



The high prevalence of chronic undernutrition and nutritional deficiencies observed in indigenous populations in Brazil is a hallmark of the social and nutritional inequalities in the country(Reference Coimbra, Santos and Welch1,Reference Horta, Santos and Welch2) . The First Brazilian National Survey on Indigenous People’s Health and Nutrition (2008–2009) revealed that 26 % of children under 5 years of age were stunted and that 51 % had anemia(Reference Horta, Santos and Welch2). Nevertheless, recent studies have shown that short stature in relation to age affects more than 80 % of Yanomami children, thus revealing severe vulnerability and a nutritional deficiency in this population(Reference Pantoja, Orellana and Leite3,Reference Orellana, Marrero and Alves4) .
Such problems result not only from the difficulty of producing or acquiring food but also from the historical violation of basic rights, precarious socio-economic conditions and land conflicts(Reference Alves5). Traditionally, the Yanomami are considered hunters and gatherers(Reference Albert6,7) ; however, the regular presence of invaders (especially loggers and prospectors) on their traditional territory drastically affects the areas used for hunting, fishing and gathering and, consequently, the availability and variety of the native food sources(Reference Pontes8,Reference Ramos, Abrahão and Rodrigues9) , thus causing scarcity of these items(Reference Pontes8,Reference Ramos, Abrahão and Rodrigues9) . Even without previous authorisation, some villages have been obliged to live with non-indigenous people from different parts of Brazil, including representatives of the Brazilian State as well as other kinds of invaders in their traditional territories. Among other consequences, this forced interaction has created a local scenario of socio-environmental vulnerability and has exposed almost all families, especially children, to the consumption of industrialised products and ultra-processed foods of low nutritional value, which are high-energy-dense, low in fibre and micronutrients and rich in preservatives and industrial additives(Reference Coimbra, Santos and Welch1,7,Reference Leite10) . Currently, the foods that mainly contribute to the energy intake of the Yanomami are acquired in regional markets, especially rice, tubers, beans, manioc flour and fruits(Reference Leite10).
Previous studies carried out with indigenous children from Latin America have provided data on nutritional status, though with limited information on dietary indicators(Reference Gatica-Domínguez, Mesenburg and Barros11–Reference Maciel, Coca and Castro14). There are a few studies that have been carried out with indigenous children in Brazil that have reported monotonous diets(Reference Mattos, Morais and Rodrigues13,Reference Maciel, Coca and Castro14) that are quantitatively below nutritional needs(Reference Serafim15,Reference Ribas, Sganzerla and Zorzatto16) and which contain a substantial presence of ultra-processed foods, such as soft drinks made from powder, soda, candy, bread, cookies, artificial juice, artificial yogurt, canned foods and instant noodles(Reference Maciel, Coca and Castro14,Reference Ribas, Sganzerla and Zorzatto16) , thus indicating the importance of more profound studies on this topic.
Evidence of a nutritional transition in Brazilian non-indigenous children between 6 and 59 months of age has revealed a consumption at least once a week of cookies, soft drinks and snacks(Reference Bortolini, Gubert and Santos17). A systematic review that included thirty-one studies that evaluated the diet of Brazilian children under 7 years of age concluded that the diet of this population was characterised by a high consumption of fried foods, soft drinks, sweets and salt(Reference Mello, Barros and Morais18). No previous research on the food profile has been conducted on Yanomami children who live in isolated areas in the rainforest where there is limited contact with non-indigenous society.
Since the central and transformative promise of the 2030 Sustainable Development Goals Agenda is to ‘leave no one behind’(19) and, in order to fill an important gap in the literature and show the vulnerable situation in which Yanomamis live, we aimed to characterise the food profile of indigenous Yanomami children aged from 6 to 59 months, according to the degree of food processing and to investigate its association with socio-economic, demographic, maternal and anthropometric factors. Our hypothesis is that Yanomami indigenous children living in regions in close contact with non-indigenous society consume more ultra-processed foods when compared with those living without contact with non-indigenous society.
Methods
Study area and population
In the extreme north of Brazil, the Yanomami population is of approximately 27 000 individuals, who are distributed in more than 300 villages that are located in an area of 9 664 975 hectares(Reference Magalhães and Cavalcanti20), which is known as the Yanomami Indigenous Territory. The current study was carried out in two administrative regions: (i) Auaris, which is located in the extreme north of the state of Roraima, with access exclusively by air from the state capital, Boa Vista and (ii) Maturacá, situated in the state of Amazonas, with access by air from Boa Vista, or by a combined land and boat trip from the municipality of São Gabriel da Cachoeira, Amazonas (Fig. 1). In the Auaris region, eight small villages (Koronau, Kolulu Guarape, Traira/Auaris Posto, Katimani, Amonokomaú, Grabi-I, Polibi and Laranjeira) were included. In the Maturacá region, two large villages (Ariabú and Maturacá) were included. For this reason, in the present study, three strata of comparison were used.

Fig. 1 Map of the Yanomami indigenous territory, Brazilian Amazon
Sample design and selection
This is a cross-sectional study based on a census of indigenous children under 5 years of age that was conducted between December 2018 and February 2019. Households with children under 5 years of age and their respective mothers/guardians were invited to participate in the current study. Initially, 304 children under 5 years of age comprised the sample. As complementary feeding is recommended at 6 months of age, we excluded fifty-three children under 6 months of age. The final sample consisted of 251 children aged 6 to 59 months: 39 % from Maturacá, 33 % from Ariabú and 28 % from Auaris.
Data collection
Trained researchers conducted the interviews with mothers/guardians of children under 5 years of age during home visits and applied a structured questionnaire and took anthropometric measurements. When necessary, the interviews were simultaneously translated from Portuguese into the predominant language of the region, with the support of native interpreters.
Food profile
The food profile was established by using a pre-structured questionnaire composed of a list of foods in order to verify the child’s consumption of these foods on the day preceding the interview. This questionnaire consisted of a list of thirty-four food items with objective questions (yes/no) for each of them, in addition to an item ‘others’ for the inclusion and description of foods not included in the list. The food list was elaborated after a formal planning meeting with anthropologists, nutritionists and health professionals who have long experience working in the target communities. This list was pre-tested with a group of Yanomami women and their children in Boa Vista, the capital of Roraima state, as well as with selected Yanomami leaders in the month preceding the field work. The thirty-four food items are presented in Table 1.
Table 1 List of the thirty-four food items that composed the food questionnaire applied to indigenous children aged 6 to 59 months. Yanomami indigenous territory, Brazil, 2018–2019
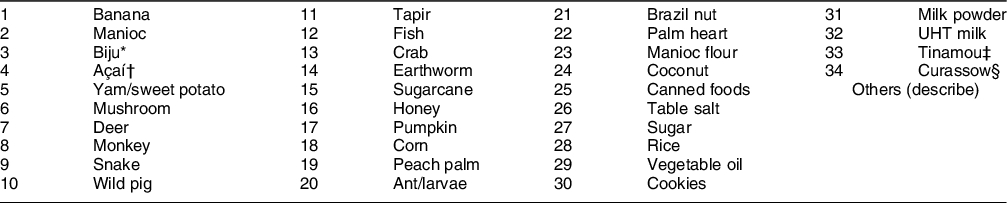
* Biju is a starch flat cake made with manioc flour that is typical of indigenous of Amazon region.
† Brazilian fruit predominantly grown in the Amazon region, rounded, with a dark colour, ranging from purple to black, it grows in bunches and, predominantly, in places with more humid or flooded soils.
‡ Small-billed tinamou is a bird from the Amazon region, similar to the guinea fowl, brown in colour, it has a meat that is much appreciated, especially by the indigenous people.
§ A gallinaceous bird native to the forests of Central and South America, with a well-developed crest and black plumage with yellow (male) or brown or reddish tones (female).
Using the NOVA system(Reference Monteiro, Cannon and Levy21), the foods consumed were classified in the following manner according to their degree of processing: in natura or minimally processed foods (e.g. fruits, vegetables, meats and beans), processed culinary ingredients (e.g. vegetable oil, salt and sugar), processed foods (e.g. canned foods, processed meats and bread) and ultra-processed foods (food products designed to create low cost, long shelf-life, convenient and hyperpalatable products, e.g. chocolate powder, artificial juice, soft drink and noodles). In natura or minimally processed foods were subdivided into two groups: ‘regional’ (of indigenous preparation or food available naturally in the village/forest) or ‘urban’ (food from the city that is available in small food markets in the community and/or exchanges with non-indigenous people working in the villages). Honey and pepper are usually classified in the urban environment as processed culinary ingredients. Due to the way in which it is obtained and consumed among indigenous people, it was included in the group of in natura or minimally processed foods.
Anthropometric assessment
Birth weight was obtained by consulting the birth certificate, child health booklets, vaccination cards or by consulting the demographic module of the Indigenous Health Care Information System. Children born with < 2500 g were classified as low birth weight(22).
Maternal and infant anthropometric data (weight and length/height) were collected according to the techniques recommended by the Brazilian Ministry of Health(23). To measure the weight in kilograms of children with the ability to stand and their mothers, a portable digital scale (Seca®, model 877) with a maximum capacity of 150 kg and precision of 0·1 kg was used. For infants, the mother–infant function was used, in which the baby was weighed on the mother’s lap and the mother’s weight was subtracted from the mother–infant weight.
The stature of children aged over 24 months and their mothers was measured using a vertical stadiometer (Alturexata®, 213 cm total extension, 1 mm precision). Children aged 24 months or less were measured in dorsal decubitus using an infantometer (Alturexata® 108 cm total extension, 1 mm precision). Children were classified as stunted and adolescent mothers of short stature if they had Z-scores of length/height-for-age < 2 SD from the median reference population, according to the WHO(24). For adult mothers (>19 years), the cut-off point for short stature was <145 cm(25).
The nutritional status of the children was evaluated as height-for-age and BMI-for-age in Z-scores, calculated using WHO AnthroPlus® software. The cut-off points established by the WHO(24) were considered.
Socio-economic, demographic, maternal and infant characteristics
The following socio-economic and demographic characteristics were considered and were categorised as follows: regular income (yes/no), conditional cash transfer program – Bolsa Família (yes/no), availability of a place for purchases of food in the community (yes/no), place of residence (Auaris/Maturacá/Ariabú) and number of residents in the household (≤9/≥10 people).
Regarding maternal characteristics, the following variables were considered and classified as follows: marital status (with partner; without partner), age (≤19/20–29/≥30 years) and short stature (yes/no).
The children’s characteristics and the variables of nutritional status were classified as follows: sex (male/female), age (6–23/24–59 months), birth weight (<2500/≥2500 g), stunted (no/yes) and BMI-for-age (thin/normal weight/risk of overweight/overweight/obesity).
Statistical analyses
Absolute and relative frequencies were estimated according to socio-economic and demographic characteristics, maternal and infant characteristics, as well as food profile. Considering the particularities of feeding in childhood, the analyses were stratified by age group (6–23/24–59 months). The frequency of consumption of each food group (‘regional’ in natura or minimally processed, ‘urban’ in natura or minimally processed, processed and ultra-processed) was estimated according to socio-economic, demographic, maternal and child variables, with respective 90 % CI. Pearson’s χ 2 or Fisher’s exact tests were used to verify differences in the proportions of the food groups between the categories of each of the variables.
Due to changes in the dietary patterns of children in Brazil, as well as the negative impacts of ultra-processed food consumption on health(Reference Lane, Davis and Beattie26), the analyses were focused on the factors associated with the consumption of ultra-processed foods. Poisson regression analysis with robust variances was applied to estimate the crude and adjusted prevalence ratios with a 90 % CI. Variables with P-values <0·20 in the bivariate analysis were included in the multivariate analysis, considering a probability <10 % as a level of statistical significance in the final model. Since the study was based in hard-to-reach areas in the Brazilian Amazon with a small sample size, P-values of 0·10 were adopted to capture any potential association that due to small sample size would be disconsidered if a P-value of 0·05 was used. Furthermore, it is worth remembering that we carried out a census in the investigated villages and that all children under 5 years of age were included in the study. Data were analysed using Stata 14.0 software (StataCorp.).
Results
Of the 251 children investigated, approximately 51 % were male and 73 % were between the ages of 24 and 59 months. Prevalence of low birth weight was 11 %. The overall prevalence of stunting was 91 %, of which 19 % were stunted and 72 % severely stunted. In general, the children had a normal BMI-for-age (77 %). Regarding maternal characteristics, most of the mothers (54 %) were between 20 and 29 years of age, had a short stature (73 %) and lived with a partner (91 %). Most households comprised up to nine residents (66 %) and were in the vicinity of small food markets (84 %). More than half of the families had no regular income (56 %) and did not participate in any government cash transfer program (59 %) (Table 2).
Table 2 Socio-economic, demographic, maternal and individual characteristics of indigenous children aged 6 to 59 months living in villages of the Yanomami indigenous territory, Brazil, 2018–2019 (n 251)

* 10 data missing.
† 8 data missing.
‡ 15 data missing.
§ Maternal short stature cut-off: Z-score ≤ -2 (women aged ≤ 19 years) and stature ≤ 145 cm (for women aged 19 years or more).
‖ 4 data missing.
¶ 5 data missing.
** 40 data missing.
†† 4 data missing.
‡‡ 3 data missing.
The items most reported in the group of in natura or minimally processed ‘regional’ foods were fruits (69 %), corn, roots or tubers (45 %); peach palm or palm heart (33 %); fish or crab (33 %) and biju or couscous (32 %). Among ‘urban’ foods, the most reported were black beans (29 %), rice or pasta (19 %), chicken (17 %), coffee or coffee with milk (15 %) and powdered cow’s milk (10 %). The most frequently reported ultra-processed foods were cakes or cookies (25 %) and chocolate or chocolate powder (6 %) (Table 3).
Table 3 Frequency of food consumption according to the degree of food processing of indigenous children aged 6 to 59 months living in villages of the Yanomami indigenous territory, Brazil, 2018–2019 (n 251)

* Pineapple, açaí, banana, cocoa, coconut, cupuaçu, guava, ingá (Inga edulis), orange, watermelon, passion fruit and tucumã (Astrocaryum aculeatum).
† Corn, manioc and yam/sweet potato.
‡ Tapir, snake, agouti, monkey, curassow, small-billed tinamou, paca, wild pig, toad and deer.
§ Breast milk, vegetables and legumes, ant or larvae, honey, natural fruit juice, earthworm, pepper, vegetable/fish broth and Brazil nut.
‖ Beef or egg soup, oatmeal.
Consumption of ‘regional’ in natura or minimally processed foods and processed culinary ingredients was significantly higher among children ≥23 months. Consumption of ‘urban’ in natura or minimally processed, processed and ultra-processed foods was significantly higher in children from Maturacá and Ariabú (Table 4). Prevalence of ‘urban’ in natura or minimally processed foods, culinary ingredients, processed and ultra-processed foods was significantly higher in children of households with beneficiaries of the Bolsa Família cash transfer program and those who live in households near to small food markets. Prevalence of ‘urban’ in natura or minimally processed, processed and ultra-processed foods was significantly higher in children of mothers of adequate stature. Children with adequate birth weight had a higher prevalence of consumption of ‘urban’ in natura or minimally processed foods. Children of mothers without a partner had a significantly higher consumption of processed foods (Table 4).
Table 4 Prevalence and associations of food consumption according to the socioeconomic, demographic, maternal and individual characteristics of indigenous children aged 6 to 59 months living in villages of the Yanomami indigenous territory, Brazil, 2018–2019 (n 251)

P value refers to Poisson regression test.
In the adjusted analysis, place of residence and maternal short stature remained associated with the consumption of ultra-processed foods. The prevalence of ultra-processed food consumption was 11·6 times higher in Maturacá and 9·2 times higher in Ariabú when compared with Auaris. Ultra-processed food consumption was 31 % lower among children whose mothers had short stature than among children of mothers with adequate stature (Table 5).
Table 5 Crude and adjusted analysis of the association between consumption of ultra-processed foods and characteristics of indigenous children aged 6 to 59 months living in villages of the Yanomami indigenous territory, Brazil, 2018–2019 (n 251)
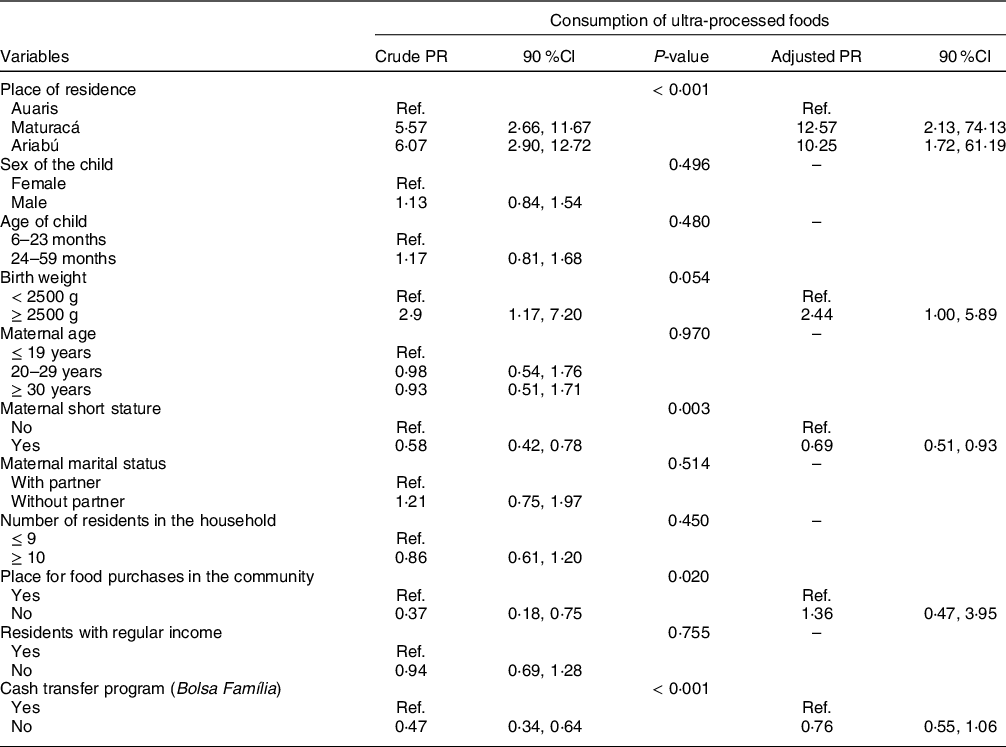
P value refers to Poisson regression test.
Discussion
The current study presents unprecedented information on the food profile of the Yanomami indigenous children. There was a high prevalence of consumption of ‘regional’ (93 %) and ‘urban’ (56 %) in natura or minimally processed foods. The overall prevalence of ultra-processed foods was 32 % and was associated with the place of residence and maternal stature. Moreover, a huge proportion of the children was stunted.
Few studies have been dedicated to assessing the diet consumption of Brazilian indigenous children. The First Brazilian National Survey on Indigenous People’s Health and Nutrition(Reference Horta, Santos and Welch2), for example, evaluated only the acquisition of food and the food profile of the family/household without detailing the food consumption of the child(Reference Welch, Ferreira and Souza27). Mattos et al. (Reference Mattos, Morais and Rodrigues13) reported that indigenous children from the Alto Xingu River (Brazilian mid-western region) had manioc porridge, watermelon, fruit and fish as their food base. However, Ribas et al. (Reference Ribas, Sganzerla and Zorzatto16) revealed a diet consisting primarily of rice, manioc, sugar and meat with a high fat content among Terena indigenous children under 5 years of age. More recently, Silva et al. (Reference Silva28) observed that the dietary intake of children under 5 years of age from Karapotó (Brazilian Northeastern region) was similarly monotonous and based on rice, sugar, powdered milk and beans.
The presence of ultra-processed foods in the diet of the Brazilian indigenous children has also been described by other authors(Reference Maciel, Coca and Castro14,Reference Ribas, Sganzerla and Zorzatto16,Reference Silva28,Reference Silva29) . Studies conducted prior to the publication of the NOVA system did not use the term ultra-processed. Nonetheless, it is possible to infer the presence of ultra-processed foods in these previous studies because of the description of items consumed. Maciel et al. (Reference Maciel, Coca and Castro14), when evaluating the indigenous people of Acre (northern region of Brazil), reported a frequency of 52·6 % and 28·6 % consumption of ultra-processed foods in children aged 6–12 months and 13–23 months, respectively. Silva et al. (Reference Silva28) reported a frequency of consumption of 33 % frankfurters, 31 % instant noodles and 27 % soft drinks among Karapotó children under 5 years of age. Ribas et al. (Reference Ribas, Sganzerla and Zorzatto16) also observed the presence of ultra-processed foods, such as powdered soft drinks, soft drinks, candies and cookies, in the diet of Terena indigenous children. Silva et al. (Reference Silva29) noted the presence of cookies, sweets, snacks and chocolates in the diet of indigenous children from São Paulo (southeastern region of Brazil).
Previous studies suggest that the country is experiencing a transition in the eating habits of Brazilian indigenous children(Reference Maciel, Coca and Castro14,Reference Welch, Ferreira and Souza27) . Traditionally, the diet of these children consisted predominantly of in natura foods that are available in the forest; however, there is growing access to processed foods as a result of the contact with non-indigenous population(Reference Eloy30). In a study conducted with Ecuadorian children who live in the Amazon region, high consumption of processed/ultra-processed foods was associated with a higher percentage of body fat in children(Reference Urlacher, Snodgrass and Dugas31).
The prevalence of consumption of ultra-processed foods in our study was higher among children in the regions of Maturacá and Ariabú when compared with those of Auaris. Despite the geographical isolation of Yanomami indigenous communities, this can be explained by the fact that these locations have relatively easier access to urban centres, while in the Auaris region, access is more difficult and costly, since all trips are by air(Reference Basta and Orellana32). In contrast, the Auaris region has a higher frequency of cultivation and collection of wild foods than Maturacá and Ariabú(Reference Basta and Orellana32,Reference Lizot33) .
Our results also showed an association between the consumption of ultra-processed foods and maternal stature. The high prevalence of short stature in mothers (73 %) indicates the previous vulnerability to malnutrition to which these mothers are/were exposed. Previous studies carried out among Yanomami indigenous groups reported that they experience an ongoing intergenerational cycle of malnutrition(Reference Orellana, Marrero and Alves4,Reference Orellana, Domínguez and Vaz34) . Orellana et al. (Reference Orellana, Marrero and Alves4) revealed that the risk of having a severely short stature was 2·1 times higher in children whose mothers had short stature in two distinct Yanomami regions. Our findings suggest that Yanomami families have a high degree of socio-environmental vulnerability, which results in a permanent state of food insecurity. Considering that indigenous peoples in Brazil suffer from accumulated deficits in access to public services, such as clean water, sewage treatment and healthcare, when compared with the non-indigenous population(Reference Coimbra, Santos and Welch1), it is not possible to ignore the literature that associates stunting with sanitation and subclinical illness, i.e. environmental enteric dysfunction(Reference Budge, Parker and Hutchings35), diarrhoea(Reference Escobar, Coimbra and Welch36). Such conditions reduce the absorption of nutrients or make it impossible to absorb nutrients from the few foods they eat and, thus, affects their potential growth.
In a meta-analysis of individual data from low- and middle-income countries, mothers with short stature were more likely to give birth to babies that were small-for-gestational-age or preterm, confirming that the height-for-age deficit may begin at conception(Reference Kozuki, Katz and Lee37). Intrauterine growth faltering can be observed at birth, but if socio-environmental conditions continue to be precarious, such as poor quality of food intake, the growth deficit accumulates up to 2 years of age, and it is possible to observe the maximum height-for-age deficit between 2 and 5 years of age in preschool children(Reference Victora, Christian and Vidaletti38).
Furthermore, our results also showed that the consumption of ultra-processed foods was 31 % lower among children of mothers with shorter stature. In this case, the short maternal stature may be a proxy of the socio-economic disadvantages, since obtaining these ultra-processed foods requires a certain level of purchasing power. Consequently, these women did not have the opportunity to ingest energy, proteins and other nutrients in sufficient amounts to achieve adequate nutritional status from any kind of food, including ultra-processed foods.
In order to meet the SDG Goal 10 ‘Reduce inequality within and among countries’, in governmental policies for food and nutrition security, it is critical to target disadvantaged populations(Reference Mayén, Mestral and Zamora39). Additionally, to minimise the chances of increasing the participation of ultra-processed foods in the diet of indigenous children, it is essential to recognise that indigenous communities need to be given priority in public policies that promote healthy eating habits through the combination of nutritional education with the improvement of access to foods and/or social support to prevent child malnutrition. Moreover, the promotion of healthy eating habits needs to target all health care programmes for the indigenous populations, as well as provide guidance to non-indigenous people that come into contact with indigenous communities. Article 11 of the International Covenant on Economic, Social and Cultural Rights(40) of 1966 on the Rights of Indigenous Peoples recognises ‘the right of everyone to an adequate standard of living…, including adequate food, housing, and continued improvement of living conditions’ and the ‘fundamental right of everyone to be free from hunger’, including indigenous peoples. The Declaration of the Rights of Indigenous Peoples of the United Nations(41), adopted by the General Assembly in 2007, recognises and stresses indigenous rights such as provisions regarding land, natural resources and subsistence activities relevant to the realisation of their right to food.
The current study has some limitations that need to be mentioned. First, the use of a pre-structured food list, which is useful for avoiding biases in information and memory bias, limits the understanding of food variability in the community, especially considering the context of seasonality, typical in the Amazon(Reference Gatica-Domínguez, Mesenburg and Barros11,Reference Leite, Santos and Coimbra42) . However, the use of a recall method regarding their diet may not adequately capture the exposure to ultra-processed food consumption. We acknowledge that the applied food list did not contain a specific item for infant formula, and no infant formula was recorded in the open question ‘others’. Because it is a high-cost product in Brazil and is not provided by the primary care health system, the use of infant formula is unlikely in the Yanomami indigenous population. Another limitation was the use of non-validated questionnaires for the indigenous population. However, due to the immense social diversity in Brazil, it is not possible to use any data collection instrument that is validated for wide use in different ethnic groups. At the time of the current study, no valid generalised instruments had been identified to capture data on the diet of children of indigenous groups. Future research is needed to develop and validate methods for assessing indigenous dietary intake, especially that of the children. In addition, some interviews were conducted with the support of interpreters, and the possibility of misinterpretations cannot be discarded. To minimise problems, prior to the field work, all interviewers received training to standardise data collection.
The present study has important strengths. The study was designed as a census of children living in villages in three difficult-to-access regions in the Brazilian Amazon and contributes with data on this specific and underrepresented group. Due to geographic isolation, the studied villages may spend months without receiving visits from the health teams. Therefore, increasing our knowledge of the health situation in these locations is essential. Furthermore, the way data were collected allowed the application of the NOVA system to classify foods and identify factors associated with the consumption of ultra-processed foods.
Finally, despite the high consumption of in natura and minimally processed foods among Yanomami indigenous children, the consumption of ultra-processed foods was also high and was associated with the area of residence as a proxy for access to food from contact with people of the non-indigenous population and with mothers of adequate stature. The current study also emphasises the need for culturally acceptable programmes and interventions that promote complementary food education actions for families with chronic nutritional deficits, especially in areas close to indigenous territories, and consumer protection policies that guarantee consumers information on the harmful effects of the consumption of ultra-processed foods(Reference Costa, Del-Ponte and Assunção43,Reference Costa, Rauber and Leffa44) .
Acknowledgements
Acknowledgements: On behalf of the chiefs Davi Kopenawa Yanomami, Francisco Xavier da Silva and Floriza da Cruz Pinto which represent of Hutukara Yanomami Association (HAY), Association of Yanomami Women (Kumirãyõma) and Yanomami of Cauaburis River and Tributaries Association (AYRCA), we thank the Yanomami indigenous people for the trust placed in our team and the support in carrying out the research. We would thank Dr Cristina Albuquerque and the technical team from UNICEF Brazil for funding this research. We thank the Yanomami Indigenous Special Sanitary District (DSEI-Y) coordination, which spared no effort to support us in all stages of the fieldwork. We thank Anderson Vasconcelos, Clarisse do Carmo Jabur and Túlio Caio Binotti from National Indian Foundation (FUNAI) to the logistic and legal support. Finally, we thank the interviewers Amanda Villa Pereira, Ana Claudia Santiago de Vasconcellos, Ananda Meinberg Bevacqua, Bárbara Lopes Paiva, Cristiano Lucas de Menezes Alves, Gabriela Protázio, Maíra Posteraro Freire, Mauricio Caldart and Monique Layla Paixão Alves. Financial support: This research was funded by the United Nations International Children’s Emergency Fund (UNICEF), contract number 43246507/2018. We appreciate the Joênia Wapichana Federal Deputy for her support for publication fee costs through the parliamentary amendment number 41510004. Authorship: J.D.Y.O. and P.C.B. were responsible for designing and carrying out the study. A.O.S.M. and E.I.S.M. conducted the statistical analysis and writing of the manuscript. G.G.D., P.A.R.N. and J.S.V. contributed to the relevant critical review of the manuscript’s intellectual content. All authors reviewed and commented on writing of the manuscript and approved the final. Ethics of human subject participation: The current study was conducted in accordance with the guidelines of the Declaration of Helsinki, and the study protocol was submitted and approved by the Research Ethics Committee of the National School of Public Health and the Brazilian National Research Ethics Commission of the National Heal Council (CAAE: 91612218.8.0000.5240, Opinion # 2.896.403) Access to indigenous territory was granted by National Indian Foundation (N° 103/AAEP/PRES/2018) with prior consultation with the local leaders. The interviews and data collection were conducted after clarification of doubts, and a written consent form was obtained from all mothers/caregivers of the children’s participants in the study.
Conflicts of interest:
The authors have no conflicts of interest to disclose.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980022001306









 Open access
Open access