


China has experienced a significant increase in the prevalence of obesity during recent decades( Reference Du, Sun and Yin 1 , Reference Xi, Liang and He 2 ), with increasing BMI and waist circumference (WC) over time, particularly for those at the highest BMI and WC levels( Reference Stern, Smith and Zhang 3 ). The increasing obesity epidemic has also shown gender disparities in terms of sociodemographic characteristics. For example, obesity prevalence was higher in lower educated women, but in men with higher education( Reference Gordon-Larsen, Wang and Popkin 4 ).
One of the major factors underlying the obesity epidemic is considered to be the dramatic transition in dietary intake and eating behaviours in China. Previous work has identified higher fat and sodium intakes, accompanied by increasing consumption of edible oils and animal-source foods, and prevalent snacking and eating out( Reference Zhai, Du and Wang 5 ). Typically, food away from home (FAFH) is defined as food eaten or prepared outside the home, including restaurant food, which comprises the majority of FAFH, as well as foods obtained from canteens and fixed or mobile stalls. In China, consumption of FAFH has increased substantially. The share of urban food expenditure on FAFH rose from 14·7 % in 2000 to 20·6 % in 2008( Reference Dong and Hu 6 ). A large body of literature has shown that FAFH consumption is associated with high intakes of energy and saturated fat, and low micronutrient intakes( Reference Bezerra, Junior and Pereira 7 – Reference Lachat, Nago and Verstraeten 10 ).
Meanwhile, other studies in developed countries have reported a relationship between increased FAFH consumption and higher BMI or risk of obesity, which varied by away-from-home location( Reference Duffey, Gordon-Larsen and Jacobs 11 – Reference Larson, Neumark-Sztainer and Laska 13 ). However, most previous studies focused on the association of FAFH with weight-related indicators evaluated at the mean level, which do not take into account different conditions across the entire distribution of weight-related indicators. For example, the extent of the association between FAFH and BMI or WC for individuals at the bottom quantiles may differ from that for individuals at the upper quantiles( Reference Kim, Lee and Han 12 ). It is especially unclear how FAFH consumption affects body weight outcomes across the distribution among Chinese adults when considering the gender difference.
The present study explored gender disparities in the associations between FAFH consumption and two body weight outcomes among Chinese adults aged 18–60 years, using the latest cross-sectional data from a large-scale cohort study, in order to depict the role of FAFH in the growing prevalence of obesity in a developing country.
Methods
The data used in the present study were drawn from the 2011 China Health and Nutrition Survey (CHNS), which is a longitudinal, household-based study that began in 1989( Reference Zhang, Zhai and Du 14 ). The CHNS included eight or nine diverse provinces differing in terms of economic development and geography in the first eight waves (1989, 1991, 1993, 1997, 2000, 2004, 2006, 2009) and an additional three megacities (Beijing, Shanghai, Chongqing) in the latest 2011 wave. A multistage cluster random sampling method was used to derive the original sample. Counties in each province were stratified by income (low, middle and high) and a weighted sampling scheme was used to randomly select four counties. In addition, the capital and a lower-income city of a province were selected when feasible, except that other large cities rather than capitals had to be selected in two provinces. Four villages and townships within the counties and urban/suburban neighbourhoods within the cities were selected randomly. Twenty households were selected randomly in each candidate community. Dimensions of data collected in the CHNS included demographics, socio-economics, diet, physical activity and health from individual, household and community levels. Details of the project are described elsewhere( Reference Popkin, Du and Zhai 15 ).
Our analysis included non-pregnant individuals aged 18–60 years in the 2011 survey with complete dietary records and weight, height and WC measurements. Participants who reported having been diagnosed with non-communicable chronic diseases were excluded because they may have strict limitations on eating behaviours and weight control (n 837). A final sample of 7738 adults (3604 males and 4134 females) was available.
The CHNS provided detailed individual food intake information through in-person interviewer-administered 24 h recalls conducted by trained staff over three consecutive days, including two working days and one weekend day. For each ingredient of foods consumed in the period, details were collected on the amount consumed, the time of the meal, dining place, and preparation method and location. The energy and nutritional contents of reported food items were coded according to the China Food Composition Table. Household condiment consumption was determined by examining changes from the beginning to the end of each day during the aforementioned 3 d. All condiments (including edible oils) remaining after the last meal before initiation of the survey were weighed and recorded. Condiments brought into the household unit and wasted were estimated in the next 3 d. At the end of the dietary survey, all remaining condiments were again weighed and recorded. The number of household members and visitors was recorded at each meal across 3 d. Energy intake from condiments was divided among members and visitors by proportion of total food intake in households. Total energy intake was summed as energy from individual reported foods and energy from weighed household condiments, mainly cooking oil. All food items in a mealtime that were prepared away from home regardless of dining place were defined as FAFH( Reference Guthrie, Lin and Frazao 8 , Reference Lin, Wendt and Guthrie 16 , Reference Adair and Popkin 17 ). In the present study, FAFH specifically referred to food prepared at restaurants, including fast-food restaurants, full-service restaurants and outdoor fixed food stalls. Food prepared at friends’ or relatives’ home was counted as food at-home consumption. Then we calculated energy from total FAFH and derived the percentage of energy intake from FAFH.
Field-measured height, weight and WC were used for analysis. BMI was calculated as weight divided by squared height (kg/m2). Anthropometric measurements were conducted by trained local staff according to protocols of the WHO( Reference Shankar 18 , Reference Wang, Du and Zhai 19 ). We used a stadiometer (SECA 206) and electronic weight scales (SECA 882) for height and weight measurement, respectively. A measuring tape was used for WC measurement.
Demographic, socio-economic, diet and lifestyle variables were controlled in the models as covariates, including age (years), highest level of education attained (primary school and below=0, junior school=1, senior school and above=2), per capita annual household income level (low tertile=0, middle tertile=1, high tertile=2), urbanization level of resident community (low tertile=0, middle tertile=1, high tertile=2), daily energy intake (kJ/day), current smoking (yes/no), drinking alcohol over the last year (yes/no) and work-related moderate-to-vigorous physical activity (yes/no). The information was collected by questionnaire survey on individual, household and community levels. More definitions of above variables can be found on the website (http://www.cpc.unc.edu/projects/china/data/questionnaires).
Descriptive analyses were conducted to investigate the distribution of main variables. According to the multilevel characteristics of eating behaviours and body weight outcomes, we performed series of quantile regression models for continuous BMI and WC for males and females, respectively, to investigate the varied impacts of percentage of energy from FAFH on different quantiles of body weight outcomes. In model 1, we only included percentage of energy from FAFH in the quantile regression model to investigate the association with BMI/WC. Model 2 controlled for additional individual variables (age, total energy intake, education level, smoking, drinking and moderate-to-vigorous physical activity). Model 3 additionally included the household variable (per capita annual household income level); model 4 controlled for the community variable (urbanization level) besides aforementioned covariates. All statistical analyses were performed using the statistical software package SAS version 9.2. The quantile regression was estimated using the PROC QUANTREG procedure.
Results
Summary statistics of variables used in the present study are presented in Table 1. Mean and median values for continuous variables and percentages for category variables are shown. The average BMI and WC was 23·6 kg/m2 and 82·6 cm in the participants, mean age 42·9 years, respectively. The energy attributed to FAFH was 1357 kJ/d (324·4 kcal/d) in total, 1624 kJ/d (388·1 kcal/d) in males and 1124 kJ/d (268·7 kcal/d) in females, which contributed 15·4 % to total dietary energy intake in total, 16·9 % in males and 14·2 % in females.
Table 1 Demographic characteristics of the sample of non-pregnant individuals aged 18–60 years, China Health and Nutrition Survey 2011

FAFH, food away from home.
The estimates for FAFH consumption in the distribution of BMI are shown in Fig. 1. For males (Fig. 1(a)), the quantile regression coefficients for the percentage of energy from FAFH across all BMI quantiles were statistically significant. For females (Fig. 1(b)), significant coefficients for the percentage of energy from FAFH were observed only at the 10th, 25th, 90th and 95th BMI quantiles. Moreover, the increases in BMI were higher at the upper v. the lower end of the BMI distribution, indicating that heavier males and females got larger increases in BMI with an additional percentage of energy from FAFH, compared with individuals with lower body mass. Increases in BMI attributed to an additional percentage of energy from FAFH across the quantiles were 0·01–0·03 kg/m2 in males and 0·01–0·02 kg/m2 in females.

Fig. 1 Association between percentage of energy from food away from home (FAFH) and BMI in quantile regression model, according to gender (a, males; b, females), among non-pregnant individuals (n 7738) aged 18–60 years, China Health and Nutrition Survey 2011. The solid line represents the quantile estimates; the grey area surrounding the solid line represents the 95 % confidence interval for the estimates. All models controlled for age, total energy intake, education level, household income, urbanization level, smoking, drinking and moderate-to-vigorous physical activity
The quantile regression estimates for FAFH consumption in the distribution of WC are displayed in Fig. 2. For males (Fig. 2(a)), similar to the findings for BMI, we observed a significant increase in WC with additional FAFH consumption across all WC quantiles. For females (Fig. 2(b)), the quantile regression coefficients for FAFH consumption at the 5th, 10th, 25th and 75th WC quantiles were statistically significant. However, significant associations were not observed at the other quantiles. The increases in WC were higher at the lower than the upper end of the WC distribution, indicating that females with lower WC experienced larger increases in WC with an additional percentage of energy from FAFH, compared with individuals with higher WC.
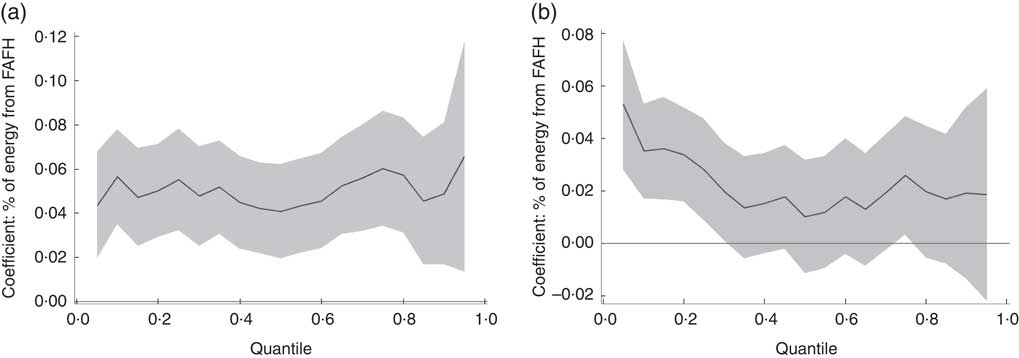
Fig. 2 Association between percentage of energy from food away from home (FAFH) and waist circumference in quantile regression model, according to gender (a, males; b, females), among non-pregnant individuals (n 7738) aged 18–60 years, China Health and Nutrition Survey 2011. The solid line represents the quantile estimates; the grey area surrounding the solid line represents the 95 % confidence interval for the estimates. All models controlled for age, total energy intake, education level, household income, urbanization level, smoking, drinking and moderate-to-vigorous physical activity
Adjusted associations between FAFH consumption and body weight outcomes in males and females were estimated, respectively, using quantile regression, as shown in Table 2. In general, the effects of FAFH on body weight outcomes were weaker for females than males. The extent of the association was larger for WC than for BMI in both genders across the entire distribution. The regression estimates generally increased with the outcomes’ quantiles, except for WC in females, which demonstrated a decreasing trend by quantiles. In the context of our findings, an additional 10 % of energy from FAFH will result in an increase of BMI of 0·08 to 0·31 kg/m2 and an increase in WC of 0·41 to 0·66 cm across the entire quantiles for males (P<0·05); while in females the corresponding values are 0·12 to 0·25 kg/m2 increment in BMI and 0·26 to 0·53 cm increment in WC at the lower and middle-upper quantiles (P<0·05).
Table 2 Quantile regression estimatesFootnote † for the association between percentage of energy from food away from home (FAFH) and body weight outcomes, according to gender, among non-pregnant individuals (n 7738) aged 18–60 years, China Health and Nutrition Survey 2011

*P<0·05, **P<0·01.
† Model 1 included percentage of energy from FAFH in the quantile regression model to investigate the association with BMI/waist circumference; model 2 controlled for individual variables (age, total energy intake, education level, smoking, drinking and moderate-to-vigorous physical activity); model 3 controlled for an additional household variable (per capita annual household income level), based on model 2; model 4 controlled for an additional community variable (urbanization level), based on model 3.
Discussion
The current study evidenced the different associations by gender between FAFH consumption and BMI or WC in adults using data from China Health and Nutrition Survey 2011. In addition, the heterogeneity of the association of FAFH consumption with the body weight outcomes across the entire conditional distribution of BMI and WC was also observed.
Our results concurred with previous studies that showed higher FAFH consumption may play an important role in the current obesity epidemic for adults. Away-from-home eating has been shown to be characterized by high energy and fat intakes, especially saturated fat, along with low micronutrient intakes( Reference Bezerra, Junior and Pereira 7 – Reference Orfanos, Naska and Trichopoulou 9 , Reference Bezerra, de Moura Souza and Pereira 20 , Reference Gorgulho, Fisberg and Marchioni 21 ), which could explain why more FAFH consumption increases the body weight indicators. A national survey among Korean adults reported that heavy FAFH consumption (obtaining ≥5858 kJ (≥1400 kcal) from FAFH per day), specifically at full-service restaurants, was significantly related to higher BMI and WC, in which larger associations were found at higher quantiles( Reference Kim, Lee and Han 12 ). Other studies also have shown that frequent away-from-home meals were related to higher body weight outcomes, such as BMI, WC and weight, or higher risk of becoming overweight/obese( Reference Duffey, Gordon-Larsen and Jacobs 11 , Reference Kant, Whitley and Graubard 22 – Reference Fulkerson, Farbakhsh and Lytle 24 ). Building on the previous literature in developed countries, the present study explored more evidence on gender disparities in the association between FAFH consumption and body weight outcomes using data from China, which could help understanding the effects of nutrition transition on human health in developing countries. As a phenomenon of socio-economic development, eating at restaurants is becoming more popular than in past decades and is beginning to play an important role in the modern diet( Reference Bezerra, de Moura Souza and Pereira 20 , Reference Kant, Whitley and Graubard 22 , Reference Bezerra, Souza Ade and Pereira 25 – Reference Mehta and Chang 28 ). Restaurant foods provided 15·4 % of total energy in the present study, which showed positive associations with higher BMI and WC for Chinese adults.
We found that the associations between FAFH consumption and body weight outcomes were different by gender. Overall, the quantile regression results demonstrated that more FAFH was significantly associated with higher body weight outcomes among males, while the association was not always significant among females throughout the distribution of both outcomes. Our findings further indicated that the magnitude of the association appeared to be larger for males than for females.
Gender disparities in BMI and obesity were reported in previous studies, which illustrated that socio-economic factors may induce more effects on men than women( Reference Plurphanswat and Rodu 29 , Reference Ouyang, Wang and Su 30 ). Other studies demonstrated that multifaceted causes may contribute to the gender differences in FAFH consumption and body weight outcomes. For example, changes in food prices and income account for half of weight gain for males, but only a small fraction for females( Reference Buttet and Dolar 31 – Reference Han and Powell 33 ). Meanwhile, gender norms set different roles in the household and status in society. The literature reports that male, unmarried, employed, higher-educated and high-income individuals consume more meals away from home( Reference Kwon and Ju 34 ). On the other hand, women take more responsibilities in caring for the family in China, which makes them eat out less often than men. Furthermore, females usually prefer to control weight and choose relatively healthy foods when eating out, which may explain the limited association between FAFH consumption and body weight outcomes for females.
Previous studies showed that individuals at high percentiles of the BMI distribution have a greater increase in BMI induced by FAFH than those at low percentiles( Reference Ouyang, Wang and Su 30 , Reference Razak, Corsi and Subramanian 35 ). Our results also indicated that the associations between FAFH and body weight outcomes showed higher magnitude in the upper tail of the BMI distribution for both genders. Inconsistent with a Korean study, which found that heavy FAFH consumption had overall larger associations with both BMI and WC at higher quantiles( Reference Kim, Lee and Han 12 ), however, the present study indicated the similar finding only on BMI among Chinese adults. Furthermore, FAFH played smoothly positive effects on the entire distribution of WC for males, while it played stronger effects at the lower tail of the WC distribution for females. Relative to FAFH, other demographic and lifestyle variables may largely contribute to the increase in WC in females at the upper tail of the WC distribution. For the two outcomes, FAFH indicated a larger influence on WC than on BMI among both genders. The findings imply that FAFH consumption may increase the risk of larger BMI and WC for Chinese adults, which are established as harmful factors for non-communicable chronic diseases.
Our study has several limitations. First, although the sample included twelve provinces in China covering a wide demographic distribution, the cross-sectional data from CHNS used in present study are not nationally representative; therefore, extrapolated conclusion should be made cautiously. It is also important to note that the cross-sectional analysis does not allow assessment of the causal relationship of FAFH consumption with body weight outcomes. Second, the dietary data were drawn mainly from self-reported detailed dietary recall and in-household weighing, which may not include cooking oil intake when eating away from home and thus may underestimate energy from FAFH. Therefore, the extent of the positive association of FAFH consumption with body weight outcomes may be also underestimated in the present study. Lastly, unlike other studies conducted in Western countries, fast foods are not prevalent in China, so we combined all restaurant foods into one category in the study, which may weaken the heterogeneity of associations of FAFH consumption in different types of restaurant with body weight outcomes.
The present study fills a gap in the literature concerning different associations between FAFH consumption and body weight outcomes in the conditional distribution by estimating quantile regression models among Chinese adults, revealing potential implications for public health policy making.
Conclusions
In summary, our study highlights the different associations of FAFH consumption with body weight outcomes among Chinese adult men and women. Males are more likely affected by FAFH than females, as a result having higher BMI and WC. More FAFH consumption may result in higher BMI and WC among Chinese adults, with heterogeneity across the distribution of body weight outcomes. Our results imply that efforts considering these gender disparities should be made to promote healthy food choices when eating away from home. These initiatives will help the public to respond effectively to challenges from the away-from-home food environment and the consequent health risk.
Acknowledgements
Acknowledgements: This research used data from the China Health and Nutrition Survey (CHNS). Financial support: The authors thank the National Institute for Nutrition and Health at the Chinese Center for Disease Control and Prevention, the Carolina Population Center (grant number 5 R24 HD050924), the University of North Carolina at Chapel Hill, the US National Institutes of Health (NIH; grant numbers R01-HD30880, DK056350, R24 HD050924 and R01-HD38700) and the Fogarty International Center, NIH, for providing financial support for the CHNS data collection and analysis of files from 1989 to 2011 and future surveys. The research was also supported by a research grant from the NIH (grant number 1U54 HD070725-01), the Eunice Kennedy Shriver National Institute of Child Health & Human Development, and the Office of Behavioral and Social Sciences Research. It is part of the collaboration project between the National Institute of Nutrition and Health at the Chinese Center for Disease Control and Prevention and the University at Buffalo, State University of New York. The funders had no role in the design, analysis or writing of this article. Conflict of interest: All the authors declare no conflict of interest. Authorship: B.Z. conceived and supervised the study. W.-W.D., H.-J.W. and C.S. analysed and interpreted data. W.-W.D. drafted the manuscript and Z.-H.W., J.-G.Z., J.Z., X.-F.J. and H.-R.J. revised it. All authors approved the final version of the manuscript. Ethics of human subject participation: This research has been approved by the Institutional Review Committees of the University of North Carolina at Chapel Hill and the National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention. All subjects gave written informed consent for their participation in the survey.




