


The acquisition of healthy habits, especially those related to diet and physical activity, are greatly influenced by one’s environment, including political, cultural, social, demographic and economic factors( Reference Cutler, Flood and Hannan 1 , Reference Campbell and Hesketh 2 ). Education plays a fundamental role in the acquisition and development of knowledge about healthy behaviours, that will develop into healthy attitudes and therefore healthy habits( Reference Birch and Davison 3 ). This is especially important during early childhood, when behaviours are formed largely through the influence of the child’s immediate environment, which is mostly the family( Reference Campbell and Hesketh 2 , Reference dos Santos Barroso, Sichieri and Salles-Costa 4 ). Knowledge about basic nutrition is, for instance, one of the key influences on eating behaviours and therefore has been the target of many intervention strategies and policies( Reference Worsley 5 ). However, unhealthy behaviours are influenced only weakly by interventions that focus on a single factor and overall improvements in healthy lifestyle require more comprehensive interventions into the individual’s attitudes and habits. One of the best dietary patterns to follow given the scientific evidence supporting its cardioprotective effects is the Mediterranean diet( Reference Sotos-Prieto, Zulet and Corella 6 , Reference Estruch, Ros and Salas-Salvado 7 ).
Parents are usually the principal role model for their children and there is a strong parent–child association in terms of dietary habits( Reference Mitchell, Farrow and Haycraft 8 – Reference Lazarou, Kalavana and Matalas 11 ). However, a recent systematic review aimed at defining the degree of association between the dietary intake of children and that of their parents showed that the agreement is weak and varies considerably between studies( Reference Wang, Beydoun and Li 12 ). Dietary assessment in young children is challenging and most of the few studies conducted were based on parental reporting of their children’s habits( Reference Wang, Beydoun and Li 12 ). There are concerns about whether parental responses reflect accurately children’s behaviour or represent only an idealized view. Few studies have addressed this issue and analysed whether there is a genuine association between the dietary and physical activity habits of parents and their children, and even fewer studies have been conducted with children under 5 years of age( Reference dos Santos Barroso, Sichieri and Salles-Costa 4 , Reference Fisher, Mitchell and Smiciklas-Wright 13 – Reference Hu, Ye and Li 15 ).
Parental sociodemographic factors such as ethnicity or literacy seem to influence the ability of children to opt for healthy choices( Reference Cutler, Flood and Hannan 1 , Reference Garemo, Lenner and Nilsson 16 ). Many studies have shown that a low educational level in parents is linked to less healthy dietary habits in their children and to unhealthy behaviours in general( Reference Garemo, Lenner and Nilsson 16 – Reference Antonogeorgos, Panagiotakos and Grigoropoulou 19 ). The design of effective strategies for health promotion therefore requires an understanding of the determinants of healthy choices in children from a very early age.
The present study evaluated the dietary and physical activity habits of Spanish children aged 3–5 years, with the following specific aims: (i) to evaluate whether self-reported dietary and physical activity habits of children correspond to the assessment of these habits by the children’s parents; (ii) to study whether parents’ health-related behaviours and other characteristics are associated with those of their children; and (iii) to explore how children’s dietary and physical activity habits are influenced by parental educational level and income status.
Methods
Study design and population
Program SI! is an educational school intervention aimed at promoting cardiovascular health through the acquisition of healthy behaviours from early childhood. The efficacy of this intervention is currently being assessed through a cluster-randomized controlled trial of children aged 3–5 years and their parents, teachers and school environment, carried out in the city of Madrid, Spain, in a total of twenty-four schools (ClinicalTrials registration number: NCT01579708). With regard to the recruitment of schools, the trial is based on a hierarchical design where schools are the experimental units that receive the intervention and therefore are the units that are randomized to either intervention or control group. We randomized the schools using the percentage of immigration as a stratification factor with four levels (according to quartiles) to ensure that the groups were balanced with respect to differences in cultural background. From the total of seventy-three schools that were invited to participate, thirty-five agreed to participate and finally twenty-four were chosen, excluding larger schools with more than two classrooms per level in order to have a similar number of students in each school. The primary outcome of the trial is the 3-year change in markers of behavioural change, defined as knowledge, attitudes and habits (KAH) in four areas: (i) healthy diet; (ii) improved physical activity patterns; (iii) knowledge of the human body and heart; and (iv) management of emotions. The Program SI! is implemented in the classroom during four complete weeks within each of the three academic years (from 2011 to 2014). The detailed study protocol and the materials and strategies used for the intervention have been described elsewhere( Reference Peñalvo, Santos-Beneit and Sotos-Prieto 20 ). After a school year follow-up, results have recently been published showing changes in scores for KAH among children( Reference Penalvo, Sotos-Prieto and Santos-Beneit 21 ).
For the present study we used baseline data collected during October to November 2011 from children (3–5 years old, n 2062; 1021 girls, 1041 boys) and their parents (n 1949; 1519 women, 430 men). A cross-sectional design was adopted for the purpose of the present study.
The study was conducted in accordance with the Declaration of Helsinki and all procedures involving participants were approved by the Regional Committee for Clinical Research Ethics (CEIC-R) for the Madrid area. Informed written consent was required from the children’s parents or legal guardians. The document specifies the purpose of the intervention and evaluation study, as well as the various tests and measurements that are taken. Once parents or guardians had signed the informed consent, they and their child or children were formally included in the study. A data encryption system was used to guarantee confidentiality of the information provided. The information collected is managed according to Spanish Law 15/1999 for the Protection of Personal Data.
Questionnaires
Children’s dietary and physical activity assessment
Information about children’s habits was obtained through the Program SI! questionnaire, which assesses KAH in relation to diet and physical activity( Reference SitiSabariah, Zalilah and Norlijah 22 , Reference Cespedes, Briceno and Farkouh 23 ) (Table 1). This information was self-reported by the children with guided assistance by a trained psychologist. Additionally, parents completed two short questionnaires previously developed for the Spanish enKid study( Reference Serra-Majem, Ribas and Ngo 24 ) to evaluate children’s adherence to a Mediterranean diet (Kidmed) and physical activity habits (Krece Plus; Table 1).
Table 1 Children’s and parents’ questionnaires used in Program SI! (including the number of items, score range and outcome evaluated)
PA, physical activity; K, knowledge; A, attitudes; H, habits; MD, Mediterranean diet.
The Kidmed questionnaire consists of sixteen questions related to the principles of Mediterranean dietary patterns. The score ranges from −4 to 12 points, since questions with negative connotations with respect to the Mediterranean diet are assigned a value of −1 (frequent intake of fast food, increased consumption of sweets, skipping breakfast, frequent intake of pastries for breakfast). Parameters with positive connotations are assigned +1 point (e.g. takes a fruit or fruit juice every day, consumes fish regularly (at least 2–3 times/week)) as indicated previously( Reference Serra-Majem, Ribas and Ngo 24 ). As suggested by Serra-Majem et al.( Reference Serra-Majem, Ribas and Ngo 24 ), the total score was divided into three categories of Mediterranean diet quality: ≤3 points, poor diet quality; 4–7 points, average diet quality; and ≥8 points, good diet quality (optimal Mediterranean diet style).
The Krece Plus score ranges from 0 to 10 points and classifies lifestyle according to the average daily hours watching television or playing video games and the average weekly hours engaged in after-school physical activity. The test scoring system classifies children’s lifestyle as poor (≤5 points for boys, ≤4 points for girls), average (6–8 points for boys, 5–7 points for girls) or good (≥9 points for boys, ≥8 points for girls).
Parents’ dietary and physical activity assessment
Parents completed a Program SI! questionnaire( Reference Peñalvo, Santos-Beneit and Sotos-Prieto 20 , Reference Cespedes, Briceno and Farkouh 23 ) that assessed KAH related to diet, physical activity and knowledge of human health (Table 1). Physical activity habits were assessed as the number of days during the past week on which respondents engaged in physical activity for at least 30 min and the hours per workday spent seated while engaged in non-work related activities (Table 1).
Additionally, parents also completed a validated fourteen-item questionnaire (Predimed) assessing adherence to the traditional Mediterranean diet( Reference Schröder, Fitó and Estruch 25 ). Values of 0 or 1 were assigned to each questionnaire item, producing a test score between 0 and 14 points, with higher scores indicating greater Mediterranean diet adherence( Reference Schröder, Fitó and Estruch 25 ). Scores were grouped to define three categories: poor adherence to the Mediterranean diet (≤4 points), average adherence (5–8 points) and high adherence (good: ≥8 points).
Cross-referenced items and agreement
In the assessment of children’s self-reported habits, four items for dietary habits and two for physical activity were identical in both the Program SI! and enKid (Kidmed and Krece Plus) questionnaires. The duplicated dietary items relate to questions on breakfast habits (skipping breakfast, eating dairy products, eating cereals or grains, eating commercially baked goods or pastries) and the duplicated physical activity items relate to sedentary behaviour.
For the comparison of children and parents, five items were common to the Kidmed and Predimed questionnaires: vegetable consumption (≥2 servings/d), fruit consumption (≥2 servings/d), fish consumption (>2–3 servings/week), nut consumption (>2–3 servings/week) and use of olive oil as the main culinary fat at home. This information was used to evaluate the degree of association and the influence between parents’ and children’s dietary habits.
Socio-economic and demographic data
Parents completed a short questionnaire to gather information on age, gender, relationship with the child or children (mother, father or legal guardian), education level, number of persons in the household and family income. Parental education level was first classified according to the guidelines of the Instituto Nacional de Estadística (INE; www.ine.es) and then categorized into three bands according to the International Standard Classification of Education (ISCED; http://www.uis.unesco.org/Education/Pages/international-standard-classification-of-education.aspx, 2011): low (none or primary studies; ISDED 0–2), medium (completed high school; ISCED 3 or 4) and high (high qualification or completed university degree; ISCED 5 or 6). Income status was classified as above or below (or equal to) the Spanish annual average of €22 500 (Wage Structure Survey, 2009; www.ine.es).
Statistical methods
Continuous variables are presented as means and standard deviations, whereas categorical variables are presented as absolute and relative frequencies. Categorical variables were compared by using contingency tables and the χ 2 test. The t test and ANOVA were applied to compare unadjusted means. Kappa statistics were used to evaluate the agreement between questions related to dietary and physical activity habits answered by children and their parents. We calculated Pearson correlation coefficients and kappa statistics to measure the association between parents’ healthy habits and those of their children.
We conducted a nested analysis adjusting for school level, as children from the same schools may be more similar to each other. Logistic regression analyses were used to examine the effect of parental education level and income status on the percentage of respondents achieving a 1-point positive score for each healthy behaviour of the questionnaires. Dichotomous variables were used for all the questionnaire items assessed. High parental education level or high income status was set as the reference category. The influence of participants’ sociodemographic characteristics on Kidmed and Krece Plus scores was assessed by ANCOVA models. All models were adjusted for gender (male, female), age (as continuous), origin (Madrid, rest of Spain, rest of Europe, Latin America, Africa, others) and school plus education level when this was not the variable of interest. The P value for linear trend was tested across each category.
Statistical significance was set at the <0·05 level and all tests were two-tailed. All statistical analyses were conducted with the STATA statistical software package version 12·0.
Results
Sample characteristics
A total of 2062 children (49·5 % girls) and 1949 parents (77·9 % women) were involved in the study at baseline (Table 2). The mean age of children was 3·7 (sd 0·9) years and that of parents was 36·5 (sd 5·8) years. Most parents self-reported medium (20·6 %) or high (63·3 %) education level, and 36·5 % of parents reported an annual salary above €22500. Diet quality within the household, measured by adherence to a Mediterranean diet pattern, was moderate for both children (average Kidmed score=7·4 (sd 2·0) points) and parents (average Predimed score=6·3 (sd 2·4) points). Children’s scores on physical activity habits were also moderate (Krece Plus score=5·5 (sd 2·0) points).
Table 2 Baseline characteristics of the study sample: children (n 2062) aged 3–5 years and their parents (n 1949), Madrid, Spain, October–November 2011 (Program SI!)
Continuous variables are expressed as mean and standard deviation; categorical variables as n (sample size) and percentage.
Dietary and physical activity reporting of children’s habits by parents and children
The level of agreement for items common to parent- and self-reported assessments of children’s habits is shown in Table 3. Reporting was in agreement for item 1 (skips breakfast) and across age strata (κ>0·1; P<0·001; Table 3). For item 3 (cereals and grains) the overall number of agreement (yes or no) was low (1094 of 2062; 53·1 %) but still statistically significant (κ=0·054; P=0·058); however, significant agreement across ages was maintained only for 5-year-olds (κ=0·091; P=0.020), and this was also the case for item 2 for 5-year-olds (κ=0·102; P=0·007; data not shown in Table 3).
Table 3 Correspondence between parental reporting v. children’s self-reporting of dietary and physical activity habits; children (n 2062) aged 3–5 years and their parents (n 1949), Madrid, Spain, October–November 2011 (Program SI!)
† Parental reporting regarding children’s habits (diet: Kidmed; physical activity: Krece Plus).
Parent- and self-reported assessments diverged significantly for item 4 (commercially baked goods; 45·4 % overall agreement; κ=−0·058; P=0·001). Disagreement was more pronounced for physical activity assessments, with only 24·9 % of parents and children agreeing on the time children dedicate during the week to sedentary activities (item 5: television and video games) and only 33·2 % agreeing on the time spent engaged in physical activity (item 6).
Association between parents’ and children’s dietary and physical activity habits
The association between parents’ and their children’s dietary and physical activity habits is revealed by the data in Table 4. A positive agreement and higher odds to have the same dietary habits between parents and their children was found for consumption of vegetables, fruit, fish and olive oil (OR>2; κ>0·1; P<0·001), but not for consumption of nuts (P=0·516). The same pattern was observed for parents and their children for physical activity habits (P<0·001). Significant correlation was found for parents’ and children’s adherence to the Mediterranean diet (r=0·356; P<0·001; data not shown).
Table 4 Association between parents’ dietary and physical activity habits and those of their children; children (n 2062) aged 3–5 years and their parents (n 1949), Madrid, Spain, October–November 2011 (Program SI!)
Two-sided level of significance: *P<0·05, **P<0·001.
† OR determined by logistic regression model. Reference category: negative answer (no).
‡ P value for κ test agreement.
Sociodemographic determinants of Kidmed and Krece Plus scores
A higher parental educational level and income status were associated significantly with higher Kidmed (mean score for educational level: 7·59; 95 % CI 7·47, 7·70 for high v. 6·59; 95 % CI 6·56, 7·04 for low; income status: 7·58; 95 % CI 7·41, 7·74 for high v. 7·25; 95 % CI 7·13, 7·38 for low) and Krece Plus (mean score for educational level: 5·67; 95 % CI 5·55, 5·78 for high v. 4·91; 95 % CI 4·69, 5·15 for low; income status: 5·81; 95 % CI 5·55, 5·87 for high v. 5·37; 95 % CI 5·25, 5·49 for low; Fig. 1).
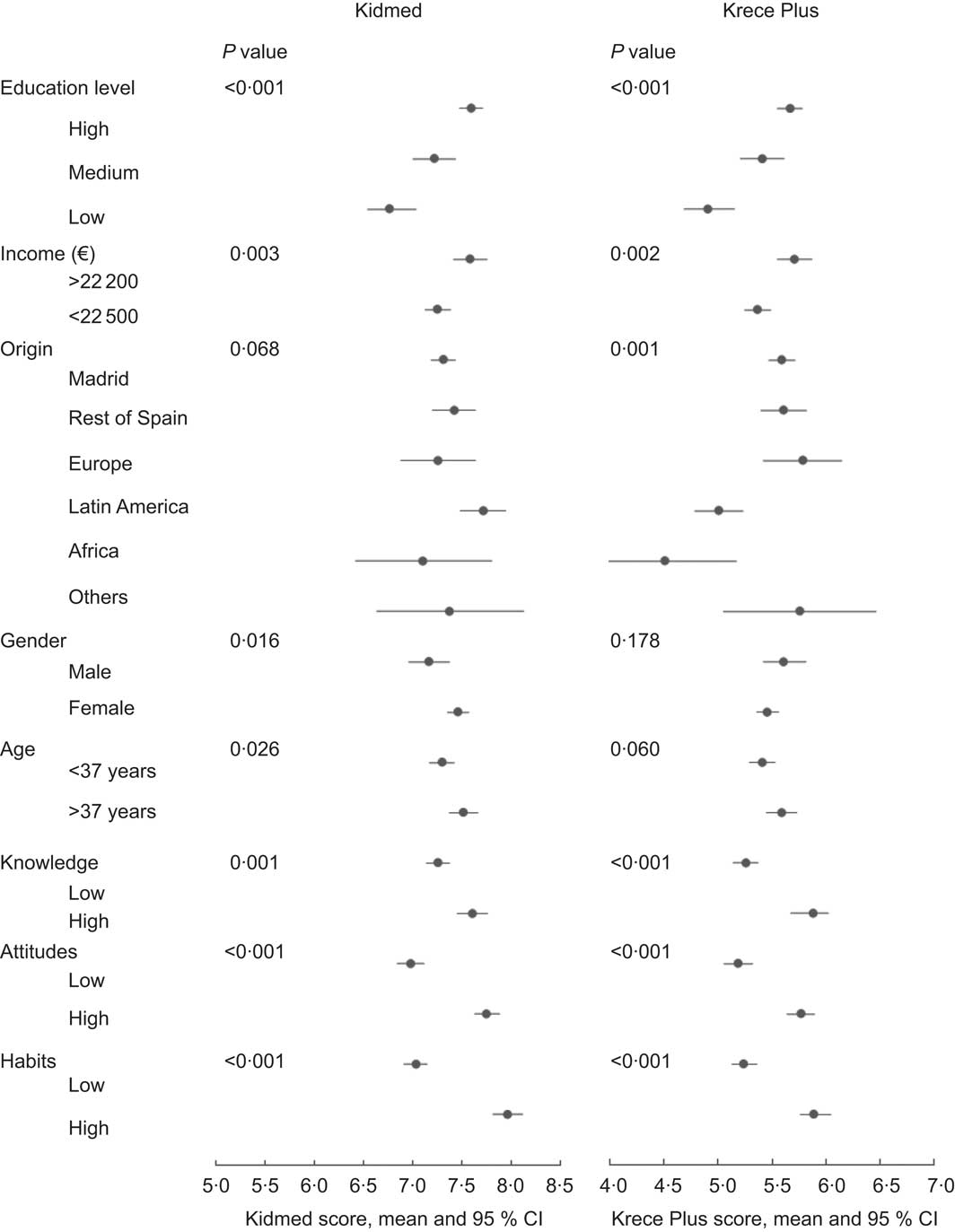
Fig. 1 Mean Kidmed and Krece Plus scores (with 95 % confidence intervals represented by horizontal bars) among children (n 2062) aged 3–5 years according to selected variables, Madrid, Spain, October–November 2011 (Program SI!). The influence of participants’ sociodemographic characteristics on Kidmed scores (indicating adherence to a Mediterranean diet, range −4 to 12 points) and Krece Plus scores (indicating physical activity behaviours, range 0 to 10 points) was assessed by ANCOVA models adjusted for age, gender, geographic origin, school and socio-economic status, unless the variable was the one of interest. Statistical significance was set at the <0·05 level and all tests were two-sided. ‘P value’ refers to P for trend in those variables with more than two categories; otherwise, P value is for the ANCOVA test
Parents of Latin American origin reported higher Kidmed scores (7·71; 95 % CI 7·48, 7·93) but lower Krece Plus scores (5·01; 95 % CI 4·79, 5·23) compared with families originating in Spain, other European countries, African or other regions. Mothers reported higher Kidmed scores (7·46; 95 % CI 7·35, 7·56) than fathers (7·17; 95 % CI 6·97, 7·37; P=0·016), whereas fathers tended to report higher scores for Krece Plus (5·61; 95 % CI 5·42, 5·81) than mothers (5·46; 95 % CI 5·36, 5·56; P=0·178). Parental age was also associated with higher scoring; compared with parents younger than 37 years, those older than 37 years reported higher scores for Kidmed (7·30; 95 % CI 7·17, 7·42 v. 7·51; 95 % CI 7·37, 7·65; P=0·026) and Krece Plus (5·41; 95 % CI 5·29, 5·53 v. 5·59; 95 % CI 5·45, 5·73; P=0·060). Interestingly, a higher parental KAH score for healthy behaviours was significantly associated with higher Kidmed and Krece Plus scores (P<0·001).
Since socio-economic status (SES) was associated with better scores, we further investigated the influence of parental education and income status on their children’s adoption of healthy habits. Frequencies of a 1-point positive score for each healthy behaviour and odds ratios (with 95 % confidence intervals) for all Kidmed and Krece Plus items are shown in Tables 5 and 6.
Table 5 Prevalence of 1-point score and odds ratios (and 95 % confidence intervals) from logistic regression, showing the correlation of parental education level with children’s Kidmed and Krece Plus items; children (n 2062) aged 3–5 years and their parents (n 1949), Madrid, Spain, October–November 2011 (Program SI!)
Two-sided level of significance: *P<0·05, **P<0·001.
† High education level: n 1197, 63·3 %; medium education level: n 389, 20·6 %; low education level: n 304, 16·1 %.
‡ Adjusted OR and 95 % CI determined by logistic regression models. Models adjusted for age, gender, geographic origin and school. Reference group=high education level.
§ Pulses include beans, peas, lentils and chickpeas.
|| Kidmed score (range −4 to 12 points): poor, ≤3 points; average, 4–7 points; good, ≥8 points. Reference group=poor+average; OR presented for good v. poor+average.
¶ Krece Plus score (range 0–10 points): poor, ≤5 points (boys), ≤4 points (girls); average, 6–8 points (boys), 5–7 points (girls); good, ≥9 points (boys), ≥8 points (girls). Reference group=poor+average; OR presented for good v. poor+average.
Table 6 Prevalence of 1-point score and odds ratios (and 95 % confidence intervals) from logistic regression, showing the correlation of parental income status with children’s Kidmed and Krece Plus items; children (n 2062) aged 3–5 years and their parents (n 1949), Madrid, Spain, October–November 2011 (Program SI!)
Two-sided level of significance: *P<0·05, **P<0·001.
† High income status (>€22 500): n 650, 36·5 %; low income status (≤€22 500): n 1130, 63·5 %.
‡ Adjusted OR and 95 % CI determined by logistic regression models. Models adjusted for age, gender, geographic origin and school. Reference group=high income level.
§ Pulses include beans, peas, lentils or chickpeas.
|| Kidmed score (range −4 to 12 points): poor, ≤3 points; average, 4–7 points; good, ≥8 points. Reference group=poor+average; OR presented for good v. poor+average.
¶ Krece Plus score (range 0–10 points): poor, ≤5 points (boys), ≤4 points (girls); average, 6–8 points (boys), 5–7 points (girls); good, ≥9 points (boys), ≥8 points (girls). Reference group=poor+average; OR presented for good v. poor+average.
Parental educational level was associated with a positive answer rate frequency for children’s daily consumption of fruit or juice, eating fresh or cooked vegetables daily, having cereals or grains for breakfast and having a diary product for breakfast (P trend=0·028, 0·001, 0·004 and 0·015, respectively). The largest odds ratio differences were found in the low educational level category (reference category=high) for using olive oil at home (OR=0·23; 95 % CI 0·13, 0·41) and skipping breakfast (OR=0·36; 95 % CI 0·23, 0·55; Table 5). Similar results for these items were shown when analysing by income status (olive oil at home: OR=0·23; 95 % CI 0·09, 0·54; skipping breakfast: OR=0·42; 95 % CI 0·25, 0·68; Table 6). However, higher odds of accomplishing the recommendations were observed in the low v. the high education category for consuming pulses (beans, peas, lentils or chickpeas) more than once weekly (OR=1·71; 95 % CI 1·14, 2·55; Table 5).
Low parental educational level and low income status showed a similar association of lower odds of a positive score for consuming fresh cooked vegetables more than once daily and consuming fish regularly at least 2–3 times/week (P trend<0·005; Tables 5 and 6), and going to a fast-food restaurant more than once weekly and having commercially baked foods or pastries for breakfast were associated lower odds of a positive score when comparing educational level categories (Table 5).
However, higher odds of accomplishing positive scores were observed for consuming nuts regularly (OR=1·58; 95 % CI 1·15, 2·15 for low v. high education level and OR=1·49; 95 % CI 1·13, 1·97 for low v. high income status). We found a high percentage of pasta or rice consumption ≥5 times/week (χ 2 test: P=0·001 and P<0·001) in low parental educational level and income status (Tables 5 and 6), although we did not find significant association in the logistic regression analysis.
A higher percentage of good Mediterranean diet adherence was observed in children of parents with a high educational level (53·3 %) compared with those in the middle (46·5 %) and low educational categories (42·8 %; P<0·001). Similar results were found for income status (high 53·3 % v. low 42·8 %; P<0·001). Similarly, a good level of physical activity was achieved by 15·0 % of children whose parents had high education level compared with 13·8 % of children whose parents had low education level (P<0·001; Table 5). No significant results were found by income status (P=0·137).
Discussion
Although kappa statistics showed low rates of agreement (a paradox that has been described previously( Reference Feinstein and Cicchetti 26 – Reference Cicchetti and Feinstein 28 )), our results showed from a moderate to a positive percentage of agreement between parental assessment and children’s self-reports for three of the six questions evaluated, and this association seemed to be stronger for children aged 5 years old. An inverse agreement was found for the item assessing the consumption of pastries for breakfast. While several intervention studies in children have been reported, very young children have been studied only in the IDEFICS (Identification and prevention of Dietary- and lifestyle-induced health effects In Children and infantS) study (2–9 years old) and a few others( Reference dos Santos Barroso, Sichieri and Salles-Costa 4 , Reference Hu, Ye and Li 15 , Reference Garemo, Lenner and Nilsson 16 ). These studies assumed that parents or other child carers report children’s habits accurately. Dietary assessment in children at this age is a particular challenge for investigators, since it raises the issue of the reliability of information provided by parents, who may provide, instead of an accurate assessment, what they consider to be the correct answer. We might hypothesize that the inverse agreement found in our study could be due to the fact that the parents recognize this as an unhealthy dietary habit, leading them to report low consumption for this item in contrast to the higher values reported by the children. Additional reasons could be: (i) children are accurate reporters of their own behaviour, particularly with regard to dietary intake and physical activity that may happen while at school (or at least when they are not at home under the supervision of their parents); or (ii) children are poor reporters and parents are accurate. However, this is only our interpretation and further analysis should be carried out to address this point.
Our study further provides evidence that, at least in this particular Spanish population, there is a significant association between the health habits of parents and those of their children. Parents’ adherence to a Mediterranean diet and regular physical activity positively affect their children’s health habits. Consistent with our results, a meta-analysis analysing parents’ influence on children’s eating habits showed weak or moderate correlations (0·20–0·30) for key dietary measures( Reference Wang, Beydoun and Li 12 ), although that meta-analysis included few studies with children under 5 years of age. A study of children from the ages of 2 to 18 years, using a total dietary quality score, showed a mother–daughter correlation of 0·18 and a mother–son correlation of 0·28( Reference Beydoun and Wang 29 ). Our study shows a higher correlation (0·356) and even stronger associations as the children grow. The positive association between parents’ consumption of vegetables, fruit, fish and olive oil and consumption of these foods by their children has also been observed by other studies( Reference Hart, Raynor and Jelalian 30 – Reference Riediger, Shooshtari and Moghadasian 32 ). This suggests that parents have an important influence on their children’s dietary intake and that this is especially relevant at a young age, when children develop lifelong habits.
Our findings also show variations of children’s Kidmed and Krece Plus scores with specific parental characteristics. The Kidmed and Krece Plus scores were higher for children whose parents were aged 37 years or older. Moreover, Kidmed score was also higher for responses from mothers and from parents of Spanish or Latin-American origin. Our results agree with previous studies which reported that older parents included a greater number of healthy items in their children’s diet( Reference dos Santos Barroso, Sichieri and Salles-Costa 4 ). This might be related to the acquisition of knowledge and awareness with age. Interestingly, we also found that parents’ KAH scores for human health determined children’s dietary and physical activity scores, so that children of parents with higher KAH scores are likely to have better scores for healthy behaviours. This effect was seen regardless of parents’ education level, indicating that parents’ KAH score for nutrition is independently associated with children’s Kidmed and Krece Plus scores. In agreement with our results, an Australian study( Reference Zarnowiecki, Sinn and Petkov 33 ) in 193 children aged 5–6 years found that parents’ nutritional knowledge directly predicted that of their children, including an ability to distinguish between healthy and unhealthy foods( Reference Hu, Ye and Li 15 ). Studies carried out in older children (9–11 years) emphasized that better parental knowledge of nutrition leads parents to place greater emphasis on teaching their children about healthy foods and therefore to improve their health-related behaviours and choices( Reference Mitchell, Farrow and Haycraft 8 , Reference Savage, Fisher and Birch 9 , Reference Lazarou, Kalavana and Matalas 11 , Reference Gibson, Wardle and Watts 34 ). The current study, with younger children, suggests that in addition to parents’ knowledge, their attitudes and habits are also likely to lead to better adherence to a healthy diet and physical activity by their children.
Another factor influencing children’s dietary and physical activity habits identified by our analysis is parental SES (education level and income status). Our findings indicate that this association affects most of the health-related questions evaluated. The likelihood of achieving a 1-point positive score for eating fruit or juice every day, consuming fresh or cooked vegetables daily, having cereals or grains for breakfast and having a diary product for breakfast was higher for children of parents in the highest education level category. Most previous studies that analysed parental SES found a similar relationship with health-related behaviours( Reference Bammann, Gwozdz and Lanfer 17 , Reference Tandon, Zhou and Sallis 18 , Reference Riediger, Shooshtari and Moghadasian 32 ). In the IDEFICS study( Reference Miguel Fernandez-Alvira, Mouratidou and Bammann 35 ) on children between 2 and 9 years of age, parental educational level was associated with fruit and vegetable intake, as in other studies( Reference Hart, Raynor and Jelalian 30 , Reference Cooke, Wardle and Gibson 31 ), but was additionally associated with intake of fish and cereals. A recent Greek study( Reference Antonogeorgos, Panagiotakos and Grigoropoulou 19 ) in older children (10–12-year-olds) also used the Kidmed score and found an association between higher parental education level and a healthier lifestyle and dietary profile among children (Mediterranean diet and time devoted to sports activities), expanding on earlier results obtained in another Greek population( Reference Kontogianni, Farmaki and Vidra 36 ).
Lower SES in our study was associated with modest scores for vegetable and fish consumption, skipping breakfast, fast-food intake and consuming pastries for breakfast. It is noteworthy that the largest differences seen in children from low-SES households were the lower olive oil consumption, the higher consumption of pulses (beans, peas, lentils or chickpeas) and the higher frequency of pasta/rice consumption, since these products are associated with purchasing power. Lower education level may be linked to lower income and subsequently to a relatively greater availability of less expensive foods such as rice, pulses and junk food( Reference dos Santos Barroso, Sichieri and Salles-Costa 4 ). Conversely, olive oil is an expensive item that is less accessible for low-income households in which cost is a key factor in food choice. Such a conclusion is consistent with a study that reported a poorer diet among 5-year-old children from less advantaged backgrounds( Reference Skafida 37 ).
A strength of our study is the stratified randomization process for selecting schools for intervention, which decreases the chance of bias in the study sample. The questionnaires used to assess parents’ and children’s dietary and physical activity habits both yielded comparable information for the same items, thus allowing evaluation and correlation of the information obtained. In addition, many earlier studies did not include information about which parent (mother or father)( Reference Lazarou, Kalavana and Matalas 11 , Reference Johannsen, Johannsen and Specker 38 ) answered the questionnaire, and our results indicate that this should be taken into account since it seems to have an influence on children’s choices.
A limitation of our cross-sectional study is that, by design, bidirectionality is likely for all observed associations and cause-and-effect relationships cannot be established. Another limitation is that, since the study population is characteristic of the city of Madrid, the findings might be applicable only to similar urban environments.
Conclusions
The present study shows that children’s dietary and physical activity habits may be associated with those of their parents and also influenced by the socio-economic characteristics of the household. Our results showed low agreement between parental report and children’s self-report for those items that the parents recognized as representing unhealthy habits. Therefore, parental reporting bias must be taken into consideration in studies involving pre-school children, although additional reasons could be considered as well (such as children are accurate regarding their own behaviour in the school; or in contrast, children are poor reporters and parents accurate). Older parental age (>37 years), maternal health habits, Spanish origin and higher KAH in relation to human health were identified as the main parental determinants of higher scores in children. Given the difficulty of changing socio-economic indicators, interventions that include strategies to increase parental responsibility for the family’s health will increase the opportunities for their children to adopt a healthier lifestyle. This intervention should begin with parents and their children in their early years, when there is a window of opportunity for instilling lifelong healthy behaviours.
Acknowledgements
Financial support: This study was funded by the Fondo de Investigación Sanitaria del Insituto de Salud Carlos III, Madrid (research grant PI11/01885). Conflict of interest: All authors declare no conflict of interest. Authorship: M.S.-P. assisted with data collection, performed data management and statistical analyses, and interpreted and drafted the manuscript. G.S.-B. coordinated data collection, interpreted results and helped draft the manuscript. R.J. interpreted data and helped draft the manuscript. S.P. oversaw statistical analyses and helped draft the manuscript. V.F. conceived the intervention study and helped draft the manuscript. J.L.P. coordinated and designed the study, interpreted the results and helped draft the manuscript. Acknowledgements: The authors would like to thank the International SHE Foundation, intellectual owner of Program SI! They also thank the ALICIA Foundation and Sesame Workshop for providing the materials needed for the intervention.







