and Ascher15).
Individual-level factors related to dietary behaviours include biology (e.g. age, gender, genes), demography (e.g. race/ethnicity, income), cognition (e.g. attitudes, knowledge, taste and preferences), lifestyle, outcome expectations, self-efficacy, motivations and behaviour control(Reference Story, Kaphingst and Robinson-O’Brien16–Reference Verstraeten, Van Royen and Ochoa-Aviles22). In an overview of determinants of dietary behaviours among youth, Sleddens et al. concluded that social-cognitive determinants have been mostly addressed towards the end of the 20th century, whereas environmental determinants have been studied only within the past 10 years(Reference Sleddens, Kroeze and Kohl21). Environmental-level influences can be separated into social, physical and macro-level environments. Influences within the social environment correspond to role modelling, social support and social norms from family, friends, peers and others(Reference Story, Neumark-Sztainer and French14,Reference Story, Kaphingst and Robinson-O’Brien16,Reference Krolner, Rasmussen and Brug17,Reference Rasmussen, Krolner and Klepp20,Reference Sleddens, Kroeze and Kohl21,Reference Gasser, Mensah and Clifford23) . Influences within the physical environment include accessibility and availability of food products in the different settings where adolescents eat or get food(Reference Story, Neumark-Sztainer and French14,Reference Story, Kaphingst and Robinson-O’Brien16,Reference Krolner, Rasmussen and Brug17,Reference Rasmussen, Krolner and Klepp20,Reference Sleddens, Kroeze and Kohl21) . Influences within the macro-level environment are mostly distal levels of influence and include social norms, agriculture and economic policies, food production and distribution structures, food marketing and prices(Reference Story, Neumark-Sztainer and French14,Reference Story, Kaphingst and Robinson-O’Brien16,Reference Krolner, Rasmussen and Brug17,Reference Rasmussen, Krolner and Klepp20,Reference Sleddens, Kroeze and Kohl21,Reference Deliens, Deforche and Annemans24,Reference Boyland and Halford25) .
The WHO emphasizes that national-level data are necessary to inform national decision makers on the most relevant policies to promote adolescent health(26). Quantitative studies can be used to rank the importance of influences on behaviour, while qualitative studies can generate a more thorough understanding of the behaviour(Reference Krolner, Rasmussen and Brug17,Reference Rasmussen, Krolner and Klepp20) . The mixed-methods approach is a procedure for collecting, analysing and mixing both quantitative and qualitative data at some stage of the research process within a single study(Reference Creswell and Plano Clark27). Mixed-methods studies bring together the strengths of quantitative and qualitative studies and could therefore provide a clearer understanding of the occurrence of adolescent behaviours(Reference Creswell and Plano Clark27).
With regard to Moroccan adolescents, the 2016 GSHS found that 13·9 % of Moroccan adolescents were overweight, nearly half drank carbonated soft drinks, 15 % ate fast foods and more than half did not consume enough F&V(8). Morocco, like many other developing countries, is also transitioning towards a Westernized diet, namely one that is low in nutrients and high in energy-dense refined sugars and fats and that includes processed foods(Reference Ford, Patel and Narayan5,Reference Aboul-Enein, Bernstein and Neary28,Reference Golzarand, Mirmiran and Jessri29) . So far, few studies have investigated what influences the dietary behaviours of Moroccan adolescents(Reference Aboul-Enein, Bernstein and Neary28,Reference El Achhab, Marfa and Echarbaoui30,Reference Musaiger, Al-Mannai and Tayyem31) and none of them used a qualitative or mixed approach. To help fill this gap, we conducted a sequential explanatory mixed-methods study to investigate the prevalence and social-ecological influences on adolescent dietary behaviours.
The objective of the quantitative phase was to determine the prevalence of four unhealthy dietary behaviours (skipping breakfast, inadequate F&V intake, fast-food consumption and soft drink consumption) in adolescents and to identify their sociodemographic-associated factors. The objective of the qualitative phase was to explore social-ecological influences on dietary behaviours examined in the quantitative phase, to allow a contextualized understanding of why these dietary behaviours occur.
Methods
Study design and target population
In this sequential, explanatory mixed-methods design (which begins with the collection of quantitative data, followed by the collection of qualitative data to explain and enrich the quantitative findings(Reference Creswell and Plano Clark27)), we connected quantitative and qualitative phases during the development of a guide for focus group (FG) discussions and through discussions of the outcomes of the entire study. The present study is part of larger ongoing research project(Reference El Achhab, El Ammari and El Kazdouh32), which has a major goal of developing and implementing an intervention that supports a healthy lifestyle among adolescents. Our study group included school-aged adolescents from Taza city, a medium-sized city (207 984 inhabitants) in north-central Morocco(33).
Quantitative study
Survey participants
We recruited 764 adolescents from February to March 2016. The sample size was estimated based on a population of 30 000 students(34), a confidence level of 95 % and a population proportion of 0·50. A multistage, stratified, cluster-random sampling method was used and a design effect coefficient of 2 was chosen, resulting in a final sample size of 760 (380 × 2). By using a stratified cluster-random sampling, six middle and secondary schools were selected from seventeen middle and secondary schools existing in Taza city. Thus, in the first step, two schools were randomly selected from each of three neighbourhoods defined by social-economic level (disadvantaged, average and advantaged). Next, four classes were randomly selected within each school. All students in these classes were invited to participate in the survey, resulting in a sample size of 764 adolescents.
Quantitative data collection
Students were asked to complete the Moroccan version of the GSHS. This questionnaire was developed by the WHO and the US Centers for Disease Control and Prevention in collaboration with other institutions. Details on the GSHS, a useful tool to assess health behaviours among students aged 13–17 years, are available on the Centers for Disease Control and Prevention’s website(8).
We were interested in four dependent variables: consumption of breakfast, F&V, soft drinks and fast foods. To assess breakfast consumption, the question ‘During the past 30 days, how often did you eat breakfast?’ allowed response options that ranged from 1 (= ‘never’)to 5 (= ‘always’). Skipping breakfast was defined as eating breakfast never, rarely or sometimes. To assess F&V consumption, the question ‘During the past 30 days, how many times per day did you usually eat fruit (e.g. bananas, apples, oranges or any other fruit) or vegetables (e.g. potatoes or tomatoes)?’ allowed response options that ranged from 1 (= ‘I did not eat fruits or vegetables during the past 30 days’) to 7 (= ‘I ate fruits or vegetables five or more times per day’). Inadequate F&V consumption was defined as having <5 servings/d. To assess soft drink consumption, the question ‘During the past 30 days, how many times per day did you usually drink carbonated soft drinks, such as Coca Cola or Fanta?’ provided response options that ranged from 1 (= ‘I did not drink carbonated soft drinks during the past 30 days’) to 7 (= ‘I drank carbonated soft drinks five or more times per day’). Participant responses were then coded as 1 (drinking carbonated soft drinks ≥1 times/d) or 0 (never). To assess fast-food consumption, the question ‘During the past 7 days, on how many days did you eat food from a fast-food restaurant, such as McDonald’s or Pizza Hut?’ allowed response options that ranged from 1 (= ‘0 days’) to 8 (= ‘7 days’). Responses were coded as 1 (ate food from a fast-food restaurant on ≥3 d) or 0 (ate food from a fast-food restaurant on <3 d).
Independent variables included sex, age, BMI, academic performance, perceived family income, educational level of parents and mother’s employment status. The international age- and sex-specific child BMI (calculated as weight/height2; kg/m2) cut-off points were used to define overweight and obesity(35).
Quantitative data analysis
Data were analysed using the statistical software package IBM SPSS Statistics version 19. Bivariate and multivariate analyses were performed to evaluate associations between dependent and independent variables. Statistical significance was defined as P < 0·05. Odds ratios with 95 % confidence intervals were derived where appropriate. Independent variables were included in the multivariate analysis if they had a significant association (P < 0·20) with a dependent variable in the bivariate analysis.
Qualitative study
Participants in focus group discussions
Participants were recruited from two middle schools (disadvantaged and advantaged per socio-economic level) that participated in the quantitative portion of the study. From each school, 14–16-year-old students were invited to participate in focus group discussions (FGD). Adolescents, parents and teachers received an information letter that provided a comprehensive explanation of study objectives and processes, as well as an informed consent form to sign. After participant informed consent was received, researchers, participants and school officials selected an appropriate date and setting to conduct FGD. Sampling continued until data saturation was reached.
Qualitative data collection
We chose the FG method because it encourages interactive discussions between participants(Reference Morgan36). Discussions with participants were conducted by a moderator with the assistance of an observer who were trained to conduct FGD. These discussions followed a semi-structured guide underpinned by the social-ecological framework as a theoretical framework(Reference Sallis, Cervero and Ascher15). This guide was pilot-tested with a convenience sample of each type of participant and refined before definitive use. Discussions were aimed at exploring social-ecological factors influencing the consumption of breakfast, F&V and fast/snack foods among adolescents. Snack foods were those that are energy-dense and nutrient-poor (high in sodium, sugar and/or fat) that are prepared outside the home such as cookies, cakes, sugar-sweetened beverages, chips and some unhealthy street foods(Reference Hess, Slavin and Jonnalagadda37). Table 1 shows the main questions asked during FGD. The total number of FG was determined by the saturation principle.
Table 1 Focus group discussion steps

* Questions in Steps 2 and 3 served to map discussions; however, there were other direct questions that emanated from participants to clarify their statements.
FG were homogeneous with regard to sex to overcome possible bias and to provide an opportunity for possible sex-specific factors to appear. Discussions were conducted in a suitable room in the participating schools and were audio-recorded with permission from participants. Participants also gave permission to use their anonymous quotes in research publications.
Qualitative data analysis
Audio tapes from the discussions were fully transcribed and organized into separate data sets for adolescents, parents and teachers. All data sets and notes from the observer were then analysed using the thematic analysis method of Braun and Clarke(Reference Braun and Clarke38). Thematic analysis is an easy and flexible qualitative analytic method that can identify, analyse and report themes within data(Reference Braun and Clarke38). Themes are patterns which capture something interesting about the data in relation to the research question(Reference Braun and Clarke38). During analysis, coders followed one-by-one the different steps outlined by Braun and Clarke, which are: becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, defining themes and producing the report(Reference Braun and Clarke38). Coders started reading and re-reading transcripts to become familiar with the data, took notes and jotted down early impressions. Then, open coding was used; that means we did not have pre-set codes but developed and modified the codes as we worked through the coding process. In addition, the coding process included consideration of our research question. So, this was an inductive-deductive thematic analysis. The next step was to search for themes; once the initial codes were generated, we started to combine them to form overarching themes. Themes were predominantly at the semantic level; that is, they were identified within the explicit or surface meanings of the data. After developing the initial themes, they were continually reviewed, created and discarded using an iterative process. Thus, we constantly moved back and forth between the selected extracts from the data and the entire data set to check if the themes made sense and accounted for all the coded extracts and the entire data set, to assess the applicability of themes. Finally, each theme was defined, labelled and analysed. A thematic map was also established, in which themes were organized within individual and environmental levels of the social-ecological model.
Doubts or disagreements between coders were discussed under the supervision of another researcher skilled in qualitative analysis until consensus was reached. Some quotes illustrating themes and sub-themes were translated into English. The analysis was conducted manually (i.e. no software was used in the data analysis).
Results
Quantitative results
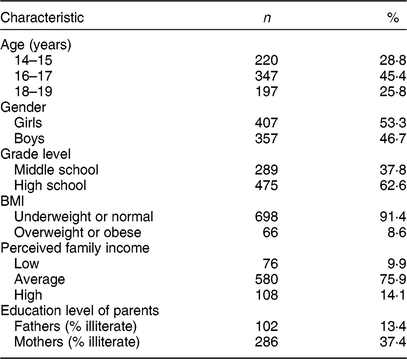
The survey sample consisted of 764 adolescents aged 14–19 years (response rate of 95·5 %); 53·3 % were girls. Other sample characteristics are presented in Table 2. Overall, 46·1 % of surveyed adolescents skipped breakfast, 60·6 % had inadequate F&V intake, 39·4 % consumed soft drinks and 28·0 % consumed fast foods (Fig. 1).
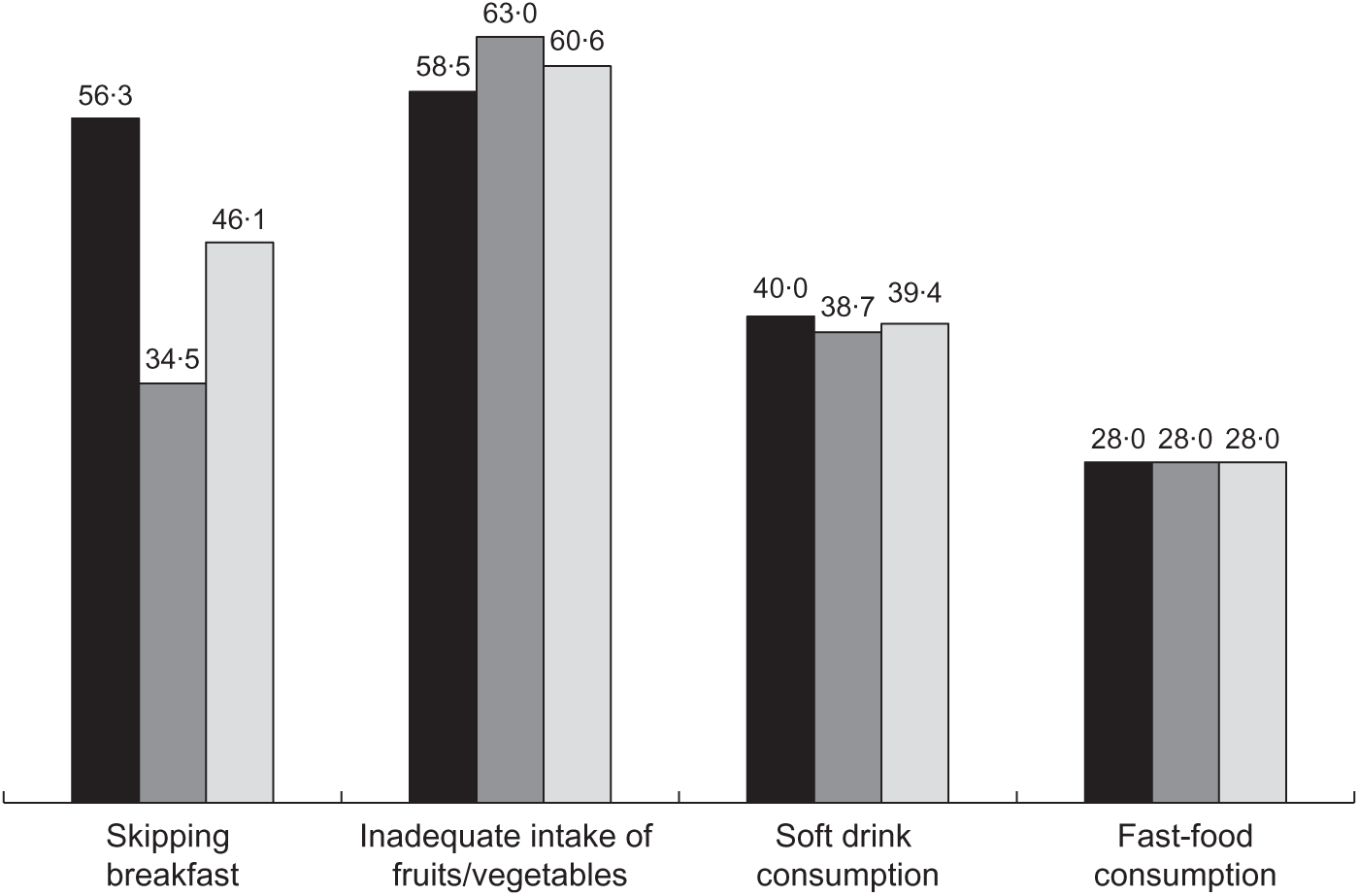
Fig. 1 Prevalence (%) of four unhealthy dietary behaviours, by sex ( , girls;
, girls;  , boys;
, boys;  , total), among adolescents aged 14–19 years (n 764) from Taza city, Morocco, February–March 2016
, total), among adolescents aged 14–19 years (n 764) from Taza city, Morocco, February–March 2016
Table 2 Sociodemographic characteristics of participants in the quantitative phase of the study: adolescents aged 14–19 years (n 764) from Taza city, Morocco, February–March 2016
In multivariate analysis (Tables 3 and 4), skipping breakfast was most prevalent among girls, adolescents with low academic performance and those who consumed fast foods. Inadequate F&V intake was negatively associated with consumption of soft drinks and fast foods. Soft drink consumption was negatively and positively associated with inadequate F&V intake and fast-food consumption, respectively. Fast-food consumption was most prevalent among breakfast skippers and those who consumed soft drinks. However, it was negatively associated with adolescents who were between 16 and 17 years old, those with a low perceived family income, those who had an illiterate mother and those with inadequate F&V intake.
Table 3 Associations between dependent variables (skipping breakfast and inadequate intake of fruits and vegetables) and sociodemographic variables among adolescents aged 14–19 years (n 764) from Taza city, Morocco, February–March 2016

UOR, unadjusted odds ratio; AOR, adjusted odds ratio; ref., reference category.
Significant P values are indicated in bold font.
Table 4 Associations between dependent variables (consumption of soft drinks and fast foods) and sociodemographic variables among adolescents aged 14–19 years (n 764) from Taza city, Morocco, February–March 2016

UOR, unadjusted odds ratio; AOR, adjusted odds ratio; ref., reference category.
Significant P values are indicated in bold font.
Qualitative results
A total of 100 people participated in the seventeen FGD. The estimated point of saturation was observed after eight FG of adolescents (n 56; 50 % boys), five FG of parents (n 26; 81 % males) and four FG of teachers (n 18). The average number of participants per FG was seven for adolescents, five or six for parents, and four or five for teachers. Each FGD lasted between 50 and 80 min.
After data analysis, we identified seven main themes regarding potential social-ecological influences on adolescent dietary behaviours studied in the quantitative phase. Four themes were at the individual level, which included cognitive (theme 1), affective and biological (theme 2), lifestyle (theme 3) and outcome expectation (theme 4) influences. Three themes were at the environmental level, which included social network (theme 5), accessibility and availability (theme 6) and macro-level (theme 7) influences. Figure 2 presents a thematic map of main themes summarizing the social-ecological influences on adolescent dietary behaviours. Example quotes to support themes and sub-themes are shown in Table 5 and in the online supplementary material. Table 6 summarizes the number of codes and quotes for each theme.

Fig. 2 Thematic map of main themes regarding social-ecological factors influencing adolescent dietary behaviours ( , environmental influences;
, environmental influences;  , individual influences; T, theme; →, one-way effect; ↔, mutual effect between two themes; >>>, environmental factors influence individual factors, and together they influence adolescents’ dietary behaviours)
, individual influences; T, theme; →, one-way effect; ↔, mutual effect between two themes; >>>, environmental factors influence individual factors, and together they influence adolescents’ dietary behaviours)
Table 5 Quote examples from each of the themes and sub-themes arising from seventeen focus group discussions conducted with 100 participants (fifty-six adolescents aged 14–16 years, twenty-six parents and eighteen teachers) from Taza city, Morocco, February–March 2016

T, theme.
Table 6 Number of codes and quotes for each theme, according to the category of participants, arising from seventeen focus group discussions conducted with 100 participants (fifty-six adolescents aged 14–16 years, twenty-six parents and eighteen teachers) from Taza city, Morocco, February–March 2016

T, theme.
Theme 1: Cognitive influences (individual level)
Two sub-themes emerged from this theme: (i) perceived healthy and unhealthy dietary patterns; and (ii) knowledge, awareness and attitudes.
With regard to the first sub-theme, adolescent and parent participants categorized dietary behaviours among adolescents into healthy and unhealthy patterns. Healthy patterns included a balanced diet, diversified diet and diet based on natural products, as well as more frequent family meals eaten at home. Traditional eating patterns were considered better than less traditional patterns. Unhealthy dietary patterns were perceived as eating food away from home (i.e. ‘eating out’, which could include fast foods, snacks, soft drinks, cookies, sweets and chips), skipping meals, fewer family meals and inadequate consumption of F&V and cereals. Teachers, for their part, confirmed these views and mentioned that today’s adolescents are largely oriented towards adopting unhealthy dietary patterns.
According to all participant groups, knowledge, the second sub-theme, can influence adolescent dietary choices and behaviours. Adolescents make good dietary choices if they have sufficient nutritional knowledge, including nutritional recommendations and information on benefits and risks related to foods or dietary behaviours. Concurrently, participants reported that adolescents may lack appropriate nutritional awareness to make good eating choices. Adolescents perceived that F&V intake is beneficial to health, but they ignored the daily recommended amount. Parents and teachers recognized their role in shaping dietary culture among adolescents, while each of them minimized their responsibility. Finally, some adolescents stated that they consume some foods despite awareness that these foods can harm their health.
Theme 2: Affective and biological influences, including appetite, taste and preferences, and hunger (individual level)
Adolescent girls and parents indicated that poor appetite in the morning was an important cause for breakfast skipping, especially among girls.
Adolescent participants indicated a preference for tasty foods, with fruits favoured over vegetables and some vegetables even hated. There also was a preference for snacks, soft drinks and cookies consumed away from home v. prepared at home, with the former perceived as tastier. This view was shared by parents and teachers. In addition, adolescents also stated that hunger was another reason for eating fast foods.
Theme 3: Lifestyle-related influences (individual level)
Two sub-themes emerged from this theme: (i) time and convenience; and (ii) behaviours.
All participant groups considered lack of time, the first sub-theme, as a real barrier to healthy eating in adolescents. Indeed, adolescents, especially boys, who woke up late in the morning reported not having enough time to eat breakfast. Adolescents and parents reported that academic achievement pressures and spending time away from home seemed to push adolescents to eat fast foods. According to all groups of participants, some unhealthy foods (e.g. cookies, fast foods) were found to be more convenient than healthy foods (e.g. dairy products, F&V) or those prepared at home.
With regard to the second sub-theme, all participants stated that many adolescent eating behaviours (healthy or unhealthy) are rooted in those established when much younger; therefore, eating behaviours can be tracked from childhood to adolescence. Some participants, especially teachers, reported that adolescent lifestyle can influence eating behaviours. Thus, an organized lifestyle (i.e. with good time management) seemed to positively affect adolescents’ eating habits.
Theme 4: Health and social outcome expectation influences (individual level)
Some health expectations were reasons for adolescents to adopt good eating behaviours. Adolescents expressed a desire to preserve their current and future health from certain diseases (e.g. overweight, diabetes and hypertension). Most of these adolescents had parents or relatives who had these diseases. Some adolescents reported that they consume breakfast to better concentrate in class, whereas others, especially girls, stated adopting certain eating habits to maintain a desirable weight or physical appearance. From a social perspective, some adolescents, parents and teachers thought that adolescents consumed fast foods in order to show off in front of their friends or to not feel isolated from the group.
Theme 5: Social network (environmental level)
This theme includes two sources of influences: family members and peers. Regarding family influences, all participant groups mentioned that parents play a primary role in building dietary behaviours and background knowledge among adolescents. They reported that parents play an important role through different mechanisms, including having frequent family meals, preparing tasty and healthy meals, and advising and/or controlling the dietary habits of their children. In the same vein, adolescents and teachers found that parents do not play this role properly. One student stated, ‘I do not take my breakfast because my mother does not prepare it for me’ (Table 5). Parents, in turn, stated that providing a nutritional education to children is a real challenge, acknowledging an inability to overcome the pressures (e.g. availability and affordability of competitive unhealthy foods, food advertising and peer pressure) to which their children are exposed. According to all groups of participants, other barriers related to the family environment included working parents and low family income.
Influences of peers were seen as barriers to good dietary behaviours among adolescents by all participant groups. Regarding obtaining food outside of home, quotes from FGD among adolescents included ‘Everybody buys, I buy them too’ and ‘I eat them with my friends’ (Table 5).
Theme 6: Availability and affordability of foods (environmental level)
The quotes shown in Table 5 with regard to theme 6 suggest that an adolescent’s dietary intake is positively influenced by availability and variety of healthy food options such as F&V in the home. Adolescents found unhealthy competitive foods to be readily available,affordable, tasty and varied compared with foods prepared at home and stated a preference for them. This was reiterated by parents and teachers. Furthermore, students said that they buy unhealthy foods during recess from the school environment, which is not controlled by the relevant authorities.
According to all participant groups, prices of F&V, dairy products and other healthy foods were perceived as high, limiting their affordability for socio-economically disadvantaged families. Some parents mentioned that living in a poor neighbourhood could limit adolescents’ access to healthy foods.
Theme 7: Distal influences (environmental level)
Although all groups of participants considered that media could improve nutritional awareness among adolescents, most of them found media played a negative role, including encouraging adolescents to adopt unhealthy eating habits through advertisements.
Regarding the role of schools in dietary decisions, teacher participants confessed that this role was insufficient. ‘The school currently has a very limited role’, said one teacher (Table 5). Parents and adolescents had the same point of view as teachers. When asked to explain this, teachers reported that, on the one hand, current school programmes do not provide adequate nutritional education. On the other hand, this lack of health education is countered by the abundance of unhealthy foods, influences of media and advertising and peer pressures.
Parents and teachers affirmed that Moroccan society is becoming increasingly involved in modern and Western food patterns, with some foods considered as symbols of fashion and cultivation.
Discussion
Overall, the extent of unhealthy dietary behaviours among adolescents was concerning. Many skipped breakfast (46·1 %), had inadequate intake of F&V (60·6 %), consumed soft drinks (39·4 %) and ate fast foods (28·0 %). Quantitative and qualitative findings showed that the dietary behaviours of adolescents were the result of inseparable interactions among individual and environmental factors.
Breakfast intake
Although many adolescents skip breakfast, the regular consumption of breakfast has been shown to be of benefit to their general health(Reference de la Hunty, Gibson and Ashwell39,Reference Hallstrom, Labayen and Ruiz40) . Quantitatively, we found that breakfast skippers were more often girls than boys, ate more fast foods and had lower academic performance.
In the literature, skipping breakfast is typically more prevalent among girls(Reference Rampersaud, Pereira and Girard41,Reference Savige, Macfarlane and Ball42) . This gender difference is not fully understood, but was often explained by the higher weight-related concerns among girls compared with boys(Reference Mullan, Wong and Kothe43,Reference Rashidi, Mohammadpour-Ahranjani and Karandish44) . The girls in our survey reported that lack of hunger and appetite in the morning was the main reason to skip breakfast. Like previous studies(Reference Moreno, Rodriguez and Fleta3,Reference Rampersaud, Pereira and Girard41,Reference Savige, Macfarlane and Ball42) , our findings showed that adolescents who skipped breakfast ate more fast foods. The mechanism linking breakfast skipping and fast-food intake was clarified during the FGD, with breakfast skippers reporting that they purchased fast/snack foods at school when they felt hungry. Because fast/snack foods are energy-dense, skipping breakfast could lead to weight gain in adolescents(Reference Moreno, Rodriguez and Fleta3,Reference de la Hunty, Gibson and Ashwell39) . Moreover, breakfast-skipping behaviour has been associated with other health-risk behaviours such as physical inactivity, which explains the high frequency of this behaviour among obeseadolescents(Reference Rampersaud, Pereira and Girard41). Therefore, habitual breakfast consumption could contribute to prevention of childhood obesity(Reference Mesas, Munoz-Pareja and Lopez-Garcia45).
In addition, our survey showed a positive association between breakfast skipping and low academic performance. During FGD, some breakfast eaters conveyed that they have breakfast to not feel hungry and to better concentrate in class. In assessments of the effects of breakfast consumption on cognitive and academic outcomes(Reference Rampersaud, Pereira and Girard41,Reference Edefonti, Rosato and Parpinel46) , it was found that adolescents may be more vulnerable to the nutritional effects of breakfast on brain activity and associated cognitive and academic outcomes than adults(Reference Edefonti, Rosato and Parpinel46). Although evidence is not consistent, habitual breakfast consumption could improve many aspects of cognitive and academic outcomes (e.g. memory, attention and concentration, school attendance) by hunger alleviation(Reference Rampersaud, Pereira and Girard41,Reference Edefonti, Rosato and Parpinel46) , with type of breakfast and time of administration also having possible effects(Reference Edefonti, Rosato and Parpinel46).
We found that skipping breakfast in adolescents was influenced by several individual and environmental factors. Individual factors included sex (girl), lack of time (because of waking up late), and lack of hunger and appetite in the morning. Environmental factors were mainly at the family and home level and included insufficient parental support (e.g. not preparing breakfast for children, not having breakfast together) and lack of availability of varied foods.
Given the importance of breakfast consumption for adolescent health, interventions aimed at improving this dietary behaviour are needed. Some of the modifiable influences that we have identified could be used to design a future intervention programme; these could include improving adolescent knowledge and skills regarding the importance of breakfast consumption and improving time management skills. Parents need to be involved in such interventions to provide family support (e.g. preparing breakfast, providing various items, acting as a role model, controlling pocket money).
Intake of fruits and vegetables
Many adolescents (60·6 %) in our study did not reach the threshold of eating five daily portions of F&V, which is close to the national prevalence (54·5 %) and compares with findings of other low- and middle-income countries(8,Reference Darfour-Oduro, Buchner and Andrade10) . Although epidemiological evidence has suggested that a diet rich in F&V could promote health and prevent chronic diseases(2,Reference Lim, Vos and Flaxman6,Reference Spear, Barlow and Ervin47) , diets low in F&V were responsible for more than 6 million deaths in 2010(Reference Lim, Vos and Flaxman6).
It is well known that F&V intake is strongly influenced by socio-economic status(Reference Krolner, Rasmussen and Brug17). Our survey results showed that adolescents with uneducated mothers consumed fewer F&V. These results are congruent with previous studies because parents’ education level can be used to assess family socio-economic level(Reference Currie, Molcho and Boyce48). Individuals at low socio-economic levels had decreased F&V availability, which in turn decreased their intake, as confirmed by participants during FGD.
We also found that various individual and environmental factors contributed to inadequate F&V intake. Individual factors included attitude, knowledge, taste, perceived time constraints, convenience and outcome expectations. Environmental factors included availability and affordability of F&V in the home and social factors.
Although most of our participants perceived that F&V intake is beneficial to health, adolescents were unable to list these benefits and they were unaware of the daily recommended amount of F&V. Because poor knowledge about the recommended intake level might lead to an overestimation of own F&V intake(Reference Wind, Bobelijn and De Bourdeaudhuij49), we suggest improving adolescents’ awareness regarding recommendations through interventions.
Another barrier to F&V intake in our participants was perceived bad taste, especially of vegetables. It has been documented that children value taste over health and that F&V are not among their favourite foods(Reference Krolner, Rasmussen and Brug17). Given that taste is influenced by some features such as familiarity and methods of preparation, parents are encouraged to expose their children to a variety of F&V from a young age and should pay more attention to methods of preparation.
Convenience was another factor that influenced F&V consumption in adolescents. Compared with competitive unhealthy choices such as fast/snack foods, participants perceived that F&V are less convenient as they are not easy to prepare, transport and eat outside the home. This inconvenience has been shown to be a key barrier limiting F&V intake, with greater influence than other factors(Reference Krolner, Rasmussen and Brug17). In addition, children do not eat inconvenient F&V, even those that they perceive as tasty(Reference Krolner, Rasmussen and Brug17).
Our findings showed that F&V intake in adolescents was driven by their health outcome expectations, which have been previously classified as short- and long-term outcomes(Reference Krolner, Rasmussen and Brug17). In accordance with previous studies(Reference Krolner, Rasmussen and Brug17,Reference Story, Stang, Stang and Story50) , our adolescent participants tended to be more concerned about short-term outcomes (e.g. energy, healthy weight, physical appearance, school performance) than long-term outcomes such as chronic diseases. For future intervention, messages to youth related to diet should focus on short-term or immediate benefits, as they would have more appeal(Reference Story, Stang, Stang and Story50).
Participants in our study stated that availability of F&V at home was a key factor affecting adolescents’ F&V consumption. This importance is asserted by other studies, which stated that F&V intake increased despite not liking the taste when F&V are available at home(Reference Story, Kaphingst and Robinson-O’Brien16,Reference Krolner, Rasmussen and Brug17,Reference Sleddens, Kroeze and Kohl21) . Because prices of F&V were perceived as high, their affordability was limited, especially for socio-economically disadvantaged families. Not surprisingly, F&V intake in adolescents is influenced by their home accessibility(Reference Story, Kaphingst and Robinson-O’Brien16,Reference Krolner, Rasmussen and Brug17) . Although F&V availability at home is difficult to ameliorate because it depends on socio-economic level, parents need to be aware of the importance of F&V to increase accessibility to their children.
Our qualitative findings also showed that the social environment was both a facilitator and barrier for F&V intake in adolescents; consequently, the social environment can be both supportive and unsupportive. Mechanisms in an adolescent’s social environment (e.g. support and pressure from family, friends and peers) that can influence F&V intake include role models, social support and social norms(Reference Story, Kaphingst and Robinson-O’Brien16,Reference Sleddens, Kroeze and Kohl21,Reference Story, Stang, Stang and Story50,Reference Patrick and Nicklas51) . We therefore suggest that intervention programmes should involve parents because of their key roles in an adolescent’s social environment.
Fast and snack foods eaten outside home
Many foods prepared and consumed outside of home, such as fast foods and soft drinks, have low nutrient levels and are energy-dense(Reference Moreno, Rodriguez and Fleta3,Reference Scharf and DeBoer4,Reference Hess, Slavin and Jonnalagadda37) . Among our Moroccan adolescents, 39·4 and 28·0 % consumed soft drinks and fast foods, respectively. Consumption of soft drinks and fast foods was prevalent among adolescents who skipped breakfast and adolescents with working mothers. Those adolescents who skipped breakfast reported being hungry later in the day, resulting in more fast-food consumption, compared with those who ate breakfast. Busy work schedules of parents and lack of time prompted adolescents to eat outside the home. In addition, parental work schedules contributed to decreased supervision of adolescents’ dietary habits, thereby allowing adolescents to eat unhealthy foods(Reference Jenkins and Horner52).
We found that adolescents with educated mothers or low family income consumed fewer fast foods and soft drinks. This issue was not evoked during FGD. Educated mothers may be more aware of the negative health consequences of food choices and consequently thus supervise the eating habits of their children. Furthermore, mothers from low-income households in Morocco are generally housewives, which could decrease intakes of fast foods and soft drinks by increasing the frequency of family meals.
Qualitative analysis through FGD allowed us to thoroughly understand the individual and environmental factors facilitating food consumption outside of home (e.g. snack and fast foods, street foods, soft drinks). Individual factors were mainly greater preference, time constraints, educational plans, pocket money, low awareness and social expectations (e.g. social integration). Environmental factors were availability and affordability of fast/snack foods, low parental support, peer pressure, media advertising and insufficient health education at school. The availability of snack and fast foods and beverages in the school environment was considered a real problem. Reducing the availability of unhealthy foods and increasing the availability of healthy ones in the school environment has had promising results(Reference Bowen, Barrington and Beresford53). Other intervention strategies have been effective in reducing the consumption of fast/snack foods(Reference Scharf and DeBoer4), including plain packaging, warning labels and taxes on sugary beverages(Reference Bollard, Maubach and Walker54). In accordance, because of the many causes of unhealthy dietary behaviours, multifaceted programmes are required(Reference Scharf and DeBoer4,Reference Spear, Barlow and Ervin47) .
Contrast in the participants’ perspectives
Altogether, the perspectives from the different groups of participants were usually convergent and complementary. As has been shown in Table 6, all themes emanated from all groups of participants even though some themes were unequally supported.
Differences between participants’ perspectives concerned responsibilities of parents and school to improve adolescents’ dietary patterns (e.g. background knowledge and behaviours). These findings were consistent with the concept of attribution error (i.e. the tendency of blaming situational factors when justifying one’s behaviour) which has been reported by previous studies(Reference Verstraeten, Van Royen and Ochoa-Aviles22,Reference Heider55) . Indeed, adolescents and teachers perceived that parents do not play their role properly, while parents blamed other factors such as availability and affordability of competitive unhealthy foods, food advertising and peer pressure. Moreover, previous research has suggested that because of low perceived control, parents absolve themselves of personal responsibility for the behaviours of their children. In this way, they can pose a barrier to the success of intervention campaigns(Reference Hart, Herriot and Bishop56). While teachers recognized the role of school in shaping adolescents’ dietary behaviour, they minimized their responsibility. When asked to explain this, teachers mentioned various factors like school programmes which did not provide adequate nutritional education, the abundance of unhealthy foods, influences of media and advertising, and peer pressures.
Limitations
Because of the cross-sectional and qualitative nature of this research, we could not infer causality or define which factor was the most significant in influencing adolescent dietary behaviour. During the qualitative phase of the study, we explored all potential social-ecological influences on adolescent dietary behaviours, whereas, in the quantitative phase, we investigated only the sociodemographic factors as independent variables.
Conclusions
The prevalence of unhealthy dietary behaviours in our study group of Moroccan adolescents is a concern. Unhealthy dietary behaviours are the result of inseparable interactions between individual and environmental factors. Modifiable factors should be targeted in the design of future interventions aimed at improving breakfast and F&V consumption and reducing fast/snack-food consumption among adolescents.
Acknowledgements
Acknowledgements: The authors are very grateful to all participants (adolescents, parents and teachers) who took part in FGD. They also thank the provincial director of the education ministry and teachers/headmasters/principals of the participating schools for their invaluable collaboration. Special thanks are due to Rasa G. Hamilton and Peter A. Kanetsky (Moffitt Cancer Centre) for their valuable support in editing the manuscript. Thanks also go to H. Azzam and her team for the workshops organized in Morocco on capacity building where this project has matured. The authors would also like to thank K. El Rhazi for the coordination of these workshops. Financial support: This study was supported by Moffitt Cancer Centre under the National Institutes of Health (NIH) International Fogarty Centre (Principal Investigator, Anna Giuliano; award number 5D43TW009804). The funder also contributed to the study design and English language editing of the manuscript. Conflict of interest: None. Authorship: A.E.-A. carried out the literature searches, drafted and finalized the paper. All authors contributed equally in designing the study. A.E.-A., H.E.K. and S.B. were responsible for data collection, transcription, coding and analysis. Y.E.-A. and S.E.F. helped in data coding and analysis, supervised the study and coordinated the research team. All authors have read, revised and approved the final draft of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Faculty of Medicine and Pharmacy of the Casablanca Research Ethics Committee and by the National Control Commission for the Protection of Personal Data (A-RS-193-2015). Written informed consent was obtained from all parents and teachers, and adolescents’ consent forms were signed by their parents.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1368980019003641










