



Supermarkets have a powerful influence on the relative healthfulness of Australian food environments and have been described as gatekeepers of the food supply(Reference Pulker, Trapp and Scott1). They are the dominant retail food environment in Australia, responsible for 60 % of total food expenditure(2). Despite making fresh fruit and vegetables available, supermarkets are a driver of poor diet and have mainly negative impacts on public health(Reference Pulker, Trapp and Scott1,Reference Hawkes3) . The majority of supermarket packaged food products are highly processed and high in added nutrients of public health concern, such as saturated fat, sugar and Na(Reference Ni Mhurchu, Brown and Jiang4). Regular consumption of a dietary pattern high in these foods contributes to a poor diet, a key determinant for many of the most significant health concerns facing Australia, including obesity, CVD, type 2 diabetes and some cancers(Reference Forouzanfar, Afshin and Alexander5,6) .
Supermarket chains Coles and Woolworths control two-thirds of the grocery retail market in Australia and sell their own exclusive ranges known as supermarket own brands (SOB)(Reference Cloutman7). Previously in Australia, branded products dominated the market but SOB have been steadily increasing in popularity over the last decade to account for 25 % of all supermarket sales in 2018(Reference Cloutman7). The growth of discount retailer Aldi’s own brand products has pushed Coles and Woolworths to compete by expanding their own brand ranges, driving innovation and quality in these products(Reference Pulker, Trapp and Scott1,Reference Cloutman7) .
Following the trend set by UK supermarkets, Coles and Woolworths have significantly expanded their ranges of SOB chilled convenience foods (SOBCCF), including ready meals(8). In 2017, their share of the chilled and frozen ready meals market was one-third, with the strongest growth coming from sales of chilled ready meals(8). Chilled convenience foods are stored in refrigerators and defined as ‘any fully or partially prepared foods in which significant preparation time, culinary skills or energy inputs have been transferred from the home kitchen to the food processor and distributor’ (p. 3)(Reference Traub and Odland9). Chilled ready meals are convenient meals, prepared outside of the home, stored in the refrigerator and cooked or reheated in the home(Reference de Boer, McCarthy and Cowan10).
Convenience is increasingly marketed to consumers to influence their food choice, based on factors including ageing population, time scarcity and changing household structures(Reference Jackson and Viehoff11,Reference Sheely12) . Due to increases in sales and consumption of supermarket convenience foods and domination of SOB, especially in the chilled convenience foods sector, it is important to assess their nutritional quality. Public health professionals can then provide evidence-based advice on the relative healthfulness of these products. There is scope for public health professionals to liaise with supermarkets to improve the nutritional quality of SOB foods, which could contribute to improved Australian population diets(Reference Glanz, Bader and Iyer13,Reference Burch, Dixon and Lawrence14) .
Fourteen international studies have evaluated the nutritional quality of chilled convenience foods and found substantial variation between brands and within product groups, which could also reasonably be predicted to be observed in Australia(Reference Ahuja, Pehrsson and Cogswell15–Reference Waterlander, van Kouwen and Steenhuis28). Although this category of food is typically high in saturated fat, sugar and Na, the large variation in nutritional quality highlights the importance of identifying healthier choices(Reference Poti, Mendez and Ng25). Seven studies have assessed the nutritional quality of Australian supermarket chilled convenience foods(Reference Ni Mhurchu, Brown and Jiang4,Reference Christoforou, Dunford and Neal29–Reference Webster, Dunford and Neal33) . Five of the studies did not investigate SOB, and two evaluated SOBCCF by comparing the nutrient content to branded products(Reference Cleanthous, Mackintosh and Anderson30,Reference Trevena, Neal and Dunford32) . Neither of the studies of Australian SOBCCF used standardised measures to assess nutritional quality, such as the Australian government’s food selection guide the Australian Guide to Healthy Eating (AGTHE)(34), the NOVA classification based on the level of food processing(Reference Monteiro, Cannon and Levy35) or front-of-pack (FOP) nutrition labels such as the Health Star Rating (HSR)(36). Assessing the nutritional quality of Australian SOBCCF using standardised measures incorporates the latest credible scientific evidence supporting the association between diet and health and longevity(34).
Currently, the nutritional quality of Australian SOBCCF is unknown, yet consumption of these foods is increasing. This study aimed to assess the nutritional quality of Australian SOBCCF, by addressing the following research questions: (1) What proportion of Australian SOBCCF are classified as healthy or unhealthy using contemporary nutrition recommendations and assessment criteria, including the AGTHE, NOVA and HSR score? (2) Does classification of nutritional quality of SOBCCF differ between the three measures? (3) Does the nutritional quality of SOBCCF differ between supermarkets?
Methods
Selection of supermarkets
Two conveniently located, large exemplar supermarkets from the major supermarkets present in Perth, Western Australia (Coles and Woolworths) were selected for this study. An Independent Grocers of Australia store was audited, but no SOBCCF were present. Discount retailer Aldi was not included in this study due to the limited range of foods sold(37) and because it had only just entered the Western Australia market at the time of the study(38). The specific stores were selected because they were identified as ‘optimised’ or examples of best practice for the chains, that is, they were large supermarkets with the most up-to-date layouts and displays and an increased likelihood of stocking a large range of SOB foods. A detailed description of the supermarket audit protocol is available elsewhere(Reference Pulker, Trapp and Foulkes-Taylor39).
Identification of SOBCCF
SOB foods were identified by the presence of the supermarket’s branding on the front of packaging(Reference Pulker, Trapp and Foulkes-Taylor39). The term ‘convenience foods’ is contested and used inconsistently(Reference Jackson and Viehoff11,Reference Peltner and Thiele40) . The authors applied the definition by Traub et al. because it remains relevant today and provides more detail than the alternatives. Chilled convenience foods were displayed in refrigerators and identified as ready-prepared foods which save consumers significant preparation time and require little to no cooking skills, as effort has been transferred from the home kitchen to the food manufacturer(Reference Traub and Odland9). The audits identified all chilled convenience foods which carried a SOB.
Chilled convenience foods were available in the following product groups: ready meals, pizza, soup, quiche and pies, pasta and pasta sauce, garlic bread and naan bread, dressed salads (e.g. coleslaw), salad kits and bowls (e.g. products that contain salad, dressing and toppings), antipasto and dips, prepared vegetables (e.g. mashed potato), sauces and salad dressings, desserts, prepared meat (e.g. marinated, stuffed or pre-cooked products) and vegetarian food (e.g. marinated tofu). All SOBCCF collected during the audits were included in the sample, and no categories of SOBCCF were excluded.
Data collection
Data were collected over a 3-week period in February 2017. In addition to conducting photographic audits of all 3940 SOB foods present in the selected stores, 302 SOBCCF were purchased to conduct more detailed examination of packaging information. Each SOBCCF was assigned a code, and the packaging was photographed in a food laboratory at Curtin University. The code was visible in all laboratory-based photographs, for easy identification of the products. Photographs taken of the FOP and back-of-pack (BOP) were stored in an electronic filing system using the assigned product code.
Data extraction
Data from the FOP and BOP of the SOBCCF were extracted into a Microsoft Excel (2016) database, including supermarket, product group, product photo code, SOB name, product name, HSR score, all information from the nutrition information panel and all ingredients in the ingredients list in the order displayed. Where nutrition information panel values were ‘<0·1’, they were recorded in the database as ‘0’.
Of the 302 SOBCCF, eleven had missing BOP photos, so their nutrition information panel and ingredients list were unavailable. As products are regularly reformulated and the original data could not be obtained, these SOBCCF were removed from the data set. Fibre content is not a mandatory requirement on packages in Australia, and forty-four SOBCCF nutrition information panels did not include it. A product information spreadsheet provided by Woolworths in March 2017 was used to obtain fibre data for one product, and data for the remaining forty-three products were obtained by locating identical or similar products in FoodWorks 9 Professional (Xyris). Therefore, 291 SOBCCF were included in the analysis.
Assessment of nutritional quality
Nutritional quality was assessed using the principles of the AGTHE(34), NOVA classification of level of food processing(Reference Monteiro, Cannon and Levy35) and HSR scores(36).
The Australian government’s food selection guide, the AGTHE, aims to assist people to make food choices that contribute to overall health and minimise the risk of diet-related disease(34,41) . SOBCCF were classified as either healthy (recommended five food group foods or mixed products using mainly five food group foods) or unhealthy (discretionary foods which are not essential for a healthy diet or mixed products high in sugar, fat or salt)(Reference Pulker, Trapp and Foulkes-Taylor39). Due to the difficulty of classifying convenience foods using the information provided in the AGTHE’s Educator Guide(41) and the Australian Bureau of Statistics’ principles for identifying discretionary foods(42), two mixed food groups were created (i.e. mixed products using mainly five food group foods and mixed products high in sugar, fat or salt)(Reference Pulker, Trapp and Foulkes-Taylor39). Supplemental Table 1 describes the classification procedure in detail.
The NOVA system classifies foods according to the intention for use and degree of industrial food processing and is the basis of the recommendations of the dietary guidelines of Brazil, Uruguay, Ecuador and Peru(Reference Monteiro, Cannon and Lawrence43). The classifications include unprocessed or minimally processed foods; processed culinary ingredients; processed foods and ultra-processed foods (UPF)(Reference Monteiro, Cannon and Levy35). UPF have been transformed and degraded through industrial processes, leading to the removal of beneficial food components and the inclusion of cosmetic additives(Reference Monteiro, Cannon and Levy35). UPF are typically hyper-palatable and higher in energy, saturated fat, sugar and Na than less processed food(Reference Monteiro, Cannon and Levy35). Higher intakes of UPF are associated with poor diet quality and some diet-related diseases and are recommended to be avoided(Reference Monteiro, Cannon and Moubarac44,Reference Monteiro, Cannon and Moubarac45) .
The HSR is Australia’s government-led FOP nutrition labelling system that aims to help consumers compare similar packaged foods to make healthier choices(36). The HSR provides a rating from half a star to 5 stars, where 5 stars are the healthiest rating (see Supplemental Fig. 1). HSR scores are calculated using an algorithm based on the Food Standards Australia New Zealand nutrient profiling scoring criterion, which was developed to determine whether health claims can be made on packaging(37). The HSR applies an algorithm that allocates points for dietary fibre, protein and the proportion of fruit, vegetables nuts and legumes (FVNL), subtracts points for saturated fat, Na and total sugars and then converts the points to a score of ½ to 5 stars, with 5 stars indicating the healthiest choice(38). The ability of the HSR to discriminate nutritional quality is essential to meeting its policy aim(46); however, the appropriate HSR cut-off score to demarcate healthy and unhealthy food choices is contested(Reference Lawrence, Pollard and Vidgen47,Reference Pulker, Trapp and Scott48) . A score of 2·5 stars is considered an appropriate ‘pass mark’ by some researchers(Reference Pulker, Trapp and Scott48,Reference Lawrence, Dickie and Woods49) , whereas 3·5 has also been used by others(Reference Jones, Shahid and Neal50). The pass mark is taken to mean that a score of 2·5 (or 3·5) stars or more is appropriate for foods the AGTHE recommends, and the scores below the pass mark are appropriate for foods the AGTHE recommends to avoid. This study will use the two cut-off measures: (i) HSR of <2·5 for unhealthy foods and HSR of 2·5 or more for healthy foods and (ii) HSR of <3·5 for unhealthy foods, HSR of 3·5 or more for healthy foods, to examine the impact of the cut-off.
As the HSR is voluntary and not all SOBCCF displayed a HSR, a score was calculated for all SOBCCF using the Excel calculator provided on the HSR website(51). The HSR calculator requires input of the total percentage of FVNL and the total percentage of concentrated fruit and vegetable content. For products which included ingredients lists with the percentage content listed for FVNL, these amounts were used to calculate the total percentage present. Estimates of missing FVNL content were made based on the percentages provided for ingredients preceding or following the ingredient within the listing provided on packaging. Total FVNL contents of 1 % or less were excluded from the calculations. Minor discrepancies between the HSR displayed on the FOP of seven products from Coles and ten from Woolworths were identified, compared with the calculated HSR. For these products, the HSR scores displayed on the FOP appeared to have overlooked the fibre or FVNL content, so the calculated HSR was used for all SOBCCF included in the analysis.
The following SOBCCF were classified as unhealthy: discretionary foods, mixed products high in sugar, fat or salt, UPF, products with a HSR <2·5 stars and products with a HSR <3·5 stars.
Data analysis
Data were analysed using SPSS for Windows (version 24.0, IBM Corp.). To identify the proportion of Australian SOBCCF classified as unhealthy using three different measures of nutritional quality, the frequency of products classified as unhealthy was obtained overall and for each product group. The mean HSR, sd and frequency of products scoring <2·5 stars and <3·5 stars were calculated for the total data set and each product group.
To assess whether classification of nutritional quality of SOBCCF differed between the three measures, Cohen’s kappa test and percentage agreements were used to determine the level of agreement. A κ value of <0·20 was classified as poor agreement; κ = 0·21–0·40 was classified as fair; κ = 0·41–0·60 was classified as moderate; κ = 0·61–0·80 was classified as good and κ = 0·81–1·00 was classified as very good(Reference Dunford, Huang and Peters52). The percentage agreement between measures was calculated, and above 80 % was considered acceptable(Reference Dunford, Huang and Peters52).
To assess whether nutritional quality of SOBCCF from the two supermarket chains differed, a χ 2 test of independence was conducted to examine the relationship between the proportions of SOBCCF classified as unhealthy using each of the measures of nutritional quality and supermarket chain.
Results
Of the 291 SOBCCF included in this study, 177 were from Woolworths and 114 from Coles (Table 1).
Table 1 The nutritional quality of Australian supermarket own brand chilled convenience foods*
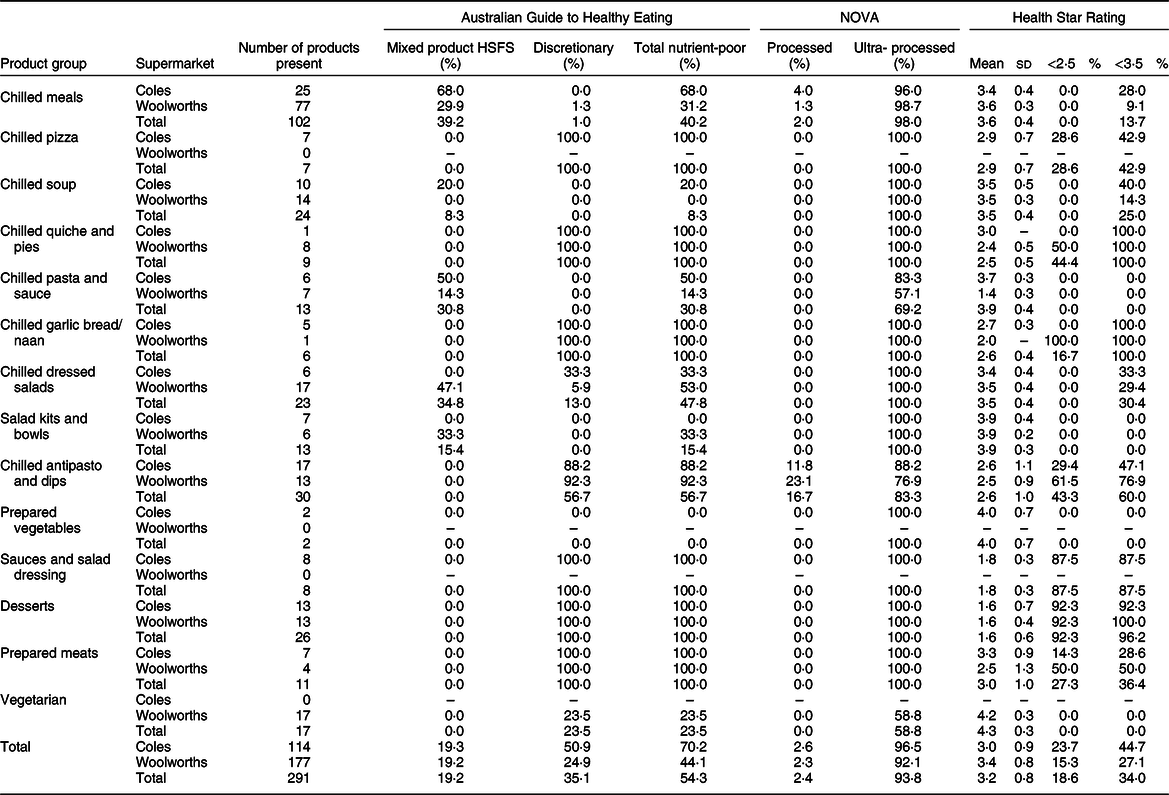
HSFS, high sugar, fat or salt.
* References for classification of nutritional quality include the Australian Guide to Healthy Eating(34), NOVA level of food processing(Reference Monteiro, Cannon and Levy35) and Health Star Rating score(36).
Prevalence of supermarket own brand chilled convenience foods classified as unhealthy
Table 1 shows that 54·3 % of all SOBCCF were classified as unhealthy using the principles of the AGTHE (70·2 % of Coles SOBCCF and 44·1 % of Woolworths SOBCCF). Almost all SOBCCF (93·8 %) were classified as UPF using NOVA (96·5 % of Coles SOBCCF and 92·1 % of Woolworths SOBCCF), based on the presence of industrial ingredients, colours, flavours, emulsifiers, stabilisers and thickeners.
Using a HSR <2·5 as the cut-off, 18·6 % of all SOBCCF were classified as unhealthy (23·7 % of Coles SOBCCF and 15·3 % of Woolworths SOBCCF) (Table 1). Using HSR <3·5 as the cut-off, 34·0 % of all SOBCCF were classified as unhealthy (44·7 % of Coles SOBCCF and 27·1 % of Woolworths SOBCCF).
Some SOBCCF product groups provided a greater proportion of healthy choices, including ready meals from Woolworths, soups, pasta and sauce, salad bowls and kits, prepared vegetables and vegetarian meals. They were considered healthy because few of the products were rated as unhealthy when applying the principles of the AGTHE, NOVA and HSR (Table 1).
The SOBCCF product groups that provided a greater proportion of unhealthy foods included ready meals from Coles, pizza, quiche and pies, garlic bread and naan, dressed salads, antipasto and dips, sauces and salad dressings, prepared meats and desserts. This is because the product groups had high proportions of products rated as unhealthy using the principles of the AGTHE, NOVA and HSR (Table 1).
Comparison of classification of nutritional quality of supermarket own brand chilled convenience foods using the three measures
Cohen’s kappa test found moderate agreement between the AGTHE and the HSR (3·5 stars cut-off) (κ = 0·51; 95 % CI 0·42, 0·60; P < 0·001); fair agreement between AGTHE and the HSR (2·5 stars cut-off) (κ = 0·32; 95 % CI 0·25, 0·40; P < 0·001) and poor agreement between AGTHE and NOVA (κ = 0·09; 95 % CI 0·04, 0·14 ; P < 0·001) and between NOVA and the HSR (3·5 stars cut-off) (κ = 0·04; 95 % CI 0·02, 0·06 ; P < 0·05) (Table 2).
Table 2 Cohen’s kappa test between measures of nutritional quality using Australian Guide to Healthy Eating (AGTHE)(34), NOVA, Health Star Rating (HSR)(36) using a 2·5 star cut-off and HSR using a 3·5 star cut-off

* Significant at P < 0.05.
** Significant at P < 0.001.
The percentage agreement between the AGTHE and the HSR (3·5 stars cut-off) was deemed unacceptable (58·2 %) for classifications of unhealthy, and for healthy, it was acceptable (94·7 %). There were 66 (41·8 %) SOBCCF classified as unhealthy by the AGTHE but as healthy using the HSR (3·5 stars cut-off) (Table 2).
The percentage agreement between the AGTHE and the HSR (2·5 stars cut-off) was considered unacceptable (34·2 %) for classifications of unhealthy, and for healthy, it was acceptable (100 %). The AGTHE classified 104 (65·8 %) SOBCCF as unhealthy, but they were classified as healthy using the HSR (2·5 stars cut-off).
The percentage agreement between the AGTHE and NOVA was acceptable overall (100·0 %) for classifications of unhealthy, and for healthy, it was unacceptable (8·3 %). There were 122 (91·7 %) SOBCCF classified as healthy by the AGTHE that were classified as UPF (unhealthy) by NOVA.
The percentage agreement between NOVA and the HSR (3·5 stars cut-off) was deemed unacceptable (35·4 %) for classifications of unhealthy, and for healthy, it was acceptable (100·0 %). There were 181 (64·6 %) SOBCCF classified as UPF (unhealthy) by NOVA that were classified as healthy by the HSR (3·5 stars cut-off).
Comparison of nutritional quality of supermarket own brand chilled convenience foods by supermarket chain
A χ 2 test of independence found that there were greater proportions of unhealthy foods at Coles in comparison with Woolworths, using the AGTHE (70·2 v. 44·1 %, P < 0·001), and a HSR <3·5 (44·7 v. 27·1 %, P < 0·05) (Table 3). For example, 70·2 % of Coles SOBCCF were classified as unhealthy using the principles of the AGTHE compared with 44·1 % at Woolworths.
Table 3 χ 2 tests of independence between supermarket chain and measures of nutritional quality
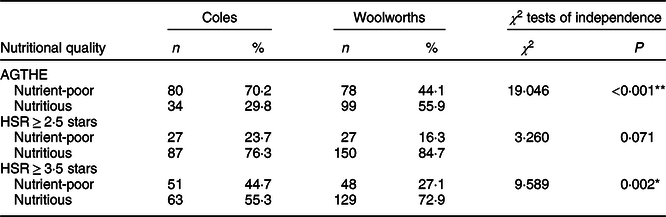
AGTHE, Australian Guide to Healthy Eating; HSR, Health Star Rating.
* Significant at P < 0.05.
** Significant at P < 0·001.
Discussion
Supermarkets have driven the increase in availability of chilled convenience foods such as ready meals in Australia and other developed countries, by developing SOB product ranges(Reference Hawkes3,Reference Burch and Lawrence53) . This current study found that a large proportion of these foods were classified as unhealthy, regardless of the measure of nutritional quality applied.
The proportion of unhealthy foods identified is broadly consistent with other studies, including two which assessed the Australian packaged food supply(Reference Dunford, Huang and Peters52,Reference Crino, Sacks and Dunford54) , indicating that the nutritional quality of SOBCCF is similar to that of all processed packaged foods. The very high proportion of UPF identified in this study is consistent with the research that identified UPF dominated Australian new product launches in 2015(Reference Spiteri, Olstad and Woods55). This is of public health concern because evidence suggests consumption of UPF can increase overall energy density of diets, displace unprocessed and minimally processed foods and contribute to diet-related diseases(Reference Monteiro, Cannon and Moubarac44,Reference Monteiro, Levy and Claro56) . In addition, these ready-to-eat or ready-to-heat, convenient, UPF can displace home-cooked foods, disrupt social patterns of eating, harm cultural food habits and cause economic and environmental issues through the domination of big corporations(Reference Monteiro, Cannon and Moubarac44).
Some SOBCCF product groups were rated healthier choices compared with others. It was anticipated that salad bowls and kits, and prepared vegetables would be healthier choices due to the high vegetable content of these products. However, it was unexpected that ready meals from Woolworths and all soups and vegetarian meals would also be healthier choices, since other studies have found high proportions of convenience foods to be unhealthy(Reference Ni Mhurchu, Brown and Jiang4,Reference Crino, Sacks and Dunford54) . Other product groups which were rated as unhealthy overall, including pizza, quiches, pies and desserts, were expected due to their classification as discretionary choices in the AGTHE(34). This study’s findings show the variability in healthfulness of current SOBCCF products; therefore, packaging information that reliably indicates healthier choices is essential to guide consumer food selection(Reference Pulker, Scott and Pollard57). Presence of some healthier product groups indicates potential for Australian supermarkets to improve the nutritional quality of SOBCCF, by changing the ingredients or recipes used for existing products or changing the types of products that are available.
This study found low levels of agreement between the different measures of nutritional quality for classifications of SOBCCF as either healthy or unhealthy. Of particular concern, the Australian government-led HSR FOP nutrition label was a poor indicator of foods that were consistent with the recommendations of the AGTHE, regardless of the cut-off selected (i.e. 2·5 stars or 3·5 stars). The study findings reveal that the main flaw of the current HSR system is the failure of the algorithm to allocate appropriately low scores (i.e. HSR of 2·0 stars or less) to foods to avoid in the AGTHE. Allocating HSR scores of 2·5 stars or above to foods recommended to be avoided promotes unhealthy food choices(Reference Pulker, Trapp and Scott48). Of the products that were classified as unhealthy according to the principles of the AGTHE, two-thirds were classified as healthy using a HSR cut-off of 2·5 stars. This study’s findings are consistent with those of an assessment of Australian packaged foods by Crino et al. which showed differences in nutritional quality ratings of convenience foods when applying the HSR, AGTHE and a NOVA-based level of processing(Reference Crino, Sacks and Dunford54).
The low levels of agreement between the three measures of nutritional quality used in this current study are likely to reflect inherent differences in the scope and function of the assessment measures. Dichotomous classification of nutritional quality based on the AGTHE identifies foods that are part of five food groups essential to healthy diets and foods to avoid which are energy-dense and nutrient-poor(34). The AGTHE is based on extensive modelling of dietary patterns that meet nutrient requirements and promote health, but does not consider the level of processing(58). Classification of foods using NOVA groups foods according to the level of processing and does not consider types of foods or levels of individual nutrients(Reference Monteiro, Cannon and Levy35). The NOVA system was developed in response to the dramatic increase in production and consumption of highly processed foods globally and concern about the impact of displacing traditional foods(Reference Monteiro59). Benefits of combining food types and level of processing when making population dietary recommendations have been identified(Reference Moubarac, Parra and Cannon60). In contrast, the HSR algorithm does not currently consider either the contribution of types of foods to healthy diets or the level of food processing, instead taking a reductionist approach (i.e. nutrient-orientated) to focus on levels of individual nutrients and presence of FVNL(Reference Lawrence, Pollard and Vidgen47). This is consistent with its purpose which is to identify healthier options within groups of similar foods(46), without considering level of processing or whether foods are consistent with the AGTHE recommendations. These findings demonstrate the complexities of measuring the nutritional quality of individual foods, and chilled convenience foods are additionally challenging because they are a mixed food and a relatively new type of food in Australia. This is important because consumers are likely to be unaware of the relative healthfulness of these foods.
This study found a greater proportion of healthy SOBCCF products available at Woolworths, compared with Coles, when applying two of the measures of nutritional quality. There were ninety-nine chilled convenient products that were consistent with the recommendations of the AGTHE available at Woolworths, which indicates the potential for these types of products to make a positive contribution to population diets. There have been no other studies comparing the nutritional quality of convenience foods between supermarket chains, to the authors’ knowledge. These findings indicate that similar analysis of SOBCCF in other countries would be of interest and may assist in identifying public health interventions that could improve the contribution of chilled convenience foods to population diets. The variability in nutritional quality of SOBCCF between supermarket chains found in this study also highlights the need for public policies to assist consumers to select healthy foods. Modifying the HSR so that it provides a robust indication of consistency with the recommendations of the AGTHE is needed in Australia. Warning labels have been adopted by some countries including Chile to identify foods that are high in sugar, fat, salt or energy content; studies indicate they can help consumers to identify whether foods are healthy or not(Reference Temple61). Consideration of a dichotomous system which allocates HSR to AGTHE five food group foods and warning labels for discretionary foods is recommended.
Strengths of this study include the selection of best practice supermarkets, which increased the likelihood of most available SOBCCF products being displayed in the stores during the audits. All HSR scores were calculated using the latest downloadable calculator, to ensure consistency and accuracy. However, calculations were limited by the quality of the data displayed on BOP. The FVNL content was estimated using percentages from BOP ingredients lists. Fibre content was missing for several SOBCCF; however, values were located from exact or similar product matches in FoodWorks 9 Professional (Xyris) or from a Woolworths’ product information spreadsheet from March 2017. Findings from this study may be affected by seasonality, as data were collected between Christmas and Easter, and product availability may differ at other times of the year. Aldi was not included in this study. The discount retailer has been credited with making a significant impact on Australian supermarkets, including driving discount pricing strategies and development of SOB foods(Reference Cloutman7), so the nutritional quality of Aldi SOBCCF deserves further investigation. More observational studies that assess the nutritional quality of SOB and branded foods from a wide range of food categories are recommended.
Supermarkets wield substantial power in Australia, and retail food environments hold great potential for positive change. Identifying supermarket policies to improve health holds the potential to stimulate change throughout the food system(Reference Taillie and Jaacks62). This study found that a large proportion of SOBCCF were unhealthy but some convenience food groups provided healthier choices overall, and a greater proportion of healthy choices were available at Woolworths. Both supermarkets can make significant improvements to the nutritional quality of SOBCCF by changing the ingredients or recipes for existing products and changing the types of products that are available. Removal of industrial ingredients, colours, flavours, emulsifiers, stabilisers and thickeners would change NOVA classification of SOBCCF from UPF to processed foods. A study finding of particular concern was the failure of the current HSR algorithm to allocate appropriate scores to foods that the Australian government’s food selection guide advises people to avoid. Public policies to assist consumers to select healthy foods need to address difficulties in identifying healthy chilled convenience foods, including modifying the HSR so that it provides a more robust indication of consistency with recommendations of the AGTHE.
Acknowledgements
Acknowledgements: The authors would like to thank France Foulkes-Taylor for assistance with data collection. Financial support: C.E.P. has a Health Promotion Research Training Scholarship from Healthway (No. 24124) and is supported through an Australian Government Research Training Program Scholarship. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. Conflict of interest: None. Authorship: C.E.P. conceived the study design and research objectives in consultation with J.A.S., C.E.P. and H.R.F. developed the research questions, C.E.P. collected the data, H.R.F. extracted and analysed the data, and H.R.F. wrote the first draft of the article in consultation with C.E.P. All authors reviewed and edited the manuscript. Ethics of human subject participation: Not applicable.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020000051




