


Several scientific reports have shown that the obesity epidemic has reached children and adolescents in Europe. The reports suggest that there are clear geographic differences within the continent, with southern Europe and the British Isles reporting the highest prevalence rates of overweight/obesity among children and adolescents(Reference Branca, Nikogosian and Lobstein1–Reference Currie, Gabhainn and Godeau4). In 2007, WHO Europe published a report on the challenge of obesity in Europe(Reference Branca, Nikogosian and Lobstein1). It was concluded that objectively measured and valid data on BMI were lacking for about half of the European countries. Furthermore, making comparisons between countries was difficult due to great variation in response rates, age ranges included, years of data collection and definition of overweight and obesity(Reference Branca, Nikogosian and Lobstein1). Considering the importance given to childhood obesity in the current public health discourse, as well as the urgent need to have high-quality data to inform policy formation and interventions, it seems important to assess to what extent these methodological challenges are being addressed in the more recent publications. Thus, the aim of the present paper is to provide an updated review of available data objectively measuring overweight/obesity in national representative samples of European adolescents (aged 10–18 years). Furthermore, the aim was to review available studies assessing trends in overweight/obesity over time in this target group, and to evaluate the ability of these data to describe the obesity epidemic across sociodemographic subgroups.
Methods
Data on prevalence rates and trends in overweight/obesity among adolescents (aged 10–18 years) in the twenty-seven European Community member states, Iceland, Norway and Switzerland were retrieved up until the end of 2009 from the following three sources: (i) a systematic search in the MedLine database combining the general search: ((Child OR Adolescent) AND (Overweight OR Obesity OR Body Mass Index OR BMI) AND (Trend OR Prevalence)) with each of the country names and including only reports published in English. The reference lists of selected articles were screened for other relevant studies. (ii) Data from the WHO Nutrition Policy Database(5) and the report ‘The challenge of obesity in the WHO European Region and the strategies for response’(Reference Branca, Nikogosian and Lobstein1) were searched for additional data. (iii) The WHO regional office for Europe and the International Obesity Task Force (IOTF) were contacted to obtain the most recent data on overweight/obesity among adolescents in the region. The latter two sources also contained data not published in scientific international journals. From these three sources, reports on the most recent (from 1995 until the end of 2009) objectively measured height and weight of national representative samples of adolescents were abstracted.
No inclusion criteria with regard to study quality were used to present the total picture of the data available. To evaluate whether comparability across studies had improved and the ability of the studies/reports to describe the obesity epidemic among adolescents in Europe, the following information was abstracted for the prevalence studies: year of data collection, sample size, response rate, age range included, trends by age, definition of overweight/obesity, sociodemographic variables and the source of information. For the trend data, the following information was abstracted: year of data collection, age, definition of overweight/obesity, number of cross-sectional surveys, sample size, method of data collection (self-reported, measured or measured register data) and type of sample (national or other).
The 2001–2002 and 2005–2006 WHO Collaborative study: Health Behaviour in School-aged Children (HBSC) reports(Reference Currie, Roberts and Morgan3, Reference Currie, Gabhainn and Godeau4) were used to assess trends and checked for the availability of data in countries lacking objectively measured data on overweight/obesity from national representative samples. HBSC is a survey of 11-, 13- and 15-year-olds in forty-one countries (mainly in Europe and North America) conducted every fourth year.
Results
Prevalence of overweight in national representative samples based on objective measurements
Prevalence data for overweight/obesity based on national representative samples and objectively measured data were found for eighteen of the thirty countries (Table 1). The well-known geographical differences across Europe with the highest prevalence among adolescents from southern Europe and the British Isles were confirmed. All studies reported their data by gender, but there were no clear patterns of gender differences across the countries. Among girls, there seemed to be a decrease in the prevalence of overweight/obesity with increasing age (Table 1). The majority of the studies reported prevalence rates of overweight/obesity using the age- and gender-specific cut-offs recommended by IOTF(Reference Cole, Bellizzi and Flegal6). However, the age ranges studied and the year of the data collection varied, as did the sources of the information. Sample sizes and response rates were often not reported. The type of data collected on other sociodemographic factors also varied, and their relationship with overweight/obesity prevalence rates was often not reported.
Table 1 Prevalence of overweight (including obesity) based on objectively measured weight and height among national representative samples of adolescents in the twenty-seven European Community member states and Norway, Iceland and Switzerland: the HOPE project, WP4
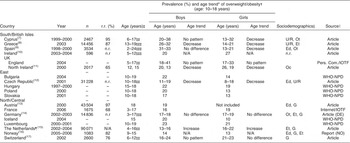
HOPE, Health-promotion through Obesity Prevention across Europe; WP, work package; r.r., response rate; n.r., not reported; N/A, not applicable; Ed, education; In, income; Oc, occupation; A, area social class; Et, ethnicity; U/R, urban/rural; G, geographical region; Ot, other; IOTF, International Obesity Task Force; WHO-NPD, WHO Nutrition Policy Database; ENNS, Etude National Nutrition Sante.
* Age trend is indicated as no pattern, increasing or decreasing prevalence by increasing age.
†The prevalences are given as range for the adolescent age group 10–18 years, IOTF age- and gender-specific definitions for overweight (including obesity)(Reference Cole, Bellizzi and Flegal6) was used for all except: Austria (adult cut-offs for BMI), Germany (national standard) and Luxembourg (2000 CDC growth charts).
‡Age range for the entire study; ‡‡Age can be disaggregated by year; ‡‡‡Age can be disaggregated by age intervals.
§Data collected on other sociodemographic factors: Ed, In, Oc, A, Et, U/R, G, Ot (i.e. composite measures of socio-economic class).
∥Source: Article, published scientific article (language if other than English); Pers. Com./IOTF, Tim Lobstein & Rachel Leach, Reanalysis of HSE 2004, personal communication, T Lobstein, May 2009; WHO-NPD(5); Internet/IOTF, ENNS 2006 – Institute de Veille Sanitaire in personal communication, T Lobstein, May 2009 and http://www.invs.sante.fr/surveillance/nutrition/enns.htm (accessed August 2009).
¶Collected from community health services, weighted for ethnicity and municipality size to match the distribution in the general population.
Availability of other data on prevalence of overweight
About half of the countries that did not have objectively measured national data had data on objectively measured height and weight from subnational or convenience samples, in addition to the self-reported HBSC data (data not shown). Prevalence data on overweight/obesity based on self-reported data from 11-, 13- and 15-year-olds were available from twenty-nine of the thirty countries (only Cyprus was missing) through the HBSC survey in 2005–2006. The majority of the countries (n 24) also participated in the HBSC survey in 2001–2002 in which such data were collected for the 13- and 15-year-olds. The new countries added in 2005–2006 were Bulgaria, Iceland, Luxembourg, Romania and Slovakia.
Trends in overweight based on objective and self-reported measurements
The WHO Europe report from 2007 and the paper by Jackson-Leach and Lobstein(Reference Branca, Nikogosian and Lobstein1, Reference Jackson-Leach and Lobstein2) reported increasing trends of overweight/obesity among adolescents in the following countries between 1958 and 2003: Greece (Crete), Denmark (Copenhagen), France (Northern), Germany (Zerbst, Hettsted, Bitterfield), Northern Ireland, Spain (various regions), Sweden (Umeå and Gothenburg), Switzerland and the UK (England and Scotland and South Northumberland).
Additional reports on the trends in the prevalence of overweight and/or obesity were found for the following countries (Table 2): Cyprus, Greece, Portugal, Spain (Cuenca), Ireland (Co Kildare), UK (West Scotland), the Czech Republic, Poland (Cracow, East rural), Finland, France, the Netherlands (national, the Hague), Norway (Bergen, Trøndelag) and Sweden (national, Stockholm, Gothenburg)(Reference O’Neill, McCarthy and Burke10, Reference Anderssen, Kolle and Steene-Johannessen16, Reference Savva, Tomaritis and Chadjigeorgiou18–Reference Sundblom, Petzold and Rasmussen37).
Table 2 Trends in prevalence of overweight/obesity or other measures of adiposity based on measured and self-reported weight and height among adolescents in the twenty-seven European Community member states and Norway, Iceland and SwitzerlandFootnote *: the HOPE project, WP4

HOPE, Health-promotion through Obesity Prevention across Europe; WP, work package; IOTF, International Obesity Task Force; BMIsds, BMI standard deviation scores; N/A, not applicable; SES, socio-economic status.
? = data not clearly reported in articles.
* References found in addition to those in the report ‘The challenge of obesity in the WHO European Region and the strategies for response’ (WHO, 2007)(Reference Branca, Nikogosian and Lobstein1) and the article by Jackson-Leach and Lobstein(Reference Jackson-Leach and Lobstein2).
† Age range for the entire study; ††Age can be disaggregated by year; †††Age can be disaggregated by age intervals.
‡ Anthropometric measures obtained/definition of overweight/obesity used: IOTF, age- and gender-specific definitions for overweight and obesity from the IOTF(Reference Cole, Bellizzi and Flegal6).
§ Study design: CSS × n, cross-sectional times number of measurement points; n, number of participants at each time point. Data collection: M, measured; Mr, measured, but collected from records; SR, self-reported; Representativity: N, national; O, subnational or other convenience sample.
∥ Overall conclusions from the articles: ↑, increase in overweight and/or obesity over time; ↓, decrease; – no change.
¶ Notes are comments on whether the trends were only pertaining to overweight or obesity, special groups, whether there were different patterns over time or by age or gender.
The three recent studies from Sweden, all based on objective measurements, show stagnation or even a decrease in obesity prevalence among girls in the samples of 10-year-olds from Stockholm and Gothenburg(Reference Sjoberg, Lissner and Albertsson-Wikland36, Reference Sundblom, Petzold and Rasmussen37) and in a sample of 16-year-olds(Reference Ekblom, Bak and Ekblom35) (Table 2). This recent indication of stabilized overweight/obesity trends was also reported from Ireland, England, France and among Dutch girls based on data collected from 1998 to 2007(Reference Barron, Comiskey and Saris22, Reference Boddy, Hackett and Stratton23, Reference Lioret, Touvier and Dubuisson30, Reference de Wilde, van Dommelen and Middelkoop31), all based on objective measurements except for the first time point in the French study. In the Dutch study(Reference de Wilde, van Dommelen and Middelkoop31), an increase was, however, found in the Turkish subsample(Reference de Wilde, van Dommelen and Middelkoop31). In Finland, an increase in overweight/obesity rates was found up until 2005 based on self-reported measurements, and this trend was similar across the multiple sociodemographic indicators used(Reference Kautiainen, Koivisto and Koivusilta29).
Considering only changes greater than ±3 % between the two latest HBSC surveys(Reference Currie, Roberts and Morgan3, Reference Currie, Gabhainn and Godeau4), changes in the prevalence of overweight/obesity among 15-year-olds were found only in about half of the countries (Table 3). The majority of these changes were small (3–4 %), and were not always seen for both genders within the same country. The only decreases in self-reported prevalence rates based on the HBSC data were seen for England and Ireland between 2001–2002 and 2005–2006.
Table 3 Countries within the twenty-seven European Community member states and Norway, Iceland and Switzerland with a reported change (≥3 %) in prevalence of overweight (including obesity) according to the IOTF criteria(Reference Cole, Bellizzi and Flegal6): based on self-reported weight and height in national representative samples of 15-year-olds in the 2001–2002 and 2005–2006 HBSC surveys(Reference Currie, Roberts and Morgan3, Reference Currie, Gabhainn and Godeau4)
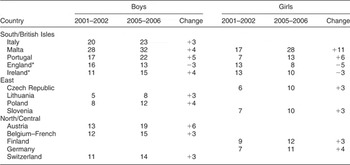
IOTF, International Obesity Task Force; HBSC, Health Behaviour in School-aged Children.
*England had 30 % or more missing data in the 2005–2006 survey, Ireland had 30 % or more missing data in both the surveys(Reference Currie, Roberts and Morgan3, Reference Currie, Gabhainn and Godeau4).
Discussion
The results presented in the present paper provide an overview of the most recent objectively measured data on overweight/obesity in the nationally representative samples of European adolescents, the availability of trend data in this age group and the ability of these data to describe the obesity epidemic across various subgroups. Earlier findings are supported in that we see large geographical differences in the prevalence of overweight/obesity among adolescents (aged 10–18 years) within the twenty-seven European Community member states and Norway, Iceland and Switzerland. The results further suggest, based on the review of recent publications, that the prevalence rates of overweight/obesity among adolescents have been increasing in countries across Europe, but might have started stabilizing according to the most recently collected data (2005–2007). However, the large heterogeneity in the quality and comparability of the available data on prevalence rates and trends of overweight/obesity among adolescents in Europe remains.
A lack of objectively measured data on national representative samples was still evident by the end of 2009. However, as most of the data presented were based on the age- and gender-specific cut-offs from IOTF(Reference Cole, Bellizzi and Flegal6), comparison between countries has become easier. In the WHO report from 2007(Reference Branca, Nikogosian and Lobstein1), there were twelve countries among the twenty-seven European Community member states, Iceland and Norway and Switzerland, which had objective measures on national representative samples of adolescents. In the present paper, such objectively measured data were found for eighteen of the thirty countries. The majority of these data were collected from 2000 to 2005, making them already 5–10 years old. Considering the rapid increase in the prevalence of overweight/obesity among adolescents in the USA over the past two to three decades(Reference Ogden, Carroll and Flegal38), and also the more recent publications on trends indicating stabilized rates in some countries/subgroups(Reference Barron, Comiskey and Saris22, Reference Boddy, Hackett and Stratton23, Reference Lioret, Touvier and Dubuisson30, Reference de Wilde, van Dommelen and Middelkoop31, Reference Ekblom, Bak and Ekblom35–Reference Sundblom, Petzold and Rasmussen37), caution should be observed regarding whether the data presented in Table 1 can be considered representative of the current situation among European adolescents, despite including only prevalence studies reporting data collected after 1995.
No clear patterns regarding gender differences in prevalence rates of objectively measured overweight/obesity were observed. This is contrary to the results from the self-reported data among 15-year-olds in the latest HBSC survey in which higher prevalence rates among boys were found in the majority of countries(Reference Currie, Gabhainn and Godeau4). The only other cross-national European survey – the Pro Children Study – used parent-reported data on weight/height among 11-year-olds from nine European countries(Reference Yngve, De Bourdeaudhuij and Wolf39). They found the same geographical differences as in the HBSC surveys, and also consistent gender differences as found in the HBSC surveys(Reference Currie, Gabhainn and Godeau4, Reference Yngve, De Bourdeaudhuij and Wolf39). However, a recent review of measured v. self-reported height and weight of adolescents in the USA found that girls and overweight youth underestimate their weight, and thus self-reported data underestimate the real prevalence of overweight and should only be used when measured data are not obtainable(Reference Sherry, Jefferds and Grummer-Strawn40). In addition, large variations in the response rates in these self- and/or parent-reported survey results(Reference Currie, Roberts and Morgan3, Reference Currie, Gabhainn and Godeau4, Reference Yngve, De Bourdeaudhuij and Wolf39) may further have biased the results. In studies employing objective measures (Table 1), the available response rates appeared high, but the total number of participants varied largely and might have weakened the precision of the prevalence estimates.
The results of the European HELENA study (promoting Healthy European Lifestyle through Exercise and Nutrition in Adolescence), with its thorough measurement of body composition of ten representative urban samples of 13–16-year-olds across Europe, will soon become available(Reference de Henauw, Gottrand and de Bourdeaudhuij41). The data from the HELENA study will further enrich our insight into prevalence rates across Europe and by sociodemographic groups. Furthermore, the ongoing WHO European Childhood Obesity Surveillance Initiative among primary-school children (aged 6–10 years) in fifteen countries across Europe should provide good-quality data for this age group, as well as useful experiences in order to design a similar surveillance system among adolescents(42). In the Norwegian part of the present survey, measurements were obtained for 89 % of the 3952 invited children(Reference Hovengen, Meisfjord and Biehl43). Measures were taken by trained school nurses using standardized protocols for calibration of measurement tools and to measure and report weight, height and waist circumference(Reference Hovengen, Meisfjord and Biehl43). The experience so far clearly indicates that this is a highly feasible method for collecting data, and it shows that it is also possible to include other measures of adiposity (i.e. waist circumference) within such a surveillance system.
Other issues not properly addressed in the available literature were variation in prevalence by age through adolescence and by sociodemographic subgroups. It seemed that most studies measured several age groups (Table 1). Thus, data are available to address whether there are differences in prevalence by age, but repeated cross-sectional surveys in the same age groups are needed to address whether these are true age differences or cohort differences because of variation in year of data collection in the different age groups. Data on other sociodemographic differences, such as indicators of socio-economic status (SES) and ethnicity, were only infrequently collected and presented. Finally, many of the identified reports were not published in scientific journals or in English, which makes it difficult to systematically review the results and poses serious questions about the quality of the data from studies since they have not undergone peer review. National public health institutes are likely to be in charge of national surveillance of available data on overweight/obesity in their populations, and they should be able to add to their routine by submitting reports to a cross-European surveillance system. Several of the studies on trends were already making use of various register data(Reference O’Neill, McCarthy and Burke10, Reference van den Hurk, van Dommelen and van Buuren15, Reference Cardoso and Padez20, Reference de Wilde, van Dommelen and Middelkoop31, Reference Sjoberg, Lissner and Albertsson-Wikland36, Reference Sundblom, Petzold and Rasmussen37).
The reports on trends in overweight/obesity among adolescents in Europe confirmed the finding that these data are largely subnational, based on two time points only, and still one-third reported on trends before the year 2000. On the positive side, these studies were mainly based on objectively measured data. Furthermore, recently published studies do, to a larger extent than previous ones, analyse by sociodemographic subgroups such as SES(Reference Kautiainen, Koivisto and Koivusilta29, Reference Lioret, Touvier and Dubuisson30) and ethnicity(Reference de Wilde, van Dommelen and Middelkoop31), and one also included a measure of thinness(Reference Martinez-Vizcaino, Sanchez Lopez and Moya Martinez21). A scarcity of data on older adolescents and from Eastern European countries is noted as well. Data from these groups would be of particular interest as dietary habits and physical activity tend to deteriorate during adolescence, and the social and economic transitions in Eastern Europe are likely to influence these behaviours. The methodological weaknesses of the HBSC data (self-reported and variable response rates) make it impossible to draw any firm conclusion regarding the trends in overweight and obesity rates among European adolescents. In particular, the quality of data from England and Ireland, which showed a decreasing trend, might be biased because of larger proportions of missing data on height and weight in the more recent surveys(Reference Currie, Roberts and Morgan3, Reference Currie, Gabhainn and Godeau4). However, regional trend data from Liverpool and Co Kildare(Reference Barron, Comiskey and Saris22, Reference Boddy, Hackett and Stratton23) do support a possible levelling off and stabilization of overweight/obesity rates. The need for routinely collected, objectively measured data in national representative samples across Europe is thus strongly recognized.
In conclusion, current data indicate that there is geographical variation and that there has been an increase in the prevalence of overweight over time among adolescents in Europe, but that this increase might now be levelling off and stabilizing for some countries and some sociodemographic groups. Objectively measured data on national representative samples of adolescents appear scattered, and there is a great heterogeneity with respect to the quality and comparability of available data. Data by sociodemographic subgroups, and in particular by SES, are scarce and should be included in future analyses, given the indication that the stabilization might not be equal across sociodemographic groups. A cross-national monitoring system of overweight/obesity in adolescence and with good data on SES and ethnicity may provide the best data, but in the mean time the increased use of the IOTF criteria for overweight/obesity in publications should be continued.
Acknowledgements
Sources of funding: The present paper has been facilitated by the EU-funded HOPE project: Health-promotion through Obesity Prevention across Europe (the Commission of the European Communities, SP5A-CT-2006-044128). The study does not necessarily reflect the Commission’s views and in no way anticipates the Commission’s future policy in this area. Conflict of interest declaration: None of the authors had conflict of interest. Authorship responsibilities: N.L., M.W. and K.-I.K. planned the study. M.W., L.L.N. and H.B.B. conducted the searches, collected the data and summarized the findings. N.L. drafted the first manuscript and completed the final one based on input from all authors.



