


In recent decades, there has been an increase in BMI and waist circumference (WC) in women worldwide(1,Reference Walls, Stevenson and Mannan2) . Data from 186 countries revealed a BMI increase from 22·1 kg/m2 in 1975 to 24·4 kg/m2 in 2014 among adult women(1). Moreover, the National Health and Nutrition Examination Survey indicated a WC increase of 0·72 cm among women from 1988 to 2006, after adjusting for BMI(Reference Walls, Stevenson and Mannan2).
The increase in BMI and WC may be caused by multiple factors, including the consumption of processed and high energetic density foods as well as a lack of physical activity and sedentary behaviour levels(Reference Okop, Lambert and Alaba3,Reference Fuentes, Rowaedh and González4) . Sleep problems can also be highlighted as poor sleep quality and have been associated with increased BMI and WC(Reference Dekker, Noordam and Biermasz5–Reference Patterson, Malone and Grandner7). The mechanisms involved in this association, however, have not been fully explored(Reference Grandner8). It has been hypothesised that inadequate sleep may alter the balance between consumption and expenditure of energy, resulting in weight gain and abdominal fat accumulation, that is, inadequate sleep may be related to satiety and appetite-regulating hormones (decrease in leptin level and increase in ghrelin level, respectively)(Reference Broussard, Kilkus and Delebecque9–Reference Taheri, Lin and Austin11). This dysregulation may lead to greater consumption of high-energy-density foods such as sweets, snacks and sugary drinks(Reference Broussard, Kilkus and Delebecque9,Reference McNeil, Forest and Hintze12–Reference Prather, Leung and Adler16) . Four nights of sleep restriction, for example, may result in a higher energy consumption derived from foods rich in carbohydrates; sleep restriction elevated the consumption of sweet and snacks by approximately 1184 ± 544 kJ(Reference Broussard, Kilkus and Delebecque9).
Inadequate sleep can also cause fatigue during the day, which could decrease physical activity and increase sedentary behaviour(Reference Timmermans, Mackenbach and Charreire17–Reference Lakerveld, Mackenbach and Horvath23). A previous study revealed that individuals with poor sleep quality were 46 % more likely to be insufficiently active than those with good sleep quality(Reference Štefan, Sporiš and Krističević19); another study showed that individuals with short sleep duration (<6 h/d) had 26·5 min/d more sedentary behaviours than those with normal sleep (6–9 h/d)(Reference Lakerveld, Mackenbach and Horvath23). Additionally, inadequate sleep may alter cortisol secretion, a hormone involved in the regulation of body composition(Reference Huang, Poole and Vetter24). Sleep restriction may be related to the activation of the endocannabinoid system, which also regulates food intake and metabolism(Reference Hanlon, Tasali and Leproult25).
Although the mechanism that explains the association between inadequate sleep and anthropometric measurements may be mediated by behavioural issues, few studies have explored these relationships in adult women. Thus, this study aims to investigate the direct and indirect effects of poor sleep quality on BMI and WC in a sample of adult women from southern Brazil. Physical activity, sedentary behaviour and fast food consumption were explored as potential intermediate variables in these relationships.
Methods
A population-based cross-sectional study was conducted with a representative sample of women aged 20–69 years from the urban area of the city of São Leopoldo, Rio Grande do Sul, Brazil. A multiple-stage sampling design was adopted. In the first stage, forty-five census tracts of São Leopoldo were chosen by systematic random sampling. Next, the blocks and street corners that served as the starting point for each of the census tracts were randomly selected. Households were selected as follows: from the starting point in the first block, always proceeding to the left when facing the starting corner, the first house was selected for the study; the next two houses were skipped, and the third house was selected. This process was repeated until thirty-six households had been visited in each census tract.
The sample size was calculated to identify a 2·0 risk ratio at a 95 % confidence level, with a statistical power of 80 %, and maintaining a 1:2 unexposed:exposed ratio. The estimated sample size was increased in 10 % for possible losses and refusals and 15 % for possible confounding factors in the data analysis. Therefore, the final sample size was calculated as 1281 women. More details about the description of the sample size calculation, sampling and other study methodological procedures can be verified in a previous publication(Reference Neutzling, Leite and Paniz26).
Trained interviewers conducted interviews at the participants’ homes between February and October 2015 using a standardised and pretested questionnaire. Women who were pregnant at the time of the survey were excluded from the study. Data consistency was obtained by replication through telephonic interviews in 10 % of the sample.
BMI was assessed using the formula weight (kg)/height (m)2. Weight and height were measured using an analogue portable scale and a portable stadiometer, respectively. WC was measured at the midpoint between the last costal arch and the iliac crest using an inextensible measuring tape. All the measurements were taken twice, and the respective mean values were considered in the analysis. A third measurement was taken if there was a significant difference found in the first two measurements. All anthropometric measurements were taken by trained interviewers using standard protocols.
Sleep quality was assessed using the Brazilian version of the Pittsburgh Sleep Quality Index (PSQI-BR)(Reference Buysse, Reynolds and Monk27,Reference Bertolazi, Fagondes and Hoff28) . This questionnaire comprised nineteen questions that provided information on the sleep patterns during the previous month. The questions were subdivided into seven components: (1) subjective sleep quality, (2) sleep latency (time between bedtime and falling asleep), (3) sleep duration, (4) habitual sleep efficiency, (5) sleep disturbances, (6) use of sleep medication and (7) daytime dysfunction. Each component was scored from 0 to 3; thus, the total PSQI-BR score ranged from 0 to 21 points. In the analysis, the final score was used as a numerical discrete variable with higher scores indicating poorer quality of sleep.
Based on the literature review, three behavioural characteristics were collected and explored as intermediate variables: physical activity, sedentary behaviour and fast food consumption. The first was assessed using the short version of the International Physical Activity Questionnaire which comprises questions on the frequency and duration of commuting and leisure-time physical activities for a duration of at least 10 continuous minutes in the previous week (last 7 d). The physical activity level was determined by the total time spent in physical activities per week (a numerical continuous variable). Sedentary behaviour was assessed using an instrument to identify the time spent in leisure-time activities every day, including use of computer, tablet or cell phone; watching television and visiting or meeting relatives/friends and others. A numerical continuous variable was used considering the total time in hours/week in the analysis. Finally, fast food consumption in the last 3 months was assessed using a FFQ which collected data on consumption of fast foods (hamburgers, hot dogs, pizza, etc.) and, if so, the number of days per week (up to 7 d) or month (up to 10 d) they were consumed. These data generated a numerical discrete variable in relation to monthly fast food consumption.
Exploratory variables were used to characterise the sample and to control for possible confounding factors in the multivariate analysis. The demographic variables assessed were as follows: age, reported by the interviewee in years; skin colour, categorised as white and non-white and marital status, categorised as with and without a partner. Socio-economic variables included income and schooling. The first was estimated in monthly family income in Reais, and the second was measured as completed years of schooling. Behavioural variables were smoking status (non-smoker, ex-smoker and smoker) and alcohol consumption. Participants were asked about the usual frequency of alcohol consumption, including each type and amount of drink consumed in the last year. They were categorised into three groups: abstinence, light/moderate consumption (<15 g ethanol/d) and high consumption (≥15 g ethanol/d). Occupational variables included current occupation status (not working and working) and night shift (who reported work at least one night/overnight shift in her current or last job).
Statistical analysis
Data entry was performed using the EpiData version 3.1 software, including double entry and validation. Data analyses were performed using Stata version 13.0 and Mplus version 7.0. Numerical variables were described using mean and sd, and categorical variables were described using absolute and relative frequencies. There was no significant interaction between exposure and the intermediate variables (data not shown); thus, the classic direct effect between exposure and outcome was used(Reference Richiardi, Bellocco and Zugna29). Linear regression analysis with robust estimation was performed to verify the association between explanatory variables and outcomes (BMI and WC) in the bivariate analysis. Variables with a difference value lower or higher than 10 % in the adjusted-effect measures of association between PSQI-BR score with BMI and WC were used in the multivariate analysis. The possible confounding factors were selected a priori based on the following criteria: (a) be associated with the main exposure (sleep quality) in the literature; (b) be associated with the outcomes (BMI and WC) in the literature and (c) not be part of the causal chain between exposure and outcomes, nor a consequence of the outcomes(Reference Kleinbaum, Sullivan and Barker30). Direct and indirect effects were estimated using the path analysis technique. The theoretical model was developed based on the premise that behavioural factors may be indirectly involved in the association of poor sleep quality with BMI and WC increase. The analysis was conducted in stages as recommended by Hair et al. (Reference Hair, Black and Babin31). Nonstandard estimates (linear regression coefficients) of the effects were taken, and CI were obtained using the bootstrapping technique with 6000 resamples and maximum likelihood estimation. Missing data were analysed using full information maximum likelihood. The following criteria were used to check the quality of the model’s fit: χ 2 P-value > 0·05, Comparative Fit Index > 0·90, Tucker–Lewis Index > 0·90, RMSE of Approximation < 0·05 and Standardized Root Mean Squared Residual < 0·08. After estimating the proposed model, modification indices (>3·84) were verified to identify significant associations that could improve the model’s fit.
Results
Sample characteristics
Of the total sample, 153 (11·9 %) were considered losses or refusals and 11 (0·9 %) did not provide complete data for the exposures explored. Thus, the final analysis included a sample of 1117 women.
The mean age of the women was 43·3 (sd 13·4) years. They had a mean schooling and family income of 8·4 (sd 4·0) years and R$ 3596·00 (sd R$ 3355·00), respectively. Predominantly, the women were white, lived with a partner, were working and did not work in night shifts. Regarding behavioural characteristics, most did not smoke and consumed alcohol moderately. The mean time spent in physical activities per week was 0·85 (sd 2·0) h, while in sedentary behaviours was 25·1 (sd 22·7) h. The mean fast food consumption was 2·5 (sd 4·2) times/month. The mean PSQI-BR score was 5·6 (sd 3·4, median 5, minimum 0 and maximum 17). The mean BMI and WC were 28·3 (sd 6·2) kg/m2 and 90·3 (sd 14·7) cm, respectively (Table 1).
Table 1 Sample characteristics and unadjusted linear regression coefficients for BMI and waist circumference according to demographic, socio-economic and behavioural variables among Brazilian adult women (n 1117)
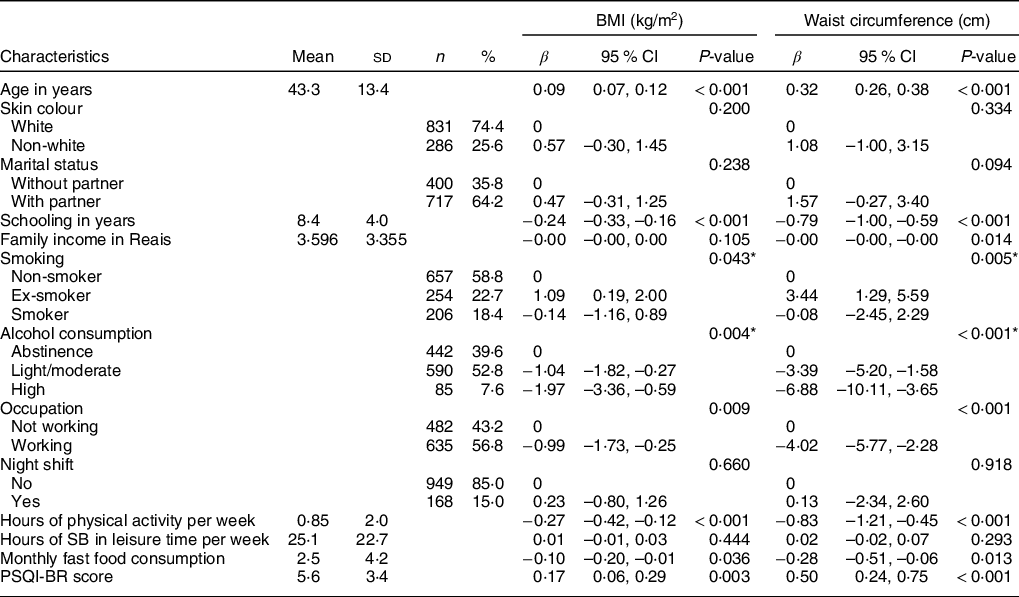
SB, Sedentary Behaviour; PSQI-BR, Brazilian version of the Pittsburgh Sleep Quality Index.
* Wald test for heterogeneity of proportions.
Association between explanatory variables and outcomes (BMI and waist circumference)
Table 1 shows the bivariate analysis for the association between explanatory variables and outcomes (BMI and WC). There was an increase in BMI and WC according to the increase in age, as well as in those who had stopped smoking, and in those with higher PSQI-BR scores. On the other hand, BMI and WC were lower in women with a higher education level, those with moderate and excessive alcohol consumption, who worked, with a high physical activity level and with high fast food consumption. Family income was only associated with WC.
The direct and indirect effects of poor sleep quality on the BMI and waist circumference (path analysis)
The variables with a difference value lower or higher than 10 % in the adjusted-effect measures of association between PSQI-BR score with BMI and WC were: age, education, alcohol consumption, occupation and night shift work; therefore, they were included in the final path analysis model. The goodness-of-fit test indicated an adequate model fit, and the verification of the modification indices showed that all significant associations were specified in the proposed model (Fig. 1). Women with poor sleep quality (higher PSQI-BR scores) showed a lower physical activity level (β = –0·05; 95 % CI –0·09, –0·01). The association between the PSQI-BR score and other intermediate variables was not significant (Table 2; Fig. 1).
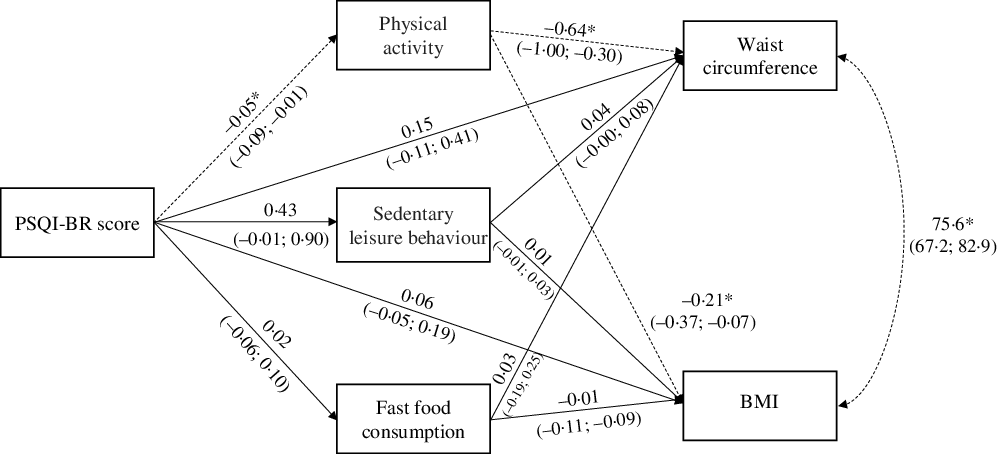
Fig. 1 Path diagram for direct and indirect effects of Brazilian version of the Pittsburgh Sleep Quality Index (PSQI-BR) score on BMI and waist circumference (WC) through behavioural factors in Brazilian adult women (n 1117) Rectangles represent observed variables. Straight lines with an arrow indicate direct effects. Curved lines with two arrows indicate covariance. Non-standardised coefficients and their respective 95 % CI were reported. The 95 % CI were estimated using the bootstrapping technique. Analysis was adjusted for age, schooling, occupation, night shift and alcohol consumption (omitted from the figure). *P < 0·01 (dashed lines). Model goodness-of-fit measures: df = 3; P-χ 2 value = 0·249; Comparative Fit Index (CFI) = 1·000; Tucker-Lewis Index (TLI) = 0·993; RMSE of Approximation (RMSEA) = 0·018; 95 % CI RMSEA = 0·000–0·057; Standardized Root Mean Squared Residual (SRMR) = 0·006
Table 2 Estimated non-standardised coefficients for poor sleep quality effects on BMI and waist circumference among Brazilian adult women (n 1117)
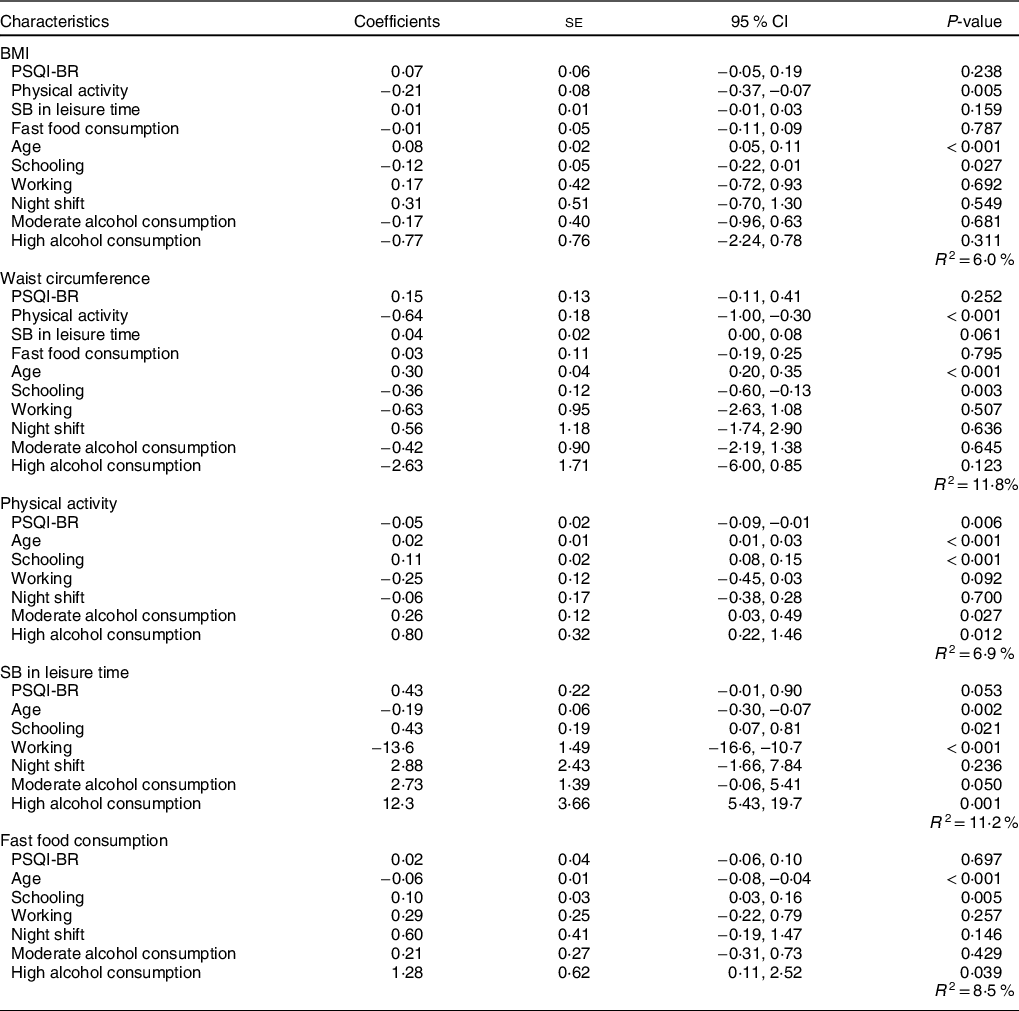
PSQI-BR, Brazilian version of the Pittsburgh Sleep Quality Index; SB, sedentary behaviour.
Physical activity level was inversely associated with BMI (β = –0·21; 95 % CI –0·37, –0·07); however, this variable showed no significant indirect effect with other intermediate variables on the association between the PSQI-BR and BMI. There was also no significant direct effect between the PSQI-BR score and BMI (Tables 2 and 3; Fig. 1). Regarding WC, physical activity level was associated with lower WC (β = –0·64; 95 % CI –1·00, –0·30). Additionally, less physical activity showed a significant indirect effect on the association between poor sleep quality and increased WC (β = 0·03; 95 % CI 0·01, 0·07). The indirect effects of sedentary behaviour and fast food consumption on the association between PSQI-BR score and WC were not significant (Tables 2 and 3; Fig. 1).
Table 3 Estimated coefficients for poor sleep quality effects on BMI and waist circumference via behavioural factors among Brazilian adult women (n 1117)
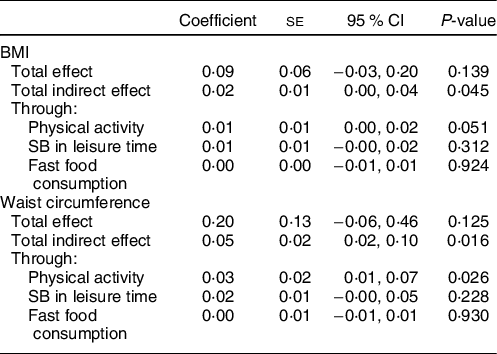
SB, sedentary behaviour.
Discussion
This study investigated the direct and indirect effects of poor sleep quality on BMI and WC in a representative sample of adult women in southern Brazil. There was no direct effect of poor sleep quality on BMI and WC. However, lower physical activity showed a significant indirect effect on the association between poor sleep quality and increased WC.
The mean BMI of this sample was higher compared with other international and national results in women; previous data revealed a mean of approximately 26·1 kg/m2 in Brazilian adult women, for example(1). We hypothesised that this may be because the prevalence of physically active women was lower. In our study, only 14·4 % were sufficiently active (>150 min/week), whereas in Brazilian national studies, it was between 30 and 45 %(Reference Casas, Bernal and Jorge32,Reference Cruz, Bernal and Claro33) .
Physical inactivity is one of the possible factors in which inadequate sleep may result in obesity; poor sleep quality may cause fatigue during the day, resulting in restricted daily activities and decreased energy expenditure. Similarly, a previous study showed that physical activity has an indirect effect on the association of sleep quality with BMI(Reference Magee, Reddy and Robinson34). Three indirect paths were observed in these associations: those with poor sleep quality, frequent sleep disorders and long-term sleep deprivation had a higher BMI because of low physical activity. However, there was no significant indirect effect for WC(Reference Magee, Reddy and Robinson34).
The relationship between sleep and physical activity has been explored. Sleep restriction (5·5 h/d) showed a reduction of 31 % in the step count and 24 % in the practice of moderate and vigorous physical activity compared with the control group (8·5 h of sleep per d) in a 1-week experiment(Reference Bromley, Booth and Kilkus18). For example, young Croatian adults with poor sleep quality (PSQI score > 5) were 46 % more likely to be insufficiently active than those with good sleep quality(Reference Štefan, Sporiš and Krističević19). In a North American longitudinal study, those individuals who reported better sleep quality at baseline showed a higher physical activity level at the end of the study(Reference Holfeld and Ruthig20). In addition, in a longitudinal study, Finnish adults with frequent symptoms of insomnia at baseline had a 27 % higher chance of being physically inactive at the end of the follow-up period(Reference Haario, Rahkonen and Laaksonen22).
There was no significant indirect association between sedentary behaviour and fast food consumption in this study. This may have occurred because the monthly fast food consumption reported was below expectations; for example, a Brazilian study estimated that 23 % of total energetic intake came from ultraprocessed foods(Reference Simões, Barreto and Molina35). Also, a lower fast food consumption has been observed among Brazilian women with economic disadvantage, and in older women (aged 40 years or over)(Reference Simões, Barreto and Molina35,Reference Fröhlich, Garcez and Canuto36) . This aspect may partly explain the low fast food consumption in this study sample. Moreover, fast food consumption and sedentary behaviour showed a high sd in this study.
Despite the above-mentioned results, previous studies found significant results. An increase in the PSQI score was associated with an increase in BMI through greater disinhibition of eating in adults from the USA, for example(Reference Blumfield, Bei and Zimberg37). Binge eating disorder partially mediated the association between poorer sleep quality (higher PSQI score) and higher BMI among Australian adults(Reference Yeh and Brown38). Sedentary work-related behaviour mediated the association between sleep duration and obesity in European adults(Reference Timmermans, Mackenbach and Charreire17). In addition, African-American adults with short sleep (≤6 h/d) had a higher BMI through sedentary behaviour(Reference Wu, Nguyen and Balachandran6).
There was no significant direct association of poor sleep quality with BMI and WC in this study. Other studies also did not show this association in adult women(Reference Liu, Qian and Wang39,Reference Vézina-Im, Lebel and Gagnon40) ; however, a significant association was previously reported in men(Reference Liu, Qian and Wang39). It is possible that women are more resilient to poor sleep effects than men and, therefore, require a greater degree of exposure to be affected(Reference Wells41).
Among the strengths of this study are the representative population-based design and the large sample size. Moreover, we used a validated instrument to identify multiple components of sleep quality and to test a mechanism that could explain the relationship between inadequate sleep and anthropometric measurements, considering behavioural factors as intermediate variables. Nevertheless, some limitations should be noted. First, the assessment of sleep quality was subjective and possibly influenced by response bias and inaccuracy; participants could underestimate sleep problems in relation to instruments that objectively assess sleep, such as actigraphy and polysomnography. Second, information about recent pregnancy or child rearing were not collected; this could influence the association between poor sleep quality and anthropometric measurements. Third, despite statistical significance, the magnitudes of the associations were low; however, our outcomes were prevalent, not diminishing the importance of the findings. Finally, because it is a cross-sectional study, a causal relationship was not established. Thus, there is the possibility of a reverse causality bias for associations. It is known that the association between sleep and obesity can be bidirectional, for example(Reference Sokol, Grummon and Lytle42). Individuals with obesity may have more sleep problems, such as obstructive apnoea syndrome(Reference Ogilvie and Patel43). However, a previous study revealed that the effect of obesity on poor sleep quality was less robust and consistent(Reference Madrid-Valero, Martinez-Selva and Ordonana44). The association between sleep and physical activity can also be bidirectional. The practice of physical activity could be linked to significant effects on sleep; however, most of these associations explored sleep duration(Reference Kline45). Additionally, the other two longitudinal studies demonstrated only a significant effect of sleep problems on the practice of physical activity; that is, the inverse association was not significant(Reference Holfeld and Ruthig20,Reference Haario, Rahkonen and Laaksonen22) . Even so, our results can support the formulation of hypotheses to be tested by longitudinal studies using objective instruments to assess sleep quality.
The present study identified direct and indirect effects on the association between poor sleep quality and anthropometric measurements in adult women. This is the first study that revealed a significant indirect effect of low physical activity level on the association between poor sleep quality and increased WC in women. Taking into account the multifactorial aetiology involved in the development of abdominal obesity, this study highlights the causal chain of this condition as well as the importance of prevention strategies.
Acknowledgements
Acknowledgments: H.M.L. received a scholarship from the Coordenação de Aperfeiçoamente de Pessoal de Nível Superior – Brasil (CAPES). M.T.A.O. received research productivity grant from the National Council of Technological and Scientific Development (CNPq; grant 307175/2017-0). J.S.D.C. received research productivity grant from the National Council of Technological and Scientific Development (CNPq; grant 310599/2018-0). Financial support: This study was financed in part by the Coordenação de Aperfeiçoamente de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001. The funders had no role in study design, data collection and analysis, decision to publish and the preparation or approval of the manuscript. Conflict of interest: The authors declare no conflicts of interest. Authorship: H.M.L. and M.T.A.O. participated in the study concept and design, analysis and interpretation of data, the writing of the first draft of the manuscript and critical review of intellectual content. A.G., F.B. and J.S.D.C. contributed to the study concept and design, interpretation of data and critical review of intellectual content. All authors have approved the final version of the manuscript and are responsible for all aspects of the work in ensuring the accuracy and completeness of any part of the work. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the Research Ethics Committee of UNISINOS (number 650.443). Written informed consent was obtained from all subjects/patients.




