


Approximately 11·5 % of individuals (37·2 million people) in the USA are living with food insecurity, which the United States Department of Agriculture (USDA) defines as lack of access to enough food for an active, healthy life(Reference Coleman-Jensen, Rabbitt and Gregory1). Food insecurity often results from insufficient availability, access and/or utilisation of resources due to socio-economic or geographical barriers(Reference Barrett2). Food insecurity can manifest with or without hunger and is associated with various adverse physical correlates such as overweight, obesity, malnourishment and asthma(Reference Bhattacharya, Currie and Haider3–Reference Townsend, Peerson and Love7), as well as negative psychosocial outcomes, including poorer cognitive function, school performance and social skills(Reference Gao, Scott and Falcon8–Reference Silva, Kleinert and Sheppard10) and increased anxiety, depression and binge eating(Reference Rasmusson, Lydecker and Coffino11,Reference Hadley and Patil12) .
Researchers have studied the prevalence of food insecurity in undergraduate students, particularly in relation to poor academic achievement and low grade point average(Reference Chaparro, Zaghloul and Holck13–Reference Payne-Sturges, Tjaden and Caldeira19). Food insecurity prevalence estimates in undergraduate student samples range from approximately 13 %(Reference Hughes, Serebryanikova and Donaldson15,Reference Payne-Sturges, Tjaden and Caldeira19) to nearly 60 %(Reference Maroto, Snelling and Linck16,Reference Patton-Lopez, Lopez-Cevallos and Cancel-Tirado18) , at times drastically surpassing the national average. As Hughes and colleagues(Reference Hughes, Serebryanikova and Donaldson15) note, these estimates vary depending on the method of analysis and criteria used to determine the presence of food insecurity. Notably, even studies that report lower prevalence estimates find that an additional 5–25 % of their samples are marginally food secure or at-risk for food insecurity(Reference Chaparro, Zaghloul and Holck13,Reference Gaines, Robb and Knol14,Reference Payne-Sturges, Tjaden and Caldeira19) . These elevated rates of food insecurity indicate that a large proportion of undergraduate students are in need of additional campus-based or student resources. Many schools, such as the University of California, have begun to address this challenge by instating food pantry programmes for students and staff(Reference Jordan20).
Although cited as a public health concern for undergraduate students, the prevalence and correlates of food insecurity in graduate students are noticeably understudied. In fact, we only know of one recent study that assessed food insecurity specifically in graduate students(Reference Soldavini, Berner and Da Silva21). Soldavini and colleagues(Reference Soldavini, Berner and Da Silva21) found that 17·8 % of graduate students reported food insecurity, with an additional 20·7 % endorsing marginal food security. Rates of food insecurity in graduate students may differ from those in undergraduate students due to differing demands on and resources available to the two groups. Graduate students are typically older than undergraduate students and may have greater financial responsibilities and fewer opportunities for financial or familial assistance. For example, borrowing rates and average debt are higher among graduate students compared with undergraduate students(Reference Baum and Steele22). In many instances, graduate students need to balance a budget on a stipend or student loans while completing more extensive research and advanced classwork than their undergraduate counterparts. Research has demonstrated that graduate students work and volunteer more hours compared with undergraduate students(Reference Wyatt and Oswalt23). Furthermore, graduate students are at increased risk for negative mental health outcomes(Reference Dahlin, Joneborg and Runeson24–Reference Peluso, Carleton and Asmundson26) compared with the general population. At a large public university, Eisenberg and colleagues(Reference Eisenberg, Gollust and Golberstein25) found 11·3 % of graduate students met screener criteria for a depressive disorder and 3·8 % met screener criteria for panic disorder or generalised anxiety disorder.
The current study assesses initial prevalence estimates of food security status among graduate students and examines the relationship between food insecurity and endorsement of depression, anxiety and stress symptoms. We hypothesised that greater levels of food insecurity would be associated with more elevated levels of depression, anxiety and stress. The relationship between food security and mental health could help us better understand predictors of depression, anxiety and stress in graduate students and suggest avenues for intervention, such as increasing access to healthy food resources to reduce stress and promote mental health.
Methods
The current study was approved by the researchers’ Institutional Review Board, and participants provided consent prior to study procedures. Data were collected online from January 30, 2017 through December 19, 2017.
Participants
Participants were graduate students at a university in the northeastern region of the USA (n 263). Study inclusion criteria required participants to be (1) at least 18 years of age, (2) fluent in English and (3) a current master’s or doctoral student at the university. All participants were recruited via the university’s graduate student association email listserv and were invited to complete a 15–20 min survey to assess unmet needs of graduate students and determine areas that may influence their education experience. Participants provided information on demographic variables, programme satisfaction, utilisation of campus resources, need for additional resources, financial support, safety concerns, satisfaction with diversity on campus and food insecurity status. For the purposes of this study, the variables of interest included demographic information, the Depression, Anxiety, and Stress Scales – 21-item short form(Reference Lovibond and Lovibond27), and the US Household Food Security Survey Module: Six-Item Short Form(Reference Blumberg, Bialostosky and Hamilton28). Participants were excluded from analyses if they did not provide information on food security status (n 47).
Measures
Depression Anxiety and Stress Scales – 21-item short form (DASS-21)
The DASS-21 consists of three subscales measuring past week symptoms of depression (e.g. ‘I found it difficult to work up the initiative to do things’; Cronbach’s α = 0·93 in the present sample), anxiety (e.g. ‘I was aware of dryness in my mouth’; Cronbach’s α = 0·88) and stress (e.g. ‘I found it difficult to wind down’; Cronbach’s α = 0·89). All items are scored on a scale of 0–3, with 0 representing ‘did not apply to me at all’ and 3 representing ‘applied to me very much or most of the time’. Depression, anxiety and stress subscale scores were summed and multiplied by two and then categorised into ‘normal’ (0–9, 0–7, 0–14, respectively), ‘mild’ (10–13, 8–9, 15–18, respectively), ‘moderate’ (14–20, 10–14, 19–25, respectively), ‘severe’ (21–27, 15–19, 26–33, respectively) or ‘extremely severe’ (28+, 20+, 34+, respectively) categories, per established cut-offs(Reference Lovibond and Lovibond27).
The US Household Food Security Survey Module: six-item short form
This measure assesses food security and is scored from 0 to 6, with scores of 0–1 representing high/marginal food security, scores of 2–4 representing low food security and scores of 5–6 representing very low food security (Cronbach’s α = 0·92)(Reference Blumberg, Bialostosky and Hamilton28). For each item, respondents receive a score of 1 if they answer ‘often’, ‘sometimes’, ‘almost every month’ or ‘some months but not others’ to frequency-type questions or ‘yes’ to questions that require a yes or no response. Respondents receive a score of 0 if they respond ‘never true’, ‘don’t know’ or ‘no’. Affirmative item responses are summed to create a total score.
Statistical analysis
Statistical analyses were conducted using SPSS version 25. We employed χ 2 tests and ANOVA tests to examine between-group differences in demographic variables by food insecurity status. We examined distribution properties and normality of all outcome variables prior to data analyses. Due to skewness of the data, we used rank-based independent samples Kruskal–Wallis H tests to examine DASS-21 scores by food insecurity status. Finally, we used pairwise comparisons to examine between-group differences in post hoc analyses.
Results
Participants (n 216) included graduate students in master’s and doctoral programmes at a university in upstate New York. A majority of participants (71·7 %) reported that they were enrolled in a doctoral programme, and 44·0 % reported that their programme was housed in the College of Arts and Sciences. Participants on average were 29·01 years of age (sd = 7·06) and reported an average BMI of 26·21 (sd 6·41) kg/m2. A majority of the participants self-identified as female (69·0 %, n 149), White (68·9 %, n 146) and currently in a relationship or married (63·1 %, n 132). Approximately 18 % (17·7 %, n 38) of participants self-identified as having food insecurity. Additionally, approximately 60 % of graduate students reported high/marginal food security (59·7 %, n 129) and approximately 40 % of students reported low (18·5 %, n 40) and very low food security (21·8 %, n 47) on the US Household Food Security Survey Module. More White students than non-White students reported high/marginal food security, and more non-White students reported low and very low food security (P = 0·02; see Table 1 for additional demographics).
Table 1 Demographics by food security status
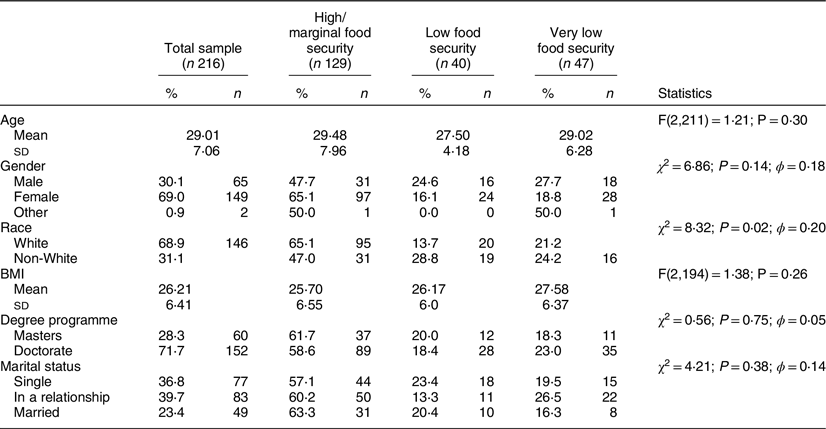
Table 2 summarises DASS-21 depression, anxiety and stress subscale scores by food insecurity status. The mean depression subscale score of the total sample was 9·82 (sd = 10·82) with significantly higher scores in students with very low food security (M = 17·02, sd = 9·82) compared with low food security (M = 8·57, sd = 10·42) and high/marginal food security (M = 7·56, sd = 8·38). The mean anxiety subscale score of the total sample was 7·20 (sd = 9·05) with significantly higher scores in students with very low food security (M = 14·23, sd = 13·05) compared with low food security (M = 5·54, sd = 6·38) and high/marginal food security (M = 5·11, sd = 6·31). The mean stress subscale score of the total sample was 12·37 (sd = 10·17) with significantly higher scores in students with very low food security (M = 19·19, sd = 11·53) compared with low food security (M = 11·94, sd = 10·28) and high/marginal food security (M = 10·03, sd = 8·47).
Table 2 Depression, anxiety and stress scores by food security status

* Significantly different from high/marginal food security.
† Significantly different from low food security.
Discussion
The present study determined initial prevalence estimates of food insecurity and the relationship between levels of food security and symptoms of depression, anxiety and stress in a sample of graduate students. This study expanded upon other studies that found that food insecurity is common among undergraduate students(Reference Chaparro, Zaghloul and Holck13–Reference Payne-Sturges, Tjaden and Caldeira19). In the present sample of graduate students, 40·3 % were considered to have either low food security or very low food security according to the US Household Food Security Survey Module: Six-Item Short Form. These rates are substantially higher than the overall US household food insecurity rate of approximately 11 %1 and comparable or higher than several recorded prevalence rates of food insecurity among undergraduate students(Reference Chaparro, Zaghloul and Holck13–Reference Payne-Sturges, Tjaden and Caldeira19). Moreover, graduate students with very low food security reported significantly elevated levels of depression, anxiety and stress. Specifically, students with self-reported high/marginal food security or low food security had depression, anxiety and stress subscale scores in the normal range, whereas students with very low food security reported depression, anxiety and stress in the moderate range.
In addition to the US Household Food Security Survey Module: Six-Item Short Form, participants were asked whether they considered themselves to be food insecure, and only 17·7 % reported that they considered themselves to be food insecure. This suggests that many students may not accurately recognise their level of food security and consequently not seek out available community and campus resources. Similarly, research has demonstrated that Canadian undergraduate students with food insecurity did not identify with their food insecurity status(Reference Maynard29). Based on elevated rates of food insecurity and the lack of awareness of their own food insecurity status in undergraduate and graduate students, campuses should educate students on food insecurity to address this public health issue.
This is the first study, to our knowledge, that specifically recruited graduate students to assess food insecurity and mental health outcomes. Participants were not primed that they were participating in a study about food insecurity, but rather the study was framed more broadly as assessing unmet needs of graduate students. Limitations of the study include the self-reported nature of the questionnaires and the non-diagnostic capability of the DASS-21 in identifying mental health outcomes. Additionally, the USDA Food Security Survey Module used in this study has shown inconsistencies in the response patterns of college students when compared with a national sample(Reference Nikolaus, Ellison and Nickols-Richardson30). Future studies should assess food insecurity with additional measures. Furthermore, this study is cross-sectional so we cannot assume causality between food insecurity status and depression, anxiety and stress. This sample was drawn from one university and primarily consisted of graduate students in that university’s College of Arts and Sciences. It is not clear whether this sample was representative of the university’s broader graduate student body, due to a lack of publicly accessible demographic data. Future research should obtain more diverse samples of graduate students.
Future research should also examine additional measures of mental health, including those that quantify mental health symptoms with greater specificity. Future studies should also sample from multiple, diverse institutions (e.g. rural, private and public) and professional programmes (e.g. business and law). This could provide more insight regarding the correlates of food insecurity in graduate students such as costs of living, insufficient funding and time commitments. Further, additional comparative research regarding graduate v. undergraduate student food insecurity should be done to disentangle potentially conflated variables and to better address possible nuances of graduate student mental health outcomes and food insecurity in possible interventions. So far, only one study at a large southeastern university compares rates of food insecurity in undergraduate and graduate students(Reference Soldavini, Berner and Da Silva21).
It is vital for universities to sponsor solutions to combat both undergraduate and graduate student food insecurity. To our knowledge, there are no efficacy or effectiveness studies assessing food insecurity interventions in undergraduate and graduate students(Reference Bruening, Argo and Payne-Sturges31). Future research should examine which interventions successfully reduce levels of food insecurity on college campuses. Some suggested interventions include providing meal plans in compensation packages, opening more easily accessible campus-based food pantries, connecting students to community-run food pantries, initiating student or public gardens and coordinating easier access to supermarkets. Previous research demonstrated that when university-based food pantries were available, students at risk for economic hardship were the most likely to use them(Reference Payne-Sturges, Tjaden and Caldeira32). However, Loopstra and Tarasuk(Reference Loopstra and Tarasuk33) discuss how food pantries are merely short-term solutions that do not effectively address the fundamental causes of food insecurity, but instead cater to people who are driven to use their services due to their dire and acute need of food. It is therefore important that universities provide multiple solutions to reduce food insecurity on campus. For example, a nonprofit organisation called ‘Swipe Out Hunger’ has a programme that encourages students to donate their extra meal plans to peers who are living with food insecurity on campus(34). Additionally, potential graduate student-oriented solutions can include increasing stipend funding to better accommodate costs of living.
Findings reported here suggest that support must also be provided to graduate students to address negative mental health outcomes associated with food insecurity. Research has demonstrated that undergraduate and graduate students experience significant depression, anxiety and stress during school(Reference Dahlin, Joneborg and Runeson24–Reference Peluso, Carleton and Asmundson26,Reference Eisenberg, Gollust and Golberstein35,Reference Garcia-Williams, Moffitt and Kaslow36) . Additionally, older students, including graduate students, may be at an elevated risk for suicide(Reference Silverman, Meyer and Sloane37). It is possible that depression, anxiety and stress associated with food insecurity further exacerbates poor mental health outcomes. These findings support the need for greater identification of students with food insecurity and efforts to prevent and treat poor mental health outcomes in these individuals. It is important for universities to highlight the availability of mental health services to all students and implement outreach at different tiers of education so all students are aware that these services exist.
Graduate school is a transformative time for many young adults as advanced education is a determinant for career choice, a qualifier for employment, and a catalyst in shaping minds into responsible consumers of knowledge. It is also a time of uncertainty. Students may enter higher education without necessary funds to afford healthy groceries nor the knowledge needed to cook healthy meals. Food insecurity among graduate students has important public health implications as it likely has ramifications on mental health and quality of life.
Acknowledgements
Financial support: Not Applicable. Conflict of interest: None. Authorship: J.A.C., S.P.S., R.D.D. and J.M.H. developed the study aims and hypotheses and designed the study. J.A.C. collected the data on which the present analyses are based. J.A.C. and J.M.H. conducted the statistical analyses. All authors were involved in the writing of the manuscript and approve of its submission in its current form. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the IRB at the University at Albany, State University of New York. Written informed consent was obtained from all subjects/patients.


