


 Open access
Open access
Crossref Citations
This article has been cited by the following publications. This list is generated based on data provided by Crossref.
Fofanah, Bobson Derrick
Kamara, Ibrahim Franklyn
Kallon, Christiana
Kamara, Rugiatu
Nuwagira, Innocent
Musoke, Robert
Tengbe, Sia Morenike
Lakoh, Sulaiman
Korjie, Musa Mustapha
Sheriff, Bockarie
Maruta, Anna
Katawera, Victoria
Kamara, Abibatu
Hailu, Binyam Getachew
Kanu, Joseph Sam
Makamure, Tendai
Njuguna, Charles
and
Kabego, Landry
2024.
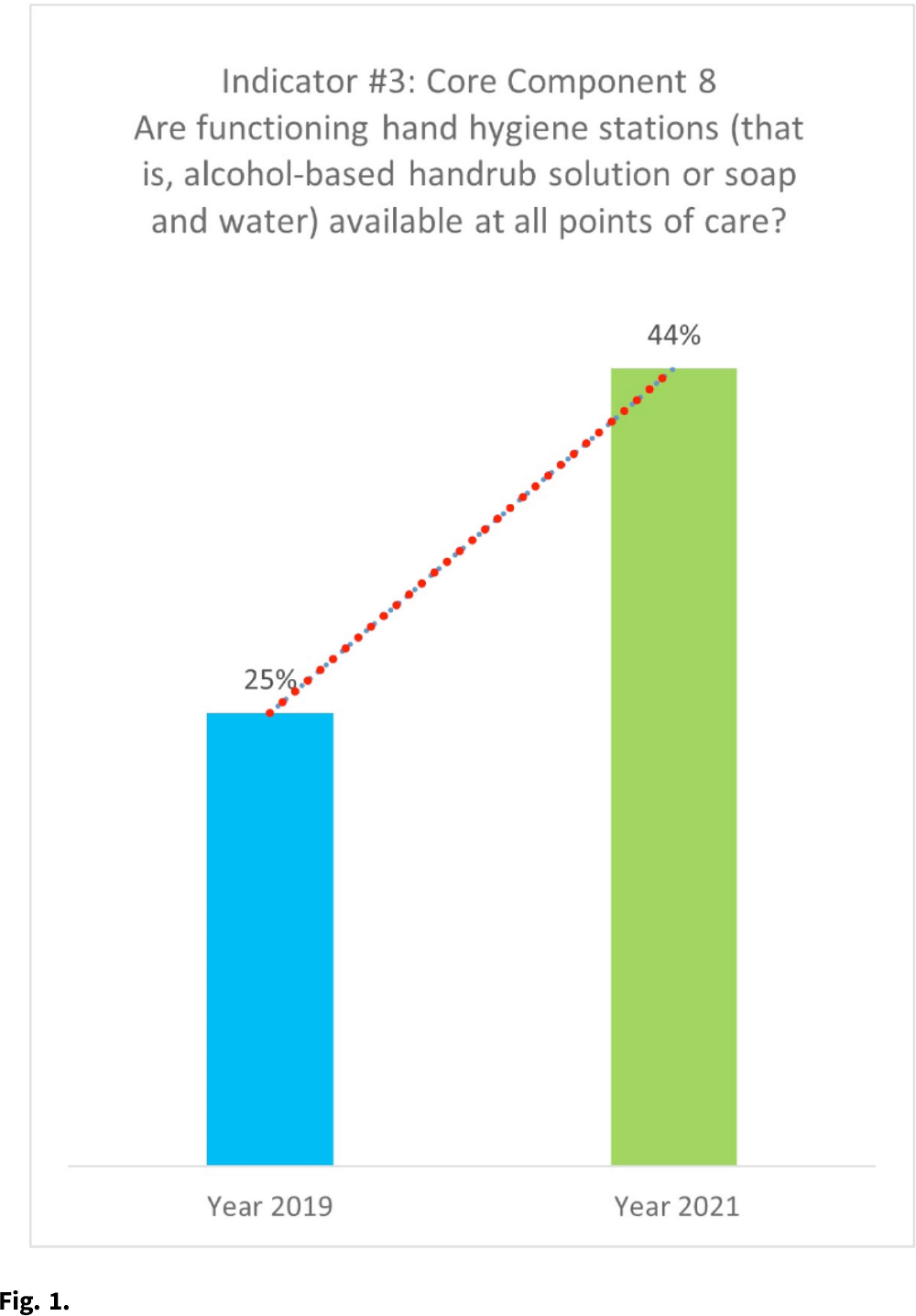
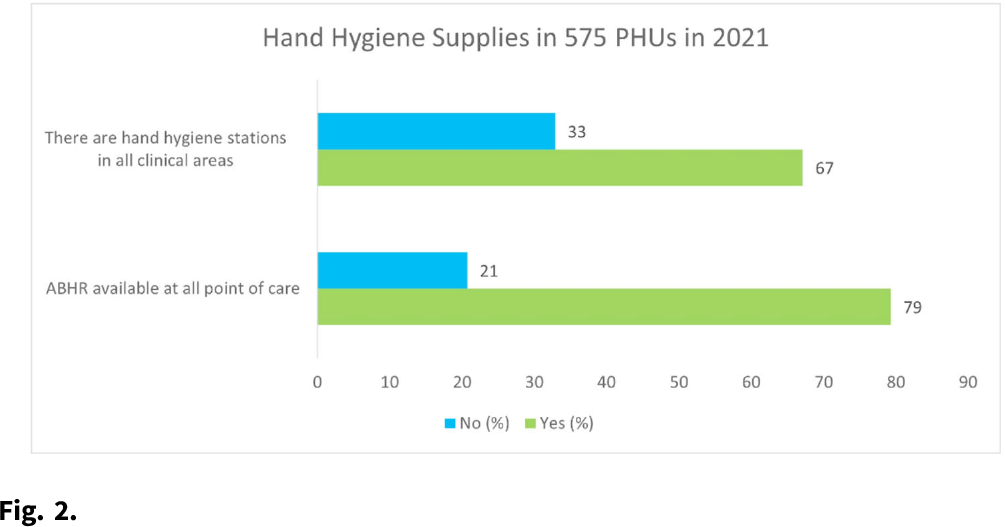
Evaluating the tolerability and acceptability of a locally produced alcohol-based handrub and hand hygiene behaviour among health workers in Sierra Leone: a longitudinal hospital-based intervention study.
BMC Health Services Research,
Vol. 24,
Issue. 1,