


Breast-feeding has been associated with a host of child health benefits, including improved immunity( Reference Hanson 1 ), diminished risk of infection( Reference Duijts, Ramadhani and Moll 2 ), lower blood pressure( Reference Martin, Gunnell and Smith 3 ), reduced risk of respiratory illness( Reference Cushing, Samet and Lambert 4 ) and decreased likelihood of childhood overweight/obesity( Reference Harder, Bergmann and Kallischnigg 5 , Reference Yan, Liu and Zhu 6 ). Despite the long line of literature linking breast-feeding to various health outcomes in offspring, only recently have scholars considered whether offspring dietary patterns during childhood are also predicted by breast-feeding history( Reference Abraham, Godwin and Sherriff 7 – Reference Soldateli, Vigo and Giugliani 12 ). This tendency to overlook diet is somewhat surprising, as research has found both breast-feeding( Reference Harder, Bergmann and Kallischnigg 5 , Reference Yan, Liu and Zhu 6 ) and dietary habits( Reference Leech, McNaughton and Timperio 13 , Reference Swinburn, Caterson and Seidell 14 ) to be associated with overweight/obesity. Even so, this small but growing body of research is quite consistent in its findings, suggesting that breast-feeding does indeed improve infant and child dietary patterns( Reference Abraham, Godwin and Sherriff 7 – Reference Soldateli, Vigo and Giugliani 12 ). This association appears to hold across multiple age groups and dietary components and may be partly explained by (i) lower maternal feeding restriction and enhanced infant self-regulation of intake( Reference Taveras, Scanlon and Birch 15 ) and/or (ii) repeated exposure of the breast-fed infant to the array of flavours found in the mother’s diet that are transmitted through breast milk( Reference Scott, Chih and Oddy 11 ).
Apart from the studies linking breast-feeding to health-related outcomes, scholars have also detected associations between breast-feeding and specific demographic variables, namely race/ethnicity( Reference Forste, Weiss and Lippincott 16 , Reference Mickens, Modeste and Montgomery 17 ) and socio-economic status (SES)( Reference Forste and Hoffmann 18 – Reference Heck, Braveman and Cubbin 20 ). Black women have historically been, and currently are, least likely to initiate and continue breast-feeding compared with other racial and ethnic groups in the USA( Reference Forste, Weiss and Lippincott 16 , Reference Mickens, Modeste and Montgomery 17 ). Possible reasons for racial/ethnic disparities in breast-feeding include, but are not limited to, differential preferences for bottle-feeding, the availability of free formula from the Special Supplemental Nutrition Program for Women, Infants and Children (WIC), variation in comfort levels with breast-feeding v. formula-feeding, limited availability of WIC breast-feeding support for minority women, degree of family support and differences in breast-feeding ambivalence( Reference Forste, Weiss and Lippincott 16 , Reference Chapman and Pérez-Escamilla 21 , Reference Kaufman, Deenadayalan and Karpati 22 ). Relatedly, women of lower SES are also less likely to breast-feed their infants in the USA( Reference Forste and Hoffmann 18 – Reference Heck, Braveman and Cubbin 20 ), whereas high levels of educational attainment and work in executive occupations among women and/or their partners increase the likelihood of breast-feeding( Reference Forste, Weiss and Lippincott 16 , Reference Heck, Braveman and Cubbin 20 ). Highly educated mothers may be (i) more likely to search out information on the health aspects of infant feeding choices and (ii) better able to afford feeding supplies( Reference Forste and Hoffmann 18 , Reference Heck, Braveman and Cubbin 20 , Reference Celi, Rich-Edwards and Richardson 23 ). Women working in lower-status occupations, however, may find expressing breast milk while at work more challenging, especially when their occupations are hazardous( Reference Heck, Braveman and Cubbin 20 , Reference Scott, Landers and Hughes 24 ).
Whatever the reasons for the disparities in breast-feeding, race/ethnicity and SES may be worth considering when examining associations between breast-feeding and child health outcomes, particularly since such outcomes, including obesity and diet, also vary by race/ethnicity and SES( Reference Fuemmeler, Stroo and Lee 25 – Reference Guerrero, Mao and Fuller 27 ). A handful of scholars have employed this line of reasoning by examining whether the influence of breast-feeding on overweight/obesity varies as a function of race/ethnicity and/or SES( Reference Armstrong and Reilly 28 – Reference Grummer-Strawn and Mei 32 ). The results, however, have not been entirely consistent. One study found no evidence that the influence of breast-feeding on childhood obesity varies by level of SES( Reference Armstrong and Reilly 28 ). However, in the case of race/ethnicity, some scholars have found a significant association between breast-feeding and overweight/obesity for whites and blacks, but not Hispanics( Reference Ehrenthal, Wu and Trabulsi 31 ). Still, the findings are far from uniform, with one group of researchers detecting an association between breast-feeding and overweight/obesity among non-Hispanic whites( Reference Grummer-Strawn and Mei 32 ), and another among Hispanics only( Reference Burdette and Whitaker 29 ). It therefore remains unclear whether race/ethnicity moderates the link between breast-feeding and child health, at least in the case of overweight/obesity.
Despite a number of studies examining race/ethnicity and SES as moderators of the link between breast-feeding and overweight/obesity, researchers have yet to consider whether the association between child diet and breast-feeding might differ across subsets of the population distinguished by SES and race/ethnicity. Historically, breast-feeding has varied across these racial/ethnic and socio-economic groups, and, in some studies, the benefits of breast-feeding for overweight/obesity has also varied across these groups. The current study aimed to extend this body of literature by examining whether junk food consumption during childhood varies as a function of breast-feeding history and whether the pattern of results differs on the basis of specific demographic features known to be associated with both breast-feeding practices and childhood dietary patterns (i.e. SES and race/ethnicity).
Materials and methods
Participants
The present study employed data from the Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), a nationally representative study of children born in the USA in 2001. The ECLS-B follows a large cohort of children from birth through their kindergarten school year (2007/2008). The study sampled birth certificates registered with the National Center for Health Statistics using the technique of stratified sampling, which permitted the inclusion of approximately 99 % of US births during 2001 in the sampling frame. Children were deemed ineligible if they met any of the following criteria: (i) they died before the age of 9 months; (ii) they were adopted before the age of 9 months; or (iii) their mothers were younger than 15 years at the time of birth. Birth certificates, direct child assessment, parent interviews and teacher questionnaires were all employed to obtain the data. In total, five waves of data have been collected. Importantly, the data contain various details concerning both the health and nutrition of the child, including her/his duration of breast-feeding and junk food intake during childhood. Various familial, developmental and demographic details are also included. These features of the data make the ECLS-B well suited to the present study.
Measures
Junk food consumption
At the fourth and fifth waves of data collection, when the focal children were in kindergarten, parents were asked to report how frequently their child ingested a number of junk foods during the 7d prior to the interview. The questions covered various domains of junk food consumption, including fast-food consumption, soda/sugary beverage consumption, salty snack consumption and sweets consumption. Specifically, parents were asked the following questions.
-
1. Fast-food consumption: ‘During the past 7 days, how many times did your child eat a meal or snack from a fast food restaurant with no wait service such as McDonald’s, Pizza Hut, Burger King, Kentucky Fried Chicken, Taco Bell, Wendy’s and so on? Consider both eating out, carry out, and delivery of meals in your response.’
-
2. Soda consumption: ‘During the past 7 days, how many times did your child drink Soda pop (for example, Coke, Pepsi, or Mountain Dew), sports drinks (for example, Gatorade) or fruit drinks that are not 100 % fruit juice (for example, Kool-Aid, Sunny Delight, Hi-C, Fruitopia, or Fruitworks)?’
-
3. Salty snack consumption: ‘During the past 7 days, how many times did your child eat potato chips, corn chips such as Fritos or Doritos, Cheetos, pretzels, popcorn, crackers or other salty snack foods?’
-
4. Sweets consumption: ‘During the past 7 days, how many times did your child eat candy (including Fruit Roll-Ups and similar items), ice cream, cookies, cakes, brownies, or other sweets?’
Response options to each of these items included ‘not at all in the past 7 days’ (7), ‘1–3 times during the past 7 days’ (5), ‘4 to 6 times during the past 7 days’ (6), ‘1 time per day’ (1), ‘2 times per day’ (2), ‘3 times per day’ (3) and ‘4 or more times per day’ (4). The items were ultimately recoded so that higher scores were assigned to children whose parents reported that they ate junk foods more frequently, with ‘not at all in the past 7 days’ being assigned the lowest value (0) and ‘4 or more times per day’ being assigned the highest value (6). Consequently, possible scores on each item ranged from 0 to 6. Junk food items were then summed and averaged to create a composite measure of junk food consumption across junk food domains. Importantly, children who had not entered kindergarten by wave 4 were not included in the fourth wave of data collection, but were instead included at wave 5 (i.e. the wave during which they entered kindergarten). Thus, junk food consumption was measured at wave 4 for most children and at wave 5 for a smaller portion of children, contingent on their timing of entry into kindergarten.Footnote *
Breast-feeding duration
At waves 1 and 2 of data collection, when children were approximately 9 months and 2 years of age, mothers were asked three questions about breast-feeding their child. The first question was: ‘Did you ever breast-feed (the child)? Yes (1) or No (2)’. The follow-up question was: ‘Are you still breast-feeding (the child) now? Yes (1) or No (2)’. Mothers who responded that they had terminated breast-feeding were then asked: ‘For how many months did you breast-feed (the child)?’, to which mothers responded with the number of months the child was breast-fed. Data from waves 1 and 2 were used to construct a variable that measured the duration of breast-feeding (in months) for each child, ranging from 0 to 21. Children in the final sample who were still breast-feeding at wave 2 were all at least 21 months old. As a result, focal children whose mothers reported that they were still breast-feeding at wave 2 were assigned a value of 21. However, it is important to note that being assigned a value of 21 on this variable indicates 21 months or more of breast-feeding, as the data provide no means of determining the precise duration of breast-feeding for children who were still breast-feeding at wave 2. Additionally, children who were no longer breast-feeding at wave 2, but had discontinued breast-feeding at the age of 21 months or more, were also assigned a value of 21 on this variable. Importantly, just under 3 % of the full sample was reported as being breast-fed for 21 months or more.Footnote † Despite this slight truncation of the measure, our continuous, dose–response measure of breast-feeding is an improvement over most measures used in prior studies, at least in terms of specificity of duration( Reference Evenhouse and Reilly 33 – Reference Reynolds, Hennessy and Polek 36 ).
Socio-economic status
The first key moderator of interest in the present study is SES. The ECLS-B data contain a comprehensive measure of household SES that has been utilized in prior research( Reference Mollborn and Lovegrove 37 , Reference Tucker-Drob, Rhemtulla and Harden 38 ). The item was constructed by ECLS-B researchers and is derived from the primary parent interview (i.e. usually the mother). The item includes a composite of scores pertaining to household income, maternal education, paternal (or resident partner) education and occupational prestige. In cases where the father was a non-resident, additional indicators tapping other economic resources were included in the composite measure, including monthly child support paid and other financial help from the father (e.g. childcare expenses). Ultimately, higher scores reflect a higher level of household SES. In the current study, the item was standardized for the purpose of creating multiplicative interaction terms( Reference Jaccard, Wan and Turrisi 39 ).
Race/ethnicity
The second key moderator in the present analysis is race/ethnicity. For the present study purposes, the construct is divided into three dichotomous variables: white (non-Hispanic), Hispanic and black. Importantly, race/ethnicity pertains to the mother in the current study, although in the vast majority of incidences the mother and child were concordant on race/ethnicity.
Child sex
The biological sex of the child was included as a covariate in the analysis, with male offspring being assigned a value of 1 and female offspring being assigned a value of 0.
Child age
The child’s age at wave 1 (in months) was also included as a covariate in the analysis.
Child attachment security
Considering the link between breast-feeding and attachment security( Reference Jackson 40 ) and attachment security and offspring diet( Reference Bost, Wiley and Fiese 41 ), we opted to include a dichotomous measure of attachment security in the present analysis that was derived from the Toddler Attachment Sort–45 (TAS-45). Securely attached children were assigned a value of 1, whereas insecurely attached children were assigned a value of 0.
Maternal age at birth
The mother’s age at birth (in years) was also included as a covariate in the analysis due to its correlation with breast-feeding practices( Reference Vogel, Hutchison and Mitchell 42 ) and its potential relevance for child dietary patterns( Reference Northstone and Emmett 43 ).
Marital status
Marital status was also included as a covariate in the analysis, with married maternal respondents being coded as 1 and unmarried respondents being coded as 0.
Employment
An item pertaining to the mother’s employment at the first wave of data collection was also included in the analysis, due to the negative correlation between employment and breast-feeding duration( Reference Scott, Binns and Oddy 44 ). Mothers who reported that they were employed at the first wave of data collection were assigned a value of 1, whereas mothers who were not employed at the first wave of data collection were assigned a value of 0.Footnote *
Participation in the Special Supplemental Nutrition Program for Women, Infants and Children
A dichotomous item tapping WIC participation during pregnancy and following childbirth was also included in the analysis, as WIC participation has historically been negatively associated with breast-feeding duration and initiation( Reference Ryan and Zhou 45 ). Mothers who reported that they had participated in WIC during this time were assigned a value of 1, whereas mothers who did not participate in WIC were assigned a value of 0.
Postpartum depression
At wave 1, parents were asked twelve questions about the extent to which they felt depressed. For instance, they were asked how frequently they felt restless, lonely, sad, depressed, unfocused and unmotivated during the week prior to the survey. Response options ranged from ‘less than a day’ (1) to ‘most or all days’ (4). Ultimately, in order to tap parents’ overall depressive symptomatology, a scale was created by summing the twelve items together (α=0·87).
Maternal involvement
Mothers were also asked several questions about their involvement with their infant at the first wave of data collection. To illustrate, mothers were asked how often they read books, tell stories and sing songs to their infant. Response options ranged from 1 (‘not at all’) to 4 (‘every day’). Higher scores on this item correspond to higher levels of maternal involvement (α=0·66).
Food rules
At the third wave of data collection, when focal children were approximately 4 years old, mothers were asked, ‘In your house, are there rules and routines about what kinds of food the child eats?’ Mothers who responded in the affirmative were assigned a value of 1. Mothers who reported that there were no household rules concerning food were assigned a value of 0.
Family meals
At wave 3, respondents stated the following during the interview with the mother: ‘In a typical week, please tell me the number of days at least some of the family eats the evening meal together.’ Response options ranged from ‘one day per week’ (1) to ‘seven days per week’ (7). Thus, the item is coded so that higher scores reflect a greater number of family dinners in a typical week.
Statistical analysis
The current analysis proceeded in a series of steps. First, descriptive statistics of the all of the variables included in the analyses were calculated and examined. Next, hierarchical regression techniques (ordinary least squares) were employed to first explore whether breast-feeding duration independently predicted junk food consumption among offspring during childhood. Subsequently, the possibility of a statistical interaction between breast-feeding duration and SES in the prediction of junk food consumption was tested. Next, we divided the sample by race/ethnicity to examine (i) whether the influence of breast-feeding and SES on offspring junk food consumptions varied by race/ethnicity and (ii) whether race/ethnicity moderated any interaction between breast-feeding duration and SES. Finally, the specific domains of junk food consumption (i.e. fast foods, soda, salty snacks and sweets) were employed as outcome variables to examine whether any three-way interactions detected between breast-feeding duration, SES and race/ethnicity were robust to the type of junk food examined. In line with a large body of prior research, variables that comprise interaction terms were standardized before multiplication( Reference Jaccard, Wan and Turrisi 39 ) and the statistical significance of relevant coefficients and interaction terms across models distinguished by race/ethnicity was determined by conducting z tests for the equality of regression coefficients( Reference Paternoster, Brame and Mazerolle 46 ).
Results
We proceeded with the analysis by first examining the descriptive statistics presented in Table 1, which revealed that the average breast-feeding duration in the full sample was approximately 4 months. Roughly 45 % of mothers were white, whereas 17 and 16 % were Hispanic and black, respectively. Children, on average, ate sweets most frequently (mean=2·22) and fast foods least frequently (mean=0·91). Male children made up 51 % of focal subjects and the approximate age of children at wave 4/5 was 69 months (or 5 years and 9 months). Roughly half of mothers were employed at wave 1, 68 % of mothers were married and 52 % of mothers participated in WIC during their pregnancy. Finally, the majority of families had established rules concerning food (75 %) and ate dinner together most days of the week (mean=5·97).
Table 1 Descriptive statistics of the nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008
SES, socio-economic status; WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
Next, we explored whether breast-feeding duration independently influences junk food consumption and whether this influence varies by level of SES. The results of these analyses are displayed in Table 2. Model 1 of Table 2 revealed that a longer duration of breast-feeding was indeed associated with significant reductions in offspring junk food consumption, net of covariates (P<0·01). The standardized effect associated with breast-feeding duration (β=−0·07, P<0·01), however, was roughly half the size of the standardized effect of SES (β=−0·15, P<0·01), yet was similar in size to the standardized effect of food rules (β=−0·08, P<0·01). The results of Model 1 also indicated that male children exhibited higher levels of junk food consumption and that, relative to the reference category (i.e. other race/ethnicity), children of black and white mothers were more likely to eat junk food more often. Model 2 of Table 2 expands upon the findings of Model 1 by examining the interaction between breast-feeding duration and SES as a predictor of junk food consumption. The interaction emerged as significant and positive (β=0·05, P<0·01), suggesting that the negative effect of breast-feeding duration on offspring junk food consumption was diminished (i.e. was more positive) among higher-SES individuals and was enhanced (i.e. was more negative) among lower-SES individuals.
Table 2 Breast-feeding duration and offspring junk food consumption, and moderation by socio-economic status (SES), in a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008
WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
*P<0·05, **P<0·01.
The relationship between breast-feeding duration and offspring junk food consumption was explored further by dividing the sample into subgroups distinguished by race/ethnicity. The results of these analyses appear in Models 1, 3 and 5 of Table 3. The findings indicated that breast-feeding duration significantly reduced offspring junk food consumption among whites and blacks, but not among Hispanics. The z tests for the equality of regression coefficients revealed that breast-feeding had a significantly stronger negative effect on junk food consumption among whites than among Hispanics (z=−2·00). Breast-feeding coefficients, however, were not significantly different between blacks and whites (z=−0·73) or blacks and Hispanics (z=−1·56). In addition, Models 1, 3 and 5 revealed that SES was significantly and negatively associated with junk food consumption across all racial/ethnic groups. The z tests for the equality of regression coefficients, moreover, revealed that the negative association between SES and junk food consumption was significantly larger among blacks than among whites (z=−3·66). SES coefficients, however, were not significantly different between blacks and Hispanics (z=−1·40) or Hispanics and whites (z=−1·71).
Table 3 The interactive effects of breast-feeding duration and socio-economic status (SES) on offspring junk food consumption by race/ethnicity in a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008
WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
*P<0·05, **P<0·01.
After examining the influence of breast-feeding and SES across racial/ethnic groups, we proceeded to model the breast-feeding×SES interaction by racial/ethnic group to explore the possible role of three-way interactions between these variables in the prediction of offspring junk food consumption. These results are presented in Models 2, 4 and 6 of Table 3. A significant three-way interaction emerged between race/ethnicity, breast-feeding duration and SES. Specifically, the z tests for the equality of regression coefficients revealed that breast-feeding duration was associated with significantly lower levels of offspring junk food consumption, but that this effect was especially pronounced among low-SES blacks (blacks v. whites: z=−3·75, P<0·01; blacks v. Hispanics: z=−4·20; P<0·01).
This significant three-way interaction is depicted in Fig. 1, which illustrates that, across racial/ethnic groups, breast-feeding duration had little to no effect on offspring junk food consumption among high-SES individuals. However, among low-SES individuals, the influence of breast-feeding duration on junk food consumption varied by race/ethnicity. In particular, breast-feeding duration had little association with junk food consumption among low-SES Hispanics, a significant negative association with junk food consumption among low-SES whites and a significantly larger negative association with junk food consumption among low-SES blacks. To illustrate, the predicted junk food consumption value among low-SES blacks who were never breast-fed was 1·84, which equates to the 73rd percentile on the junk food consumption measure. Comparatively, the predicted junk food consumption value among low-SES blacks who attained the highest score on the breast-feeding measure was 0·79, which equates to the 21st percentile on the junk food consumption measure (a difference of 52 percentile points).Footnote *
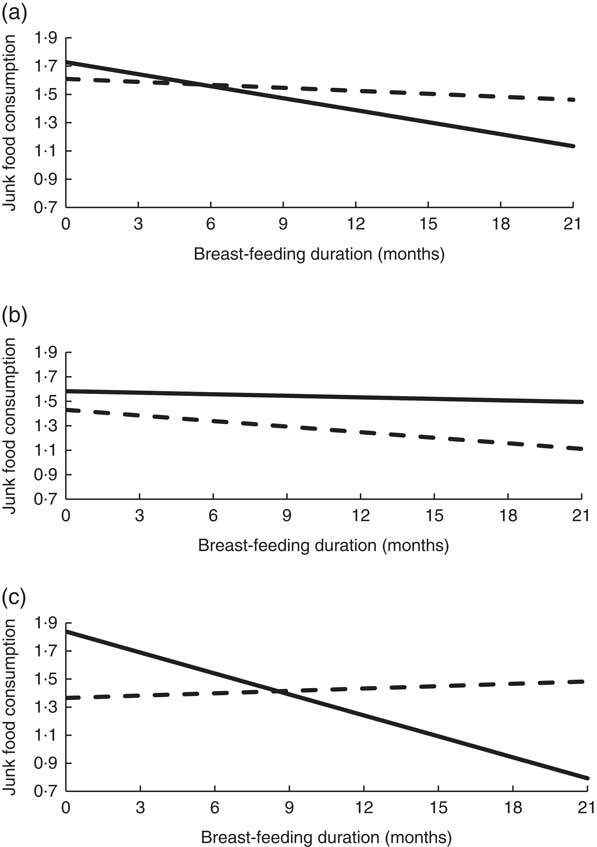
Fig. 1 Interaction between breast-feeding and socio-economic status (SES; ![]() , low SES;
, low SES; ![]() , high SES) on junk food consumption by race/ethnicity (a, whites; b, Hispanics; c, blacks) among a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008. Low SES=below the median SES value; high SES=above the median SES value
, high SES) on junk food consumption by race/ethnicity (a, whites; b, Hispanics; c, blacks) among a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008. Low SES=below the median SES value; high SES=above the median SES value
Finally, we conducted a series of ancillary analyses to examine whether the protective effect of breast-feeding duration on junk food consumption among low-SES blacks persisted across each of the junk food domains (i.e. fast foods, soda, salty snacks and sweets). The results are presented in Table 4. The findings revealed that the breast-feeding×SES interaction was significantly and positively associated with all of the junk food domains among blacks, suggesting that the findings among the black sample are robust to junk food type.Footnote † Figure 2 depicts the findings presented in Table 4. As illustrated in Fig. 2, a longer duration of breast-feeding among high-SES blacks had no consistent effect on junk food consumption across the four junk food domains. Conversely, a longer duration of breast-feeding was consistently associated with lower levels of fast-food, soda, salty snack and sweets consumption among low-SES blacks.
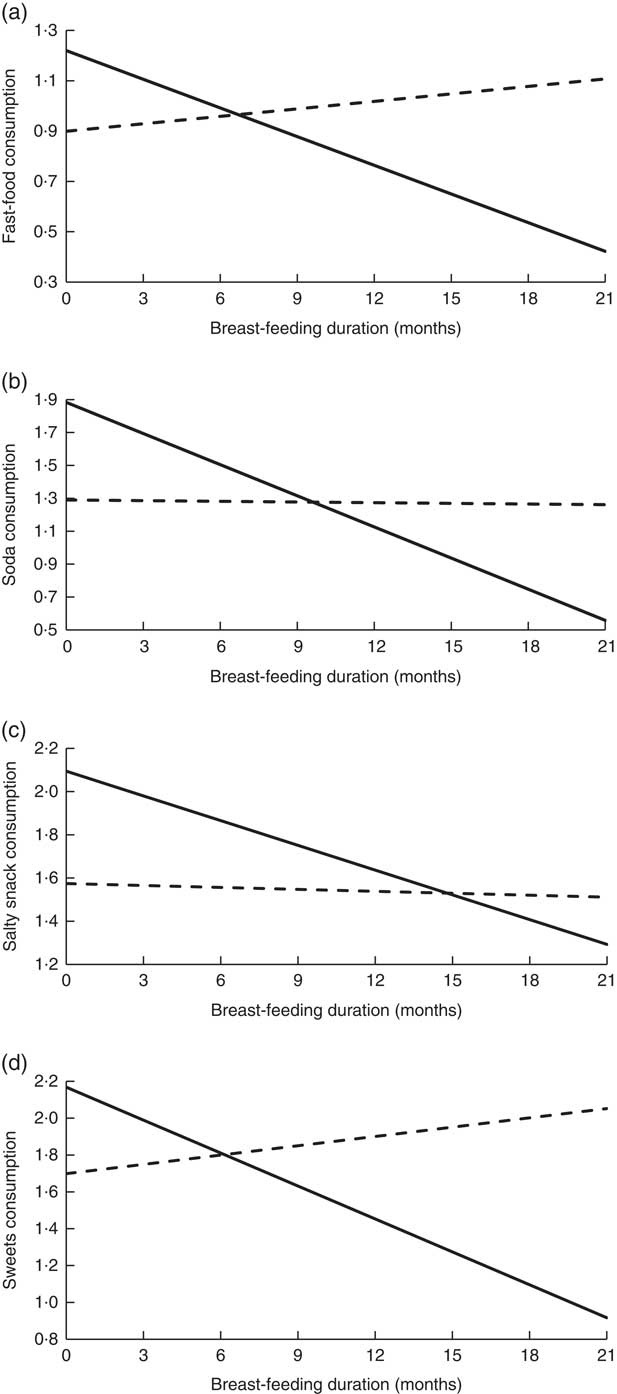
Fig. 2 Interaction between breast-feeding and socio-economic status (SES; ![]() , low SES;
, low SES; ![]() , high SES) on junk food consumption (a, fast foods; b, soda; c, salty snacks; d, sweets) among blacks in a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008. Low SES=below the median SES value; high SES=above the median SES value
, high SES) on junk food consumption (a, fast foods; b, soda; c, salty snacks; d, sweets) among blacks in a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008. Low SES=below the median SES value; high SES=above the median SES value
Table 4 The interactive effects of breast-feeding duration and socio-economic status (SES) on offspring junk food consumption among blacks in a nationally representative sample of US-born children, Early Childhood Longitudinal Study: Birth Cohort (ECLS-B), 2001–2007/2008
WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
*P<0·05, **P<0·01.
Discussion
Breast-feeding has been found to promote offspring health in myriad ways( Reference Hanson 1 – Reference Yan, Liu and Zhu 6 ). The present study adds to this body of research by revealing a negative relationship between breast-feeding and offspring junk food consumption, particularly among low-SES blacks. To be precise, a longer duration of breast-feeding was associated with lower levels of junk food consumption among low-SES blacks across the four measured domains: fast-food, soda, salty snack and sweets consumption. Associations between breast-feeding and each of the junk food dimensions, however, were not consistently detected among Hispanics or whites, regardless of SES, nor were they detected for high-SES blacks, yielding a three-way interaction between breast-feeding, SES and race/ethnicity in the prediction of junk food consumption.
In light of the findings of the current study, it would be worthwhile to identify and promote strategies that assist women in their efforts to breast-feed. Our findings suggest that this may be particularly true in the case of low-SES black women, as breast-feeding among these women appears to have the greatest potential to improve offspring diet. To date, a number of effective breast-feeding promotion strategies for black women have been identified and/or are in development. Studies that evaluate social support interventions have found that a combination of strategies such as daily in-hospital visits, postpartum visits, prenatal visits or telephone calls from peer counsellors during the postpartum period, the provision of breast pumps, prenatal/childbirth classes taught by a nurse/peer counsellor, telephone support from either a nurse or a lactation consultant, and/or unlimited access to a nurse via pager have had a positive impact on breast-feed initiation and duration( Reference Chapman and Pérez-Escamilla 21 , Reference Anderson, Damio and Young 47 – Reference Wolfberg, Michels and Shields 55 ). Social support that targets family members and the broader community has also significantly improved breast-feeding rates among black women. In a breast-feeding class for male partners, for instance, men learn the benefits of breast-feeding, ways to support their partner’s decision to breast-feed and strategies to deal with those who may not be supportive of breast-feeding. Community Breastfeeding Gatherings, sponsored monthly by the African American Breastfeeding Network in Wisconsin, also promote breast-feeding by bringing together pregnant and breast-feeding mothers, their families and board-certified lactation consultants. Community Breastfeeding Gatherings begin with a family-style meal and facilitate an informal and educational community dialogue, with recent events including a Peer Father Advocate component( 56 ).
Although it is important to identify breast-feeding promotion strategies that have been shown to be effective among black women, the present findings highlight the particular relevance of breast-feeding for the early health behaviours of children of a narrower subset of women: low-SES black women. A potentially useful point of intervention for these women is the WIC programme, as low-SES black women are, and have historically been, over-represented among WIC participants( Reference Thorn, Tadler and Huret 57 ). Any effort to promote breast-feeding among low-SES black women would be remiss if it did not consider the WIC programme as a unique opportunity to provide breast-feeding education and support to women who might not breast-feed otherwise. Not only has research revealed breast-feeding to be less common among WIC participants( Reference Dunn, Kalich and Fedrizzi 58 – Reference Robinson, VandeVusse and Foster 64 ), it has also revealed that black WIC participants have the lowest breast-feeding rates( Reference Evans, Labbok and Abrahams 59 , Reference Marshall, Gavin and Bish 63 ) and are significantly less likely to receive breast-feeding advice from their health-care providers and/or WIC counsellors than white participants( Reference Evans, Labbok and Abrahams 59 , Reference Robinson, VandeVusse and Foster 64 , Reference Beal, Kuhlthau and Perrin 65 ).
In an effort to improve breast-feeding rates among WIC participants, especially black participants, the WIC programme expanded its breast-feeding education to include the Breastfeeding Peer Counseling Program( Reference Chapman, Morel and Anderson 66 , Reference Gross, Powell and Anderson 67 ). The WIC peer counsellor must have breast-fed at least one child for 6 months or longer and be a current or previous WIC participant. Breastfeeding Peer Counseling Programs are offered as a means of providing educational, emotional and social support for new breast-feeding mothers( Reference Evans, Labbok and Abrahams 59 , Reference Robinson, VandeVusse and Foster 64 ). Recent research has revealed that Breastfeeding Peer Counseling Programs have had positive effects on increasing breast-feeding initiation and continuation for black mothers enrolled in WIC( Reference Baumgartel and Spatz 68 , Reference Campbell, Wan and Speck 69 ). Breastfeeding Peer Counseling Programs have discovered that black women tend to place high value on breast pumps as a matter of convenience and a way to exert control over breast-feeding( Reference Gross, Powell and Anderson 67 ). Moreover, the educational component of the Breastfeeding Peer Counseling Program regarding the benefits of breast milk for infants has resulted in increasing breast-feeding rates among black WIC participants( Reference Evans, Labbok and Abrahams 59 , Reference Robinson, VandeVusse and Foster 64 ). Due to many complex factors that affect lower-income black women’s decision to breast-feed, a comprehensive approach should be implemented in order to improve breast-feeding initiation and duration rates among this subset of the population( Reference Dunn, Kalich and Fedrizzi 58 , Reference Robinson, VandeVusse and Foster 64 ).
The current study is the first to examine the association between breast-feeding and offspring junk food consumption separately for racial and SES groups using a nationally representative sample of US families. It is not, however, without its limitations. First, we would have preferred additional breast-feeding details (e.g. extracted milk v. feeding at the breast), including additional WHO core indicators of infant nutritional patterns (e.g. the ratio of breast milk v. formula, or predominant breast-feeding) but these details were not available in the data( 70 ).Footnote * Second, we were only able to examine certain components of food consumption at one point in time (i.e. the kindergarten school year). Future research would benefit from an examination of a broader array of foods and changes in consumption over time. Third, due to data limitations, we were unable to fully examine maternal attitudes and education concerning general health and nutrition, despite accounting for food rules and routines within the familial context. Future studies should build upon our findings by exploring associations between breast-feeding duration, health awareness and nutritional knowledge among low-SES black women. Finally, apart from familial rules and routines regarding food consumption, the ECLS-B does not provide specific details concerning the dietary patterns of the parents. Maternal diet has been shown to influence offspring diet( Reference Durão, Severo and Oliveira 71 ); even so, prior studies linking breast-feeding to offspring diet are supportive even when they account for maternal diet( Reference Jones, Moschonis and Oliveira 9 ). As has been the case in prior research( Reference Perrine, Thompson and Scanlon 10 ), ancillary analyses of a sub-sample of participants that account for pre-pregnancy BMI resulted in no changes to our findings.
Despite the shortcomings of the current study, it represents an important extension of prior research as it considers ways that dietary patterns during childhood can be differentially shaped by breast-feeding practices across racial and socio-economic subsets of the population. Although we found the association between breast-feeding and child diet to be more pronounced among low-SES black women and children, it is important to promote breast-feeding for all racial/ethnic and SES groups due to the many health benefits associated with this practice( Reference Hanson 1 – Reference Yan, Liu and Zhu 6 ). Efforts to promote breast-feeding among women require a comprehensive approach that seeks to shape health attitudes, enhance nutrition education and buttress social support systems. This comprehensive approach to developing interventions that facilitate breast-feeding may be particularly important for low-SES black women. Future research should aim to replicate and build upon the present study by (i) uncovering mechanisms that might link breast-feeding duration to offspring diet and (ii) exploring exactly how these processes might vary across racial and SES groups. Doing so can help to elucidate strategies that promote breast-feeding among low-SES black women and improve nutritional habits in low-SES black children, setting the stage for future health and well-being.
Acknowledgements
Acknowledgements: The authors would like to acknowledge the Institute of Education Sciences and its sponsoring agencies, which provided the corresponding author with access to the ECLS-B data. Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: The authors declare that they have no conflicts of interest. Authorship: D.B.J. conceived of the study, developed the research design, analysed the data, tabulated the results and drafted the manuscript. K.R.J. drafted the manuscript and aided in the interpretation of the findings. Both authors reviewed and approved the final version of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the University of Texas at San Antonio. Written informed consent was obtained from all participants.






