


The disparities in health between groups with high and low socio-economic position (SEP)(Reference Mackenbach, Stirbu and Roskam1) are also apparent in their diets. High-SEP groups have healthier intakes of key nutrients(Reference Kant and Graubard2, Reference Lopez-Azpiazu, Sanchez-Villegas and Johansson3), higher intakes of fruit and vegetables(Reference Kant and Graubard2, Reference Irala-Estevez, Groth and Johansson4, Reference Bihan, Castetbon and Mejean5) and healthier dietary patterns(Reference Kant and Graubard2, Reference Mullie, Clarys and Hulens6–Reference Boylan, Lallukka and Lahelma8) than low-SEP groups. One of the reasons for the inequity in dietary intake might be the cost of healthy eating(Reference Drewnowski and Eichelsdoerfer9).
There is increasing knowledge about the relationship between consumer food costs and diet. In theory, it is quite possible to compose a nutritious diet at low cost(Reference Carlson, Lino and Juan10, Reference Maillot, Ferguson and Drewnowski11). However, these theoretical diets do not always correspond to real-life situations(Reference Blisard and Stewart12, Reference Maillot, Darmon and Drewnowski13). Generalized models of healthy diets, planned on a food group level, have been shown to be too expensive for low-SEP families(Reference McDermott and Stephens14, Reference Kettings, Sinclair and Voevodin15). When comparing costs of consumed diets, studies show somewhat mixed results: cross-sectional dietary surveys often show that healthier diets cost more(Reference Townsend, Aaron and Monsivais16–Reference Bernstein, Bloom and Rosner24) while in intervention studies, on the other hand, the healthy diets are often less expensive than the control diet(Reference Burney and Haughton25–Reference Raynor, Kilanowski and Esterlis28); although contradicting examples can be found(Reference Stender, Skovby and Haraldsdottir29, Reference Ryden, Sydner and Hagfors30).
Although accumulating evidence indicates that healthy eating is more expensive, the need for additional studies of consumed diets is apparent. An intriguing question that has not yet been fully answered is why a healthier diet costs more. Energy-dense foods, which contribute to a less-healthy diet if eaten in excess(Reference Patterson, Warnberg and Poortvliet31), are often cheaper(Reference Drewnowski and Darmon32); however, the complexity of dietary behaviour implies that this is not the only reason for differences in diet costs. It is also important to investigate costs in different parts of the world, because food prices and dietary habits differ among countries(Reference Slimani, Fahey and Welch33). Few studies have examined the relationships among diet, cost and socio-economic variables.
The aim of the present study was to examine diet costs in relation to dietary quality and SEP in Swedish children. We also investigated reasons for differences in diet costs by relating cost to intake on a food group level. To our knowledge, no other studies in this area have been conducted using the dietary intake of children. If healthy food cost is related to SEP, it is an important incentive for updated public health policies.
Materials and methods
Dietary intake data were collected in 2003 in a Swedish national food survey called ‘Riksmaten – children’(Reference Enghardt Barbieri, Pearson and Becker34). The population consisted of randomly selected children, who were 4, 8 or 11 years old, from a stratified sample of municipalities representative of Sweden. The stratification considered regional differences and parents’ income and education. The 4-year-old children were selected individually, while the 8- and 11-year-olds were included class-wise (grades 2 and 5) from randomly selected schools. In total, 3423 children were sampled (924 children aged 4 years, 1209 children from grade 2, 1290 children from grade 5). Of these children, 3055 (89 %; 823, 1070 and 1162 children who were 4, 8 and 11 years old, respectively) agreed to participate, and 2535 (74 %; 590, 909 and 1036 children who were 4, 8 and 11 years old, respectively) completed the study. Forty-one children were excluded due to incomplete dietary data, leaving a final population of 2494 children (49 % girls).
Assessment of dietary intake, BMI and sociodemographic factors
Dietary assessments were made using open, estimated food diaries covering four consecutive days. All days of the week were evenly represented. Parents or other caregivers were responsible for the diaries of the 4-year-olds, whereas the schoolchildren registered their dietary intake by themselves or with assistance from an adult (parent and/or teacher). Specially trained informers visited the families of each 4-year-old to inform them about the survey and how to complete the food diary. Information was provided to the schoolchildren by informers who visited teachers and children in the selected classes. The food diaries were designed to be suitable for the different age groups and contained written instructions regarding the dietary assessment. During the four recording days, all foods, beverages and supplements were registered. Consumed amounts were estimated in household measures or by comparisons with a book containing pictures of different portion sizes.
The estimated intakes of energy and nutrients (including supplements) were calculated using the nutritional analysis package MATs version 4·03 (Rudans Lättdata, Västerås, Sweden) based on the Swedish National Food Administration's food composition database (version 04·1·1). In addition to the food diary, a questionnaire containing questions about the child's weight and height and parents’ education and occupation was answered. BMI was calculated from self-reported weight and height. The validity of reported energy intake was evaluated by comparing the ratio between reported energy intake (EI) and BMR with the lowest ratio plausible (EI:BMR = 1·06) for a dietary assessment over 4 d(Reference Goldberg, Black and Jebb35). The BMR was estimated according to standard equations using body weight, age and sex(Reference Becker, Lyhne and Pedersen36). If data regarding weight were missing, the BMR was calculated using age- and sex-adjusted group means. Of 2494 children, 334 (13·4 %) were classified as under-reporters and hence excluded from the analysis, leaving a total of 2160 children.
Measures of dietary quality
The 2005 Healthy Eating Index (HEI) was used to assess the healthiness of the dietary intakes(Reference Guenther, Reedy and Krebs-Smith37). In short, HEI accounts for both food and nutrient intakes and includes adequacy components as well as moderation components (Table 1). Using twelve components, a total HEI score ranging from 0 to 100 is calculated, with a higher score indicating a healthier diet. An advantage of HEI is the energy adjustment (all components are calculated per 4184 kJ (1000 kcal)), which makes it possible to evaluate diet quality while controlling for diet quantity, important when studying children of different ages.
Table 1 Healthy Eating Index-2005 components and scoring, adopted from Guenther et al.(37)
DGaOVaL, dark green and orange vegetables and legumes; SoFAAS, solid fats, alcoholic beverages and added sugars.
†Includes 100 % juice.
‡Includes all forms except juice.
§Includes legumes only after meat and beans standard is met.
||Includes all milk products such as fluid milk, yoghurt and cheese, and soya beverages.
¶Includes legumes only if the meat and beans standard is otherwise not met.
††Includes non-hydrogenated vegetable oils and oils in fish, nuts and seeds.
‡‡1 cup = approx. 237 ml.
§§1 oz = approx. 28·4 g.
Minor adjustments were made for the solid fat, (alcohol) and added sugar component; fat levels above the Swedish ‘Keyhole Symbol’ (indicating healthier alternatives within a food group(Reference Jansson38)) were considered as excess fat for the milk and meat and beans components, instead of the original threshold ‘lowest fat form’(Reference Guenther, Reedy and Krebs-Smith39). In addition, added sugar was calculated using sucrose content, as specified in the Swedish Food Database(40).
Total HEI score can be used to classify diets as ‘poor’ (total HEI score <50), ‘needs improvement’ (score 50–80) or ‘good’ (score >80)(Reference Kennedy41). However, because only three children had a total HEI score above 80 (0·1 %), diets with an HEI score >70 were classified as high-HEI diets.
Energy density (MJ/g) was calculated including beverages. Food intake variation was defined as the number of unique food items reported during the data collection period, disregarding the amount consumed.
Food price information
Food price data were compiled from national average prices collected by Statistics Sweden for 391 out of a total of 991 food items covering 71 % of the food intake. Prices for the remaining 600 food items were collected mainly from one online supermarket and one online grocery store. Both had the same prices online as in their physical store, but average prices were significantly higher at the grocery store. Hence, because the supermarket was part of a brand chain holding approximately 50 % of the market share(Reference Nordenskiöld42) and a majority of Swedish families with children shop at supermarkets(43), average prices were weighted 70/30 towards supermarket prices. Prices for meals from restaurants and fast foods were collected from Statistics Sweden and fast-food restaurants. Total food costs are presented as €/4184 kJ (1000 kcal).
All of the prices were collected in the spring of 2010. This could impose seasonal differences in the prices of fruits and vegetables. However, the average prices of fruit and vegetable staples have low seasonal variability in Sweden, with the exception of harvest season in late summer/early autumn. No dietary data were collected during this period.
The amount of food consumed was recalculated into the amount of food purchased using factors adjusting for waste and water retention/loss during cooking (e.g. 100 g of banana eaten was multiplied by a factor of 1·59 (representing the weight of the banana peel), resulting in 159 g of banana purchased).
Each food item was classified into a food group (Table 2). Subgroups were created for food groups in which healthier options were available. These reflect the subcategories in HEI (i.e. healthier option in the fruit group is the same as the whole-fruit category in HEI). In HEI, some categories are not mutually exclusive; i.e. the fatty part of a sausage is counted in the solid fat, alcohol and added sugar category, while the sausage as a whole is counted in the meat and beans category. For the food group classification, each food is represented in one food group only and, where applicable, in a subgroup. The food groups were used to assess costs as percentage of total costs, costs per 100 g, and number of unique food items within groups.
Table 2 Definition of food groups and subgroups used to analyse differences in cost
†As specified in Healthy Eating Index-2005(Reference Guenther, Reedy and Krebs-Smith37).
Statistical analysis
All statistical analyses were performed using PASW Statistics statistical software package version 18·0 (SPSS Inc., Chicago, IL, USA). When comparing groups, the Student t test for independent samples, the Mann–Whitney U test, one-way ANOVA, the Kruskal–Wallis test or the χ 2 test was used. Post hoc tests were performed using the Tukey HSD test for ANOVA and the Dunn test for Kruskal–Wallis. Multivariate analyses were made using analysis of covariance for adjusted differences between socio-economic variables and standard linear multiple regression to assess relationships between total dietary cost and food groups. P values below 0·05 (two-sided) were considered to be statistically significant.
Effect size was calculated to assess the magnitude of significant differences by using η 2 for the t test and ANOVA, and φ or Cramer's V for χ 2. Low effect size is stated in the Results section.
Results
The average total HEI score for the whole group was 59·99 (sd 7·80). Children with a total HEI score below 50 (n 221, 10·2 %) formed the low HEI-score group. Correspondingly, those with a total HEI score above 70 (n 202, 9·4 %) formed the high HEI-score group (Table 3). The high HEI-score group had a more favourable dietary intake when comparing individual nutrients, energy density and HEI component scores with those of the low HEI-score group.
Table 3 Descriptive characteristics of groups with low, intermediate and high total HEI score
HEI, 2005 Healthy Eating Index; P25–P75, 25th–75th percentile; ISO-BMI, age-adjusted BMI; EI, energy intake; %E, percentage of total energy intake; DGaOVaL, dark green and orange vegetables and legumes; SoFAAS, solid fat, alcohol and added sugar.
4184 kJ = 1000 kcal.
†HEI < 50, n 202; HEI = 50–70, n 1547; HEI > 70, n 177.
‡P for difference between HEI < 50 and HEI > 70, as calculated by Student's t test.
§P for difference between HEI < 50 and HEI > 70, as calculated by χ 2 (sex and ISO-BMI) or Mann–Whitney U test.
Energy-adjusted costs showed that the diet of the high HEI-score group was more expensive (mean difference €0·34/4184 kJ, sd 0·018, P < 0·001; Table 3). The largest proportion of the cost was placed on meat (17·3 %) in the high HEI-score group and on discretionary calories (25·4 %) in the low HEI-score group (Fig. 1). The high HEI-score group had higher average costs for fruits, vegetables, fish, poultry and grains, while the low HEI-score group had higher costs for discretionary calories, ready meals, miscellaneous and fat (P < 0·001, except for fat P = 0·003). Dividing food groups into subgroups based on healthier options (as defined in Table 2) emphasized the differences in costs between the high- and low HEI-score groups, with the high HEI-score group having higher costs in all of the healthier food groups (P < 0·001).
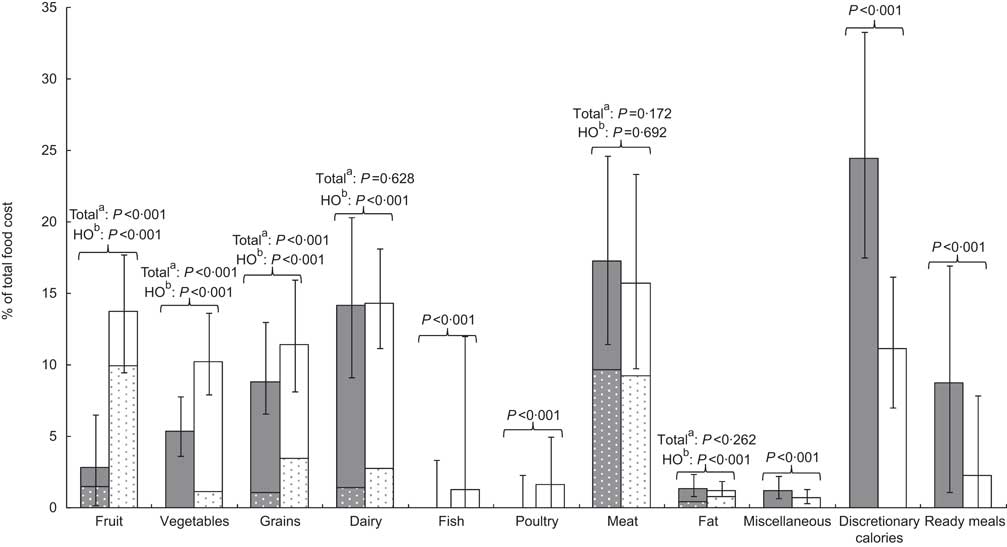
Fig. 1 Comparison of cost per food group, subdivided into the healthier option (HO) within the food group where applicable (![]() ,
, ![]() ), as median percentage of total food cost between the group with low 2005 Healthy Eating Index (HEI) score (HEI < 50, n 221;
), as median percentage of total food cost between the group with low 2005 Healthy Eating Index (HEI) score (HEI < 50, n 221; ![]() ) and the group with high HEI score (HEI > 70, n 202;
) and the group with high HEI score (HEI > 70, n 202; ![]() ), with 25th and 75th percentile values represented by error bars. aP value for the whole food group including part from the HO; bP value for the HO part of the food group
), with 25th and 75th percentile values represented by error bars. aP value for the whole food group including part from the HO; bP value for the HO part of the food group
Dividing the participants into quintiles based on dietary costs revealed the same pattern: spending more money on food resulted in higher total HEI scores (mean difference in HEI score, lowest v. highest: 4·85, sd 0·15, P < 0·001; Table 4). Energy density decreased with rising food costs (P < 0·001). Post hoc tests revealed that those in the highest cost quintile consumed more fish, poultry, fruit, ready meals, vegetables, meat and miscellaneous products than those in the lowest cost quintile (P < 0·001 to P = 0·007), while those in the lowest cost quintile consumed more dairy products (P < 0·001), expressed as grams per 4184 kJ. When comparing nutrient intakes, the highest cost quintile generally had a more favourable nutrient profile, with the exception of a lower intake of Ca and a higher intake of Na (P < 0·001 to P = 0·047); however, the magnitude of the differences was low, except for protein (percentage of energy), fibre and Na (data not shown).
Table 4 Characteristics of participants and their food intake according to daily food costs. Data are presented as mean and standard deviation for normally distributed variables or median and 25th–75th percentile where data are skewed

HEI, 2005 Healthy Eating Index; ISO-BMI, age-adjusted BMI; EI, energy intake; DGaOVaL, dark green and orange vegetables and legumes; HO, healthier option.
4184 kJ = 1000 kcal.
†Q1, n 373; Q2, n 399; Q3, n 397; Q4, n 386; Q5, n 371.
‡P for difference between groups as calculated by ANOVA.
§P for difference between groups as calculated by χ 2 (sex and ISO-BMI) or Kruskal–Wallis test.
Constitutions of differences in food costs
The highest cost quintile consumed a more varied diet (number of unique foods, Q5 v. Q1: 54·20 v. 45·98, P < 0·001; Table 4), as did the high HEI-score group (high HEI v. low HEI: 54·02 v. 47·23, P < 0·001; Table 3). In both comparisons, vegetables and fruit accounted for about half the difference in variety (data not shown).
A standard multiple regression was performed with total cost per 4184 kJ as the dependent variable and consumed amount of food (g/4184 kJ) from the different food groups as the independent variables. The adjusted R 2 value of 0·465 indicates that less than half of the variability in costs was explained by the amount of food ingested from various food groups (Table 5). However, fish, meat, fruit and ready meals together accounted for just over half of the variability in total cost (sum of unique variability = 0·586), implying that these food groups are the major contributors to the differences between high- and low-cost diets. The regression also implies that if, for example, fish intake increases by 10·92 g (1 sd), total food cost is likely to increase by €0·20 (β for fish (0·453) multiplied by sd for total cost (€0·45)).
Table 5 Standard linear multiple regression of food intake, measured as g/4184 kJ within food groups, v. total food cost (€/4184 kJ) including correlation coefficients between all variables (n 2160)
4184 kJ = 1000 kcal.
Significance: *P < 0·05, *P < 0·01, ***P < 0·001.
†Unique contribution to regression from variable, expressed as R 2.
‡Unique variability for all variables contributing significantly to model = 0·586.
By comparing cost per 100 g from different food groups among different cost quintiles, we determined that the highest cost quintile consumed more expensive foods within almost all food groups (Table 4). The largest differences between the highest and lowest cost quintiles were found for fish (mean difference €0·52, sd 0·04, P < 0·001), ready meals (mean difference €0·50, sd 0·35, P < 0·001) and meat (mean difference €0·16, sd 0·05, P < 0·001).
Socio-economic position in relation to 2005 Healthy Eating Index and cost
There were significant differences in both total HEI score and total cost in relation to parental education and occupation, but the magnitude of the differences was low (Table 6). Children whose parents had a university degree (n 1023) had a total HEI score that was 4·25 points higher on average (sd 0·61, P < 0·001) and they consumed a more expensive diet (mean difference €0·17/4184 kJ, sd 0·02, P = 0·009) than children with less-educated parents (primary school, n 73). Differences among occupational levels were smaller but still significant for both total HEI score (P = 0·001) and cost (P = 0·001). The differences remained after adjusting for age and cost or total HEI score, but were weakened slightly.
Table 6 Socio-economic position in relation to total dietary cost and total HEI score
HEI, 2005 Healthy Eating Index.
4184 kJ = 1000 kcal.
†Adjusted for total HEI score, age and sex of child.
‡Adjusted for cost/1000€, age and sex of child.
§P for difference between groups as calculated by ANOVA.
||P for difference between groups as calculated by analysis of covariance.
Discussion
The present study showed that higher dietary costs were associated with healthier eating in Swedish children. Children with higher total HEI scores had a more expensive diet, and those spending the most money on food consumed a healthier diet. This is in line with other studies showing that healthy diets cost more(Reference Townsend, Aaron and Monsivais16–Reference Waterlander, de Haas and van Amstel21, Reference Bernstein, Bloom and Rosner24). The magnitude of the difference in cost between healthy and less-healthy diets might seem rather small (€0·34/4184 kJ (1000 kcal)), but it corresponds to approximately €1000/year for a family of four.
There are most likely several reasons why healthier diets are more expensive. One reason is that energy-dense foods may be cheaper, as measured by cost per kilojoule(Reference Drewnowski and Darmon32). In our study, energy density decreased when food expenses and the healthiness of the diet increased, as has also been shown by others(Reference Townsend, Aaron and Monsivais16, Reference Murakami, Sasaki and Okubo44). Because energy density can serve as a marker for dietary quality(Reference Patterson, Warnberg and Poortvliet31) – the lower the energy density, the better the dietary quality – it makes sense that those consuming an energy-dense diet scored low on the HEI. Those with high scores on the HEI spent approximately 25 % of their food budget on fruit and vegetables, food groups characterized by their low energy density, whereas the low HEI-score group spent 25 % of the food budget on discretionary calories, for which energy density is high. Another explanation for why energy density is associated with diet cost is that one must eat more food to reach energy equilibrium if foods with low energy density are chosen(Reference Rolls, Drewnowski and Ledikwe45). Although food prices differ among and within food groups, almost all foods cost money, and increased food intake when eating low energy-dense diets will thereby increase food costs.
Another reason why healthier diets are more expensive might be due to price differences among healthy and less-healthy products within food groups. However, healthier options within a food group are not necessarily more expensive. Wholegrain products and healthier fat products are, in fact, cheaper per gram compared with their respective food groups as a whole. Healthy dairy products, on the other hand, are about twice as expensive as the total dairy group, and the average price for healthier meat options was about €1 more expensive per kilogram. This indicates that within some food groups, it is possible to choose healthier alternatives without increasing food costs, whereas in other food groups, food costs are likely to increase if healthier alternatives are chosen.
Yet another reason why healthier diets are more expensive may be due to the amount of intake within more expensive food groups, if these coincide with healthier food groups. Multiple regression analysis showed that fish, meat, fruit and ready meals accounted for more than half of the differences in total cost. With the exception of fruit, these food groups represented those with the highest cost per gram. They also represented food groups in which relative intakes increased the most among cost quintiles. This increased intake in approximately the same food groups was also found in other studies when intake was stratified by total dietary cost(Reference Lopez, Martinez-Gonzalez and Sanchez-Villegas23, Reference Murakami, Sasaki and Okubo44). High intakes of fish and fruit are consistent with healthy eating, but ready meals and meat are not generally considered to be healthy(46). However, more than half of the meat consumption in the highest cost quintile consisted of healthier options, such as lean meat and low-fat products. The healthiness of ready meals varies greatly depending on product type, and meals at restaurants are likely to be healthier than fast-food meals(Reference Duffey, Gordon-Larsen and Steffen47). In Sweden, it is generally more expensive to dine at restaurants than to buy fast foods, and the higher average cost for ready meals in the highest cost quintile could be due to a higher proportion of restaurant meals. Therefore, total food cost will increase if healthier food choices lead to higher intake from food groups in which average prices are high, even more so if healthier selections within food groups have a higher price than the group average.
A final reason why healthier diets are more expensive is that healthy diets often include a greater variety of foods(Reference Drescher, Thiele and Mensink48). In our study, the highest cost quintile consumed the largest number of unique food items, as did the high HEI-score group. On a food group level, fruit, vegetables, fish, meat (healthier options) and ready meals accounted for the majority of the difference in variety. These food groups are also those in which relative intake and cost per gram increases the most with rising food costs. This implies that a larger intake within food groups will comprise greater variety, perhaps because it might not be satisfying to eat the same food repeatedly. It also implies that it might not be possible to find alternative foods within the same food group at the same price; therefore, dietary costs would rise with increasing dietary variety.
A possible consequence of higher dietary costs when eating healthily is that low-SEP groups will find it too expensive to adhere to a healthy diet. In the present study, we found a small but significant indication that children whose parents had lower educational and occupational levels consumed a cheaper and less-healthy diet. The relationship between dietary quality and SEP is in line with several other studies based on both Swedish and international data(Reference Kant and Graubard2–Reference Dynesen, Haraldsdottir and Holm7, Reference Wadman, Boström and Karlsson49). There are, however, few studies examining the relationship between actual dietary costs and SEP. Waterlander et al. found no difference in actual food costs among income levels in adults; however, they suggested that the lack of significance could be due to the small number of participants in the low-income groups(Reference Waterlander, de Haas and van Amstel21). On the other hand, low-SEP groups have been found to spend less money on food(Reference Inglis, Ball and Crawford50, Reference Kirkpatrick and Tarasuk51) and to have less-healthy food purchasing behaviour(Reference Inglis, Ball and Crawford50, Reference Giskes, Van Lenthe and Brug52, Reference Turrell, Bentley and Thomas53), indicating the likelihood of lower actual dietary costs with lower SEP. This implies that one of the reasons for the less-healthy dietary pattern associated with low SEP is the cost of healthy eating.
Some limitations of our study are worth noting. Although we excluded obvious dietary under-reporters, our cut-off point at EI:BMR = 1·06 is likely to have allowed some under-reporters to be included. Because under-reporting is biased towards unhealthy foods(Reference Livingstone and Black54), it is possible that the high HEI scores were overestimated. This is indicated by the differences in food intake levels among HEI groups. However, it is unclear to what extent total food costs might have been affected by selective under-reporting; there was a significant difference in food intake level between the highest and lowest cost quintiles, but it is likely that the energy adjustment decreased the effect of the under-reporters.
Disposable income is likely a more important determinant with regard to food budget choice than SEP markers such as education and occupation. Although these SEP markers can be seen as reflecting income, recent studies have shown that financial situation, rather than education or occupation, is associated with a higher fruit and vegetable intake(Reference Bihan, Castetbon and Mejean5, Reference Boylan, Lallukka and Lahelma8, Reference Lallukka, Pitkaniemi and Rahkonen55). Knowledge of disposable income and/or the current financial situation of children's families might have strengthened the weak relationship between SEP groups and diet cost in our study.
Although we put much effort into verifying the accuracy of food price information, there were some shortcomings: the lack of details about the foods consumed made it necessary for us to use the average price of each food instead of using actual prices. It is likely that low-SEP families use discounts and low-cost foods to reduce food costs(Reference Inglis, Ball and Crawford50) to a larger extent, which would increase differences in total food costs compared with high-SEP families. Furthermore, food prices were collected 7 years after the diet survey was conducted. During these years, prices might have changed both within and among food groups(Reference Monsivais and Drewnowski56), which in turn could have affected dietary intake, because cost is one determinant of food purchase(Reference Glanz, Basil and Maibach57). It is also likely that the ready meals food group was underestimated, as all meals were considered home-cooked unless clearly stated otherwise. This could change the impact of ready meals on total food costs, but because the food group comprises meals bought in grocery stores, meals from restaurants and fast food, it is unclear how the underestimation would have affected food costs.
It is also important to consider that all of the participants were children. In Sweden, all school children are provided free school lunches and a majority of 4-year-olds are enrolled in day-care, where all meals are free. However, costs for these meals were calculated as if they were home-cooked. Both school and day-care meals are usually planned by nutritionally trained managers (although often with budget restraints). Hence, dietary intakes might be healthier in these settings than diets eaten within a family setting.
The strength of our study is that dietary data were based on a large number of nationally representative children using an open-survey technique (food diaries) instead of a predefined technique, such as an FFQ. When considering food costs, it is important to investigate food intake in as much detail as possible.
Conclusion
Healthy eating was associated with higher dietary cost in Swedish children. Important reasons for this are: (i) differences in food prices, in which healthier options such as fish and lean meats were more expensive; (ii) increased intakes of less energy-dense foods; and (iii) a higher cost when consuming a more varied diet. Because higher dietary costs are likely to be a barrier for low-income groups with regard to eating healthily, as indicated in our study, this result poses challenges for public health policies, especially when considering the existing inequalities in health among SEP groups. It also poses challenges for nutrition professionals who are providing dietary advice for diverse groups in society, since being informed about and considering the costs of different foods increases the likelihood of implementing successful dietary changes. Although the results of the study are in line with previously published research, the major disadvantage of the current study was the generalizations made when retrospectively connecting food prices to dietary data, which could have biased the results. Future studies should focus on true food expenditure, including discounts, in combination with detailed dietary intake data. It is also important to include valid SEP variables, preferably with information about disposable income.
Acknowledgements
This research was funded by the Swedish Nutrition Society. There were no conflicts of interest. P.J.R. designed the study, carried out the data collection, performed the analysis of the data and drafted the manuscript. L.H. participated in the design of the study, helped to analyse the data and helped to draft the manuscript. The authors would like to thank Agneta Hörnell and Phil Lyon for valuable comments and support.







