This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/eurpsy/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
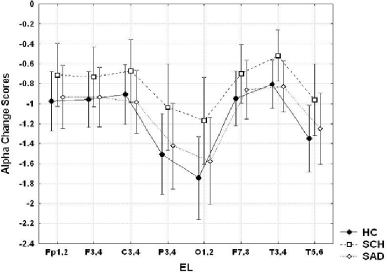
Alpha activity in the EEG is dominant in normal individuals during eyes-closed resting condition and is suppressed by visual stimulation (alpha-blockade). The differences in alpha band activity between the eyes-closed and eyes-open resting conditions are used as a measure of resting state arousal. It's known that alpha-blockade in patients with schizophrenia is less pronounced than in healthy individuals; no studies exist in schizoaffective disorder. The objective of this study was to evaluate the contribution of EEG alpha reactivity on opening the eyes, to the neurophysiology of schizophrenia and schizoaffective disorder. In total 64 patients with first episode of schizophrenia(SCH; n=32) and schizoaffective disorder (SAD; n=32) and 40 controls were enrolled into the study. All participants were assessed with EEG and alpha reactivity was computed using the logarithms of spectral power of alpha band in two experimental conditions (with eyes-closed and eyes-open). In eyes-open condition there was a significant reduction in absolute alpha power in all electrodes in schizoaffective patients and controls, indicating a similar increase in the arousal level in these groups (Fig.1). However, the alpha reactivity index was greater, corresponding to less reactivity, in the all regions in patients with schizophrenia (P < .05) as compared to controls. Our findings suggest distinct alterations in arousal mechanisms in patients with schizophrenia and schizoaffective disorder.