


Obesity is one of the most serious public health challenges of the 21st century( 1 , 2 ). Overweight and obesity is the fifth leading cause of global deaths( 1 ) and its prevalence has increased substantially over the past two decades( 2 , Reference Kelishadi, Ardalan and Gheiratmand 3 ). Obesity is associated with an increased risk of physical and psychosocial conditions, including type 2 diabetes, cardiovascular and liver diseases as well as social stigmatisation, low self-esteem and depression( 4 ). There is an increasing focus on the factors influencing the establishment of behavioural risk factors for obesity and related chronic diseases. Specifically, health-related behaviours established in adolescence often continue into adulthood and influence the risk of obesity( Reference Kelishadi, Ardalan and Gheiratmand 3 , Reference Leal, de Oliveira and Rodrigues 5 , Reference Currie, Zanotti and Morgan 6 ).
Adolescence is a transition period between puberty and adulthood, and refers to young people aged 10 to 19 years( 7 ). Adolescence is a period of increased autonomy and independent decision making that may influence health-related behaviours( Reference McKinley, Lowis and Robson 8 ). Dietary intake is one way that adolescents express their independence( Reference McKinley, Lowis and Robson 8 ), reinforcing the importance of promoting healthy eating in this stage of life( Reference Leal, de Oliveira and Rodrigues 5 , Reference Currie, Zanotti and Morgan 6 ). Adolescents’ dietary patterns are characterised by frequent snacking, fast-food consumption and meal skipping; and many adolescents do not meet nutrition recommendations( Reference McKinley, Lowis and Robson 8 , Reference Laska, Larson and Neumark-Sztainer 9 ). Adolescents and young adults are among the most frequent consumers of restaurant meals, away-from-home meals and packaged snacks( Reference Laska, Larson and Neumark-Sztainer 9 ). These dietary intake patterns promote weight gain and are associated with increased risk of obesity, type 2 diabetes, CVD and some cancers( Reference Laska, Larson and Neumark-Sztainer 9 – Reference Lichtenstein and Ludwig 11 ). Therefore, it is essential that public health promotion strategies and interventions focus on promoting healthy dietary intake during adolescence and subsequently into adulthood.
Previous attempts to reduce the prevalence of adolescent overweight and obesity have displayed minimal to modest outcomes( Reference Crowle and Turner 12 – Reference Summerbell, Waters and Edmunds 14 ). Interventions are generally successful in increasing nutrition-related knowledge but do not observe improvements in dietary intake( Reference Micucci, Thomas and Vohra 15 ). It has been suggested that these outcomes have occurred because previous interventions have failed to connect nutrition-related knowledge, skills and critical decision making about dietary intake( Reference Lichtenstein and Ludwig 11 ). Collectively, these concepts are called ‘food literacy’ and could be the key to improving the outcomes of future interventions in this area.
The concept of ‘food literacy’ is relatively new( Reference Pendergast, Garvis and Kanasa 10 ). Early studies defined food literacy as ‘the capacity of an individual to obtain, process and understand basic information about food and nutrition as well as the competence to use that information in order to make appropriate health decisions’( Reference Kolasa, Peery and Harris 16 ). Defined in this way, food literacy is not just nutrition knowledge; it includes skills and behaviours, from knowing where food comes from to the ability to select and prepare these foods and behave in ways that meet nutrition guidelines. Recently, the definition has been broadened and described as ‘a collection of inter-related knowledge, skills and behaviours required to plan, manage, select, prepare and eat foods to meet needs and determine food intake’( Reference Vidgen and Gallegos 17 ).
The concept of food literacy builds upon the work that has been done around the relationship between food knowledge and food choices, more broadly, the relationship between knowledge and behaviour. A number of well-respected behaviour change theories, such as Bandura’s Social Cognitive Theory, explain how knowledge creates the precondition for change including the self-regulation of health-related habits such as food choices( Reference Bandura 18 , Reference Rosenstock, Strecher and Becker 19 ). Although knowledge regarding healthy eating behaviour is necessary, the extensive research on behaviour change suggests that knowledge on its own is often not sufficient to change individual behaviour (including food choices)( Reference Clifford, Anderson and Auld 20 ). This highlights the need to move beyond knowledge to more inclusive concepts such as literacy to effect change in behaviours of interest, including diet( Reference Kelly, Melnyk and Belyea 21 , Reference Seeley, Wu and Caraher 22 ). As such, the concept of food literacy offers an integrative framework for investigating and understanding the factors shaping food intake and dietary patterns at an individual level.
Clarifying the influence of food literacy on dietary intake is important for the development of effective obesity prevention and management strategies. In addition, understanding the extent of the association may assist in predicting the impact of health promotion strategies that focus on improving food literacy in order to improve individuals’ dietary intake. Most food literacy interventions in adolescents have focused on process evaluation outcomes such as participant satisfaction, intentions, attitudes or preferences for healthy foods, or changes in learned skills and behaviours, rather than changes in dietary intake( Reference Condrasky, Corr and Sharp 23 – Reference Woodruff and Kirby 31 ). Therefore, it is important to critically review literature that has investigated associations between food literacy and dietary intake of adolescents. The present systematic review aimed to investigate the association between food literacy and adolescents’ dietary intake.
Methods
The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement checklist, which is a tool commonly used in reporting systematic reviews( Reference Moher, Liberati and Tetzlaff 32 ). For the purpose of the present review, ‘adolescence’ was defined as individuals aged from 10 to 19 years and ‘food literacy’ was defined as ‘a collection of inter-related knowledge, skills and behaviours required to plan, manage, select, prepare and eat foods to meet needs and determine food intake’( Reference Vidgen and Gallegos 17 ).
Search methods
Articles were sourced from electronic searches of six databases: MEDLINE (EBSCO Host), Cochrane Library, PsycINFO, Web of Science, PubMed and Scopus. These databases afford broad coverage of allied health, including nutrition and public health, literature. Due to the multifaceted definition of food literacy, a food literacy definition matrix was developed to identify relevant search terms based on each component of food literacy. The matrix was informed by previous definitions of food literacy( Reference Kolasa, Peery and Harris 16 , Reference Vidgen and Gallegos 17 , Reference Fordyce-Voorham 33 ) and encompassed factors of knowledge, skills and behaviours with food planning, management, selection, preparation and eating. The following search terms were identified and used in combinations to search each database: ‘food literacy’, ‘nutrition literacy’, ‘nutrition’, ‘food’, ‘diet’, ‘nutrition knowledge’, ‘food knowledge’, ‘cooking knowledge’, ‘food preparation knowledge’, ‘food skills’, ‘cooking skills’, ‘food preparation’, ‘food purchasing’, ‘food selection’, ‘food labels’, ‘label reading’, ‘adolescent’, ‘youth’, ‘teenager’, ‘teens’. To complement this search strategy, forward citation searching was undertaken on the reference list of articles considered for review.
Study selection
A list of potentially relevant articles from each database was identified, exported and saved into EndNote® version X6. Duplicates were identified and removed; relevant articles were scanned to confirm relevance for full review by three authors independently. Articles were included for consideration if the title, abstract or the keywords indicated the study measured an aspect of food literacy and a measure of dietary intake in adolescents. Studies were limited to adolescent populations aged 10 to 19 years without mental health or learning difficulties. If the age range of participants extended beyond 10 to 19 years, then the studies were included if the mean age was ≥10 years or ≤19 years. There was no restriction on the year of publication or language. Differences in selections were discussed before the list of included studies was finalised. Ineligible articles were removed from the list after noting the reason for exclusion. The PRISMA flow diagram was used to document the systematic review search and selection processes of the study (see Fig. 1)( Reference Moher, Liberati and Tetzlaff 32 ).
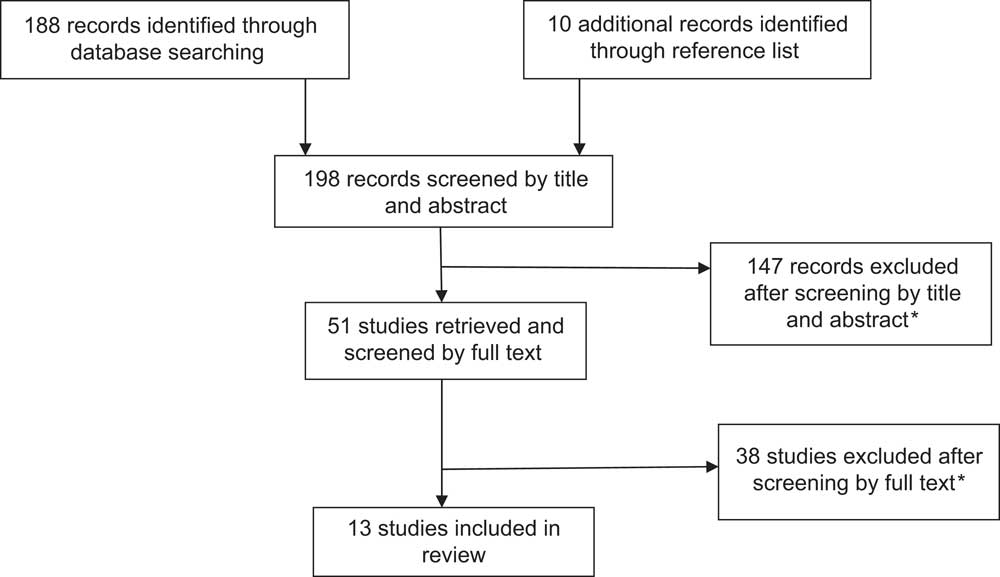
Fig. 1 Flowchart of the literature search and review process. *Reasons for exclusion: study population not adolescents (adults or young children; n 69); study did not address the main objective of the present review (n 31); study had no food literacy or dietary intake measure (n 85)
Data extraction and analysis
The key information from each study selected for review was extracted carefully by one researcher (R.V.) into a prepared evidence worksheet for comparison and quality assessment suggested by the American Dietetic Association guidelines( 34 ). The key information included title, year, author, study design, purpose, study population characteristics, study protocol, outcome variables and results. This information is summarised in Table 1.
Table 1 Summary table of studies included in the present systematic literature review and narrative description

Outcomes assessed
Relevant study outcomes to the review were those that reflected measures of food literacy (such as food knowledge, food skill and food behaviours) and dietary intake (such as dietary recalls, FFQ). Some of the studies considered for review focused on other food-related measures, such as social connectedness from community gardens/kitchens, acculturation or migration outcomes in changing dietary habits, and these studies were included only if they also investigated the outcomes of an aspect of food literacy on measures of dietary intake.
Quality assessment
According to the PRISMA checklist, risk of bias of methodological quality within each individual study was assessed by two independent researchers (R.V. and L.E.B.) using the American Dietetic Association Quality Criteria Checklist (QCC)( 34 ), see Table 2. The QCC is a tool that addresses scientific rigour and is commonly used to assess studies in the field of nutrition. The QCC includes ten criteria that assess the applicability to practice and scientific validity of each study. Through this tool, the quality attributes of each study were classified as positive, neutral or negative. The outcomes of the quality assessment are shown in Table 2.
Table 2 Quality assessment attributes for each study assessed using the Quality Criteria Checklist (QCC)
N/A, not applicable (due to cross-sectional design of study); NR, not reported.
*+, positive overall score: this overall score is given if criteria 2, 3, 6 and 7 of the QCC and one additional criterion have received a positive score. Ø, neutral overall score: this score is given if more criteria are met than for a negative overall score but an overall positive score is not reached. −, negative overall score: this score is given if six or more QCC criteria are not met.
Results
A total of 198 articles were retrieved from the six database searches. Of those studies, 147 did not qualify for further review as they were not relevant to the topic, did not incorporate adolescents, did not incorporate relevant outcome measures or were not an original research article (e.g. editorials). A full article review was conducted on the remaining fifty-one studies, after which an additional thirty-eight were excluded. Of those thirty-eight studies, eight were found not to be a study (i.e. describing an education intervention process or did not have evaluation measures) and thirty did not include a measure of food literacy or a dietary intake measure (see Fig. 1).
Summary of included studies
Table 1 provides a summary of each study included for the review. The studies were published between 1993 and 2013 and included ten cross-sectional studies( Reference Leal, de Oliveira and Rodrigues 5 , Reference Venter and Winterbach 35 – Reference Trexler and Sargent 43 ), two intervention studies( Reference Caraher, Seeley and Wu 44 , Reference Chapman, Toma and Tuveson 45 ) and one longitudinal cohort study( Reference Laska, Larson and Neumark-Sztainer 9 ). One of the cross-sectional studies( Reference Larson, Story and Eisenberg 38 ) was a part of the longitudinal cohort study( Reference Laska, Larson and Neumark-Sztainer 9 ). Six of the studies were conducted in the USA( Reference Laska, Larson and Neumark-Sztainer 9 , Reference Larson, Story and Eisenberg 38 – Reference Pirouznia 40 , Reference Trexler and Sargent 43 , Reference Chapman, Toma and Tuveson 45 ), four were conducted in Europe( Reference Leal, de Oliveira and Rodrigues 5 , Reference Tsartsali, Thompson and Jago 36 , Reference Osler and Hansen 42 , Reference Caraher, Seeley and Wu 44 ) and one each in Australia( Reference Gracey, Stanley and Burke 41 ), the Middle East (Iran)( Reference Mirmiran, Azadbakht and Azizi 37 ) and South Africa( Reference Venter and Winterbach 35 ). The number of participants ranged from seventy-two to 7669. The age range of adolescent participants was 10 to 19 years.
Questionnaires were used for data collection in all studies. None of the studies investigated all aspects of food literacy (knowledge, skills and behaviours); nine studies investigated the relationship between food knowledge and dietary intake( Reference Leal, de Oliveira and Rodrigues 5 , Reference Venter and Winterbach 35 – Reference Mirmiran, Azadbakht and Azizi 37 , Reference Pirouznia 40 – Reference Trexler and Sargent 43 , Reference Chapman, Toma and Tuveson 45 ), one study investigated the relationship between food skills (such as cooking) and dietary intake( Reference Caraher, Seeley and Wu 44 ) and four studies investigated the relationship between food behaviours (such as shopping or food preparation) and dietary intake( Reference Leal, de Oliveira and Rodrigues 5 , Reference Laska, Larson and Neumark-Sztainer 9 , Reference Larson, Story and Eisenberg 38 , Reference Huang, Kaur and McCarter 39 ). Only two studies investigated two of the three aspects of food literacy( Reference Leal, de Oliveira and Rodrigues 5 , Reference Caraher, Seeley and Wu 44 ). Dietary intake was measured by FFQ( Reference Laska, Larson and Neumark-Sztainer 9 , Reference Tsartsali, Thompson and Jago 36 – Reference Larson, Story and Eisenberg 38 ), 24 h dietary recalls( Reference Trexler and Sargent 43 , Reference Chapman, Toma and Tuveson 45 ), KIDMED index scores( Reference Leal, de Oliveira and Rodrigues 5 , Reference Tsartsali, Thompson and Jago 36 ) and other questionnaires( Reference Venter and Winterbach 35 , Reference Huang, Kaur and McCarter 39 – Reference Osler and Hansen 42 , Reference Caraher, Seeley and Wu 44 ).
The outcomes of the quality assessment are shown in Table 2. Eleven studies were assessed to have a positive quality rating, one study received a neutral rating and one study received a negative rating. Due to most studies utilising a cross-sectional design, some parts of the assessment checklist were not applicable and the checklist was modified in order to optimally evaluate the quality of cross-sectional studies. For these studies, the criteria about comparable groups were not applicable, and the criterion about describing the intervention protocol was modified to ‘description of data collection procedures’. The main reasons for not achieving a positive quality rating were most often linked to omissions in the write-up of the manuscript such as participant selection and blinding processes and withdrawals/dropouts or response rates of participants.
The relationship between aspects of food literacy was examined in three broad approaches: (i) relationship between food knowledge and dietary intake; (ii) relationship between food skills and dietary intake; and (iii) the relationship between food behaviours and dietary intake.
Food knowledge
Of the nine studies that investigated the relationship between food knowledge and dietary intake, six studies showed a positive impact of knowledge( Reference Leal, de Oliveira and Rodrigues 5 , Reference Venter and Winterbach 35 , Reference Tsartsali, Thompson and Jago 36 , Reference Pirouznia 40 – Reference Osler and Hansen 42 ), one study showed a negative impact of knowledge( Reference Mirmiran, Azadbakht and Azizi 37 ) and two studies were not able to identify a clear relationship between food knowledge and dietary intake( Reference Trexler and Sargent 43 , Reference Chapman, Toma and Tuveson 45 ). More specifically, adolescents with greater food knowledge were shown to follow healthier dietary practices( Reference Osler and Hansen 42 ) and ate a larger variety of foods( Reference Gracey, Stanley and Burke 41 ). In addition, adolescents with greater cooking knowledge followed healthier dietary practices( Reference Leal, de Oliveira and Rodrigues 5 ). Interestingly, two studies reported mixed findings, such as reduced fat intake but increased carbohydrate intake( Reference Chapman, Toma and Tuveson 45 ); and an association for sodium knowledge and intake, but not other nutrients( Reference Trexler and Sargent 43 ). Only one study found a weak, non-significant association between food knowledge and dietary behaviours, whereby adolescents with good nutrition knowledge had similar dietary practices compared with other participants( Reference Mirmiran, Azadbakht and Azizi 37 ). Four studies revealed that females had greater food knowledge than males( Reference Venter and Winterbach 35 , Reference Mirmiran, Azadbakht and Azizi 37 , Reference Pirouznia 40 , Reference Gracey, Stanley and Burke 41 ). Surprisingly, one study found that females had greater food knowledge but poorer dietary practices compared with males( Reference Mirmiran, Azadbakht and Azizi 37 ).
Food skills
Only one study investigated the relationship between food skills and dietary intake( Reference Caraher, Seeley and Wu 44 ). That intervention study found that after participating in a school-based cooking programme, adolescents enjoyed tasting new foods, making new dishes and learning new cooking skills( Reference Caraher, Seeley and Wu 44 ). Following the intervention, participants reported an increase in their food skills such as cutting fruits and vegetables, following recipes, measuring ingredients and preparing foods. Cooking confidence of adolescents increased significantly, as did vegetable consumption( Reference Caraher, Seeley and Wu 44 ).
Food behaviours
Of the four studies that investigated the relationship between food behaviour and dietary intake, two studies found a positive impact of food preparation behaviours( Reference Leal, de Oliveira and Rodrigues 5 , Reference Laska, Larson and Neumark-Sztainer 9 ), one study found a variable impact of food behaviours( Reference Larson, Story and Eisenberg 38 ) and one study found no impact of food behaviours on dietary intake( Reference Huang, Kaur and McCarter 39 ). Specifically, one study found that frequent cooking was associated with healthier dietary practices( Reference Leal, de Oliveira and Rodrigues 5 ). Similar findings were observed in the longitudinal cohort study by Laska et al., which revealed that food preparation behaviours track over time( Reference Laska, Larson and Neumark-Sztainer 9 ). Adolescents who assisted to prepare dinner were more likely to engage in food preparation-related behaviours as emerging adults (19–23 years old) such as buying fresh vegetables, writing grocery lists and preparing dinner with chicken, fish or vegetables( Reference Laska, Larson and Neumark-Sztainer 9 ). Likewise, helping to prepare food for dinner was associated with increased enjoyment of cooking ten years later( Reference Laska, Larson and Neumark-Sztainer 9 ). Interestingly, one study found that more frequent food preparation was associated with increased fruit consumption in male adolescents and increased fruit and vegetable consumption in female adolescents, and was also negatively associated with unhealthy food choices, including soft drink consumption in females and fried food consumption among male adolescents( Reference Larson, Story and Eisenberg 38 ). Only one study did not find any relationship between food behaviours and dietary intake, and specifically found that frequency of reading food labels was not associated with dietary intake( Reference Huang, Kaur and McCarter 39 ). Interestingly, three studies found that female adolescents were more involved in food-related tasks and read food labels more frequently compared with male adolescents( Reference Laska, Larson and Neumark-Sztainer 9 , Reference Larson, Story and Eisenberg 38 , Reference Huang, Kaur and McCarter 39 ).
Discussion
The present systematic review investigated the association between food literacy and the dietary intake of adolescents. Overall, the evidence from the review suggests that food literacy may play a role in shaping youth eating behaviours( Reference Leal, de Oliveira and Rodrigues 5 , Reference Laska, Larson and Neumark-Sztainer 9 , Reference Venter and Winterbach 35 , Reference Tsartsali, Thompson and Jago 36 , Reference Pirouznia 40 – Reference Osler and Hansen 42 , Reference Caraher, Seeley and Wu 44 ). In addition, findings suggest that food skills and behaviours learned in adolescence are sustained later in life( Reference Laska, Larson and Neumark-Sztainer 9 ). For example, Laska et al.’s longitudinal study found that adolescents who assisted in preparing dinner were more likely to engage in food preparation behaviours five years later( Reference Laska, Larson and Neumark-Sztainer 9 ). However, the study quality, tools utilised for collecting data and measured aspects of food literacy should be acknowledged when interpreting the findings of the systematic review.
The studies in the systematic review incorporated a variety of methodological approaches to their study design. The lack of randomised controlled trials and emphasis on cross-sectional studies reduces the ability to clarify the strength and nature of the association between aspects of food literacy and dietary intake. Furthermore, most of the studies used tools that were developed for the specific investigation being reported and did not incorporate validated tools to measure aspects of food literacy( Reference Tsartsali, Thompson and Jago 36 , Reference Huang, Kaur and McCarter 39 , Reference Gracey, Stanley and Burke 41 – Reference Trexler and Sargent 43 ). For food literacy to become established as an important concept in understanding the complex relationships between food knowledge, skills and behaviours and dietary choices, instruments that encompass the identified aspects of food literacy must be developed and validated. Also, none of the studies incorporated a holistic and comprehensive tool to measure food literacy. Rather, studies measured only one or two aspects of food literacy. For example, Osler and Hansen’s study measured food knowledge and dietary intake of Dutch adolescents( Reference Osler and Hansen 42 ) and Caraher et al. investigated the impact of a cooking programme with a chef on adolescents’ vegetable consumption and food preparation skills( Reference Caraher, Seeley and Wu 44 ). This suggests that further research is required to develop comprehensive, validated tools for measuring food literacy in order to increase the strength of future research in this area.
The quality of the studies included in the review should be considered when interpreting their findings. Although most of the studies received a positive overall quality rating( Reference Leal, de Oliveira and Rodrigues 5 , Reference Laska, Larson and Neumark-Sztainer 9 , Reference Venter and Winterbach 35 , Reference Tsartsali, Thompson and Jago 36 , Reference Larson, Story and Eisenberg 38 , Reference Pirouznia 40 – Reference Chapman, Toma and Tuveson 45 ), it should be acknowledged that the QCC quality assessment checklist was modified appropriately to assess the studies that utilised a cross-sectional study design. Seven studies did not describe the participant withdrawals/dropouts or response rate in their studies( Reference Mirmiran, Azadbakht and Azizi 37 – Reference Gracey, Stanley and Burke 41 , Reference Trexler and Sargent 43 , Reference Chapman, Toma and Tuveson 45 ); and neither of the intervention studies described the blinding procedures utilised to prevent the possibility of measurement bias( Reference Caraher, Seeley and Wu 44 , Reference Chapman, Toma and Tuveson 45 ). These attributes of the study limit confidence in determining the extent of the association between food literacy and dietary intake. Nevertheless, it should be noted that Caraher et al.’s cooking intervention study received a positive overall quality rating and also found a positive relationship between food literacy and dietary intake( Reference Caraher, Seeley and Wu 44 ). In addition, the two studies that reported no significant impact of aspects of food literacy on dietary intake received neutral and negative overall quality ratings( Reference Mirmiran, Azadbakht and Azizi 37 , Reference Huang, Kaur and McCarter 39 ). There is clearly a need for more rigorous research to effectively assess the causality between food literacy and adolescents’ dietary intake in order to confirm the extent of the relationship.
None of the reviewed studies utilised the term ‘food literacy’ in their description of the study outcomes. This is likely due to food literacy being a relatively new concept and only recently defined( Reference Vidgen and Gallegos 17 ). While broadly defined food literacy encompasses food knowledge, skills and behaviours, almost all studies investigated a specific aspect of food literacy, with most of them using food knowledge as a proxy of food literacy( Reference Leal, de Oliveira and Rodrigues 5 , Reference Vidgen and Gallegos 17 , Reference Venter and Winterbach 35 – Reference Mirmiran, Azadbakht and Azizi 37 , Reference Pirouznia 40 – Reference Trexler and Sargent 43 , Reference Chapman, Toma and Tuveson 45 ). Previous interventions for addressing adolescent overweight and obesity aimed to increase food knowledge of adolescents as the best public health strategy( Reference Micucci, Thomas and Vohra 15 ); however, this narrow focus may offer an explanation why many interventions up to date have displayed minimal or modest outcomes in reducing the prevalence of adolescent overweight and obesity. The present systematic review highlights the possible positive influence of food skills and behaviours on adolescents’ dietary intake. For example, Caraher et al.’s study reported an increase in vegetable consumption of adolescents after the cooking programme with a chef( Reference Caraher, Seeley and Wu 44 ). However, these studies require further support from future research, as only one study has investigated the impact of food skills on dietary intake and only four studies have investigated the impact of food behaviours on adolescents’ dietary intake( Reference Leal, de Oliveira and Rodrigues 5 , Reference Laska, Larson and Neumark-Sztainer 9 , Reference Larson, Story and Eisenberg 38 , Reference Huang, Kaur and McCarter 39 , Reference Caraher, Seeley and Wu 44 ).
The present systematic review highlights the opportunities for future research. First, as most of the studies employed a cross-sectional study design, it is currently not possible to clarify any causal contributions of food literacy on adolescents’ dietary behaviours. Therefore, future research should consider a longitudinal approach to be able to investigate the potential causal contribution of food literacy on adolescents’ dietary intake. Second, there are opportunities for future research to develop validated tools that comprehensively measure food literacy. These tools would enhance the comparability of findings between studies and subsequently increase the confidence in interpreting findings of the body of research in this area. Finally, there is an opportunity to investigate which aspects of food literacy are critical for improving adolescents’ dietary intake, including possible differences in male and female adolescents. There is currently a lack of evidence about the impact of food skills and behaviours on adolescents’ dietary intake. Investigating the relative influence of the components of food literacy may further inform the development of public health policies that aim to address adolescent overweight and obesity.
One of the main strengths for the present review is the systematic nature of its methodology that differs from a traditional review in which previous work is described but not systematically identified, assessed for quality and synthesised( Reference Glasziou 46 ). Introduction of bias was minimised by independent researchers using the same data extraction worksheet for each individual study and quality assessment checklist. The systematic review used six databases, which afford broad coverage of allied health, including nutrition and public health, literature. Although there are some inconsistencies in the findings of the studies, the existing research has important implications for public health practitioners and policy makers. Overall, the findings suggest that there is an influence of food literacy on dietary intake and that increasing food literacy in adolescence may be an appropriate public health strategy to address the growing prevalence of adolescent overweight and obesity.
Limitations
The present systematic review is subject to two notable limitations. First, it was challenging to compare the findings of reviewed studies due to differences in study designs, data collection methods and participant samples. The bias of this limitation was minimised through the use of the same evidence worksheet for each individual study. In addition, the studies were grouped in accordance with the food literacy definition matrix, which helped to identify major themes and report the findings. Second, most of the evidence on the impact of aspects of food literacy on dietary intake is based on self-reported data, which may influence the reporting of actual food skills capabilities( Reference Caraher, Seeley and Wu 44 ) and dietary intake by participants and reduces confidence in study outcomes. Some participants may have reported inaccurate information, responded in a socially desirable way or their answers may be subject to recall error( Reference Brener, Billy and Grady 47 ). Recognising these limitations, it is equally important to acknowledge that self-report data on food consumption have been shown to be as reliable as more formal 24 h dietary recall assessment( Reference Brener, Billy and Grady 47 ).
Conclusions
The present systematic review found that food literacy may influence adolescents’ dietary intake. It is apparent there is a lack of research that has measured all aspects of food literacy over time or longitudinally to determine the strength and nature of the association with dietary intake. The review identifies the need for rigorous research methods to attain a greater understanding of the influence of food literacy on dietary intake. The systematic review suggests that improving food literacy in adolescence may improve individuals’ food skills and healthier dietary behaviours. The evidence recommends public health promotion practitioners and policy makers to consider new public health strategies that focus on increasing food literacy in adolescence.
Acknowledgements
Financial support: This research received no specific grant from any funding agency in the public, commercial or not for-profit sectors. The study did not receive any specific non-financial support. Conflict of interest: None. Authorship: R.V. performed the original search and supported data extraction. R.V., L.E.B. and N.H. completed data extraction and quality ratings, and drafted the manuscript. L.E.B. and N.H. provided analytical support to the manuscript. Ethics of human subject participation: Ethical approval was not required because the paper was a systematic review and the findings of existing studies were available in the public domain.



