



Sleep disturbance and insomnia are highly prevalent among adolescents(Reference Zambotti, Goldstone and Colrain1), and it has been suggested that anxiety is a common cause(Reference Mullin and Simon2). A previous study from the Global School-Based Student Health Survey found that 7·8 % of adolescents had anxiety-induced sleep disturbance, but this prevalence can vary between 1·8 % and 26·8 % depending on the country(Reference Vancampfort, Van Damme and Stubbs3).
Among the risk factors for anxiety-induced sleep disturbance, unhealthy lifestyle behaviours, such as sedentary behaviour, physical inactivity and the consumption of ultra-processed foods, were highlighted(Reference Vancampfort, Van Damme and Stubbs3–Reference Werneck, Vancampfort and Oyeyemi6). In addition to their negative independent effects, these behaviours seem to be associated with each other(Reference Ashdown-Franks, Vancampfort and Firth7–Reference Martines, Machado and Neri9), a fact that can substantially increase the risk of anxiety-induced sleep disturbance. A recent study found that adolescents who reported high daily consumption of ultra-processed foods as well as increased time watching TV had higher prevalence of anxiety-induced sleep disturbance compared to reporting the negative behaviours in isolation(Reference Werneck, Vancampfort and Oyeyemi5).
TV viewing and ultra-processed food consumption can share some direct mechanisms in the association with mental disorders during adulthood, such as inflammation, but this relationship is yet to be investigated among adolescents(Reference Endrighi, Steptoe and Hamer10,Reference Firth, Veronese and Cotter11) . Moreover, both ultra-processed foods and TV viewing are associated with body satisfaction(Reference Matias, Lopes and de Mello12), loneliness(Reference Ferrer-Cascales, Albaladejo-Blázquez and Ruiz-Robledillo13) and self-rated general health(Reference Osera, Awai and Kobayashi14), which have been associated with anxiety-induced sleep disturbance(Reference Ben Simon and Walker15–Reference Kelly, Zilanawala and Booker17). Thus, these mechanisms appear to be potential mediators. However, the influence of potential shared mediators of TV viewing and ultra-processed foods in the association with anxiety-induced sleep disturbance is still not clear. Therefore, our aim was to investigate the role of potential shared mediators (i.e. body satisfaction, loneliness, self-rated health and eat while watching TV or studying) in the association of TV viewing and daily ultra-processed food consumption with anxiety-induced sleep disturbance.
Methods
Sample
Data from the present study are derived from the Brazilian Adolescent School-Based Health Survey (PeNSE in Portuguese), which is part of the surveillance of risk and protection factors for chronic diseases in Brazil. This survey aims to report on risk factors and health of Brazilian students as well as to identify priority issues for the development of public policies. PeNSE was conducted in 2015(18). The survey included a nationally representative sample of students from the final (ninth) year of elementary education, which was selected using a complex multi-stage, stratified, clustered probability design. The sampling process and methods are detailed elsewhere(18). Briefly, cluster sampling was performed in two stages in capital cities (with schools as primary units and classes as secondary units) and three stages in other municipalities (with municipalities as primary units, schools as secondary units and classes as tertiary units). From 3160 eligible schools, a sample of 3040, with 124 227 students, was eligible to be included in the sample. Of these students, 102 072 accepted to participate and were at school on the day of interview. All procedures were approved by the National Health Research Ethics Council, and the study was conducted in accordance with the principles expressed in the Declaration of Helsinki (CONEP n. 1.006.467).
Anxiety-induced sleep disturbance
Anxiety-induced sleep disturbance was assessed with the following question: ‘Considering the past 12 months, how frequently do you have insomnia due to worries or concerns? (a) never; (b) rarely; (c) sometimes; (d) frequently; and (e) very frequently’, which is based on the question of the Global School-Based Student Health Survey and used in previous studies(Reference Vancampfort, Van Damme and Stubbs3–Reference Werneck, Vancampfort and Oyeyemi5). Adolescents reporting frequent sleep disturbance due to worries and concerns were classified as having anxiety-induced sleep disturbance(Reference Vancampfort, Van Damme and Stubbs3–Reference Werneck, Vancampfort and Oyeyemi5).
TV viewing
Participants were asked about their total time watching TV per day, which was also based on the questionnaire of the Global School-Based Student Health Survey. For the analysis, we adopted the cut-point of >4 h/d for TV viewing, which corresponds to high levels of viewing relative to the wider population(Reference Werneck, Vancampfort and Oyeyemi6).
Frequency of ultra-processed food consumption
The consumption of ultra-processed foods was assessed through questionnaires asking about specific ultra-processed components: industrialized foods (such as hamburger, ham, mortadella, salami, sausage, instant noodles, packet saltiness, salty crackers), fast foods, confectionery (candies, chocolates, chewing gum, lollipops) and soft drinks. The base question was: ‘In the last 7 d, on how many days did you eat…?’ This was an adaptation based on the NOVA recommendation for ultra-processed food consumption(Reference Monteiro, Cannon and Lawrence19). Those who reported daily consumption of at least one group of ultra-processed were classified as ‘daily consumers’(Reference Costa, Flores and Wendt8).
Mediators
Body satisfaction was estimated through the question: ‘How do you feel about your body?’ Possible answers were: ‘(a) very satisfied’, ‘(b) satisfied’, ‘(c) indifferent’, ‘(d) dissatisfied’ and ‘(e) very dissatisfied’. Those who indicated options ‘a’, ‘b’ or ‘c’ were considered to be ‘satisfied’ with their body, and those who reported options ‘d’ and ‘e’ were ‘dissatisfied’ with their body. Feeling of loneliness was assessed through the question, ‘When you consider the past 12 months, how often did you feel lonely?’ Possible answers were: ‘(a) never’, ‘(b) rarely’, ‘(c) sometimes’, ‘(d) frequently’ and ‘(e) very frequently’. We considered as at risk those who felt loneliness frequently and very frequently (‘yes’), and at no risk if they indicated other options (‘no’). Self-rated health was estimated through the question, ‘How would you rate your health status?’, with the potential answers ‘(a) very good’, ‘(b) good’, ‘(c) regular’, ‘(d) bad’ and ‘(e) very bad’. We considered them to be at risk if they answered bad or very bad (‘poor’) and at no risk if they indicated other options (‘good’). For the question ‘Do you eat when watching TV or studying?’, possible answers were: ‘(a) yes, every day’, ‘(b) yes, 5–6 d a week’, ‘(c) yes, 3–4 d a week’, ‘(d) yes, 1–2 d a week’, ‘(e) rarely’ and ‘(f) no’. We classified the participants as having a daily pattern (seven times per week) and no daily pattern if ≤6 times per week.
Covariates
Chronological age and ethnicity were self-reported by participants; ethnicity was classified as white and non-white in our study. Food insecurity was used as a proxy for socioeconomic status. Participants were asked ‘During the past 30 d, how often did you go hungry because there was not enough food in your home?’ Answer options were classified as ‘never’, ‘rarely/sometimes’ and ‘most of the time/always’. Physical activity was assessed using questions related to transport, leisure time as well as physical education classes, which has been previously described(Reference Werneck, Oyeyemi and Fernandes20). We used the sum of all domains as our final indicators, with the cut-off point of 300 min/week, which is a frequently used cut-off point and also corresponds to high levels of physical activity relative to the wider population(Reference Werneck, Oyeyemi and Fernandes20). Moreover, type of city (capital or interior) and country regions (north, northeast, south, southeast, midwest) were also used as a covariate into the analyses.
Statistical procedures
The characteristics of the sample as well as the comparison between included and excluded participants were described by sex using frequencies and 95 % CI. The isolated association of daily ultra-processed food consumption and TV viewing with anxiety-induced sleep disturbance was assessed through logistic regression models, with a crude model (model 1) and an adjusted model (model 2 – adjusted for age group, ethnicity, food insecurity, country region, type of city and physical activity).
After this, mediation models were conducted to assess the influence of potential mediators (body satisfaction, loneliness, self-rated health and eat while watching TV or studying) in the associations of daily ultra-processed food consumption and TV viewing with anxiety-induced sleep disturbance (Fig. 1). The Karlson–Holm–Breen method was used for the mediation(Reference Breen, Karlson and Holm21), creating different models for each mediator. This method was applied in logistic regression models and decomposes the total effect of a variable into direct and indirect effects. This estimation also provides the percentage of explanation by the mediator (mediated percentage). The mediation models were also adjusted for age group, ethnicity, food insecurity, country region, type of city and physical activity. As an assumption for the use of the Karlson–Holm–Breen method, we tested the interactions between exposures and mediators in the association with the outcome and found no significant interactions. Sampling weights (accounted for the type of school (public or private), number of classes inside each school, valid questionnaires inside each class, number of classes selected in the school and representativeness of all country regions), strata and primary sample unit were accounted in all analyses, conducted in Stata 15.1.

Fig. 1 Theoretical model
Results
From the initial sample (102 072 adolescents), 2281 presented missing data in at least one variable of the present study and were excluded. The excluded sample presented a higher proportion of boys (66·6 % v. 48·3 %), adolescents aged >14 years (42·2 % v. 30·4 %), but with similar rates of elevated food insecurity (most of the time/always), region and type of city (Table 1). Therefore, the final sample composed of 99 791 adolescents (52 038 girls).
Table 2 shows the characteristics of the sample according to sex. Girls had higher prevalence of anxiety-induced sleep disturbance (girls 15·4 %, 95 % CI 14·9 %, 16·0 % v. boys: 6·8 %, 95 % CI 6·4 %, 7·3 %), daily ultra-processed food consumption (girls: OR 43·5, 95 % CI 42·7, 44·3 v. boys: OR 36·3, 95 % CI 35·5, 37·1), body dissatisfaction (girls: OR 31·5, 95 % CI 30·8, 32·2 v. boys: OR 22·1, 95 % CI 21·4, 22·8), loneliness (girls: OR 22·3, 95 % CI 21·7, 23·0 v. boys: OR 10·2, 95 % CI 9·7, 10·7) and poor self-rated health (girls: OR 31·5, 95 % CI 30·8, 32·2 v. boys: OR 22·1, 95 % CI 21·4, 22·8).
Table 1 Characteristics of sample according to included and excluded sample

Note. Values are presented in absolute frequencies, weighted relative frequencies as well as 95 % CI.
* n of excluded = 2173.
† n of excluded = 2097.
Table 2 Characteristics of sample according to sex
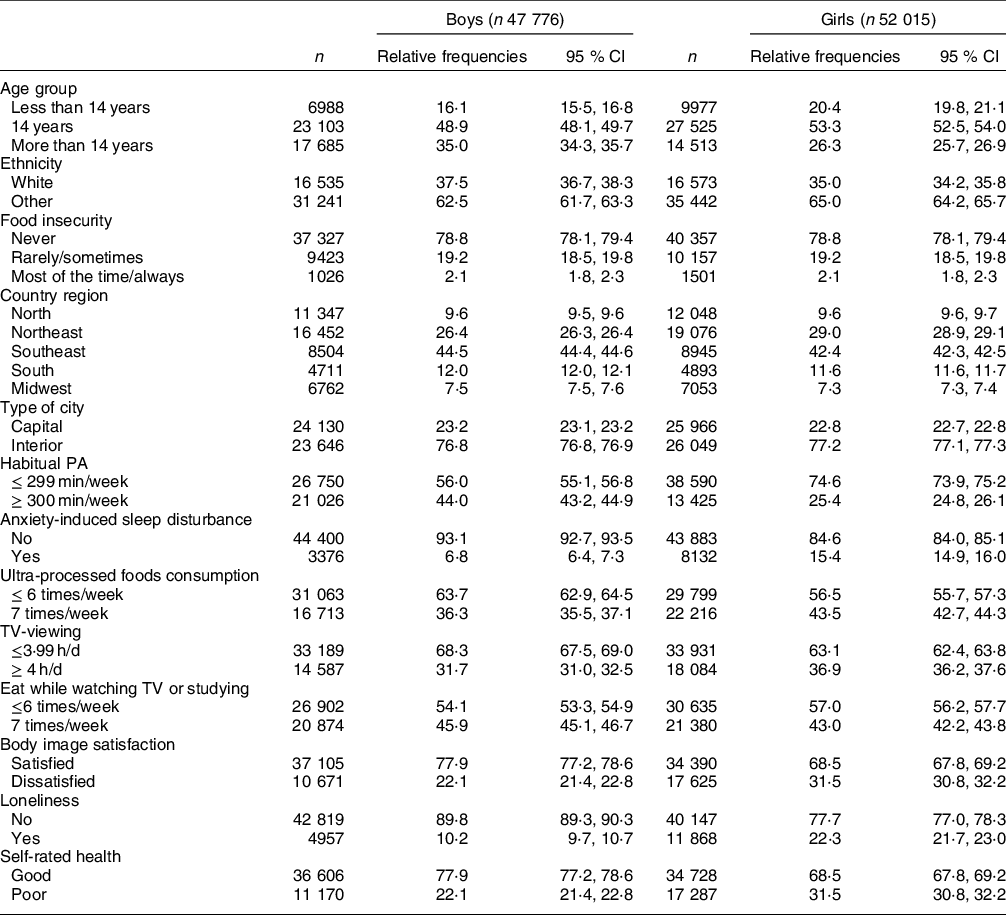
Note. Values are presented in absolute frequencies, weighted relative frequencies as well as 95 % CI.
The isolated associations of daily ultra-processed food consumption and TV viewing with anxiety-induced insomnia are presented in Table 3. Both daily ultra-processed food consumption (boys: OR 1·48, 95 % CI 1·30, 1·70; girls: OR 1·46, 95 % CI 1·34, 1·60) and TV viewing (boys: OR 1·24, 95 % CI 1·08, 1·43; girls: OR 1·09, 95 % CI 1·00, 1·19) were associated with higher odds for anxiety-induced sleep disturbance.
Table 3 Associations between daily ultra-processed food consumption and TV-viewing with anxiety-induced sleep disturbance among adolescents

CI, Confidence interval.
Note. Adjusted for age group, ethnicity, food insecurity, country region, type of city (capital or interior) and physical activity.
Considering mediation models (Table 4), we observed that loneliness and eat while watching TV or studying consistently mediated the association of both daily ultra-processed food consumption (loneliness: boys 17·4 %, girls 23·4 %; eat while watching TV or studying: girls 6·8 %) and TV viewing (loneliness: boys 22·9 %, girls 45·8 %; eat while watching TV or studying: boys 6·7 %, girls 17·9 %) with anxiety-induced sleep disturbance. Self-rated health mediated the association between daily ultra-processed food consumption and anxiety-induced sleep disturbance only among girls (9·5 %). Also, self-rated health (boys 14·2 %, girls 25·3 %) and body satisfaction (boys 9·0 %, girls 22·9 %) mediated the association between TV viewing and anxiety-induced sleep disturbance in both sexes.
Table 4 Mediation models for the association of daily ultra-processed food and TV-viewing with anxiety-induced sleep disturbance among adolescents
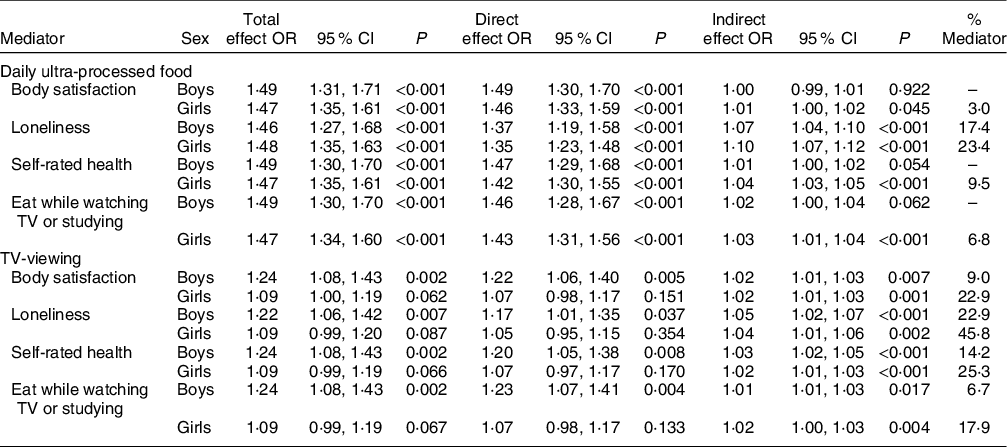
OR, odds ratio; CI, confidence interval.
Note. Adjusted by age group, ethnicity, food insecurity, country region, type of city (capital or interior) and physical activity.
Discussion
This cross-sectional study aimed to investigate the role of potential shared mediators of the associations of daily ultra-processed food consumption and TV viewing with anxiety-induced sleep disturbance. Our main finding was that daily ultra-processed food consumption and TV viewing have common mediators as loneliness and eat while watching TV or studying, and that the influence of the mediators can vary according to sex. This study advances the investigation of how ultra-processed food consumption and TV viewing, as well as their co-occurrence, can be associated with anxiety-induced sleep disturbance(Reference Werneck, Vancampfort and Oyeyemi5). Also, girls self-reported poorer health indicators, including anxiety-induced sleep disturbance, self-rated health, loneliness, body satisfaction as well as higher TV viewing and ultra-processed food consumption.
The present study is consistent with previous findings concerning the independent associations of daily ultra-processed food consumption and TV viewing with anxiety-induced sleep disturbance(Reference Vancampfort, Van Damme and Stubbs3–Reference Werneck, Vancampfort and Oyeyemi6). These independent associations can present different direct mechanisms, such as the blue light emission by television, which is associated with poorer sleep quality(Reference LeBourgeois, Hale and Chang22,Reference Tähkämö, Partonen and Pesonen23) . In addition, there are biological mechanisms linking sitting time and anxiety and sleep disturbance, such as the increase of inflammatory markers like IL-6 and C-reactive protein(Reference Endrighi, Steptoe and Hamer10). Similarly, the daily consumption of ultra-processed foods can present direct roles in the association with anxiety-induced sleep disturbance, that is, the increased consumption of fat, sugar and additives can also be associated with inflammatory markers and consequently sleep disturbance and insomnia(Reference Firth, Veronese and Cotter11,Reference Lopes, Araújo and Levy24) . However, these mechanisms have been less studied among adolescents.
However, we investigated the role of psychological/behavioural mediators such as body satisfaction, loneliness, self-rated health and eat while watching TV or studying. Body satisfaction is strongly related to weight status(Reference Reel, Voelker and Greenleaf25), which can be associated with anxiety(Reference Vannucci and Ohannessian26). However, we only found consistent mediation considering TV viewing, and not daily ultra-processed food consumption. A possible explanation could be through the stigmatization produced by the TV programmes(Reference Ata and Thompson27,Reference Eisenberg, Carlson-McGuire and Gollust28) . Therefore, weight stigmatization can be associated with poorer body satisfaction and consequently higher sleep disturbance(Reference Kelly, Zilanawala and Booker17). Self-rated health was also an important mediator concerning the association between TV viewing and anxiety-induced sleep disturbance. TV viewing is associated with self-rated health(Reference Osera, Awai and Kobayashi14), and self-rated health is closely associated with sleep disturbance(Reference Conklin, Yao and Richardson16).
We found that loneliness has a pivotal role in linking both daily ultra-processed food consumption and TV viewing with anxiety-induced sleep disturbance. This indicates that both behaviours are associated with social exclusion and frequently practised alone. Moreover, eating while watching TV is associated with considerably higher consumption of daily ultra-processed food(Reference Martines, Machado and Neri9). Therefore, it is also possible to interpret eating while watching TV or studying as an indicator of both behaviours co-occurring(Reference Ashdown-Franks, Vancampfort and Firth7,Reference Costa, Flores and Wendt8) . Thus, this co-occurrence can be a risk factor and links the social isolation caused by TV viewing with the daily consumption of ultra-processed foods, such as snacking and soft drinks consumption(Reference Werneck, Vancampfort and Oyeyemi5,Reference Ashdown-Franks, Vancampfort and Firth7,Reference Boulos, Vikre and Oppenheimer29) , and consequently with anxiety-induced sleep disturbance(Reference Eccles, Qualter and Madsen30).
We highlight that the associations of TV viewing and ultra-processed food consumption with anxiety-induced sleep disturbance can be bidirectional. Therefore, it is also possible that higher anxiety-induced sleep disturbance can lead to mediators and also to higher TV viewing and consumption of ultra-processed foods(Reference Beebe, Simon and Summer31–Reference Kruger, Reither and Peppard33). In this sense, higher sleep disturbance should lead to a lack of energy and consequently higher TV viewing, which could also pass through the mediators such as loneliness and eat while watching TV or studying(Reference Chaput and Dutil32). Also, previous studies have found that sleep deprivation can be associated with different food choices, especially increasing the consumption of sugary foods(Reference Beebe, Simon and Summer31,Reference Kruger, Reither and Peppard33) .
Our findings should be interpreted in the light of potential limitations. The cross-sectional design limits any inference of causality. Mediation models are causal models, and their interpretation is often limited in cross-sectional studies(Reference Fairchild and McDaniel34). However, there is a clear plausibility for the causal association between both exposures and mediators as well as between mediators and mental health(Reference Matias, Lopes and de Mello12–Reference Kelly, Zilanawala and Booker17). Also, there were no interactions between exposures and mediators, indicating that the mediators did not change the association between exposures and outcome, but reduced the degree of association. The consumption of ultra-processed foods relied on a 7-d recall on days per week, without further information on daily servings and specific calorie contribution of each food, which does not allow the estimation of a specific ultra-processed food’s contribution to daily energy demand. It being based on self-report, this information is prone to recall bias (7-d recall). Also, we did not consider potential unmeasured confounders such as weight status, pubertal status, parental history of mental disorders and peer influences on diet and TV viewing because such information was not available. On the other hand, we included a large nationally representative sample of Brazilian adolescents. To our knowledge, this is the first study aiming to investigate the potential common mediators of the associations of daily ultra-processed food consumption and TV viewing with anxiety-induced sleep disturbance. In terms of practical applications, these results not only reinforce the need of public health policies to reduce sedentary behaviours and unhealthy eating habits among adolescents but also indicate ways to build effective actions, focusing on the shared mediators that link TV viewing and ultra-processed food consumption with anxiety-induced sleep disturbance.
We conclude that daily ultra-processed food consumption and TV viewing share mediators in the association with anxiety-induced sleep disturbance, such as loneliness and eating while watching TV or studying. Therefore, both unhealthy lifestyle behaviours can act in synergic mechanisms in the association with anxiety disorders.
Acknowledgements
Acknowledgements: We gratefully acknowledge the contributions of all participants of the present research as well as the IBGE staff for data collection. Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. A.W. is supported by the São Paulo Research Foundation (FAPESP) with a PhD scholarship (FAPESP process 2019/24124-7). E.H. is supported by a National Health and Medical Research Council Early Career Fellowship (APP1156909). This paper presents independent research. The views expressed in this publication are those of the authors and not necessarily those of the acknowledged institutions. Conflict of interest: There are no conflicts of interest. Authorship: All authors listed met the conditions required for full authorship. Concept and study design, data analysis: A.O.W. and D.R.S. Interpretation of data: A.O.W., E.H. and D.R.S. Drafting of manuscript: A.O.W. Critical revision and approval of the manuscript for important intellectual content: all authors. Ethics of human subject participation: All procedures performed in the original studies involving human participants were approved by the National Health Research Ethics Council (CONEP: 1.006.467/2015) in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Data sharing statement: All data are open published as microdata at https://www.ibge.gov.br/estatisticas/sociais/populacao/9134-pesquisa-nacional-de-saude-do-escolar.html?=&t=microdados.





