



Excess weight, classified as either overweight or obesity, can be understood as a multifactorial problem caused by a positive energy balance, resulting from an imbalance between food intake and energetic expenditure, which favours the accumulation of fat(1).
The prevalence of overweight people in the world increased around 10 % between 1980 and 2013(Reference Ng, Fleming and Robinson2). The occurrence of this event has been observed in most countries, including those considered to be developed, and can be described as a pandemic. Therefore, it can be seen that excess weight is diffuse and constitutes a challenge for public health worldwide(Reference Popkin3–Reference Mattar, Torloni and Betrán6).This health problem can increase the risk of chronic diseases, such as diabetes mellitus and cardiovascular disorders(5,Reference Pinheiro, Oliveira and Leal7–Reference Bhupathiraju and Hu9) .
Among theories that present the biological plausibility between obesity and diabetes, for example, it is suggested that the former can trigger changes in the individual’s metabolism through the inflammation. These changes induce adipose tissue to deposit fat molecules in the bloodstream, which can affect insulin-responsive cells and generate insulin resistance. Obesity produces a variety of structural and functional cardiovascular changes. Indirectly, it can also influence coronary risk resulting from the action of related comorbidities, such as dyslipidaemia, hypertension and endothelial dysfunction(Reference Bhupathiraju and Hu9–Reference Wilson, D’Agostino and Sullivan11).
Recently, in Brazil, this event has grown steadily, as it occurs in different age groups, in both sexes and in regions with different levels of socio-economic development. However, it has been observed that the increase in obesity is higher among women. The prevalence of overweight and obesity was assessed to be 48 and 16·9 %, respectively, of adult Brazilian women in 2006, being higher in the lower income strata population groups and with an increasing trend, according to age and parity(12,13) .
In an official survey carried out by the Brazilian Institute of Geography and Statistics (IBGE), between 2008 and 2009, the prevalence of obesity was 16·9 % among women(14). In previous periods, in the 1970s, for example, obesity was present in only 8 % of women(15). This phenomenon is probably due to the rapid nutritional transition that has occurred in Brazil, characterised by the reduction of cases of classic malnutrition and an elevation of excess weight, resulting from changes in the population’s lifestyle, such as in dietary patterns and a reduction in daily energy spending(Reference Popkin3–Reference Mattar, Torloni and Betrán6).
Moreover, it is known that excess weight can generate adverse effects, specifically, for the health of women of reproductive age, from 10–49 years, since it can cause changes, such as irregular menstruation, infertility and polycystic ovary syndrome(Reference Pinheiro, Oliveira and Leal7,Reference Rosa, Silva and Giroldi16,Reference Sacomori, Cardoso and Souza17) . This increase in the prevalence of excess weight also affects unfavourable gestational outcomes, such as prematurity and/or low birth weight. Additionally, it leads to a higher risk of morbidity in the child’s first year of life(Reference Siega-Riz, Viswanathan and Moos18).
Thereby, studies that investigate the hypothesis of an association between socio-demographic factors, living conditions and obesity/overweight in women of childbearing age are justified, especially in countries with a lack of information on the topic. The objective of the current study was to evaluate the factors associated with excess weight (overweight and obese) in Brazilian women of childbearing age.
Method
Study design and context
A cross-sectional study was developed using database from the National Health Survey (PNS), from the year 2013. The National Health Survey is an epidemiological population-based study, representative of Brazil, that was developed by three institutions: the Ministry of Health, the Oswaldo Cruz Foundation (Fiocruz) and the Brazilian Institute of Geography and Statistics (IBGE).
The PNS sample was composed of clusters in three stages. First, the census sectors were selected, with probability proportional to the size of the subsample of the Primary Sampling Units (UPA), in each of its strata. In the second, households were selected by simple random sampling. In the third, a resident of 18 years or older was included from each household, selected with equal probability among all eligible residents.
The estimated sample was 63 900 households, considering a 20 % non-response rate and 95 % confidence level. In total, 81 167 households were visited, of which 69 994 were occupied, with 60 202 individual interviews with the selected resident at home. Losses were considered: closed or empty household; refusal of residents to meet the interviewer; not being able to interview the informant, after 3 or more attempts, even with the scheduling of visits. For the present study, the sample comprised all women interviewed in the age group of 18–49 years: 17 109 participants.
Participants
Women of reproductive age (18–49 years) were included in the research. Exclusion criteria were applied: pregnant women and not being the ‘proxy-respondent’ at the time of the interview. The research was approved by the National Health Council, under CAAE protocol: 10853812·7·0000·0008 according to laws 466/2012 and 580/2012. All participants signed an informed consent form, and participation in the study was voluntary.
Investigated variables
The dependent variables included overweight and obesity, which represent excess weight. For that, the BMI of each participant was calculated using the weight and height data(1). Thereby, normal weight was considered to be when the BMI presented between 18·50 and 24·99 kg/m2; overweight showed a BMI value from 25·00 to 29·90 kg/m² and obesity with values of BMI ≥ 30·00 kg/m².
The investigation of factors associated with overweight and obesity was carried out based on the theoretical–conceptual model regarding the topic. The independent variables included socio-economic and demographic factors, health history and lifestyle characteristics. The socio-economic and demographic factors analysed were age (18–25, 26–33, 34–41 and 42–49 years), race/skin colour (white or non-white), region (north, northeast, midwest, south and southeast), marital status (with partner or without partner), education level (measured in years of study and categorised in ≤ 8 years of study – low education level; or > 8 years of study – medium to high education level), employment (yes or no) and family income (> 2 minimum wages, > 1 and up to 2 minimum wages and up to 1 minimum wage. Minimum wage value at the time of data collection: R$ 678,00 – equivalent to US $ 287·65 in the year 2013).
Concerning health history, presence or not of diagnoses of hypertension, diabetes mellitus, high cholesterol, heart attack, stroke, chronic kidney disease and depression were evaluated. Menarche (before or from 12 years) and parity (primiparous or multiparous) were also investigated. For lifestyle information (yes or no) on self-reported health status, alcoholic beverage consumption, smoking and physical activity were included. Physical activity defined as at least 150 min of light or moderate physical activity, or at least 75 min of vigorous leisure physical activity per week. The abusive consumption of alcoholic beverages is defined as the ingestion of four or more doses, in a single occasion, in the last 30 d. A dose of alcoholic beverage is equivalent to a can of beer, a glass of wine or a dose of cachaça, whiskey or any other distilled alcoholic drink. Smoking habit is defined as the use of tobacco products that emit or not smoke, regardless of the amount consumed, frequency and duration.
Statistical methods
Descriptive statistics of the variables were obtained, and the prevalence of the outcome was calculated. To identify the factors associated with excess weight, this group of women was compared to those with normal weight. Poisson regression analysis was used, adopting the prevalence ratio (PR) and the respective 95 % CI.
The selection of adjusted variables was performed based on a theoretical–conceptual model of association between exposures factors and the outcomes, overweight and obesity. Two adjustment models were used. In model 1, the adjustment was made only by age. In the adjusted model 2, the selected variables were age, family income, hypertension and diabetes mellitus. Specific procedures were used in the data analysis, using weighting to correct the sample design with the definition of weights, strata and unit samples. Data analysis was performed using STATA® software version 15.0, serial number: 401506208261.
Results
For the current study, 17 109 participants were included. These women had an average age of 34·39 (sd 0·07) years, a minimum age of 18 years and a maximum of 49 years. Of these, 33·26 % presented as overweight and 21·94 % showed obesity, giving a total of 55·20 % of women with excess weight. The comparison group, normal weight, was identified in 44·80 % of the women.
The results of the adjusted association measurements between the independent variables and excess weight showed that advanced age, having a partner, family income ≤ two minimum wages, hypertension, diabetes mellitus, high cholesterol, menarche before 12 years of age, regular or poor state of health and smoking habit showed a statistically significant association for both the overweight and obesity groups (Tables 1–4).
Table 1 Socio-economic and demographic factors, according to overweight women, Brazil, 2013
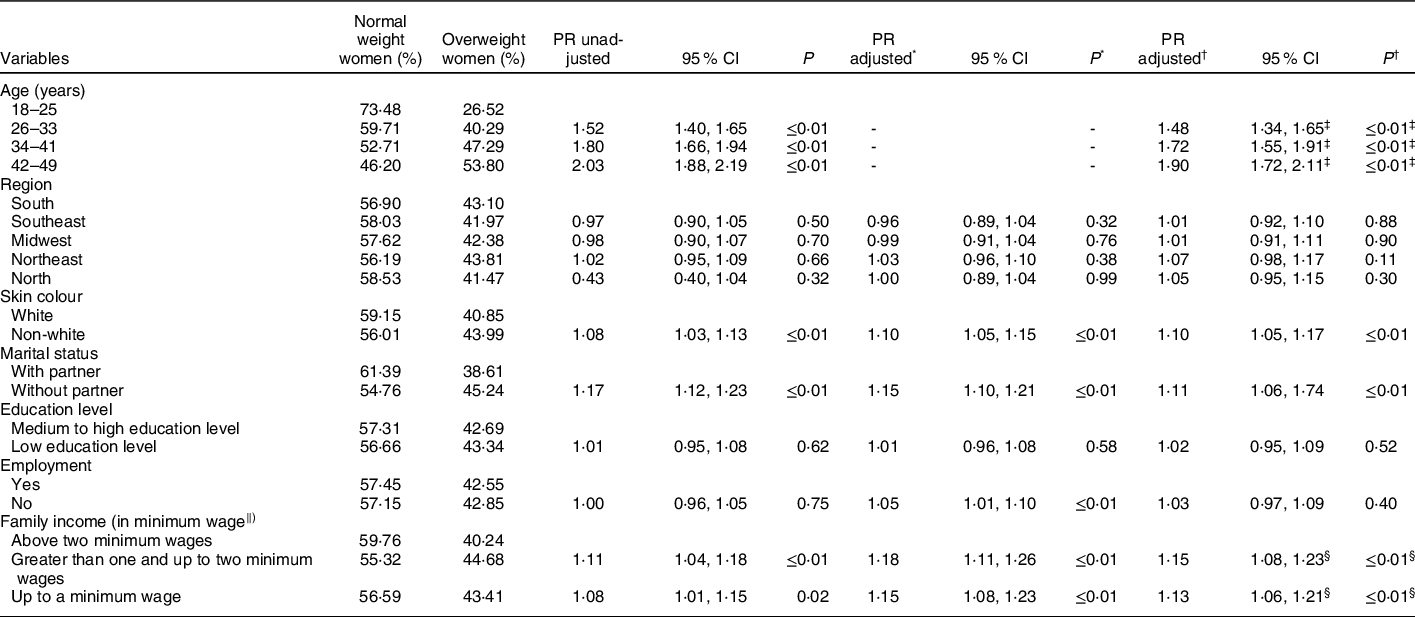
PR, prevalence ratio.
* Model 1 – adjusted for age.
† Model 2 – adjusted for age, family income, hypertension and diabetes mellitus.
‡ Model 2 – adjusted for family income, hypertension and diabetes mellitus.
§ Model 2 – Adjusted for age, hypertension and diabetes mellitus.
‖ Minimum wage value at the time of data collection: R$ 678,00 (equivalent to US $ 287.65 in the year 2013).
Table 2 Factors related to the health and lifestyle conditions, according to overweight women, Brazil, 2013

PR, prevalence ratio.
* Model 1 – adjusted for age.
† Model 2 – adjusted for age, family income, hypertension and diabetes mellitus.
‡ Model 2 – adjusted for age, family income and diabetes mellitus.
§ Model 2 – adjusted for age, family income and hypertension.
Table 3 Socio-economic and demographic factors of women, according to obesity, Brazil, 2013
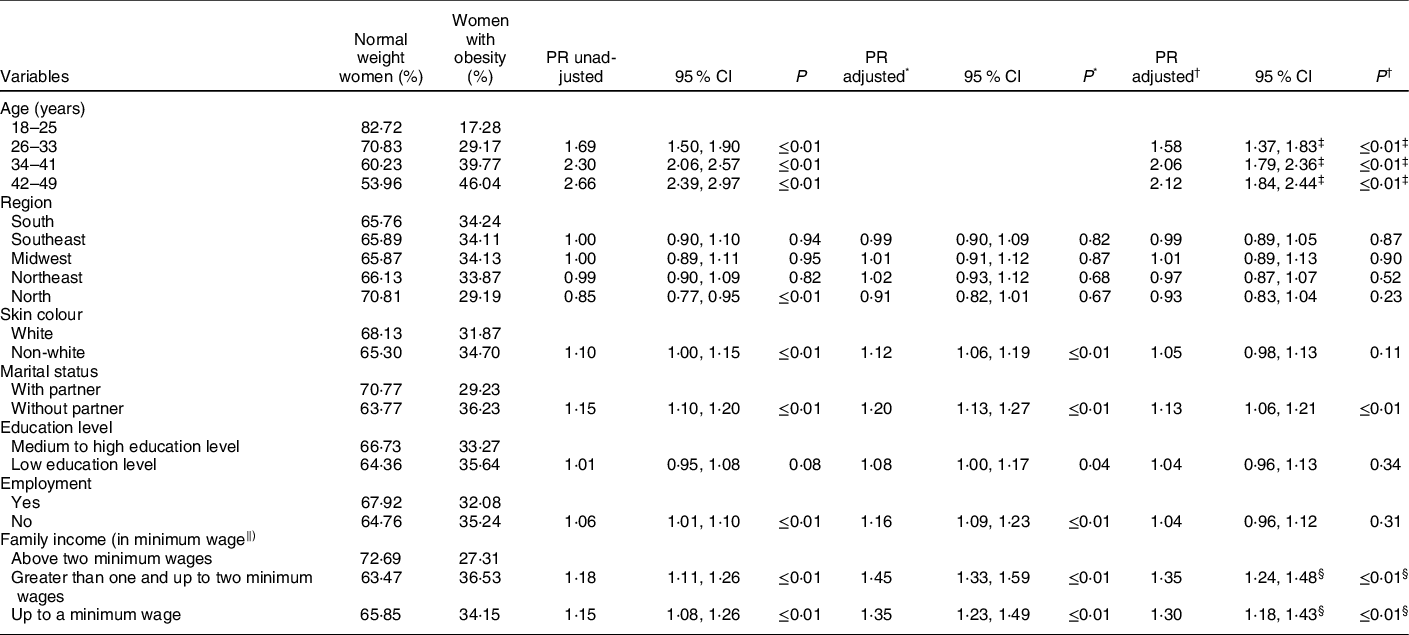
PR, prevalence ratio.
* Model 1 – adjusted for age.
† Model 2 – adjusted for age, family income, hypertension and diabetes mellitus.
‡ Model 2 – adjusted for family income, hypertension and diabetes mellitus.
§ Model 2 – adjusted for age, hypertension and diabetes mellitus.
‖ Minimum wage value at the time of data collection: R$ 678,00 (equivalent to US $ 287.65 in the year 2013).
Table 4 Factors related to the health and lifestyle conditions of women, according to obesity, Brazil, 2013
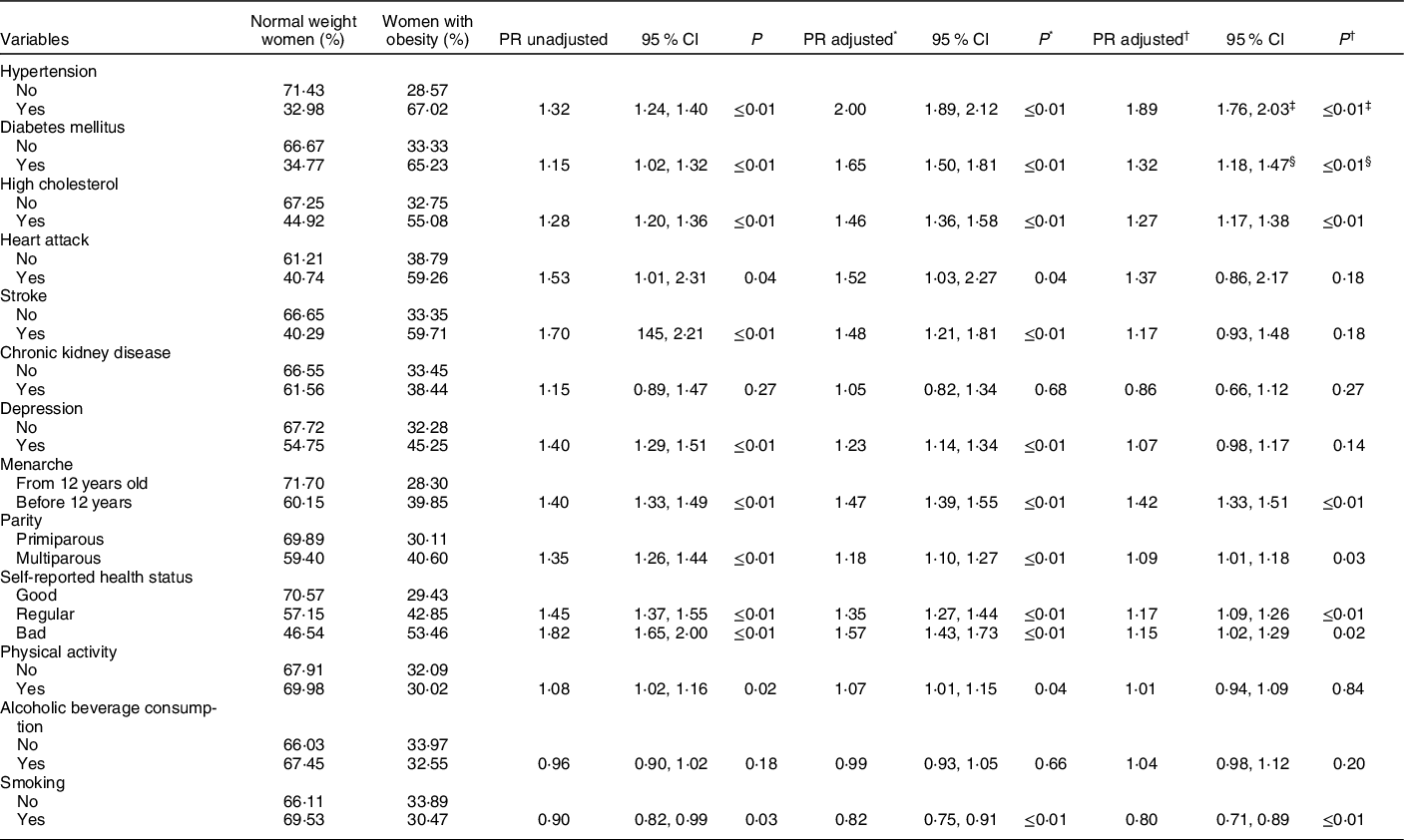
PR, prevalence ratio.
* Model 1 – adjusted for age.
† Model 2 – adjusted for age, family income, hypertension and diabetes mellitus.
‡ Model 2 – adjusted for age, family income and diabetes mellitus.
§ Model 2 – adjusted for age, family income and hypertension.
The magnitude of the association between the independent variables and excess weight was greater for the adjusted model 1, only for age. When this model was added to other adjusted variables, model 2, the association measurement showed a slight reduction. In addition, the magnitude of the association was, generally, higher for factors associated with obesity. For example, variable hypertension showed an association measurement of 1·89 with obesity, while for being overweight, this association measurement was 1·28.
Thus, having hypertension was two times more prevalent in the adjusted model 1 (PR adjusted = 2·00; 95 % CI 1·89, 2·12) among women with obesity, showing a slight reduction to 1·89 times with the employment of adjusted model 2 (PR adjusted = 1·89; 95 % CI 1·76, 2·03). In overweight women, hypertension was 32 % more frequent in the adjusted model 1 (PR adjusted = 1·32; 95 % CI 1·24, 1·39), with a slight decrease to 28 % with the adjustment of model 2 (PR adjusted = 1·28; 95 % CI 1·20, 1·37).
The association measurements of the age variable, distributed according to the age group, showed that the greater the age group, the greater the strength of association, in both weight groups, suggesting a ‘dose–response’ effect. The magnitude of the association augmented as the age group increased with the use of the adjusted model 2 (Tables 1 and 3).
It is worth noting that the independent variables race/skin colour non-white and consuming alcoholic beverages at least once a month were associated, with overweight women only, in the adjusted model 2, whereas being multiparous was also associated but only with obesity. As for the practice of physical activity, this variable showed a statistically significant association between women with obesity but only for the adjusted model 1.
Discussion
The main findings showed an association between the following factors and excess weight in Brazilian women of childbearing age: advanced age groups, having a partner, family income less than or equal to two minimum wages, hypertension, diabetes mellitus, high cholesterol, menarche before the age of 12, regular or poor health and smoking habit. Race/skin colour non-white and alcoholic beverage consumption at least once a month were factors associated with overweight women, whereas being multiparous and practicing physical activity were associated only with obesity.
Among the important findings, the prevalence of 55·2 % of excess weight in Brazilian women of childbearing age stands out in 2013, showing itself to be higher than the world estimate in the same period of 38·0 %(Reference Ng, Fleming and Robinson2). The low global prevalence, compared with Brazil, may be because, in some countries, mainly those with low socio-economic development indicators, there is a greater prevalence of low weight, thus reducing the global obesity estimate(Reference Vilella-Nebot, Abacassamo and Gómez-Olivé19). However, countries with population characteristics like those in Brazil presented a similar prevalence(Reference Sotoudeh, Khosravi and Khajehnasiri20–Reference Navarro Nuñez, Venegas Ochoa and Navarro Solares22).
The strength of association with excess weight was greater in the eldest age group. The ‘dose–response’ effect is consistent with previous studies and demonstrates a direct relationship between weight gain and the woman’s age(Reference Pinheiro, Oliveira and Leal7,Reference Rosa, Silva and Giroldi16,Reference Franke, Wichmann and Prá23,Reference Chooi, Ding and Magkos24) . This occurs mainly because of the ageing process, which triggers several physiological changes in individuals, such as the loss of muscle mass and strength associated with sarcopenia(Reference Marques, Ferreira Freitas and Araújo Veloso Popoff25–Reference Diniz, Gonçalves and Parreira27), which decreases functional performance and, consequently, reduces the frequency of physical activity and increases body weight(Reference Delacosta28,Reference Santos, Araujo and Cardoso29) .
The factor associated with family income less than or equal to two minimum wages and excess weight can be understood as a consequence of the less privileged social situation of women, which influences not only home access to food but also nutritional education and a diet poor in nutrients and, in general, hyperenergetic. These findings are in agreement with previous studies(Reference Lemamsha, Randhawa and Papadopoulos21,Reference Navarro Nuñez, Venegas Ochoa and Navarro Solares22) .
The conditions of having a partner and being multiparous were factors positively associated with obesity; similar results have been found in other studies(Reference Correia, da Silveira and Silva30,Reference Gigante, Moura and Sardinha31) . It is probably a consequence of being less concerned with body image, due to marriage and greater dedication to caring for children and the home(Reference Correia, da Silveira and Silva30,Reference Pinto, Griep and Rotenberg32,Reference Pinto, Menezes and Griep33) . Thus, the woman is not able to routinely practice physical activity and does not have an adequate diet, resulting in weight gain(Reference Correia, da Silveira and Silva30). It is worth noting that there is a need to better share household chores among family members in order to provide for an increase in women’s quality of life(Reference Lima, Lessa and Santos34).
Menarche before the age of 12 represented a factor positively associated with excess weight, corroborating other studies(Reference Pinheiro, Oliveira and Leal7,Reference Correia, da Silveira and Silva30,Reference Costa, Moreira and Florêncio35,Reference Dreyfus, Jacobs and Mueller36) . A study with 400 Indian women, signaled that the majority with early menarche had, showed higher adiposity markers such as BMI, waist hip ratio, waist height ratio and waist circumference. Based on this, these authors recommended that there is a need to focus attention on females with higher adiposity markers as it may trigger early menarche and reports on early matured females were found to associate with several risk factors(Reference Devi, Dhall and Kapoor37). Based on this, there is a need for more attention focused on overweight and obese girls, since this condition can favour early menarche, which is associated with health problems, such as cardiometabolic risk(Reference Dreyfus, Jacobs and Mueller36,Reference Werneck, Oyeyemi and Cyrino38) .
When analysing the health history of these women, it was observed that the existence of morbidities (diabetes mellitus, hypertension and high cholesterol) is more frequent among women with excess weight. It is known that being overweight and obesity are factors that predispose to the development of numerous metabolic and functional disorders, agreeing with previous investigations(Reference Salve39–Reference Souza41).
Excess weight was also associated with poor and regular self-reported health status, similar to other studies(Reference Gigante, Moura and Sardinha31,Reference Reesor, Canales and Alonso42,Reference Batsis, Whiteman and Lohman43) . Women who have negative self-perceived health, in general, affected by diseases that can be influenced by being excess weight(Reference Salve39).
In relation to lifestyle, smoking showed an inverse association with obesity, corroborating other studies(Reference Castanheira, Olinto and Gigante44,Reference Lino, Muniz and Siqueira45) . The mechanism of this inverse association is not fully known. However, there is evidence that the nicotine present in tobacco induces a feeling of satiety through the greater activity of leptin, known as the satiety hormone, which induces the reduction of neuropeptide Y, responsible for increased appetite(Reference Chatkin and Chatkin46). However, it is noteworthy that the harmful effects of tobacco are superior to the benefits of weight reduction that it provides(Reference Radzeviciene and Ostrauskas47,Reference Balachova, Zander and Bonner48) .
As for the factor associated with non-white skin colour and excess weight, it may have occurred due to historical, social, political and economic reasons. Black people often have fewer financial resources(Reference Gigante, Moura and Sardinha31,Reference Pinto, Griep and Rotenberg32) , limiting the choice of diet to the categories of foods considered most affordable and often very energetic(Reference Franke, Wichmann and Prá23,Reference Lima, Lessa and Santos34) . The socio-economic status has traditionally been indicated as a mediator of the relationship between skin colour and excess weight(Reference Daubenmier, Chao and Hartogensis49,Reference Dinsa, Goryakin and Fumagalli50) . However, this association cannot be explained only by the low socio-economic level, but it can also be a consequence of racism, which can generate stress for black individuals, contributing to the elevation of overweight markers(Reference Araujo, Baltar and Yokoo51–Reference Gee, Ro and Gavin54).
The biological plausibility that explains how racial discrimination influences the weight of black individuals is supported by the theory that substances released by stressful situations can affect the homoeostasis of hormone production such as cortisol and insulin, favouring the accumulation of adipose tissue(Reference Tomiyama55,Reference Hewagalamulage, Lee and Clarke56) .
The interpretation of the findings must consider the limitation of the cross-sectional study, such as the impossibility of inferring the causality between the studied variables. In addition, some of the information was self-reported. The fact that the participant might not have felt comfortable in answering the questions honestly at the time of the interviews may have resulted in information bias. In epidemiological surveys with large samples, self-reported information is common, not invalidating the quality of the findings(Reference Kim57,Reference Mindell, Biddulph and Hirani58) . The National Health Survey aimed to collect information on the performance of the national health system with regard to access and use of available services and continuity of care, as well as on the health conditions of the population, surveillance of chronic diseases non-communicable diseases and the associated risk factors.
However, the current study certainly has some strengths. For example, the anthropometric measurements and blood biomarkers collected in each participants using physical and laboratory tests. Moreover, the large sample size and the weighting strategy for complex samples, which made the findings more reliable, reflected in the narrow confidence intervals; its representativeness of the population of Brazilian women of childbearing age the generalisation of the findings, that is, it is possible to extrapolate these results to places with characteristics similar to that of Brazil. Another strength was the technique employed for data analysis, using an adjusted model, and weighting for complex samples.
Conclusion
Excess weight in Brazilian women of childbearing age was shown to be associated with biological factors, social aspects, and reproductive and health history. The results point to the need for interventions that promote the reduction of excess weight in women.
Acknowledgements
Acknowledgements: None. Financial support: Research carried out by the Brazilian Institute of Geography and Statistics (IBGE), Health Ministry and Oswaldo Cruz Foundation (Fiocruz). Conflict of interest: There are no conflicts of interest. Authorship: A.O.L., E.S.S., S.d.S.C., J.E.T.B., and S.M.B. contributed to the formulation of the question under investigation, the conception of the study, design, data acquisition, drafting and critical revision of the manuscript. S.S.d.C., I.S.G.-F. and A.C.M.G.F. contributed to the analysis, interpretation and critical revision of the manuscript. All authors gave final approval and agreed to be accountable for all aspects of the manuscript. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the National Health Council (CAAE protocol: 10853812.7.0000.0008). Written informed consent was obtained from all subjects/patients.




