



The consumption of ultra-processed foods (UPF) during the first 1000 d of life represents a possible collaborator for the increase in the prevalence of the double burden of malnutrition in childhood, observed in middle- and low-income countries, which is characterised by the coexistence of malnutrition, micronutrient deficiencies, overweight, obesity and chronic non-communicable diseases related to diet(Reference Popkin, Corvalan and Grummer-Strawn1). The rapid increase in the prevalence of overweight and obesity in these countries, in line with the decline in the prevalence of malnutrition, is related to the profound changes in the eating patterns of the world population, especially in vulnerable populations, where early weaning from breast-feeding is observed(Reference Alleo, Souza and Szarfarc2) as well as the replacement of fresh or minimally processed foods and culinary preparations with products ready for consumption, classified as UPF(Reference Popkin, Corvalan and Grummer-Strawn1). This increase in the consumption of UPF was due to the changes that occurred in the last decades in the control of the entire food chain by agribusiness, food manufacturers and retailers, with substantial advertising appeal, making the UPF more competitive when compared with foods that are naturally ready and culinary preparations based on fresh foods, as they are more convenient for consumption, hyper-palatable and of low cost(Reference Monteiro, Cannon and Levy3). It is evident in the literature that poverty is one of the main determinants of inadequate food(Reference Popkin, Corvalan and Grummer-Strawn1,Reference Alleo, Souza and Szarfarc2) .
To achieve adequate child growth and development, it is recommended that the child receives exclusive breast-feeding for the first 6 months and complemented breast-feeding until the age of 2 years, combined with the timely introduction of adequate and healthy complementary feeding(4,Reference Batalha, França and Conceição5) . For this reason, the first 2 years of life represent the best window of opportunity for children to establish healthy eating habits and can be a protective factor for the development of chronic non-communicable diseases, including overweight and obesity throughout their lives(4).
The benefits of continued breast-feeding are well established, and the increase in this practice can play an essential role in improving the child’s nutrition, education and health. The rise in the prevalence of breast-feeding and its continuity is associated with the prevention of morbidity and mortality, diarrhoea, infections, dental malocclusion, increased intelligence in childhood and reduced occurrence of overweight and diabetes in adulthood(Reference Warkentin, Mais and Latorre6,Reference Bortolini, Giugliani and Gubert7) .
In this context, the Bolsa Família Program (PBF) is configured as a strategy implemented by the Brazilian government to promote the guarantee of access to fundamental social rights to families in poverty and extreme poverty, through cash transfer with conditionalities in the areas of health, education and social assistance, assisting inequitable access to health services, and the promotion and guarantee of the Human Right to Adequate Food(8). Rasella et al.(Reference Rasella, Aquino and Santos9) showed that the Brazilian conditional cash transfer programme contributed to the general decrease in infant mortality among children under the age of 5 years, mainly in cases of deaths related to poverty, attributable to malnutrition and diarrhoea. In addition, families benefiting from the PBF who had children under the age of 5 years showed a significant increase in the amount and variety of foods consumed(Reference Martins and Monteiro10).
Thus, the current work aimed to evaluate the association between the consumption of UPF and the practice of breast-feeding in children under the age of 2 years who are beneficiaries of the Brazilian income transfer programme, PBF.
Methods
Design
A cross-sectional study. The current paper is part of a larger project entitled: Evaluation of the management and operationalization of the National Program for Iron and Vitamin A Supplementation and their relationship with the nutritional status of children aged 6 to 24 months in counties of Alagoas state, which was performed following the guidelines set out in the Declaration of Helsinki. The local institutional review board (CAAE 80416617.0.0000.5013) approved the study, and the legal guardian of each child gave written informed consent.
Setting and sample selection
Children aged 6−24 months, assisted by the PBF and residents of six counties in the state of Alagoas, located in the Northeast Region of Brazil. The six counties cover all physiographic regions of the state, namely Pilar (Metropolitan Region), Murici (Zona da Mata), Teotônio Vilela (South Region), São Luís do Quitunde (Northern Region), Pão de Açúcar (Sertão) and Batalha (Agreste), and were included in the study because they belong to the Early Childhood Program of the State of Alagoas, which had criteria to have 100% coverage of the Brazilian primary care, Family Health Strategy and at least one team from Family Health Support Centers. The State Early Childhood Program aims to contribute to improving the quality of life of pregnant women, nursing mothers and children through intersectoral actions developed by the areas of health, nutrition, education and social assistance.
A convenience sampling approach was used. The identification of eligible children was performed through the health monitoring map of the PBF beneficiaries by each municipality, which had their guardians invited to attend the Basic Health Units for participation in the study. This invitation came through community health workers and wide dissemination in local media such as community radios or during consultations with health professionals at the Basic Health Units. The research in the municipalities had the consent and partnership of the Municipal and State Health Departments.
Children whose parents reported a diagnosis of genetic and autoimmune haematological diseases (sickle cell disease, haemolytic, sideroblastic and aplastic anaemia, Fanconi anaemia and thalassaemia) or had previously diagnosed of other nutritional anaemias except for iron deficiency anaemia (IDA) (megaloblastic and pernicious anaemia) and those whose mothers had mental problems were excluded from the study. In families with more than one child within the inclusion criteria, only the oldest was selected to participate. In the case of twin brothers, the included child was randomly selected.
Data collection
Data were collected between May and December 2018 by a trained staff composed of four nutritionists and ten technical assistants. The children’s legal guardians were interviewed using a structured form with socio-demographic, health and environmental issues. Information on family income, sanitation, housing location and the number of residents per household was obtained from secondary data through the CadÚnico Consultation, Selection and Information Extraction database, using the Social Registration Number (SRN) of each individual, provided by the state government.
Dependent variable
The dependent variable was the consumption of UPF, identified through an adaptation of the structured 24-h dietary recall proposed by Oliveira et al.(Reference Oliveira, Castro and Silva11) based on the WHO(12) document on indicators of early childhood eating habits with pre-established questions modified to the eating habits of the region. To identify the consumption of UPF, the food classification proposed by Monteiro et al.(Reference Monteiro, Cannon and Levy3) was used.
Independent variables
The following characteristics of the household were investigated as covariates: per capita household income, the number of residents per household, housing location (urban/rural), source of drinking water (adequate – mineral or public/inadequate – well water, river or cistern)(13), sanitation (adequate – general sewage system or septic tank/inadequate – rudimentary cesspit or open sewer)(13), the situation of food insecurity (FI), the characteristics of the children’s legal guardians: age and education and the children’s characteristics: sex, age, BMI-for-age and being institutionalised in daycare centres.
For the assessment of breast-feeding practice, an adaptation of the 24-h dietary recall, also proposed by Oliveira et al.(Reference Oliveira, Castro and Silva11), was used, based on the WHO(12) document on indicators of feeding practices in early childhood. Among the fifteen indicators proposed by the WHO, eleven were evaluated, which suited the age group of the study and, among them, it was considered whether the children were breastfed at some point in life and on the continuity of breast-feeding until the first 2 years of age.
Anthropometry
The nutritional diagnosis was determined by using the anthropometric index BMI-for-age, according to the classification proposed by the WHO(14). All children underwent an anthropometric assessment to identify their nutritional status. For this, the children were weighed on a paediatric electronic scale (Welmy Indústria e Comércio Ltda) with a capacity of 15 kg and precision of 5 g. The length was measured using a portable infantometer (Alturexata Ltda) with a capacity of 110 cm and resolution in ml. Anthro software, version 3.2.2, was used to assess anthropometric indices, which uses WHO reference standards.
Food insecurity
FI was assessed through the Brazilian Food Insecurity Scale, with fourteen questions (yes or no) about the food access situation experienced at home in the last 90 d before the interview. Its analysis is based on the sum of the affirmative answers, being classified as food safety and mild, moderate and severe FI(Reference Pérez-Escamilla, Segall-Corrêa and Maranha15).
Statistical analysis
All data were entered in double entry, and the data analysis was conducted with the aid of the R statistical package (R Foundation for Statistical Computing) using the R-Commander package. The characteristics of the sample were described employing absolute (n) and relative (%) frequencies.
The analysis of factors associated with the outcome (consumption of UPF) was performed using Poisson regression with a robust estimate of variances, estimating the gross and adjusted prevalence ratios (PR) according to the theoretical model proposed by Batalha et al.(Reference Batalha, França and Conceição16) and adapted to the practice of breast-feeding. The first level included the socio-economic characteristics of those responsible for the child. The second level is related to the environment in which the child is inserted. The third level included the family’s access to food. The fourth included the individual characteristics of the child. The fifth and last level consisted of breast-feeding (Fig. 1).

Fig. 1 Hierarchical model proposed to assess the factors associated with the consumption of ultra-processed foods of children aged 6–24 months, beneficiaries of the Bolsa Família Program and their families in the State of Alagoas, Brazil, 2019
A bivariable analysis was performed simultaneously between the independent variables and the outcome within each hierarchical level, and only variables with an unadjusted P < 0·20 were maintained in the multivariable model. For each hierarchical level, variables within the same level were introduced simultaneously with variables from the previous significant levels (P < 0·20). Only the variables of the fifth level were included one at a time in the model together with the significant variables of the other previous levels, as they are dependent. The variables at the first level remained as adjustment factors for the different hierarchical levels even when in the absence of statistical significance.
Results
The study evaluated 1604 children aged 6−24 months. Those responsible for the children had a mean age of 25·69 (95 % CI 25·30, 26·07) years, and of those, 647 (41·5 %) had no education or had <9 years of schooling. Of the assessed families, 1490 (92·9 %) had a family income per capita below R$ 85·00 and 15·4 % lived in severe FI (Table 1).
Table 1 Socio-economic, demographic, environmental and health characteristics of children aged 6–24 months, assisted by Bolsa Família Program and their families in the State of Alagoas, Brazil, 2019

FI, food insecurity.
* Values are presented as total number (n) and frequency (%) for categorical variables.
† Family per capita income values do not include the amount received by the Bolsa Família Program.
‡ Secondary data obtained through the CadÚnico Consultation, Selection and Information Extraction database bank, provided by the state government.
§ Amount referring to half the minimum wage in Reais in the year of 2018 (minimum wage in 2018 = R$ 954·00); In December 2018, $US 1·00 was approximately R$ 3·88.
‖ Households were classified as ‘food secure’ grouping, those in food security and mild FI, and as ‘food insecure’ grouping, those with moderate and severe FI according to the Brazilian Food Insecurity Scale.
¶ In the BMI-for-age index, eighteen children with wasting nutritional status were excluded and nine children did not present these data.
** Foods were classified according to the NOVA classification proposed by Monteiro et al.(Reference Monteiro, Cannon and Levy3).
†† Children who had access to breast-feeding at some point in life.
‡‡ Indicator of continuity of breast-feeding at 1 year of age; sample with children aged 12–15 months who were breastfeed the day before.
§§ Indicator of continuity of breast-feeding at 2 years of age; sample with children aged 20–24 months who were breastfeed the day before.
The children had a mean age of 14·86 (95 % CI 14·28, 14·79) months, of those 599 (38·1 %) were at risk of overweight and/or overweight and only 97 (6 %) attended a daycare centre. Of the total sample, 1489 (92·8 %) of the evaluated children were breastfed at some point in life, with 223 (60·3 %) breast-feeding up to 1 year of age and 161 (47·6 %) until 2 years old. UPF consumption was observed in 1454 (90·6 %), and 1566 (97·6 %) had consumed fresh and minimally processed foods in the last 24 h. The UPF most consumed by children were biscuits, chocolate milk and baby food with the prevalence of consumption of 74·8, 66·8 and 24·9%, respectively (Fig. 2).
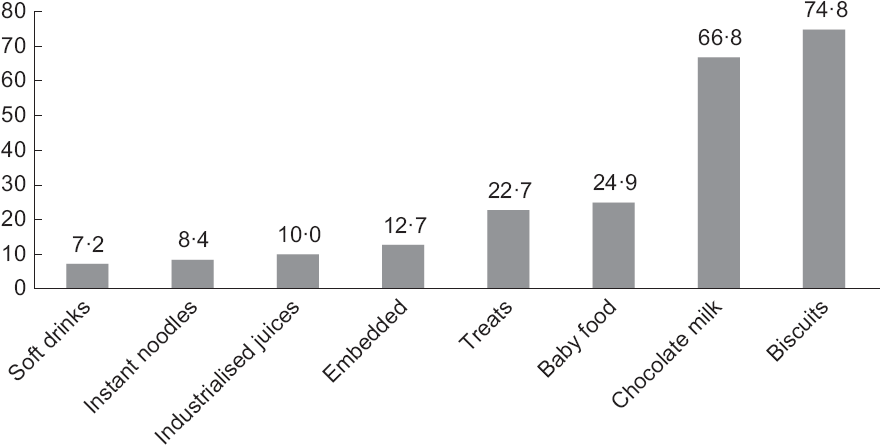
Fig. 2 Percentage of consumption of ultra-processed foods by children aged 6–24 months, beneficiaries of the Bolsa Família Program and their families in the State of Alagoas, Brazil, 2019
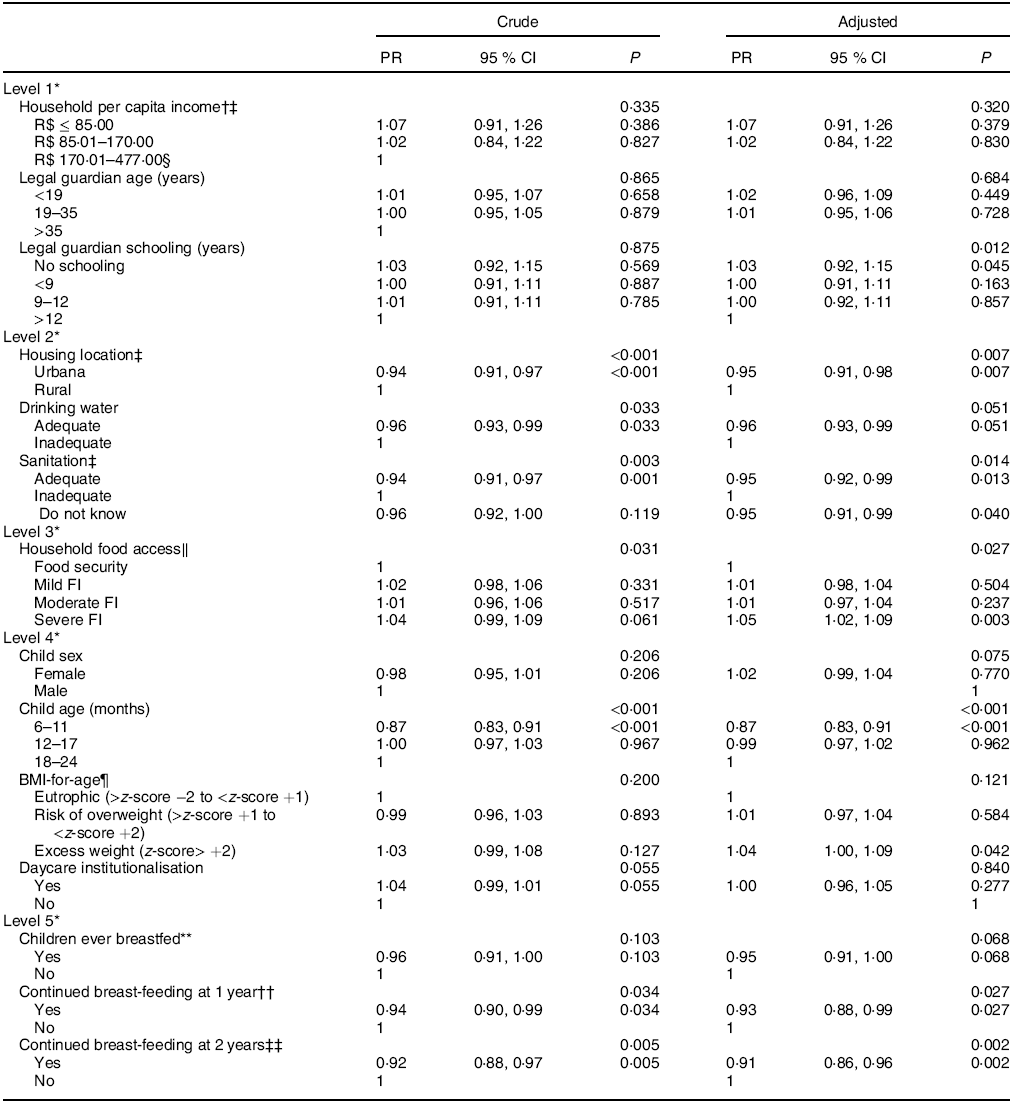
In the adjusted multivariable analysis, for each hierarchical level, the variables within the same level were introduced simultaneously with the significant variables of the previous levels (P < 0·20). The following factors were associated with a lower consumption of UPF: child aged 6–11 months (PR 0·87, 95 % CI 0·83, 0·91), living in the urban area (PR 0·95, 95 % CI 0·91, 0·98), presenting an appropriate sanitary drain (RP 0·95, 95 % CI 0·92, 0·99), remaining on breast-feeding until 2 years of life (PR 0·91, 95 % CI 0·86, 0·96) and remaining on breast-feeding until the first year of life (PR 0·93, 95 % CI 0·88, 0·99). On the other hand, families which the guardian showed low education (PR 1·03, 95 % CI 0·92, 1·15), the child was overweight (PR 1·04, 95 % CI 1·00, 1·09) and families were in severe FI (PR 1·05, 95 % CI 1·02, 1·09) were associated with the higher consumption of UPF (Table 2).
Table 2 Association by gross and adjusted hierarchical Poisson regression between the consumption of ultra-processed foods and the socio-economic, demographic, environmental and health characteristics of children aged 6−24 months, beneficiaries of the Bolsa Família Program and their families in the State of Alagoas, Brazil, 2019
FI, food insecurity; PR, prevalence ratio.
* At level 1, the adjusted analysis was performed with the simultaneous insertion of all variables at the same level; at level 2, the adjusted analysis was performed with the simultaneous insertion of all variables from levels 1 and 2. At level 3, the adjusted analysis was performed with the simultaneous insertion of all variables from levels 1 and 3, in addition to the variable with P < 0·20 in the crude analysis of level 2 (drinking water); at level 4, the adjusted analysis was performed with the simultaneous insertion of all variables from levels 1 and 4, in addition to the variable with P < 0·20 in the crude analysis of levels 2 and 3 (drinking water; FI in households). At level 5, the variables at this level were included one at a time in the model together with all the variables at level 1 and the variables with P < 0·20 from the other previous levels (location of home, drinking water, drainage, situation of FI in the households, sex and age of the child, BMI-for-age index and institutionalisation in daycare).
† Family per capita income values do not include the amount received by the Bolsa Família Program.
‡ Secondary data obtained through the CadÚnico Consultation, Selection and Information Extraction database bank, provided by the state government.
§ Amount referring to half the minimum wage in Reais in the year of 2018 (minimum wage in 2018 R$ 954·00); In December 2018, $US 1·00 was approximately R$ 3·88.
‖ Households were classified as food security those in food security and mild FI, and as FI those with moderate and severe FI according to the Brazilian Food Insecurity Scale.
¶ In the BMI-for-age index, eighteen children with wasting nutritional status were excluded, and nine children did not present these data.
** Children who had access to breast-feeding at some point in life (n 1489).
†† Indicator of continuity of breast-feeding at 1 year of age; sample with children aged 12–15 months who suckled the day before (n 223).
‡‡ Indicator of continuity of breast-feeding at 2 years of age; sample with children aged 20–24 months who suckled the day before (n 161).
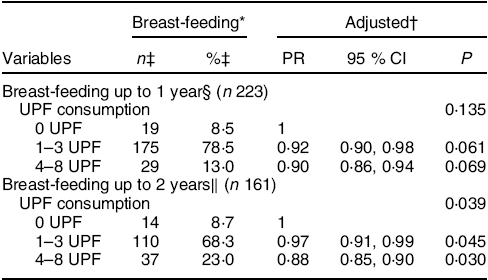
It was possible to observe that the practice of continuous breast-feeding until the age of 2 years (PR 0·91, 95 % CI 0·86, 0·96) and in the first year of life (PR 0·93, 95 % CI 0·88, 0·99) was associated with the lower consumption of UPF (Table 2). When stratified by the amount of UPF consumed, the continuation of breast-feeding for up to 1 year was not significant (Table 3).
Table 3 Hierarchical Poisson regression association stratified by the continuation of breast-feeding and the consumption of ultra-processed foods (UPF) from children aged 6−24 months, beneficiaries of the Bolsa Família Program and their families in the State of Alagoas, Brazil, 2019
PR, prevalence ratio.
* WHO subgroup analysis of early childhood eating habits indicators, 2010.
† Association by hierarchical Poisson regression adjusted for the variables: family income per capita, age of the person in charge, education of the person in charge, location of housing, drainage and age of the child.
‡ Values are presented as total number and frequency for categorical variables.
§ Indicator of continuity of breast-feeding at 1 year of age; sample with children aged 12–15 months who suckled the day before.
‖ Indicator of breast-feeding continuity at 2 years of age; sample with children aged 20–24 months who suckled the day before.
Discussion
The current study shows a high prevalence of consumption of UPF (90·6 %) by children aged 6−24 months who are beneficiaries of PBF in the State of Alagoas, Brazil. On a positive note, the continuation of breast-feeding for at least 2 years was associated with a lower consumption of UPF. The guidelines established in Brazil for the promotion of healthy and adequate food and the guarantee of the Human Right to Adequate Food to children point to the need for daily and priority consumption of fresh or minimally processed food, as well as the practice of breast-feeding and its continuation for at least 2 years. It also points to the need to avoid the consumption of UPF, which are deficient in nutrients, considering the specificity and relevance of the first years of life in the development of human beings(17). However, no significant associations were found between breast-feeding at some point in life and consumption of UPF, which was only associated with the continuation of breast-feeding until the first and second years of life.
In Brazil, one in every three children continues to receive breast milk until the second year of life(17). However, a national survey has shown that children under 2 years consume high amounts of UPF. Showing that the consumption of sugary and carbonated drinks was frequent in one-third of the children accessed (32·3 %) and crackers, biscuits or cake was consumed by more than half of this population (60·8%)(18), higher consumption percentages of these foods were found in our study. The substitution of breast milk for another type of milk is a factor associated with the high consumption of UPF in children aged 6−35 months since, in general, the milk is consumed with added flour and sugar(17).
In the current study, most of the evaluated children had access to breast-feeding (92·8 %) at some point in life. However, only 47·6% continued to be breastfed until the second year of age. Nevertheless, a previous study observed that mothers benefiting from the PBF are more informed and have a more important commitment to breast-feeding and monitoring the child’s health due to the conditions present in the cash transfer programme(19,20) .
It was possible to identify the importance of continuing breast-feeding until 2 years of life, since the children in the study aged between 12 and 15 months had a lower consumption of UPF. This is possibly because the fact that families that follow the recommendation to continue breast-feeding for up to 2 years or more are the same ones that are more likely to encourage the consumption of healthier foods and to limit the consumption of UPF, since this practice is encouraged and made available by the family context(Reference Perrine, Galuska and Thompson21). The same was possible to be noticed in other studies, reinforcing that the longer duration of breast-feeding is consistently related to the higher consumption of fresh or minimally processed foods, and the early interruption of breast-feeding is associated with the high consumption of UPF(Reference Bortolini, Giugliani and Gubert7,Reference Bell, Golley and Daniels22,Reference Lauzon-Guillain, Jones and Oliveira23) . Park et al.(Reference Park, Pan and Sherry24) showed that children at 6 years of age who were breastfed until the age of 6 months or more had a significantly lower proportion of consumption of sweetened drinks compared with those who did not breastfeed. The authors also identified a greater chance for children to consume sugary drinks more than once a week when these drinks were introduced in the second half of life.
Rinaldi and Conde(Reference Rinaldi and Conde25), analysing secondary data from Brazilian national researches, demonstrated the existence of inequality in the pattern of food consumption among Brazilian children of higher and lower socio-economic status before the age of 2 years. There was a greater consumption of fresh foods, such as fruits, vegetables, beans, meats and tubers by the wealthiest children, while the poorest children had a higher consumption of breast milk and sugary drinks, these being more exposed to malnutrition, due to the poor quality of food. Given the observed, it is necessary to strengthen public policies for the promotion, protection and support of breast-feeding and healthy complementary feeding, as well as the elimination of the promotion of breast milk substitutes (infant formula or baby food), mainly for families in poverty and extreme poverty, as breast-feeding is an accessible alternative for the prevention of diseases at all stages of life and helps in the full development of children(Reference Rollins, Bhandari and Hajeebhoy26,Reference Hawkes, Ruel and Salm27) .
The association between the guardian’s low education level and UPF consumption in children under the age of 2 years found in our study indicates that the higher educational level of the guardian is related to greater access to information. This knowledge can potentially facilitate access to healthy and appropriate foods, such as vegetables and meat, as well as the proper practice of breast-feeding and its continuity(19,20,Reference Relvas, Buccini and Venancio28) . In this context, Batalha et al.(Reference Batalha, França and Conceição16) stated that the higher prevalence of UPF consumption among children under the age of 1 year was associated with those with less education. However, in our study, it was not possible to find a statistical association between the consumption of UPF and income because of the fact that the sample studied was made up of PBF beneficiaries, and 92·5% were in the extreme poverty range (with family income per capita below R$ 85·00). Thus, this homogeneity leads to low variability regarding the income in the group, making it difficult for (or distorting) the detection of associations with this factor and other collinear factors.
In this perspective, our findings demonstrated that the poverty of this population is closely related to FI, which influences the ability to guarantee the basic conditions for healthy and adequate food for children, making it evident that the PBF was not sufficient to ensure a worthy condition of access to a healthy and adequate diet, causing damage to children’s nutritional status. Although Martins and Monteiro(Reference Martins and Monteiro29) observed that the families benefiting from the PBF had a 7·3% higher expenditure on fresh/minimally processed foods and a 10·4% higher expenditure on culinary ingredients when compared with those that did not receive the benefit, our findings show that UPF consumption during the complementary feeding phase was associated with being overweight. In contrast, Lignani et al.(Reference Lignani, Sichieri and Burlandy30) observed that the increased purchasing power of families did not reflect a benefit in the quality of the diet eaten, as there was an increase in the consumption of processed foods with high energy density, possibly associated with the lower cost of these foods.
A high prevalence of FI (66·6 %) was found in the population studied, higher than the national average (22 %)(18), and its association with the higher consumption of UPF may be a consequence of the worsening economic crisis that is effecting Brazil since 2014 and led to the impoverishment of the population, when more than 4·504 million Brazilians started to live in poverty and, consequently, in FI, hindering access to nutritionally adequate food(31,Reference Claro, Maia and Costa32) .
Families or guardians have an important role in determining the foods that children under 5 years of age consume; however, the economic factor does not allow access to adequate quality food in large numbers of Brazilian families living in households with FI moderate or severe(33). National data from the 2017–2018 Household Budget Survey revealed that low-income families committed a greater part of their budget to food expenses (22·6 %) compared with those with higher income (7·6 %)(34). This fact can certainly be made worse when referring to families in poverty and extreme poverty, as the study participants, highlighting the socio-economic disparities in access to food(31). Consequently, some authors explain that for families living in situations of poverty and extreme poverty to achieve the recommendations of a healthy diet would impact an increase of 39 and 58 % in income, that is, these households would be unable to buy healthy food facilitating the excessive purchase of cheaper and not recommended foods (UPF)(Reference Borges, Claro and Martins35).
The current work has some limitations. First, the instrument used for food consumption data collection (adapted 24-h dietary recall), with an emphasis on UPF, has potential response bias and may represent an atypical food day, not representing long-term dietary patterns. However, we follow the recommended research methodology with the use of 24-h dietary recall for the assessment of WHO indicators of feeding practices in early childhood, and this method is widely used and considered appropriate in food consumption surveys, when the objective is to describe infant feeding practices in populations(12). Second, this same instrument did not allow evaluating the details of the use of culinary ingredients present in the ‘NOVA’ classification. Third, it was not possible to collect breast-feeding history data due to memory bias and inaccuracy of responses, and so only the current breast-feeding situation was assessed. And, finally, the non-probabilistic recruitment for convenience of the sample may have caused a selection bias because those who have greater access to health services are more likely to participate in the study. Despite the observed limitations, the current study provides important information about the high consumption of UPF associated with the practice of breast-feeding in children under the age of 2 years who are beneficiaries of the PBF.
Therefore, our findings show how the promotion, protection and support of breast-feeding and healthy complementary feeding are essential for the achievement of many of the Sustainable Development Goals by 2030(36). Breast-feeding is not explicitly mentioned in the Sustainable Development Goals, but our study shows that improvements in breast-feeding practice would help achieve the goals for children’s health, food security and nutrition. Therefore, the high prevalence of children consuming UPF and early interrupting the practice of breast-feeding found in the current study makes the authors reinforce the need for the implementation of structuring public policies aimed at decent food in quality and quantity and continued breast-feeding, in conjunction with social strategies to combat poverty and FI, in addition to actions of food and nutrition education aimed at reducing the consumption of UPF, considering that the first 2 years of life are important for the encouragement and development of healthy eating habits, leading a healthy and productive adult life.
Acknowledgements
Acknowledgements: The research in the municipalities had the consent and partnership of the Municipal and State Health Departments. Financial support: The current work is part of a larger project entitled: Evaluation of the management and operationalization of the National Program for Iron and Vitamin A Supplementation and their relationship with the nutritional status of children aged 6 to 24 months in municipalities of Alagoas state, carried out with funds from Conselho Nacional de Desenvolvimento Científico e Tecnológico (process no. 408445/2017-3). The funder had no role in the design, analysis or writing of the current article. Conflict of interest: There are no conflicts of interest. Authorship: G.M.M. participated in designing the study, acquisition of data, data entry, analysis and interpretation of the data and drafting the article. M.M.M., M.G.M.F., T.M.M.T.F. and N.B.B. took part in the acquisition of data, data entry, analysis and interpretation and writing. A.P.G.C. took part in the project’s conception, obtained the respective financial support, coordinated all implementation steps and realised the final review of the article. All authors approved the final version to be submitted. Ethics of human subject participation: The current study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving study participants were approved by the Ethics Committee in Research of Alagoas Federal University (process no. 80416617.0.0000.5013). The mothers or legal guardians of all participating children aged 6–24 months gave written informed consent.





