

Preparation for entering and succeeding in private practice is one vital area that graduate programs typically cannot give adequate attention to due to the long list of “academic” courses and clinical training experiences that must be offered to ensure the development of necessary clinical competence. And it seems that there is never enough time to learn all we need to know to be fully prepared for our professional roles after graduation day. But the preparation specific to having a career as a private practitioner is an important aspect of career growth and planning. This chapter will provide guidance on how to prepare for a career in private practice.
Years ago, psychologists would receive their degree, become licensed, have business cards printed, take out a yellow pages ad, rent an office, and begin treating patients. Unfortunately, the practice landscape has become much more crowded, competitive, and complicated over the years. There are numerous mental health professionals with various amounts and types of training who are all competing for many of the same patients. While clinical proficiency is mandatory, it is not nearly enough to ensure success in private practice. Running a private practice is a business enterprise that requires advanced planning, market analysis, a business plan, targeted marketing, and solid business practices.
1. Preparation for Private Practice
Rather than using a trial-and-error approach and just learning as you go along, it is best if you prepare well in advance to enter private practice. You can begin by using the resources that surround you to explore options that will allow you to become more marketable and better prepared to be a successful private practitioner. Use your graduate school professors, professionals in your community, state and national professional associations, internet websites, and social media networking sites to explore your options as early as possible. Seek out mentors who can assist you to prepare for a successful career as a private practitioner. Refer to the checklist below to familiarize yourself with some of the issues you will want to consider both before and after receiving your degree.
1.1 While You Are Still in Graduate School
Take elective courses in specialty areas that interest you. Possibilities include group or family psychotherapy, clinical hypnosis, stress management, and neuropsychological assessment.
Explore specific externship/internship opportunities that will prepare you for the type of private practice you would like to have.
If your school offers a course in the business aspects of practice, take it!
Seek out professional continuing education classes that focus on business aspects of practice.
Join your state psychological association and Psychologists in Independent Practice (Division 42) of the American Psychological Association. Participate in one of their mentoring programs.
Talk to those professors who also work in private practice and other mentors with experience in private practice and ask questions such as:
◦ What experiences should I seek out as a student to better prepare me for a career in private practice?
◦ What challenges and obstacles might I face when entering private practice and what are some actions to take to help overcome them?
◦ What lessons have you learned over the years that contribute to being successful in private practice?
1.2 After Obtaining Your Degree
Explore post-doctoral opportunities that will enhance your skills as a private practitioner. See Chapter 23 of this volume for further information on the potential importance and role of post-doctoral fellowships.
Continue working closely with a mentor who is an experienced and successful private practitioner. There is no need to have to go it alone.
Research geographical areas that interest you and determine their needs. Consider the following when deciding to practice in a certain area:
◦ If there are any groups of potential patients whose needs are not being adequately met.
◦ Assess your local area to see if it is saturated with practitioners with a certain specialty.
◦ Consider if the region you’ve selected for your private practice is saturated with managed care or if most private practitioners in that area have fee-for-service practices.
Determine if you will be able to join managed care panels and if so, how long this process takes and when you can begin.
Consider how much “unpaid” time you will spend collecting payment from managed care organizations and if it would be worth your while to hire administrative help.
Determine if you should open your private practice immediately or if you will need to start with other work and build your private practice into a full-time enterprise over time.
Develop a business plan, including a budget, for establishing and running your private practice. Determine which experts you should consult with to assist you with this endeavor. You might wish to seek out and consult with an attorney or a Certified Public Accountant at this stage to get a feeling for the ways in which you can set up to protect yourself, financially and legally.
1.3 After You Enter Practice
Continue relationships with current mentors and seek out others who have expertise in areas of relevance to your private practice.
Continue your relationships with your attorney, Certified Public Accountant, and perhaps add the services of a Certified Financial Planner to further assist you with the legal and financial aspects of private practice.
Consider using the resources available through The Practice Institute (https://thepracticeinstitute.com) for business and marketing consultation, education, support, and assistance.
Reflect on what successes and failures you have experienced in beginning and running a private practice. Learn from them, build on your successes, and don’t repeat the failures – consider them lessons learned.
Determine the most important things you have learned about running a successful private practice and keep these lessons in mind.
Consider what impact your theoretical orientation has played on the nature of your private practice and on your level of success. Remember that you can build on what you know to be able to serve your client base more comprehensively. For instance, if you are trained in the use of Cognitive Behavioral Therapy (CBT), you may wish to enhance your competency around the practice of mindfulness meditation, which is often successfully used as a part of CBT.
Seek out continuing education opportunities that will expand the skills you can offer to the public. Always consider the niche markets in your area that will keep the clients coming.
2. Is Private Practice For You?
A career as a private practitioner is not for everyone. However, for those who are well-prepared and who have realistic expectations, it is an enriching and rewarding career choice. Educate yourself about the realities of private practice to ensure your decisions are not influenced by common myths or misunderstandings about private practice (Reference Barnett and ZimmermanBarnett & Zimmerman, 2019). Consider if private practice is a good fit for your personality, needs, and professional goals. Personal characteristics such as strong internal motivation and an entrepreneurial spirit will certainly play a role in your success in private practice, but these factors alone are not enough. Consider the pros and cons to establishing and maintaining a private practice provided in Table 17.1.
| Pros | Cons |
|---|---|
| Being your own boss | Financial uncertainty and risk with possible periods of low earnings |
| Ability to decide practice location, hours, areas of specialization | Responsibility for all expenses and overheads |
| Unlimited earnings potential | Possible professional isolation for solo practitioners |
| Flexibility | Responsibility for billing, collections, insurance, employee and staff decisions |
| Control over business decisions | |
| Full responsibility for success of practice |
After making the decision to enter private practice and considering the personal characteristics and professional issues above, it is important to start thinking about some of the more practical issues you will face as a private practitioner. For instance, how will you start your practice? Jumping right into full-time private practice is not necessarily a viable option for all recent graduates. Consider the most realistic and beneficial options relevant to your situation. Specifically, find out how much time it takes to build a full-time private practice, assess the financial demands of opening a practice in your area, evaluate how you will make ends meet while you are building your clientele, consider your need for health insurance and other benefits, and make sure you will be able to find sources of professional support, especially early on. When examining the big picture, some recent graduates prefer to start out in another setting and transition to private practice slowly. This is not considered failure or a ‘second best’ option, and in fact may teach you valuable lessons that will reinforce the success of your future practice as an independent practitioner.
One way to do this is to work full-time in a salaried position and start your private practice in the evenings and on weekends. This will provide you with a full-time salary, benefits, collegial interaction, and supervision. This is a good time to develop competence in specialty areas of practice that you can begin marketing in the local community. You will also have the opportunity to network with other professionals in the local area and to build your reputation while avoiding the potential financial instability that may be a part of your early years in practice. Or, if you have the financial flexibility, you might want to work part-time in a salaried position with benefits and build your practice in the remaining time. While perhaps slightly more risky from a financial perspective, this arrangement gives you more time to build your practice while enjoying the security and benefits of a salaried position.
An additional option is to dedicate yourself full time to the development of your private practice. This choice provides the fastest route to a full-time private practice but carries the greatest financial risk. With each of the first two choices you can decide, based on your success and/or preference, just how much of your time you want to spend in the private practice setting. Some practitioners cut back on the number of hours worked in a salaried position as their private practice grows. Others will find that working part-time in two positions provides them with the best possible combination of financial stability, benefits, varied work activities, and collegial interactions to meet their needs.
Another important decision to make concerns your practice setting. You may choose to open your own “solo” private practice; you may form a group practice with one or more colleagues; or you may join an already existing group practice, whether it be only with other psychologists or with a range of other mental health professionals. When starting out as a solo practitioner you may lease office space on your own or sublet an office in a suite with other mental health professionals. For those who decide to build their practice part-time, subletting space in a larger suite of offices may be the best course of action. Offices may typically be rented quite economically, often by the hour, the half-day, or by the day, and come furnished and offer amenities such as telephone, photocopier, internet access, and even a shared receptionist to greet patients and answer the phone. As your practice grows, you may be able to contract for additional time in the office. Another benefit of this arrangement is the proximity of colleagues. Being in a solo private practice on one’s own may be an isolating experience. Further, not having to pay for office space full time when only using it part time is much more economical. However, when working in a suite of offices with other mental health professionals it is important to ensure that your solo or independent practice is clearly represented to others so that you will not incur any liability from the actions of others in the office suite.
If you choose to participate in a group practice, an additional point to consider is the composition of the group. It may be comprised entirely of psychologists or it may be a multidisciplinary group. Further, as Reference Walfish and BarnettWalfish and Barnett (2008) recommend, “When joining a group practice, choose your associates wisely. These individuals can enhance or detract from your reputation and increase or decrease your liability” (p. 56) and your income! Thus, all potential practice arrangements should be fully investigated and careful consideration should be given before making such a decision. Table 17.2 provides an overview of the benefits and drawbacks of solo and group practice arrangements.
Table 17.2 Considerations for a solo practice or group practice
| Solo practice | Group practice |
|---|---|
| Pro: Practitioner independence. Set your own hours, salary, benefits; decide how to run your practice | Pro: When you have a psychiatrist on staff you will have easy access and ongoing communication about your patients who need treatment with psychotropic medications in addition to their psychotherapy |
| Con: You must find mentorship and supervision on your own as you need it. This might come at a cost | Pro: Interprofessional collaboration and within-group referrals |
| Con: No administrative support, you will have to allow time for paperwork and correspondence | Pro: Access to clerical and administrative support |
| Con: Higher costs of operation unless operating from your home, which has drawbacks of its own | Pro: Lower overheads/sharing of costs |
| Pro: Absolute authority over all decisions | Con: Sharing of decisions and of profits |
| Con: Unlimited personal liability | Con: Each member of the group must accept some liability for the actions of all group members |
Again, it is helpful to speak with private practitioners in a variety of practice settings to hear about their various experiences. This will help you decide on the best plan of action for you. Keep in mind, however, that many practitioners look for positions, get interviewed, accept an offer, and then see how it works. There is only so much we can know in advance; some of it must be learned through experience. However, if you consider all these issues and get a clear sense that one practice arrangement best suits your needs, personality, and comfort level, then that is what you should try.
2.1 Questions to Ask When Considering Joining a Group Practice
Who owns the group and who makes business decisions?
How are referrals shared and what assistance will be provided to help me get started?
What administrative support do I receive from the group?
What per cent of the income I generate goes to the practice and what per cent to me?
Does this percentage change over time and if so, by how much and what factors impact this?
What if I decide to leave the practice; can I take my patients with me?
What benefits am I provided; malpractice insurance, continuing education, etc.?
Am I allowed to decide which patients I will treat?
What supervision and on-call coverage opportunities and obligations exist?
What are the criteria for evaluation and how does one become an owner or partner?
As you begin to attempt to set yourself apart from the many psychotherapists, counselors, and other mental health clinicians competing with you for a limited number of potential patients, it is important to be able to be more than just another generic mental health professional. This is where your “niche” might come into play. This is not to suggest that providing psychotherapy and assessment services with excellence is not a worthy endeavor, but these skills should be viewed as the foundation for your private practice. Beyond that, consider developing an area of expertise that can be marketed to targeted audiences (and that also are typically fee-for-service endeavors where you will earn more and not have to hassle with managed care).
Psychologists in Independent Practice, Division 42 of the American Psychological Association, has an excellent series of niche practice guides that provide an excellent introduction to developing a specialty. Each guide provides a detailed description of the specialty area, information on how to enter it, what training is needed, and where to obtain it and training resources available, ethics issues to consider, marketing considerations, and a list of resources to access for additional information. Thirty six niche practice guides are presently available for such diverse areas of practice as health psychology, infertility, psycho-oncology, eating disorders treatment, marital therapy, working with stepfamilies, smoking cessation, ADHD assessment and treatment, geriatrics, sport psychology, treatment of personality disorders, neuropsychology, women’s issues, psychologist–dentist collaboration, child custody evaluations, men’s issues, and many others. These very useful guides may be ordered through the Division 42 website at www.division42.org. Developing specialty areas is an important step for setting yourself apart from other practitioners in your community. Select areas that interest you, obtain the needed training, and then begin marketing the services you have to offer.
In addition to providing clinical services, you should consider how you might apply the knowledge and skills you already possess to other areas that would augment your clinical practice. Suggestions include business consultation and team building, personal and executive coaching, divorce mediation, school consultations, and forensic evaluations. An additional excellent resource for those starting out in practice is the book by Reference WalfishWalfish (2010) that describes 50 different practice areas for providing professional services outside of managed care. While one should only enter specialty and niche areas of practice with supervision from, or consultation with, an experienced colleague, you may be surprised how little additional training and experience you’ll need to be competent in these additional areas of practice. Another useful, and hopefully inspirational, resource is Reference Verhaagen and GaskillVerhaagen and Gaskill’s (2014) book How we built our dream practice: Innovative ideas for building yours.
3. The Business of Practice
Even the most competent clinician can end up sitting alone in the office waiting for the phone to ring. After assessing your local area’s needs, developing a specialty area or practice niche, deciding on group or solo practice/multidisciplinary or all psychologists, purchasing business cards and possibly even developing a website and/or social media presence for your practice, you must now tackle the business of practice; and it is a business. Ask yourself the following questions regarding the business of running a private practice.
First, will I work as an independent contractor or an employee? An employee is hired by, and works for, an employer; is directed by the employer which patients to treat, when, and how; and the employer takes out withholding for taxes and pays a portion of the individual’s social security tax. IRS Tax Topic Bulletin 762, Independent Contractor (Self-Employed) or Employee, explains that an independent contractor is defined as an individual who is not an employee, but who works with another individual under a contractual agreement. Independent contractors treat whichever patients they like, and when and how they might like. They purchase their own supplies and set their own hours. They pay quarterly estimated taxes and no taxes are withheld by the other person. For additional information see the Internal Revenue Service’s website at www.irs.gov/taxtopics/tc762. Additional important information is provided at the IRS webpage Independent Contractor Defined at: www.irs.gov/businesses/small-businesses-self-employed/independent-contractor-defined.
If you should choose to work as an employee, ask yourself how you will establish your fee structure for services rendered and how you will be compensated by the practice. Employees typically receive a specific salary and benefits, based on a certain number of employee billable hours provided in the practice. The employer also pays a portion of the employee’s social security taxes. Additional administrative tasks may also be assigned as part of your work duties as specified in your employment contract. As an employee, you have the right to negotiate your employment contract, but do consider the learning and support you will receive as an employee as part of what you are gaining and factor that into your negotiations.
For independent contractors the typical arrangement is to pay the practice owner a certain fee or certain percentage of fees collected for each patient seen. Typically, independent contractors working within an established practice pay the practice owner 40 per cent of all fees collected and keep 60 per cent for themselves. If you are offered a lower percentage of fees collected, such as 50 per cent, be sure your contract stipulates criteria for it increasing over time. Keep in mind that a lower percentage reflects the fact that the practice may be providing referrals and your business will get built-in marketing just by being a part of an established practice with its own reputation. A typical arrangement would be to start with paying 50 per cent to the practice and then having this percentage decrease as you begin generating your own referrals. Should you begin providing referrals to others in the group due to your success, the percentage paid to the practice should decrease even further. All of this should be clearly laid out in the contractual agreement signed upon joining the group. Being aware of these long-term issues when starting out is very important to your success in private practice.
It is essential that you have all contracts reviewed by your own attorney prior to signing them. Without legal training, we are not able to know the implications of every clause that may appear in a contract. Your attorney is your advocate and considers each contract based on your best interests, at present and over the long term. An investment in legal services at the outset is an investment in yourself and your practice. Paying for the services of an attorney can save you tens of thousands of dollars over the years as opposed to trying to do it all on your own. Specifically, your attorney will help you agree to a contract that contains provisions that will grow your earnings in years to come. Failure to consult with your own attorney prior to signing a practice agreement or contract may result in your unknowing agreement to provisions that promote the best interests of the practice owners over your own best interests, and sometimes even at your expense.
Additionally, as you negotiate the contract, you will need to consider what you are receiving for the percentage of collections you pay to the practice. The practice owner is providing the office space, furnishings, office staff and supplies, and perhaps most importantly, referrals of patients for you to evaluate and treat. Typically, practice owners who are very busy and have more incoming referrals than they can personally treat will take on independent contractors. For the new psychologist just entering private practice this can be an excellent way of starting out. There is a ready stream of referrals, a furnished office with trained staff and infrastructure already in place, and the possibility of supervision and peer support. As mentioned, other contractual arrangements are possible, such as leasing space in another practitioner’s or group’s office, so consider the options available to you as you find the arrangement that is in your best interest and best meets your needs based on your particular circumstances.
Finally, be sure to educate yourself on certain business principles such as non-competition clauses before you sign a practice agreement or contract. This is a major area of concern for independent contractors, especially when and if you eventually hope to leave the practice and branch out as a fully independent practitioner. The non-competition clause will be laid out and agreed upon between you and the practice owner when signing your initial contract. This clause may specify that if you decide to leave you may not practice psychology for a specified period of time within a certain distance of the practice you are leaving. This will protect the practice owner from direct competition from you should you decide to leave after they assist you in becoming established and developing your professional reputation with referral sources in the local area. Unless you have a specialty area not otherwise available in the local area, such contractual clauses are generally deemed enforceable. The practice owner is providing you with referrals and assisting you to develop your reputation and referral sources in the local area. Without such a clause in the contract you could fill your schedule, build your reputation, and then leave and open your own practice across the street or across town. Yet, these clauses can sometimes be negotiated and they do not necessarily need to be included in practice agreements and contracts. This is another important aspect of contractual negotiations where your attorney can prove invaluable.
4. Rules of Business Success
4.1 Consult the Experts
The first thing you need to know, even if you open a solo practice, is that you can never enter or run a private practice on your own. You will need the services of experts in two key areas of expertise: legal issues and accounting. As has been highlighted, unless you have graduated from law school we strongly suggest that you never enter a business arrangement or sign any contract before first consulting with your attorney. Too many practitioners have learned the hard way just how costly a mistake being your own attorney or accountant can be. While their fees may seem expensive, these professionals will save you a great deal of money, anguish, and legal difficulties in the long run. Speak to experienced practitioners in your local area to find out who they use, if they are happy with the fees charged and services provided, and then use this input to guide you. You may also obtain referrals for attorneys through your local or state psychological association as well as through the local bar association, but be sure to check their references and reputation. Don’t rely on fancy advertisements for guiding you in such an important decision. Just to clarify the point made above … never sign any contract without first having it reviewed by your attorney who will ensure it is in your best interest and suggest any needed modifications before you sign it.
A Certified Public Accountant (CPA) can assist you with numerous important financial aspects of setting up and running your private practice. For a detailed explanation of all this see the book Financial management for your mental health practice by Reference Zimmerman and LibbyZimmerman and Libby (2015). Additionally, a CPA can assist you in making important decisions such as if you should incorporate your practice and if so, how. Numerous options exist to include incorporating as a Limited Liability Corporation or a Professional Corporation, among others. Each incorporation status brings with it different costs and benefits. Your CPA will be able to guide you to make the best choice for your needs and circumstances. A CPA can also assist you with retirement planning, something you should consider from the outset of your career.
A Certified Financial Planner can be of immense help in offering guidance on investments and retirement planning. Private practitioners need to save money for their retirement and invest it wisely over the long term. Unless one is a salaried employee who works for a company that offers a pension plan, one has to plan for and save for their own retirement. Consulting with a financial expert can make this process easier and more successful.
4.2 Market Your Practice at Every Opportunity
Even if you are an independent contractor in a group practice, but especially if you decide to open your own practice, marketing yourself to the local community and to a variety of possible referral sources is of great importance. Potential referral sources may include physicians in your community, schools, attorneys, other mental health professionals, and a variety of others depending on the type of professional services you offer. It is important that you have a visible and positive presence in-person in your community as well as online.
4.3 In-Person
Possible strategies to secure referrals include:
Send an announcement of your practice opening. Follow up with a brief letter describing your training, background, and expertise. Be sure to tailor the letters to the perceived needs of each referral source and the specific population they serve. (See Appendix A for an example.)
Telephone potential referral sources and request a brief meeting to meet and describe the services you offer (and how you can help them and their patients). Especially if you contact medical offices or other practices, determine whether you can offer a service they need and mention that specific service when you call. Let them know that you would be willing to briefly attend a few minutes at the start or the end of their next staff meeting so that you have the chance to meet everyone at once and answer any questions.
Offer free presentations to the patients of your referral sources. For example, you could offer a seminar on behavior management strategies to the parents of a pediatrician’s patients, a presentation on stress management skills to an internal medicine physician’s or cardiologist’s patients, or a seminar on strategies for working with certain types of learning disabilities for teachers at a school you hope will refer patients to you.
If you give presentations or seminars, be sure to bring business cards, brochures, and fliers describing you, your practice, and the services you offer. Ensure that all these materials include your e-mail address and the web address for your website. You can utilize marketing professionals and create your own brochure or you can purchase brochures from the APA’s Division 42 and then attach your business card to them.
The APA offers free fact sheets that provide practical information on a wide range of mental health issues and how psychologists can help address them. These are available at www.apa.org/helpcenter/fact-sheet.
Keep likely referral sources updated on additional training you receive and new types of patients you can treat.
Some private practitioners write a monthly or bi-monthly newsletter or blog that they send to members of the community. Others write columns in local newspapers or do radio talk shows or podcasts on mental health topics, and some give presentations to local groups such as C.H.A.D.D., the PTA, support groups, or at sites such as the YMCA, senior centers, and schools. These indirect forms of marketing may also be very effective in establishing your reputation as a local expert and can increase your referrals over time. When giving these presentations do not worry about lost billable time; you are making an investment that may pay significant dividends over time through the referrals these presentations may generate.
4.4 Online
Utilize available professional referral services. Some, such as Psychology Today which at present costs $29.95 per month and which provides an online listing accessible over the Internet, can be very cost-efficient. If this generates just two referrals per year you will likely be making money on your investment. Other online referral networks exist and each should be investigated to see which best meets your needs.
Use technology to market yourself as well. Create a website for your practice and link it to a variety of mental health sites. Be sure to keep it up-to-date and include useful information for visitors similar to a brochure or newsletter. If you write a blog or publish podcasts, make them public and sharable via your website so that referral sources can easily get to know you via this source.
Visit a range of other practitioners’ websites to see what you like and dislike about them as well as what you find to be effective and ineffective. You may create your own website utilizing many widely available templates that can be utilized by filling in your information. You also may hire a web designer who can assist you in designing, creating, and managing a customized website that best meets your practice’s needs.
It is also important to have a broader social media presence. This may include the use of platforms such as Facebook, LinkedIn, or Twitter, among others. Being seen as an expert by members of the public can help generate many referrals to your practice.
You should also market yourself to your colleagues. Utilize your contacts in the State Psychological Association and let them know of your practice and the services you offer. Explore the successful practices in your local area and offer to take the practitioner(s) out to lunch to introduce yourself and meet with them. Many practitioners with busy practices are frequently looking for colleagues to whom they may refer patients they can’t fit into their schedule. They also need competent practitioners to whom they can refer patients whose needs fall outside their areas of expertise. They are only likely to refer patients to you if they know you and the services you provide.
Writing articles in your State Psychological Association’s newsletter, giving presentations at conferences and continuing education events, and participating actively on the organization’s listserv, each may make you known to your colleagues in a way that highlights your professionalism and areas of professional competence.
4.5 Follow-Up
Keep in mind that only half the work is done when you have received a referral. By nurturing the contact, you will be sure to keep the referrals flowing in. For instance, when a referral is received, always send a letter (or e-mail message) of acknowledgment of the referral (with appropriate consent of the patient). In the case of specific services, be sure to keep the referral source in the loop at pertinent stages. For instance, when doing an evaluation, forward a copy of your report to the referral source; for treatment, provide periodic written updates on the patient’s treatment progress. Always be sure to first obtain the patient’s written consent before doing sharing records of any kind.
Also bear in mind that your relationship with your referral sources will be best served if you can reduce their workload and help them to solve problems. Ask them, specifically, what they need and what obstacles they are facing in their practice and market yourself accordingly, if appropriate. Initially, they may send you their most difficult and demanding patients. Satisfied clients and successful treatment outcomes are your most powerful marketing strategies (see Appendix B for a sample letter). Additionally, if a referral is inappropriate for you or your schedule is full, you may want to assist your referral source by offering other appropriate referral suggestions if you know of any. Being helpful in this way can possibly lead to receiving many more referrals from them.
In summary, you must provide high-quality services, give referral sources timely and useful feedback, and market your services both directly to referral sources and indirectly to the community. Actively follow-up all these marketing efforts on a regular basis.
5. Being a Business Person and Entrepreneur
If you are in practice, you are in business. While your goal undoubtedly is to help others in a compassionate and caring manner, if you are not adequately compensated for the professional services you provide you will not be able to stay in practice. Thus, you will need to run an effective business. You will need to create a business plan, understand what your start-up expenses will be and how much financial support you will need to run your practice while working to build it, and know how many patients you will need to have to break even and to then begin making a profit. Reference Stout and GrandStout and Grand (2005) provide an excellent template for a business plan in their book Getting started in private practice: The complete guide to building your mental health practice. Using such a template can help ensure that you have a viable and realistic business plan for your private practice and increases the likelihood of being financially successful.
You will also need to address issues such as renting or leasing office space, buying or renting furniture and décor, signing up for utilities and telephone service, and purchasing and maintaining necessary insurance (professional liability insurance, premises insurance, etc.). You will also need to decide which administrative tasks you will do yourself and which ones will be supported by someone other than you. You can either contract out certain services (like insurance billing) or you can hire administrative support staff to do it in house. Depending on who you hire and the agreement you make, support staff can handle everything from billing, collecting, and bookkeeping to scheduling, client relations, and external communications, as directed by you. Finally, with guidance from your attorney and accountant you will need to decide what tax status is most advantageous to you. You may decide to become a professional corporation, a limited liability corporation, a sole proprietor, or some other legal status. Each brings with it certain potential tax and liability costs and benefits.
It goes without saying that as a business person it is essential that you provide patients and referral sources with excellent service. In fact, you should be thinking (at least in part) of your ability to provide high-quality customer service from start to finish, just as any business owner would with their customers. Your patients are customers who are purchasing a service from you. Customer service can include business practices such as:
Returning telephone calls, emails, and texts in a timely manner. Thus, you will need to schedule time to check for messages and to return communications throughout the day. Be sure to check for messages evenings, weekends, and holidays unless you have otherwise communicated your availability directly to your patients.
Have an office that is welcoming and comfortable for patients. Many practices have complimentary water, coffee, and tea available in the waiting room. Comfortable furnishings and a professional atmosphere are important. Consider a white noise machine if you will have clients in a waiting area while you are in treatment. Even if you know that your treatment area is soundproof, your clients do not, and the extra step will give them comfort.
Ensure that office staff members are warm, welcoming, and professional with patients.
Be flexible with scheduling. Offering appointment times that are convenient to patients, especially when starting out, is very important. This may include working some early morning, evening, and weekend hours.
Complete work in a timely manner. For those conducting evaluations, be sure to schedule feedback sessions quickly and have the evaluation report ready for the patient at that time.
Be available to patients between sessions should they experience a crisis or have questions for you. If you use e-mail or texting, check it often and respond quickly. Be sure patients know how to reach you should a question or crisis arise between treatment appointments. Communicate your emergency procedures clearly and early in treatment, particularly a patient’s need to call 911 (or other local emergency services number) if they are in crisis and cannot reach you.
Return telephone calls from referral sources in a timely manner and periodically provide them with written feedback on the work you are doing with the patient they refer.
One goal is for your patients to feel that they were treated well and that the clinical services provided met all their expectations. However, Reference BermanBerman (2005) takes this one step further, speaking of customer delight, the notion of exceeding your patients’ and referral sources’ expectations and achieving high standards of excellence in all aspects of their experience with you. The goal here is to provide them with an experience that leaves them so satisfied that they share about their experience with others, thus being valuable referral sources for you.
6. Setting Up Your Practice
If you work as an employee or an independent contractor in someone else’s practice, this will be taken care of for you, but if you open and run your own private practice you must consider and address these important issues.
First consider the physical office. The actual office must be set up so that patient privacy is protected. The use of soundproofing, white noise machines, and even insulated ceilings, walls, and doors all help to keep confidential communications private. Secretarial staff should have an area apart from the patient waiting room where telephone calls can be made. A locked room with lockable file cabinets for treatment record storage is mandatory.
Next, consider insurance coverage. At a minimum you will need malpractice insurance. It is typically recommended that your coverage be for $1,000,000 per claim and $3,000,000 per year. If you obtain hospital privileges or work on any managed care panels this is typically the amount of coverage they require you obtain and keep in force. You may also wish to obtain disability insurance to provide you with coverage should you be unable to work for a period of time and you should consult your attorney about additional types of insurance for your office and staff. You may purchase two types of malpractice coverage: occurrence and claims made. Occurrence insurance provides coverage for claims made against you any time during your career, even if you discontinue your coverage. Claims made insurance only provides coverage while the policy remains in effect. While occurrence insurance is more costly, many choose it due to the coverage provided. The largest malpractice carrier for psychologists is The Trust (www.trustinsurance.com). Others include the American Professional Agency (www.americanprofessional.com) and Healthcare Providers Service Organization (www.hpso.com/individuals/professional-liability/malpractice-insurance-for-counselors).
Next, unless you plan to do all jobs (answering the phone, greeting patients, collecting fees, billing, doing insurance paperwork, filing, etc.) you will likely hire staff. Consult with your attorney and accountant and learn about applicable laws concerning interviewing and hiring practices, employment law, taxes, and related issues. Then be sure all persons hired understand both their job duties and all applicable ethical standards. Train your staff about confidentiality and related issues. Have written office policies that you instruct them in and have them agree to in writing. Be sure to supervise them adequately to ensure they do not exceed the agreed upon limits of their roles.
Another important area is fee setting. While you certainly should be paid what you are worth, it is advisable conduct an informal survey of private practitioners in your local area to see what fees they charge. You may either ask them directly, telephone their offices as a potential patient requesting information about their practice, or look for this information on their website. Not only will you learn their fees, but you will also learn about their office policies from the information they share.
You will then need to establish procedures, forms, and documents for informed consent, release of information, payment policies, billing and the use of insurance, the use of collection agencies, intake forms and questionnaires, follow-up letters to referral sources, follow-up letters for patients who drop out of treatment and for those who successfully complete treatment. You may also choose to do some patient satisfaction surveys, treatment outcome measures, and other measures. Rather than try to develop all these policies and forms yourself, you should request copies of those forms used by colleagues when you meet with them as well as from your mentor. You may also find several resources very helpful in this endeavor.
First, Zuckerman and Kolmes’ (Reference Zuckerman and Kolmes2017) book The paper office for the digital age is an excellent resource. It includes numerous sample forms, written policies, handouts, and guidelines. The book also includes a CD so that forms may be downloaded and printed for use in your practice. Typical forms include those for informed consent; a practice information form to distribute to patients that includes explanations of such issues as appointments and fees, billing, cancellation policy, emergencies and after-hours contact, the process of therapy, confidentiality, and related issues; a patient intake form; an informed consent to submit insurance form; and an employee agreement to maintain confidentiality form, and many others. They also provide useful information on marketing your practice online to include a web presence and use of social media.
You may also obtain a model informed consent to treatment form on the website of The Trust (www.trustinsurance.com). Additionally, this website provides a sample child therapy contract and a sample forensic informed consent document. You may download each of these and modify them for your use.
An additional valuable resource is the Clinical documentation sourcebook by Reference WigerWiger (2020). This volume provides many useful forms such as those designed for HIPPA compliance, administrative and intake forms, screening and assessment forms, and forms used during the course of treatment, among others. Additionally, several companies market software for tasks such as documentation and patient billing. Many psychologists find the use of such software a great benefit in terms of efficiency and consistency. Examples include TheraScribe (www.therascribe.com) and TherapyNotes (www.therapynotes.com). Finally, practice management software such as therapyappointment (www.therapyappointment.com) and TheraNest (www.theranest.com) provide software that assists in automated client management, scheduling, billing, insurance filing, and related services. Ratings of, and information on, numerous other practice management software products may be easily found by doing an online search.
Finally, supervision is especially important as you begin your career. In addition to individual supervision you may form or join a peer supervision and support group to connect you with other new private practitioners as well as more experienced colleagues. This may be of great help from a clinical standpoint, especially as you develop tools to help you better cope with the many demands of opening and running a private practice. A supervision relationship or group may also become a source of referrals. You should also consult with the information provided in Chapter 4 of this volume for much more detailed suggestions for addressing this important area of our professional development. Commit yourself to lifelong learning and ongoing professional development. It is essential that you keep your knowledge and skills current so you can best meet the assessment and treatment needs of your local community.
In conclusion, the private practice of psychology is an exciting and rewarding endeavor. With adequate advanced thought, preparation, and the use of the resources and strategies described in this chapter you should have a good head start. While a single chapter cannot be an exhaustive reference on all aspects of preparing for and being successful in private practice the information presented above and the checklist in Table 17.3 should be of assistance.
Table 17.3 Checklist for beginning your private practice
|
In a profession that is rich with complexity and virtually boundless in applications, the simplest of facts remains: if you want to practice as a psychologist, you must be licensed to do so. This is true in every state, province, and territory of the United States and Canada. In several states, you may not legally use the title of “psychologist” without a license to practice psychology. Perhaps the most damaging reality is that a license is required by nearly every third-party payer for reimbursement of services and a requisite for employment for most positions at major agencies that employ psychologists (e.g., the VA). Without the ability to independently receive reimbursement for services, there is very little you can do without a license to practice and earn a sustainable income. Although the primary rationale for the license to practice is protection of the public, it can sometimes feel like yet another hurdle to a new psychologist.
Many graduates of doctoral-level psychology programs go on to have full and rewarding careers without ever obtaining a license. University professors and research scientists have no practical need for it (although some will obtain a license to supervise clinical students, conduct treatment outcome studies, or to satisfy accreditation requirements). Nevertheless, if your plan is to rely on practicing psychology as a service provider, then the psychology license represents the first essential requirement for independent practice. You do not become a practicing psychologist when you receive your doctorate; you become one when you obtain your license.
You may have various reasons for wanting a license. You may be training to start a career as a full-time practicing psychologist, or you may plan to work in an academic setting with the hopes of doing some clinical work on a part-time basis. Perhaps you want to train and supervise students to become psychologists themselves. Regardless of your reason for seeking licensure, there are many things that you need to know in order to make the licensure process occur smoothly and expeditiously. This process has changed significantly in noticeable ways in the 20 years since this chapter was first written for the first edition of this book, as well as since the second revised edition. Prospective applicants at the dawn of the new millennium were still sitting for paper-and-pencil licensure exams, which were only offered on two fixed dates per year. Even the precursor to the iPhone, the iPod, had yet to be invented, and study preparatory kits still offered tape cassettes as part of their materials. Students and post-docs and early career psychologists sought support and answers to their questions on email listservs rather than social networking sites. Nearly every jurisdiction (state and/or province) would not allow a post-doc to take the Examination for Professional Practice in Psychology (EPPP) during their post-doc year and several other licensure laws and statutes had yet to be changed. Since the second edition of this book, there have been further changes for more states allowing newly minted psychologists to become licensed directly after internship (negating the need for a post-doc year). In addition, more recent changes have been the development and piloting of some states to require the EPPP (Part 2 – Skills) for licensure.
In spite of these changes in the past 10 years, the basics for getting licensed have not: obtaining your doctoral degree, completing internship, passing licensure examination(s), providing letters to your state or province’s board of verification of completion of educational and clinical hour requirements. This chapter is intended to provide you with the main information you need to plan and execute the process of obtaining your license. As you will discover, there is some variability among states, provinces, and territories that may play a role in your future as you plan your career. Table 18.1 lists a number of suggestions for beginning the licensure application process.
Table 18.1 Essential tips for getting licensed
Applying/Preparing (during your pre-doctoral internship year)
Studying (during your post-doctoral year)
|
1. Before You Even Get Started: Looking Ahead
Psychology licensure laws are quite different from driver’s license laws, in more ways than one. Every state, province, and territory in the United States and Canada has its own unique licensure law. Although the laws are all generally similar, there is enough variability to make some license requirements uniquely different from others (e.g., exam cut-off scores, years of supervised training hour requirements, etc.). To complicate things further, the license for each state, province, or territory applies only for that state, province, or territory in any non-federal job. If you have a license to practice in California, you cannot practice in New York unless you have a New York license; your license only applies in California. If you were to move to New York and you wanted to continue practicing, you would then need to also get licensed in New York.
Because of these differences, it is important to know the state(s) in which you plan to be licensed as you begin preparing for the licensure application process. Unfortunately, this requires an assumption that you know in which state(s) you will be living or working within a year or two; an assumption that may not always be realistic. What if you live in the Washington, DC area and you will be considering jobs in Virginia, Maryland, and the District of Columbia? What if you are considering several different states yet have no idea what jobs will be available? What if your spouse or partner will need to relocate to an as-yet undetermined area in the future? What if you decide to relocate to another state many years into your career? One interesting exception to this challenge is the psychologist practicing for the federal government (e.g., VA medical centers). In general, federal service allows for the psychologist to hold a licensure from any state.
There can be a number of reasons why you may not be certain where you will be practicing, yet you will likely only be able to apply for one state license. Because of this, it is a good idea to become familiar with the requirements for the states you are considering; particularly, your top three preferences. Knowing what these states require will be very important as you complete your internship and post-doctoral training. You want to ensure that your training, whether pre-doctoral or post-doctoral, is meeting the minimum eligibility requirements for all of the states you are seriously considering. Most pre-doctoral internships and post-doctoral fellowships will design their training so that your training hours exceed the eligibility requirements for most states.
2. General Eligibility Requirements for Licensure: What You Will Need
Although there is some variability, requirements for licensure involve three main areas: education, training/supervised experience, and examinations. As noted, each state, province, and territory has its own specific licensure requirements and the wording can often vary. For the purposes of this chapter, eligibility requirements will be described in more general terms.
2.1 Education
All licensure laws for independent practice require a doctoral degree in psychology, usually from a regionally accredited institution. Criteria are usually provided for required coursework. Because each jurisdiction is different, you will want to ensure that your transcript includes the required courses specified. Many states require that the program be accredited by the American Psychological Association (APA), Canadian Psychological Association (CPA), or designated by the ASPPB/National Register Joint Designation Committee. If you do happen to graduate from a non-APA-accredited program, you will need to provide documentation that your program provided all of the required coursework specified.
2.2 Training/Supervised Experience
Each jurisdiction has its own requirement for number of clinical hours necessary for licensure. These requirements have continued to change over the years in several states and provinces. It is generally the standard that at least two years of approved full-time supervised experience are required. Of these two years, one year is usually pre-doctoral (internship) and the other year is post-doctoral (post-doc). However, several jurisdictions have made it easier to become licensed upon graduation, rather than making it legally impossible to be licensed during the first post-doc year. At the time of the first edition of this book, only one state (Alabama) did not require a post-doc year for licensure; at the time of the second edition of this book, 11 US states, 4 Canadian provinces, and 1 US territory did not require that the supervised clinical hours be obtained post-doctorally. As of 2018, now 16 jurisdictions have optional requirements for a post-doc year depending on pre-doctoral hours accrued: Virginia, West Virginia, Kentucky, Indiana, Ohio, Maryland, Pennsylvania, Missouri, Connecticut, Massachusetts, New Hampshire, North Dakota, Wyoming, Utah, Arizona, and Washington.
As the cumulative hours of supervised clinical experience tends to range from 3000 to 4000 per year, the trend toward modifying the requirement that one of these years be post-doctoral has helped prevent the dilemma most post-docs face of being unable to obtain a license during the first year of their career and, subsequently, receive third-party payment for services, be eligible for most clinical jobs, or even legally refer to oneself as a psychologist. Criteria for supervision time, clinical internship, and residency are usually specified. Because of this, it is particularly important to check your prospective state to see what their current requirements are.
2.3 Examinations
A passing score on the EPPP is required by all states, provinces, and territories. The EPPP will be discussed in more detail later in the chapter. Only applicants for licensure are eligible to take the EPPP and eligibility requirements to sit for the exam vary by jurisdiction. The EPPP is most commonly taken upon completion of the post-doctoral year, although some jurisdictions allow post-docs to take the EPPP prior to completion of their post-doc year. Some states also require oral and/or written exams, most often the jurisprudence exam.
Assuming these requirements, it is a good idea to begin contacting any state, provincial, or territorial licensing board for licensure application information before you begin your post-doctoral year. In addition to the application, this should include a copy of the licensure law as well as the rules and regulations of the board. It will be important to determine when you will be eligible to take the EPPP exam, as well as any other required examinations, and to complete any required paperwork prior to the appropriate deadlines. You may find that materials need to be submitted by a deadline that falls during the middle of your post-doctoral year. A list of state, provincial, and territorial psychology licensing board phone numbers and addresses is provided by ASPPB and you can check your jurisdiction’s specific board requirements at: www.asppb.net/page/BdContactNewPG/.
3. Considerations of Differences among State, Provincial, and Territorial Requirements
As mentioned, each state, provincial, and territorial license law is different. As a result of this, there are roughly 63 slightly different sets of requirements. Although they are similar in many ways, you will want to be aware of the way in which they are specifically different. As you review the licensure requirements for the state, province, or territory you are considering, there are a number of questions you will need to address:
Does my degree meet the required criteria?
Do I have the minimum number of required hours for both pre-doctoral internship and post-doctoral training? Do both training experiences meet the criteria?
Do I have enough documented supervision time? Is that requirement specified?
When am I eligible to take the EPPP exam?
Will I be able to obtain my license during my first post-doc year?
What is the cut-off score for the EPPP?
Am I required to take any other examinations?
What are the deadlines for submitting my application and documentation?
What are the various fees I will be expected to pay?
The ASPPB offers a full guide of the requirements for each state, territory, and province on their website. Included in this site is an online and interactive version of ASPPB’s old Handbook of Licensing and Certification requirements, which lists the specific educational, clinical, and examinations required by their state or provincial laws. This comprehensive and easy-to-follow resource on all eligibility requirements for a majority of jurisdictions is now available at: http://psybook.asppb.org/.
As you review the requirements for your state, province, or territory, it is recommended that you consider the requirements for the other 62 licensing boards. It is ideal to exceed the requirements for all 63 licensing boards should you ever wish to obtain licensure in another state later in your career. For example, while Arizona does not require a jurisprudence exam, California does. If you were considering practice in the Washington, DC area, you would want to know that the requirements for face-to-face supervision for post-doctoral training differ from Maryland, Virginia, and the District of Columbia. It would also be important to know that the most common EPPP cut-off score is a scaled score of 500 (or approximately 70 percent), although a few boards have a different cut-off score for each test administration. A review of the requirements for all 63 licensing boards on the three main areas (education, supervised experience, and examinations) will help inform you.
4. The Examination for Professional Practice in Psychology
The EPPP was developed by the ASPPB to serve as a standardized examination to evaluate applicants for licensure. In 2020, the ASPPB bifurcated the EPPP into two components: EPPP (Part 1 – Knowledge) and EPPP (Part 2 – Skills). The EPPP (Part 1 – Knowledge) is the comprehensive exam that was previously known simply as the EPPP. Its stated intent is to evaluate the broad-based knowledge expected to be gained, following the appropriate doctoral education and supervised training in psychology. All 63 licensing boards require the EPPP for licensure in psychology.
4.1 EPPP (Part 1 – Knowledge)
Since 2002, the EPPP (Part 1 – Knowledge) has become administered entirely as a computer exam and is available at any time. The original paper-and-pencil EPPP was made up of 200 multiple-choice items; the computerized administration is made up of 225 items. For several years, the additional 25 items were used as experimental items to be determined whether to use in future administrations and the EPPP score was based on 200 scored items. This ratio shifted slightly starting August 2011, where 175 items are scored and 50 items are unscored “pre-test” items. This represents the first time that the EPPP score is based on 175 items and not 200, which may slightly shift the margin for error. On a 200-item EPPP, an applicant could miss 60 items and still pass in most jurisdictions; on a 175-item EPPP, the margin of error goes down to 52. However, the computerized administration of the EPPP has a time limit of 4 hours and 15 minutes, which allows for 15 additional minutes over the original 4-hour limit of the shorter pencil-and-paper exam, and it is available year-round.
The content of the EPPP consists of items representing eight weighted content areas. The newest current content areas (effective February 2018) are based on an analysis completed in 2017 examining what licensed psychologists do and what knowledge is required of them. Detailed explanations for each of the content areas are available from ASPPB, and are summarized below with their content percentage as well as the specific subdomains covered on the examination.
Ethical/Legal/Professional Issues (16 percent): Knowledge of (a) ethics code (b) other professional standards, (c) mental health-related legal statues, (d) identifying ethical challenges, (e) ethical-decision making models, (f) continuing education, (g) emerging ethical issues, (h) rights of patients, (i) ethics in research, (j) ethics with supervision, (k) ethics with technology.
Assessment and Diagnosis (16 percent): Knowledge of (a) psychometrics, (b) assessment theory, (c) strengths and limitations of different assessment methods, (d) appropriate use of assessments, (e) differential diagnosis, (f) assessment in organizations, (g) cultural issues in assessment, (h) diagnostic systems, (i) data interpretation, (j) epidemiology, (k) theories of psychopathology, (l) outcome measurement, (m) technology in assessment.
Treatment, Intervention, and Prevention and Supervision (15 percent): Knowledge of (a) treatment matching, (b) models of interventions, (c) techniques and their efficacy, (d) treatment of special populations, (e) group and organizational interventions, (f) consultation models, (g) vocational models, (h) telehealth, (i) health systems, (j) public health/prevention, (k) models of supervision.
Cognitive-Affective Bases of Behavior (13 percent): Knowledge of (a) intelligence, (b) learning, (c) memory, (d) motivation, (e) emotion, (f) neuropsychology, (g) cognitive-affective processes, (h) social factors in cognition.
Growth and Lifespan Development (12 percent): Knowledge of (a) growth, (b) impact of environment, (c) models of development, (d) identity developmental, (e) impact of family structure, (f) impact of major life events, (g) risk factors, (h) disease across lifespan.
Social and Cultural Bases of Behavior (11 percent): Knowledge of (a) social cognition, (b) communication, (c) group processes, (d) personality theory, (e) cultural differences, (f) diversity, (g) effects of oppression.
Biological Bases of Behavior (10 percent): Knowledge of (a) biological basis of sensation, perception, and mood; (b) psychopharmacology; (c) results of major psychopharmaceutical clinical trials; (d) genetic basis of behavior; (e) neuroimaging methods.
Research Methods and Statistics (7 percent): Knowledge of (a) sampling, (b) research design, (c) data analysis, (d) data interpretation, (e) research designs and their limitations, (f) research evaluation, (g) community research.
The computerized EPPP (Part 1 – Knowledge) can be taken 6 days a week throughout the year. Should you need to retake the examination, up to four exams are allowed per 12-month period; you would only need to wait at least 60 days from your previous administration. The EPPP is administered at an authorized Prometric Testing Center, for which there are available testing centers in every state, and you need not take the exam in the jurisdiction for which you are applying. After applying for licensure in your jurisdiction, you can then register to take the EPPP online through ASPPB’s website at www.asppb.net. Prometric Testing Centers in your vicinity can be located at www.prometric.com.
Another significant difference resulting from the shift to computerized testing is the use of scaled scores. The old pencil-and-paper EPPP utilized a raw score and was reported as a percentage. For example, an applicant receiving 150 correct answers out of 200 would receive a raw score of 150, or 75 percent. With the computerized exams, the raw scores are converted to National Scaled Scores ranging from 200 to 800. This is done in an attempt to allow comparisons of different exams with varying difficulties. A National Scaled Score of 500 is considered the equivalent of a raw score of 140, or 70 percent. A National Scaled Score of 450 is considered the equivalent of a raw score of 130, or 65 percent. Since 2002, all scores are reported as scaled scores.
No computer proficiency is needed to take the computerized EPPP. The program is designed to allow you to skip a question, if necessary, and return to it later on. Upon finishing your exam, results should be received within two to three weeks, although an unofficial score will be given right away at the testing center.
4.2 EPPP (Part 2 – Skills)
Perhaps the most significant change upon the licensure landscape since the publication of the last edition of this chapter is ASPPB’s development and introduction of a second component of the licensure exam that focuses on clinical competencies. According to the ASPPB, the impetus for adding a second component to the licensure exam was a need for a standardized assessment of clinical competencies, heterogeneity of the training of psychologists, and unreliable alternative methods of gauging clinical skill.
Development of the exam started in 2016 and a beta version of the EPPP (Part 2 – Skills) launched in late 2021. Currently, EPPP (Part 2 – Skills) is in its “early adopter phase,” which means that the jurisdictions who early adopt are now requiring completion of both the original EPPP, now named EPPP (Part 1 – Knowledge), and the EPPP (Part 2 – Skills) in order to be licensed. Currently the early adopters of the EPPP (Part 2 – Skills) are: Arizona, District of Columbia, Georgia, Guam, Nevada, Newfoundland and Labrador, and Prince Edward Island. At the time of this writing, these jurisdictions were set to begin requiring the EPPP (Part 2 – Skills) beginning in late 2020. In addition, beginning in early 2021, Manitoba will also become an early adopter of EPPP (Part 2 – Skills).
Importantly, the EPPP (Part 2 – Skills) cannot be taken without prior passing of the EPPP (Part 1 – Knowledge). The format of the exam is as follows: there are 130 scored questions with an additional 40 unscored questions. Test-takers are given 4 hours and 15 minutes to complete the exam. The test includes three formats for asking questions: 45 percent are traditional multiple-choice or multiple-response items, 45 percent are scenario-based questions, and 15 percent are identified as “Other Item Types.” ASPPB describes the scenario-based questions as giving the test-taker a clinical scenario with up to five questions based on this scenario. There are up to three different scenarios given to a test-taker. Two other types of question types are described by ASPBB: Point and Click, and Drag and Drop. Point and Click show test-takers a picture and are asked to identify the correct aspect of the image requested. Drag and Drop questions ask the test-taker to match multiple pieces of information to corresponding information on the other side of the screen.
Like the EPPP (Part 1 – Knowledge), the EPPP (Part 2 – Skills) covers a broad range of domains, subdomains, and sub-subdomains. A full explanation is available from ASPPB’s website (www.asppb.net), but major domains and subdomains of EPPP (Part 2 – Skills) are summarized below with their content percentage as well:
Assessment and Intervention (33 percent): Knowledge of (a) application of diversity to assessment, (b) clinical interviewing, (c) test administration, (d) data integration, (e) diagnostic formulation, (f) intervention selection, (g) modifying interventions.
Ethical Practice (17 percent): Knowledge of (a) practice of ethics, standards, and legal statues; (b) appropriate documentation; (c) ethical practice management.
Collaboration, Consultation, and Supervision (17 percent): Knowledge of (a) working within systems, (b) collaboration, (c) interdisciplinary work, (d) program evaluation, (e) supervisee management, (f) promotion of healthy work environment.
Relational Competence (16 percent): Knowledge of (a) applying research on social context, (b) working with groups and organizations, (c) respect for others, (d) managing professional conflicts.
Professionalism (11 percent): Knowledge of (a) boundaries of competence, (b) self-assessment and feedback.
Scientific Orientation (6 percent): Knowledge of (a) conducting a literature review, (b) proper dissemination of research knowledge.
4.3 Studying and Preparing For the EPPP (Parts 1 and 2)
Regardless of how you performed in graduate school, the EPPP is an examination that requires preparation, review, and practice. Many senior psychologists will candidly remark that, despite their experience and proficient knowledge of psychology, they would have a difficult time passing the EPPP were they to take it today. Yet, the majority of doctoral-level examinees do receive a passing score on the exam. Success on the EPPP will result from many of the same factors relied on in graduate school: a combination of preparation, knowledge, and anxiety management.
If you speak with others who have taken the EPPP, you will hear a variety of strategies to help prepare you for the EPPP. Perhaps the most focused and helpful of strategies are the EPPP study kits/programs often advertised on psychology publications such as the APA Monitor. For years, the two most common and popular programs have been available from the Association for Advanced Training in The Behavioral Sciences (www.aatbs.com) and Academic Review (www.academicreview.com). Both programs offer comprehensive multivolume home study programs with analysis of content areas, full-length practice exams modeled after EPPP exams, multivolume audio programs, computer review programs, live workshops, and other study aids designed to prepare you for the EPPP. Prices are relatively expensive, although different price levels are available and many will argue that the benefits of the program are priceless. Both programs are comparable in effectiveness and reputation.
Perhaps the most integral components of these programs are also the most inexpensive to obtain; that is, the books and practice exams. The designers of the programs do an impressive job of condensing several years of psychology graduate school into books designed purely for study and review. Some academics may bristle at the notion of creating Cliff Notes versions of graduate school in psychology; however, the comparison fits and fits well. Your old textbooks were not designed to be reviewed as efficiently as these books were. The audio files offer another mode of ingesting large amounts of information, particularly in times in which you would otherwise be doing very little, such as commuting or exercising.
The practice exams, probably beyond anything else, are the most integral tool you can use to prepare you for the EPPP. Both AATBS and Academic Review offer over half a dozen full-length practice exams modeled after the EPPP and provided with detailed explanations for each answer. Sample items from former EPPP exams are also available through ASPPB and are quite helpful. There are a few benefits of the practice exams. First, you become more familiar with the often vague or cumbersome manner in which some EPPP items are presented. Second, you can continually monitor which content areas you understand with proficiency, and in which content areas you are under-performing. Continued administration of the practice exams provides you with opportunities to learn from items answered incorrectly. Finally, practice exams demystify the EPPP and condition you to the timing and fatigue variables and facilitate development of better test-taking strategies. ASPPB also offers practice exams, administered at the same Prometric testing centers as the actual EPPP, under similar conditions as the EPPP. The Practice EPPP exams (PEPPPO and PEPPPO2) are available for a fee by going to www.asppb.net/page/Practiceexinfo/.
If you have completed a doctoral program in psychology, then you likely know what study strategies work best for you. Some people prefer to study individually; others prefer to study in groups. Your colleague may prefer to use flash cards, while you never have. Nevertheless, it is best to avoid comparing your progress to that of others preparing for the EPPP; every person is different and you need to focus on the strategy that works for you. Regardless of what that strategy is, you should set aside several months of progressively intensive study to be adequately prepared for the EPPP. Some have suggested 300–400 hours of study time, although that would depend on your study habits. A sample study schedule is provided in Table 18.2.
Table 18.2 Studying for the EPPP
Sample study schedule for a 6-month study plan
Additional Suggestions
|
It is unknown what study materials will be needed to prepare for the EPPP (Part 2 – Skills). The ASPPB website contains a video tutorial on their website as well as sample questions in their EPPP candidate handbook. At the time of this writing, it does not appear that AATBS, Academic Review, or other study preparation companies have study packages specifically available for studying for the EPPP (Part 2 – Skills), but that will most likely change.
Perhaps your best measure of your level of readiness will be reflected in your performance on the practice exams. Because of this, it is a good idea to take an initial practice exam at least 6 months in advance of your planned EPPP administration date. Both AATBS and Academic Review study programs should provide corresponding content areas for each question, which allows you to calculate percentage scores for each of the eight content areas. For example, you may find you scored 40 percent of the Treatment/Intervention questions, 51 percent of the Assessment and Diagnosis questions, and so on. Do not be alarmed if your performance on the first practice exam is poorer than you expected. Keeping track of your performance on the eight content areas serves to inform you of the areas on which you need to focus your studies. It also provides you with a barometer of your progress over time. It is a good idea to take at least one, if not two, practice exams per month. It is ideal to be scoring above the 75 percent range overall by the time you are preparing to take the EPPP. As you review your scores, take note that the practice tests in both study kits are often more difficult than the EPPP itself. Although it is unlikely you will ever feel completely comfortable and confident, you should feel relatively prepared by the time you are ready to take the EPPP.
5. After Licensure: Banking Your Credentials
Assuming you have successfully completed all of the requirements for licensure and have obtained your professional license to practice psychology, you should consider banking your credentials (see Table 18.3). This usually involves the process of submitting and verifying documentation to a centralized credentials “bank” for your education/coursework, practica, internship, doctoral degree, post-doctoral training, EPPP scores, license, and other credentials. This can be very helpful and time-saving in the future as you apply for insurance or managed-care panels, jobs, or other credentials. ASPPB offers a Credentials Bank program, which allows you to electronically store your transcripts, exam scores, and documentation of training experience so that it can be sent as needed to future licensing boards. As mentioned, you may find yourself changing jobs and location sometime in the future, whether in the next few years or decades from now. Organizing and submitting documentation can be difficult enough; it can become increasingly difficult years later after supervisors retire, programs modify or close, and addresses change. The Credentials Bank provides a readily accessible archive for necessary licensure documentation. There is an initial fee to set up the record, and then a maintenance fee every 2 years to keep the record available.
Table 18.3 To-do list after obtaining a license
Upon Licensure
|
In an effort to streamline the mobility of licensure from state to state, ASPPB also developed the Certificate of Professional Qualification in Psychology (CPQ). The CPQ is a credential given to applicants who meet certain eligibility requirements (similar to most licensure requirements), have practiced for a minimum of 5 years, and have no record of disciplinary action. ASPPB recommends to licensing boards that the CPQ be accepted as a sign of eligibility for licensure. At the time of this writing, 43 jurisdictions accept the CPQ as evidence of eligibility for licensure and several others are in the process of accepting or recognizing the CPQ.
The National Register of Health Service Providers in Psychology also provides the opportunity for credential banking. There are similar eligibility requirements, although once listed in the National Register there are additional benefits, such as verifying credentials for applications to insurance panels and the American Board of Professional Psychology (ABPP). The National Register is available at www.nationalregister.org.
Some states, provinces, and territories will allow an applicant to be “license eligible” if they hold the CPQ, National Register, or ABPP. You would usually only need to take and pass the written or oral local examination, if required, to be licensed in that jurisdiction. Some jurisdictions will also require a certain number of continuing education hours per number of years to maintain licensure.
Throughout the process, obtaining a license can be a difficult, challenging, and even frustrating task. Yet, for the practicing psychologist, it is the most important credential you will ever acquire.
6. Additional Resources
6.1 Websites
www.asppb.net – Association of State and Provincial Psychology Boards
www.aatbs.com – Association for Advanced Training in the Behavioral Sciences
www.academicreview.com – Academic Review
www.nationalregister.org – National Register of Health Service Providers in Psychology
www.prometric.com – Prometric Testing Centers
The focus of this chapter is to help you understand specialty board certification in psychology. Just as medicine and many other professions embrace the recognition of specialty skills, psychology does as well. Indeed, although relatively few psychologists are board certified as compared to physicians, the recognition of the need for specialization and board certification has grown significantly in recent years (Reference Robiner, Dixon, Miner and HongRobiner et al., 2012). Within psychology, board certification through the American Board of Professional Psychology (ABPP) is recognized as the “gold standard” and is virtually synonymous with what is being referred to when board certification is referenced in the profession (Reference Nezu, Finch and SimonNezu et al., 2009). Unlike licensure, which is required to practice and is general in scope, board certification is generally a voluntary process that is completed after earning a doctorate, completing internship and a license to practice (Reference Cox and GrusCox & Grus, 2019). It is a means of demonstrating competency in a specialty area of psychology by which the public and profession alike can know that one is competent to practice in one of the many specialties in psychology (Reference CoxCox, 2010; Reference Cox and GrusCox & Grus, 2019).
Within this context, this chapter will (1) cover a brief history of specialization and board certification in the field of psychology, (2) describe some of the benefits and advantages of becoming board certified, (3) describe the board certification process, and (4) debunk some myths regarding board certification. Hopefully, this all helps to provide some information about how and why to pursue board certification in your chosen specialty area.
If you are a graduate student (or perhaps an undergraduate student) who knows you want to become a psychologist, yet may not know what specialty area you wish to pursue, becoming familiar with the concept of specialties and related requirements is advisable as early as is feasible in your professional development. Don’t think, “That is years away, I don’t need to learn it now.” On the contrary, knowing about the specialty areas and requirements will help you plan and, more importantly, avoid missteps as you develop professionally. Little can be more disappointing than to spend years preparing to practice in a specialty area yet discover all too late that you failed to meet a particular requirement. Becoming familiar with the process and applying as early as during graduate school (this will be described later) can facilitate successful completion of the process. Early engagement includes not only learning about board certification and what is required, but also why it is important to you, potential employers, the profession, and the public that we serve. Many psychologists that have gone through the process describe it as having been a growth experience and a means of assuring themselves and others that they are engaged in practice that is focused on competent, high-quality work.
No doubt at various places within this book you will read about the increasing number of people entering psychology, increased interest in providing specialized services, the vast amount of information to learn in the field, and emerging areas of practice that have been developing in recent years. Much of this is directly reflected in the growth of specialties in psychology and the member boards of ABPP. Having started with 3 specialty boards, ABPP includes (at the time of this writing) 15 specialty boards, one subspecialty board, and has two additional specialties and another subspecialty in the process of affiliating as new member boards. Applications to ABPP have doubled in the last decade and now approach 1000 per year.
By way of background to provide you this information, my experience with ABPP is a long one. I was asked, as an active member of the Division of Rehabilitation Psychology of the American Psychological Association, to volunteer to serve on a committee exploring the need and demand for board certification in Rehabilitation Psychology. That ultimately led to establishing the examination process. That work began in 1993; the American Board of Professional Psychology (ABRP) came to fruition and formally affiliated with ABPP in 1997. At that time, I had worked in academic medical centers and hospital-based practices as well as private practice. In 2006, I was hired as the Executive Officer of ABPP. I continue to serve as the organization’s first full-time Executive Officer to this date. So, I have been associated with ABPP in some capacity for 27 years. Through all of this I have become quite familiar with each of the specialty areas, the specialty examining boards and a multitude of boards, committees, and organizations with psychology.
Work in the profession regarding specialization is ongoing and has seen strong support in recent years with several “summits” held to address specialty. A highlight for me of this continuing work has been co-facilitating the Interorganizational Summit on Specialty, Specialization, and Board Certification along with leaders of the Council of Specialties in Professional Psychology (CoS) and the Association of State & Provincial Psychology Boards (ASPPB). The four summits that we have held to date (the fifth is in the planning stages) have brought together roughly 30 of the most important boards and organizations within psychology with virtual unanimous agreement that the profession needs to emphasize the importance of specialty education, training and practice within which board certification is a natural, if not expected, step in professional development. These recent developments speak to the growing importance of specialty, board certification, and ABPP in the evolution of professional psychology.
ABPP is increasingly representative of the standards of competence for specialty practice, beyond that required of the generic licensing process. ABPP board certification is to psychology as specialty certification is within medicine, dentistry, law, and other professions. Moreover, you can initiate your application and begin familiarizing yourself with the requirements while early on in your career; I strongly encourage you to do so!
1. A Brief History of Specialization and Board Certification
Board certification of psychologists has a long history that continues to develop. ABPP began in 1947 when there was a desire to establish a means whereby the profession could identify those psychologists that were competent to provide clinical treatment (as opposed to conduct research, for example). Initially, 3 specialty areas were established; that has grown to the current 15 and growing. Comprehensive descriptions of the evolution of specialty and ABPP can be found elsewhere (Reference Baker, Cox, Johnson and KaslowBaker & Cox, 2014; Reference Bent, Packard and GoldbergBent et al., 1999).
In short, the profession evolved to the point of licensure. However, licensing of psychologists addresses education, training, and experience, and one’s ability to pass a knowledge-based test; it does not examine actual competence through review of one’s work as does the board certification process (Reference Cox and GrusCox & Grus, 2019). Psychologists that provide health care services to the public are expected be licensed by the state or jurisdiction in which they practice (with a relatively few exceptions for those working in “exempt agencies”). Licensing of psychologists is based on the broad and general aspects of applied psychology and is generic. Licensed psychologists are to ethically practice only in those areas that are within the scope of their education, training, and experience (APA, 2017). This leaves a fair amount of potential uncertainty in determining those psychologists that are competent to practice in a specialty. Consumers may be confused when trying to find an appropriate specialty provider if relying solely on licensed, non-board-certified individuals.
Specialization has become increasingly important as knowledge and information in the field increases. What you need to know in a specialty area may well double every 7–8 years (Reference Neimeyer, Taylor and RozenskyNeimeyer et al., 2012, Reference Neimeyer, Taylor, Rozensky and Cox2014). Most health care professions provide a peer-review process for the credentialing and board certification of individuals that provide health care services to the general public.
Specialty areas in psychology (Table 19.1) have a formal means whereby they are recognized (APA, 2011b). Representatives of the CoS, Commission on Accreditation (CoA), Commission for the Recognition of Specialties and Subspecialties in Professional Psychology (CRSSPP; formerly the Commission for the Recognition of Specialties and Proficiencies in Professional Psychology – CRSPPP), and the American Board of Professional Psychology (ABPP) agreed upon and adopted a definition of “specialty” that was acceptable to each of the groups (APA, 2020, p. 23):
|
A specialty is a defined area of professional psychology practice characterized by a distinctive configuration of competent services for specified problems and populations. Practice in a specialty requires advanced knowledge and skills acquired through an organized sequence of education and training in addition to the broad and general education and core scientific and professional foundations acquired through an APA or CPA accredited doctoral program.* Specialty training may be acquired either at the doctoral or postdoctoral level as defined by the specialty.
*Except where APA or CPA program accreditation does not exist for that area of professional psychology.
Board certification within a specialty area is not a requirement of licensing boards in psychology; in fact, most licensing boards do not recognize specialty practice at all. As with so many other professions, our field has grown in size, scope, and amount of information needed to competently practice. Reference RobertsRoberts (2006) wrote about the “essential tension” between specialization and “broad and general training” as has typically been referenced in psychology. Is psychology a singular field or a profession made up of a variety of specialty areas? Specialization is an “inevitable and necessary product of developmental processes in a discipline and a profession” (Reference RobertsRoberts, 2006, p. 863). Specialty board certification of psychologists is not required but is a voluntary process within the profession of psychology, overseen by the American Board of Professional Psychology (ABPP). Board certification through ABPP is considered by most psychologists as an advanced recognition of skills, knowledge and competencies (Table 19.2) and continues to be the expected credential for those that hold themselves out as a specialist.
| Foundational competencies | Functional competencies |
|---|---|
| Professionalism | Assessment |
| Reflective Practice/Self-Assessment/Self-Care | Intervention |
| Scientific Knowledge and Methods | Consultation |
| Relationships | Research/EvaluationFootnote * |
| Individual and Cultural Diversity | SupervisionFootnote * |
| Ethical Legal Standards and Policy | TeachingFootnote * |
| Interdisciplinary systems | Management-AdministrationFootnote * |
| Evidence-based Practice | AdvocacyFootnote * |
* May not be applicable to all practitioners
At this point, there is general consensus within the profession that while broad and general training remains an essential aspect of psychology education and training, specialty is where we are headed (witness the Interorganizational Summit information above and other descriptors at www.cosppp.org for more information). Clinical neuropsychology is an example of a specialty within psychology that has done a terrific job of enculturating those interested in the area, embracing board certification (Reference CoxCox, 2010). Success in such enculturation is likely associated with the clear articulation of training and education requirements within a specialty via such means as using what has become referred to colloquially as the “Psychology Taxonomy” (APA, 2012).
Most of us are aware of board certification of physicians in various specialties, yet specialty certification in psychology has grown more slowly. The American Board of Medical Specialties (ABMS) was founded in 1933, the American Board of Professional Psychology (ABPP) in 1947. Probably due to the significant reliance on board certification as a means for qualifying for medical staff privileges in medicine, that profession’s certification process has grown more widespread and become enculturated into the medical profession’s education and training process. Psychology, with less presence in hospital and medical settings, has done so more slowly. However, a recent series of profession-wide meetings – the Interorganizational Summits on Specialty, Specialization, and Board Certification among them – has resulted in a consensus that the field of psychology needs to integrate specialization and board certification much more into our education and training process than has been the case historically (Reference Silberbogen, Aosved, Cross, Cox and FellemanSilberbogen et al., 2018). That work continues and planning for “Summit 5.0” (the fifth such summit) is underway as of this writing.
2. Requirements for Becoming Board Certified
It used to be that in order to even apply for ABPP board certification one must have been five years out from receiving one’s doctoral degree. An increased focus on standardization and competency-based education and training led to earlier adoption of specialization of practice for many psychologists; this has also included an increase in number of specialty postdoctoral training programs (Reference Rodolfa, Bent, Eisman, Nelson, Rehm and RitchieRodolfa et al., 2005; Reference Silberbogen, Aosved, Cross, Cox and FellemanSilberbogen et al., 2018). Board certification is a natural next step after specialized post-doctoral training. There seems to be increasing momentum regarding competency-based education, training, and board certification (Reference Kaslow, Graves and SmithKaslow et al., 2012). Recognizing board certification as one of the goals of professional training and development, ABPP started the Early Entry Program in 2007 in an effort to reach students early in training and facilitate understanding and acceptance of board certification within psychology.
The Early Entry Program (or Early Entry Option) has been extraordinarily successful and nearly 60 percent of ABPP applicants now come through that program (Reference Edgar, Holder, Cox and SurisEdgar et al., 2019). Many education and training programs are encouraging and/or sponsoring students, interns, and post-doctoral residents to participate. Becoming familiar with the process and expectations of board certification early permits one to potentially join discussion groups, identify a mentor for the process and start integrating an identity as a specialist-in-training. Basic in its design, the program allows students, interns and post-doctoral residents to apply to ABPP, file credentials and documents as they complete each step of education and training, and eventually be ready for the formal board certification process. The program does not create any exception to the standard credentials review or examination process, but does provide for a discounted application. All other requirements for ABPP board certification remain the same; the Early Entry Program is not an “easier” path, unless one accepts familiarity with the process as making it “easier.”
Becoming board-certified through ABPP includes multiple steps: credentials review, submission of practice samples, and oral examination. The process is similar for every ABPP specialty board. A written (e.g., multiple-choice) examination is also included in the process for two specialty boards: Forensic Psychology and Clinical Neuropsychology.
ABPP has what are called Generic Requirements that are the same for each specialty board. Beyond that, each specialty has its own specialty-specific requirements. The generic and specialty-specific requirements are available online at www.abpp.org. The generic requirements (for those individuals trained in the USA and graduating from a doctoral program in 2018 or later) include a doctorate in psychology from an APA-accredited program, completion of an APA-accredited internship (if the internship is completed in 2020 or later), and licensure in at least one state at the doctoral level for the independent practice of psychology. There are slight variations of these requirements for those trained earlier and/or outside of the USA.
An application that meets the requirements of the generic review is passed on to the specialty board to review the specialty-specific requirements. Specialty-specific requirements are in addition to the ABPP generic requirements; meeting the generic requirements for ABPP is a pre-requisite for review by a specialty board. An example of specialty-specific requirements might be completion of post-doctoral training in the specialty and/or completion of coursework or training in that area of practice. Completion of a formal residency program and/or supervised experience may satisfy some or all of the specialty-specific requirements; it is always best to review the specialty board’s information on the ABPP website for up-to-date information.
Once one’s credentials have been approved by the ABPP Central Office at the generic level and also by the specialty board, most applicants will be requested to submit practice samples; the two exceptions to this are for those applying in Clinical Neuropsychology and Forensic Psychology, each of which require a multiple-choice written examination first. Practice samples are often video recordings of working with a client and/or providing supervision, or written descriptions of one’s work. The specifics vary somewhat from board to board and should be accessed via the ABPP website. Two case presentations or other samples of one’s work along with a personal professional statement are common types of written practice samples. It is understood that different clinical or employment settings or roles might affect the types of cases or materials. An overview of the practice sample submission process (Reference Davidson, Nezu, Finch and SimonDavidson, 2009) and other stages of the process can be found in Reference Nezu, Finch and SimonNezu et al. (2009).
Each specialty board requires an oral examination of approximately 3 hours. The process is expected to be collegial throughout; it is not uncommon to hear that the process was engaging and challenging, yet friendly. The format or model of the oral examination is different across boards, with some being conducted with the examinee meeting with three examiners at once, and others having the examinee spend portions of the time with different examiners. Whatever model is used, the goal is always to assess the competency of the candidate.
The oral examination is most often based in part on the practice sample(s) submitted, and may also include responding to vignettes, fact-finding about cases, or other methods of inquiry. Every specialty board oral examination must also cover legal and ethical issues. That may be examined using the submitted practice sample, or the use of vignettes provided in the examination. The oral examination is an opportunity for a candidate to “think on one’s feet” and demonstrate an ability to conceptualize a case and demonstrate competence in the ability to diagnose and/or discuss a treatment plan. Candidates will need to be prepared to discuss the practice samples in detail, present a solid rationale for what was done in the case as well as how it was done. The candidate should be prepared to demonstrate that one is up to date with relevant literature (Reference Kaslow, Nezu, Finch and SimonKaslow, 2009).
The entirety of the ABPP board certification process is based largely on the concept of professional competency (Reference Rodolfa, Bent, Eisman, Nelson, Rehm and RitchieRodolfa et al., 2005) and the Foundational and Functional Competencies recognized in professional psychology (American Psychological Association, 2011a; Reference Fouad, Grus, Hatcher, Kaslow, Hutchings, Madson, Collins and CrossmanFouad et al., 2009; Reference KaslowKaslow, 2004, Reference Kaslow, Nezu, Finch and Simon2009). These are widely integrated into graduate study and used throughout the education and training experiences in the profession.
3. Myth-Busting
Over the years, some misinformation, misunderstanding, and myths circulated and developed that I would like to debunk. I recall hearing of some of these many years ago when I was entering the field, and some have persisted.
First, ABPP board certification is not just for the “best of the best” or the “cream of the crop” of the “top 2 percent” of psychologists. This myth may have spread and persisted because only a small percentage of psychologists have historically become board-certified. However, with the advent of the Early Entry Program and dissemination of information clarifying that ABPP expects that most appropriately trained psychologists should expect that they can pass the board certification examination. Indeed, we tend to say that psychologists that are 2–3 years post-doctoral degree are likely to be able to pass and psychologists with 10 or fewer years of experience pass at a rate like those who have been practicing longer (Reference Edgar, Holder, Cox and SurisEdgar et al., 2019). That time frame permits for an appropriate, yet not overly lengthy, period of post-doctoral supervised experience; of course, that experience would need to be in the specialty area in which one is anticipating becoming board-certified.
Another myth that persists, and one that is directly related to the above, is that the examination process is grueling and really for academics. The truth is that although the examination is not a “walk in the park” it is based on the very training that one has been undertaking in the years prior to examination. The process is collegial and not adversarial. Many, perhaps even most, board-certified psychologists focus on clinical care and a good percentage are in independent practice. Indeed, the examination process is about clinical practice, not academic psychology.
Finally, some feel that nothing beyond licensure is necessary. Certainly, one must (with very few exceptions) be licensed to practice in the field, and board certification is voluntary. As has been described earlier in this chapter, the notion that one need not demonstrate competence beyond licensure is becoming increasingly unacceptable in the profession as well as with the public (Reference Cox and GrusCox & Grus, 2019). The ABPP board certification examination is the single best way of demonstrating to the public, profession, and yourself that you practice at the expected level of a specialist in a particular area.
The ABPP certification process requires extensive but manageable requirements. Preparation for the board certification process from ABPP includes:
The chance to articulate your own views and perspectives in a more advanced and sophisticated way as part of the preparation and oral exam
A structure to facilitate self-assessment where the individual gets to set his or her own pace in developing their case study, which facilitates better self-understanding and case conceptualization
An important continuing professional education opportunity (fulfills, in some states, the continuing education (CE) requirements for the biennium in which board certification occurs; those successful receive CE credits from ABPP, an APA approved CE provider)
More mobility opportunities as many state licensure boards recognize the ABPP and have a facilitated licensing process
Highest credential for a psychologist and denotes an advanced level of competence (knowledge, skills, attitudes, and competencies)
“Final examination” that gives legitimacy to the profession, along with public confidence one gets when being referred to as a board-certified specialist
Assurance to the public you are a specialist that has successfully completed the educational, training, and experience requirements of the specialty, including an examination designed to assess the competencies required to provide quality services in that specialty
A credential that is understood by other professionals and the public
(The above points were taken from a presentation at the APPIC 2007 Conference in Reference Baker and KaslowBaker, J. and Kaslow, N. (2007), “Board Certification for Internship Training Directors”.)
4. In Closing
Specialization in psychology is increasingly becoming important in the profession and gaining more widespread acceptance. In some segments of the profession, it is expected that you will be, or will soon become, board certified. This is particularly true for those of us who work in, or with, hospitals and medical centers, yet it is certainly not limited to those arenas. The public is becoming more aware of the need for expertise and look for board certification. You would likely seek a board-certified neurosurgeon if you needed brain surgery. Similarly, it follows that a specialist in psychology would be expected to be board certified. Rozensky predicts that psychology as a profession is needing specialization and that to be accepted in health care arenas, psychologists as individual professionals will want board certification.
I hope that the “take-away” from this chapter is that board certification is growing and important in our profession. Starting early is well-advised, and you can be successful in achieving board certification in the specialty for which you train. Good luck as you progress!
If you are in a professional psychology training program, it is likely that you will be asked to be a clinical supervisor at some point in your career. In fact, based on an extensive survey of the members of the American Psychological Association (APA) division that represents clinical psychologists (Division 12; Society of Clinical Psychology), it was determined that clinical supervision is provided by 55 percent of university professors, 71 percent of hospital psychologists, and 36 percent of independent practitioners (Reference Norcross, Karpiak and SantoroNorcross et al., 2005). For many of you, this is an eagerly anticipated activity, and for others, it may be a source of some uncertainty or even anxiety. The purpose of this chapter is to demystify the idea of becoming a supervisor by providing broad theoretical models for conceptualizing the practice of supervision and practical suggestions to guide you through the process of learning to be a supervisor. We will also discuss current competency-based supervision practice and provide suggestions for how to incorporate ethical and multicultural considerations into supervision. Throughout the chapter, we will include the perspectives of an experienced clinical supervisor (E.H.W.) and the perspectives of the second author (E.F.C.) from when she was an advanced graduate student just starting her journey toward becoming a competent supervisor. In this way, we aim to provide you with different perspectives on this learning process.
Most graduate students and interns see learning to supervise as a critical and expected step in their professional development. In fact, the expectation that you will attain a reasonable level of competency in supervision prior to completing your training is now integrated in a step-wise fashion into the accreditation standards for doctoral programs and internships. Doctoral students are expected to “demonstrate knowledge of supervision models and practices,” while interns are expected to “apply this knowledge in direct or simulated practice with psychology trainees, or other health professionals … examples … include, but are not limited to, role-played supervision with others, and peer supervision with other trainees” (APA Commission on Accreditation, 2015). This means that most of you, in addition to being supervised in your training programs and internships, will also be starting the process of learning to supervise others. What is it that you will be learning to do in supervision training? Let’s turn next to defining supervision and providing a broader context for this activity.
1. Defining Supervision
Despite the fact that most of us know what supervision is and what it means to be a supervisor, the terms can be surprisingly difficult to define in a comprehensive manner. A classic and broadly accepted definition is provided here:
Supervision is an intervention provided by a more senior member of a profession to a more junior colleague or colleagues who typically (but not always) are members of that same profession. This relationship is evaluative and hierarchical, extends over time, and has the simultaneous purposes of enhancing the professional functioning of the more junior person(s); monitoring the quality of professional services offered to the clients that she, he, or they see; and serving as a gatekeeper for the particular profession the supervisee seeks to enter.
Let’s walk through this definition because the elements capture the central functions of supervision (from the Latin for oversight) in contemporary professional psychology. In the first sentence of the definition, it is stated that supervision is an intervention. What does this mean? The notion that supervision is an intervention in its own right is somewhat counterintuitive. It is interesting to note that the term is derived from the Latin word intervenire or inter (between) venire (come); to come between. In our field, psychological interventions are, at their essence, intended to alter a negative course or process in order to improve psychological functioning. If supervision is an intervention, then it is attempting to come between or alter the behavior of the person in training who is, in turn, attempting to intervene with the client. If supervision is itself a complex and multifaceted process, then it is clear that teaching someone to be a supervisor is even more so. In terms of overarching goals, we are attempting to improve the skills of the supervisor-in-training, improve the clinical skills of the supervisee (usually a less-advanced practicum student), and improve treatment outcomes for the client; that is, we are attempting to intervene on multiple levels. As we will discuss later in this chapter, these levels of interweaving goals and responsibilities tend to become very complex. The definition provided above goes on to clarify that there is an ongoing and evaluative component to supervision that includes overseeing the quality of what is being provided to the clients and serving as a gatekeeper for the profession. This last statement reminds us that supervision is not only intended to ensure high-quality treatment for current clients, but for future clients as well. In training programs, it is common to differentiate between formative evaluations, which are designed to support the growth and development of the psychotherapy trainee, versus summative evaluations, which are designed to assess competencies, determine if adequate progress is being made, and provide a gatekeeping function for the academic program or internship site and the profession. It is clear that this classic definition of supervision quoted above incorporates the full range of these essential supervisory functions.
2. Taking on Your New Role
Becoming a clinical supervisor will involve several familiar roles that are merged into a new context. It will be subtly, but importantly, different from activities you have been exposed to, gained experience in, or mastered in your graduate training or personal life. In addition, you will likely have some key questions, and possibly some concerns, as you contemplate this new role: What will be expected of me? What if I have nothing to contribute? Should I focus on the supervisee or their client? It can be helpful to remember that new roles bring rewards as well as challenges. And, as mentioned above, you will indeed be able to draw from familiar roles. There are sophisticated theoretical and research analyses of the competencies and roles in supervision that you may find helpful to draw from as you begin your work as a clinical supervisor and refer back to as you become more experienced.
3. Social Role Discrimination, Developmental, and Theoretical Models of Supervision
You have likely already learned in multiple contexts that theories and models serve to organize complex experiences. The social role discrimination model explicitly describes the familiar roles that you will draw from in learning to be a supervisor. This model was initially developed by Reference BernardBernard (1979) and has been elaborated by Reference Bernard and GoodyearBernard and Goodyear (2014) in their classic text. In this model, both the role and the focus taken by the supervisor throughout the course of a supervision session are identified. As supervisors become more experienced, they are encouraged to more intentionally select the role that is enacted and the focus of the supervisory session that is selected. In this model, the three central roles that have been identified are: teacher, counselor and consultant. Here are some examples of the social roles that can be identified in supervision:
Teacher: In supervision, you may be teaching your supervisee very basic skills, such as how to schedule an appointment, complete consent forms, or complete progress notes. More complex skills might include learning how to take a detailed family history, conduct a suicide risk assessment, or introduce a mindfulness exercise. In cognitive-behavioral programs, supervisors will be teaching supervisees how to provide psycho-education to their clients regarding the interrelatedness of thoughts, feelings, and behaviors, how to collaboratively engage in a functional analysis, how to assign and analyze thought records, how to conduct behavioral activation, etc.
Counselor: In this role, a supervisor might process with the supervisee the experience of feeling more anxious about particular clients more so than others or how their own experiences might impact their interactions with a client who has a similar concern. A supervisor may also discuss various fears that the supervisee may have about beginning clinical work: What if my client replies to my questions with one-word answers? What if the client asks my age or if I am their first client? What do I do if I don’t know what to say? Will my client want to come back and see me again? It is useful to note that if you are a supervisor in training, these questions from an anxious supervisee seeing their first client might in turn make you a bit anxious in your new role as a supervisor. We will talk later in this chapter about the notion of parallel process.
Consultant: In the consultant role, the supervisor may push for the supervisee to trust their own insights about their work or challenge the supervisee to think or act on their own. For example, the supervisor might encourage the supervisee to explore and discuss complex case conceptualization issues and how these might impact the treatment plan or discuss how the client’s cultural background might necessitate altering an established evidence-based treatment, providing consultation rather than driving these discussions. This more collegial role has been identified as important, but not surprisingly, it tends to be more difficult to define or identify in both theoretical writing and in observational research.
In the social role discrimination model, the focus of supervision may be on intervention skills, conceptualization skills, or personalization skills. Some examples of each are provided below.
Intervention skills: What is the supervisee actually doing in the session? The focus may include an examination and discussion of how the supervisee implemented or plans to implement a particular intervention technique or how the supervisee reflected or summarized the client’s thoughts and emotions in the session. This may also include discussions of points in the session where the supervisee felt confident in responding, was not sure how to respond, felt that a particular intervention strategy did or did not go as intended or, more generally, had a sense that a session was or was not effective. After viewing or listening to the session, the supervisor may note points in the session related to the considerations described above and may have specific suggestions for modifying intervention strategies.
Conceptualization skills: How does the supervisee understand the client(s) and the presenting problem(s)? In supervision, the conceptualization focus might involve the supervisor and supervisee collaboratively discussing factors that contribute to the maintenance of the client’s difficulties, such as avoidance, maladaptive thinking patterns, or a lack of emotion regulation skills. Such conceptualization work may also involve the supervisee and supervisor thinking through the ways in which various background factors, such as cultural considerations, may impact the way in which the client is experiencing his or her present difficulties.
Personalization skills: How does the supervisee blend or interface their personal style with the therapy that is being provided? This may involve the supervisor and supervisee discussing how the supervisee interacts with clients: What is the supervisee’s tone of voice like? How does the supervisee’s style change (or not) with various clients or with a client’s different affective presentations? How much is the supervisee versus the client talking in session? Generally, this skill involves the supervisor working with the supervisee to learn when and how they may want to adapt their natural therapeutic tendencies for a particular client or client presentation. As with the consultation social role discussed above, this factor is clearly important, but is more difficult to clearly define or identify in a supervision session.
The 3 × 3 table of the social role discrimination model of supervision provides a useful structure for engaging in a sophisticated process and content analysis of treatment. We encourage you to consider each of the cells as you read the rest of this chapter and to use it as a guide if you are currently learning to be a supervisor or if you are in supervision yourself. Becoming more aware of the social roles and foci we are most drawn to can help us to assess whether we are taking an approach that is well matched to the needs of the supervisee and their client.
In addition to the social role discrimination model described above, there are complex developmental models for understanding supervision. These models focus on the observation and description of common developmental pathways typically taken by the supervisor in training as they move through the learning process (Reference Bernard and GoodyearBernard & Goodyear, 2014). Some of these models have been extended beyond training and into professional practice. Most useful to consider here is that early in training, supervisors in training tend to prefer clearly articulated structure and may be most concerned about “doing it right.” This same conceptualization applies to a novice psychotherapy trainee. Therefore, we would expect that when you, as a supervisor in training, are supervising a novice graduate student therapist, you will spend relatively more time in the teacher role focusing on conceptualization and intervention skills. In parallel, the novice supervisor may want a bit more specific instruction regarding how to effectively provide supervision. As novice supervisors in training and therapists become more confident (and competent), they will likely spend more time in a consultative role and in the consideration of more complex conceptualization and personalization issues.
Theoretical models of supervision are based on psychotherapeutic models. Because many academic professional psychology programs now endorse a cognitive-behavioral therapy (CBT) model, we will briefly discuss how this model translates in to the practice of supervision.
Table 20.1 Reference BernardBernard’s (1979) 3 × 3 social role discrimination model
| Focus of supervision | Social roles | ||
|---|---|---|---|
| Teacher | Counselor | Consultant | |
| Intervention | |||
| Conceptualization | |||
| Personalization | |||
A supervisor using a CBT model would tend to work collaboratively with the trainee in supervision, would be likely to incorporate active agenda setting into the supervisory process, would identify and use role playing techniques to assist the trainee in learning new behaviors, and would be alert to dysfunctional thoughts, underlying beliefs, or schemas that might interfere with optimal functioning of the supervisee. Of course, because this is not psychotherapy, the focus remains on thoughts, feelings, and behaviors that are relevant to learning to be an effective therapist.
4. Parallel Process and Alliance in Supervision
Earlier in this chapter, we mentioned the notion of parallel process. What is this? This idea has its roots in psychodynamic theory and a full discussion is outside of the scope of this chapter. For our purposes, it is the recognition that some aspect of the psychotherapy process is being recreated or reenacted (in parallel) in the supervision. For example, a client may be dissatisfied with the psychotherapy and believes that it is not good enough or not sufficiently helping. For the client, this may reflect real problems in the treatment and could also reflect early experiences and associated core schemas in which caregivers or authority figures were not helpful, validating, or supportive. The first parallel might occur when the trainee comes to the supervisor in training and expresses dissatisfaction with the assistance that they are receiving for dealing with the challenging client. In supervision training, we add another level to this parallel process when the supervisor in training becomes anxious that they are not helping the psychotherapy trainee and experiences frustration that is then directed to the faculty supervisor. As mentioned earlier, the complexities quickly escalate in supervision training, and it can be helpful to identify parallel process when it is occurring. This can be a useful perspective to consider, even in the context of CBT and supervision that does not generally tend to focus on transference and countertransference issues.
The role that a positive working alliance has on supervision process and outcome has been extensively explored (Reference Bernard and GoodyearBernard & Goodyear, 2014; Reference Ladany, Ellis and FriedlanderLadany et al., 1999). Generally, the elements of alliance in both the psychotherapy and supervisory relationship are an agreement on goals and tasks in the context of a trusting (or bonded) relationship. The research regarding the importance of a positive working alliance is more clearly demonstrated in psychotherapy than it is in supervision, as supervision research often lags behind psychotherapy research in general (Reference Kühne, Maas, Wiesenthal and WeckKühne et al., 2019). However, there is general agreement that supervisees will disclose more in supervision and experience more satisfaction when there is a strong working alliance with the supervisor. We would therefore encourage the fostering of a relationship in which your supervisee will disclose subtle areas of concern or discomfort. The alliance is also critical to a consideration of multicultural factors in therapy and supervision. Some research in this area suggests that clinical supervision may indeed be associated with greater client symptom reduction (Reference Bambling, King, Raue, Schweitzer and LambertBambling et al., 2006), but more work is needed.
5. Ethical Considerations
Supervision and supervision training occurs within an ethical and legal context. While state laws vary, it is likely that supervision is addressed in the Psychology Practice Act in your state. In contrast, the APA Ethics Code (APA, 2017) applies to all of us and provides guidance and standards regarding the practice of clinical supervision. The major ethical issues related to clinical supervision include competence and client welfare, informed consent, supervisee rights, the relationship between supervisor and supervisee, and confidentiality. Standard 2 (Competence), 2.01 Boundaries of Competence (a) reminds us that “Psychologists provide services, teach, and conduct research with populations and in areas only within the boundaries of their competence, based on their education, training, supervised experience, consultation, study, or professional experience” (APA, 2017, p. 5). It is a good general rule to not supervise a psychological treatment or assessment that you, yourself, are not competent to provide. Similarly, a faculty supervisor should always be competent in the psychological service that is being provided in a supervision training context. This standard also relates to competence as a supervisor, which we will discuss in the next section. Standard 2.05 Delegation of Work to Others is interesting to consider as it relates to learning to be a supervisor: “Psychologists who delegate work to … supervisees … take reasonable steps to … authorize only those responsibilities that such persons can be expected to perform competently on the basis of their education, training, or experience … with the level of supervision being provided” (APA, 2017, p. 5, excerpted with emphasis added). What does this mean and why is it important? In both learning to be a therapist and a supervisor, if you were already fully competent, you would not need to learn how to do it and this chapter would not need to be written. The faculty or staff supervisors in your doctoral program or internship are responsible for ensuring that you have sufficient preparation and oversight to ensure competent service is being provided to the client and competent supervision to the less-advanced graduate student while you are learning. We like to consider this to be your learning edge, and it requires careful assessment and communication to ensure that the therapist or supervisor in training is challenged, but not overwhelmed. The ethical standards related to Informed Consent (10.01) remind trainees to inform clients that they are being supervised and to provide the name of the supervisor, when legal responsibility for the treatment resides with the supervisor. The Multiple Relationship standard (3.05) reminds us to be careful about potential conflicts in roles that could impair objectivity or judgment. Therefore, it is critical to inform the faculty supervisor if a personal relationship with the trainee might preclude you from providing effective supervision. This latter issue may be a common occurrence in doctoral programs and should be discussed directly. It is also important to remember that, as a supervisor in training, your interactions with the trainee are protected by educational confidentiality. Finally, Standard 7 (Education and Training) is important; we would encourage you to review it in its entirety as you begin your role as a supervisor in training. Standard 7.06 is so important that it is cited below its entirety:
7.06 Assessing Student and Supervisee Performance
(a) In academic and supervisory relationships, psychologists establish a timely and specific process for providing feedback to students and supervisees. Information regarding the process is provided to the student at the beginning of supervision.
(b) Psychologists evaluate students and supervisees on the basis of their actual performance on relevant and established program requirements. (APA, 2017, p. 10)
Faculty supervisors, supervisors in training, and training programs are jointly and mutually responsible for ensuring that evaluations occur as specified in the ethics code and in accordance with their program’s policies and procedures.
6. Multicultural Considerations and Competencies
Supervision training can be a bridge to incorporating the knowledge of multicultural and diversity issues that are learned in courses into clinical practice. In a survey of professional psychologists, it was determined that psychologists are more likely to be able to identify best multicultural practices than they are to endorse actually following these practices (Reference Hansen, Randazzo, Schwartz, Marshall, Kalis, Frazier, Burke, Kershner-Rice and NorvigHansen et al., 2006). In considering the implications for training programs, the authors recommend that in addition to typical multicultural training practices, supervisors might initiate “a frank discussion about why clinicians do not always do what they believe to be important. Identifying and openly discussing these barriers may improve the ability of practitioners to follow through when doing psychotherapy with clients who differ racially/ethnically from themselves” (Reference Hansen, Randazzo, Schwartz, Marshall, Kalis, Frazier, Burke, Kershner-Rice and NorvigHansen et al., 2006, p. 73). The authors recommend that multicultural training include a focus on the behaviors that psychologists endorse as being important but don’t practice. In this study, the five behaviors that were found to exhibit the largest discrepancies between what psychologists say they believe in and what they actually practice were: evaluating one’s multicultural competence, using culture-specific case consultation, making DSM IV cultural formulations and culture-specific diagnoses, and implementing a multicultural professional development plan. It is clear that supervision provides a key opportunity at many levels for you, as a supervisor in training, to assist the beginning therapist in the integration of multicultural concepts and competencies into clinical practice. In addition to ensuring that what is taught in multicultural courses is incorporated into practice, addressing barriers to the use of this knowledge is an important step in improving the multicultural competence of our profession in the future.
7. The Process of Learning to be a Supervisor
7.1 From the Perspective of Someone When She Was a Supervisor in Training (E.F.C.)
Learning to be a supervisor brought up many of the same feelings that I had when I was first learning to be a therapist: excitement, anxiety, and fear, among others. As I began this journey, I also found myself having similar thoughts to those that I had when I started with my first clients: Will what I’m saying make sense? Will this person leave the session feeling satisfied? Will I know how to respond to this person’s questions/comments? Do I really have anything to offer? Thus, in many ways, this process felt very similar to beginning my work as a therapist – I found myself having a wealth of mixed emotions, as well as a good deal of doubts and worries about my own abilities. However, just as we have familiar roles that we can draw on as we take on our new role as “therapist,” by the time we are ready to become supervisors, we have even more familiar (and likely more comfortable) roles that we are able draw upon (e.g., teacher, therapist). By the time you are a supervisor in training, you will have accumulated a wealth of graduate school experiences that have all likely prepared you for this new role in some way. Although it is probably natural to have some sense of the “imposter phenomenon” when taking on your new role as a supervisor (e.g., “Sometimes I’m not quite sure what to do with my own clients, and now I’m supposed to be guiding someone else in this process?!”), it is important to recognize all of the skills that you do have and that you can draw upon in this new role. For me, that was an extremely helpful thought “reframe” to keep in mind.
In my journey towards becoming a competent supervisor, I found “supervision of supervision” to be an incredibly helpful aspect of the learning process. Having the opportunity to bounce ideas off of an experienced supervisor with many years of experience was invaluable, as was drawing from some of my most positive supervision experiences. I often found myself thinking back to my early work as a therapist and what I found most helpful in supervision. What sorts of strategies did my most helpful supervisors employ with me? Thus, in learning to be a supervisor, keep in mind that not only do you have familiar roles that you can draw upon, but that you also have a good deal of experience as a “supervisee” yourself. Some specific suggestions (adapted and expanded from Reference NeufeldtNeufeldt, 1994) are presented in Table 20.2.
Table 20.2 Key strategies for supervisors in training in working with supervisees
7.2 From the Perspective of the Faculty Supervisor (E.H.W.)
I am going to keep my section short because most readers of this book are likely to be graduate students, interns, or early career psychologists. When we began to offer supervision training in our program, I was excited, but also daunted. In my own training, the ability to be an effective supervisor was assumed rather than taught. My first professional position was in a university psychological services center. As was common practice at the time, I was assigned practicum students, interns, and psychiatric residents to supervise with limited preparation in my own training for how to do so. Therefore, for me, as for many of my professional peers, there were no clear models for either how to be supervisors ourselves or for how to teach others to supervise. Over the years, I have adopted a model that includes formal elements (readings, regular meetings, and videotaping) and more informal discussion of the process and the experience. As described above in the section on parallel process, I have quickly learned that the responsibility for a client, a novice graduate student therapist, and an advanced graduate student supervisor can be complex – even when things are going well. I have found it useful to balance our consideration of the needs of all parties involved and to be sensitive to the alliance and parallel process at all levels. For faculty supervisors who are considering becoming involved in supervision training, I will share that, for me, the supervision of supervision in an academic doctoral program has been an immensely rewarding and energizing experience. It has provided me with an impetus to read the supervision literature and to be able to notice and articulate to someone else (hopefully with some coherence!) what it is that I do when I supervise. It has become a central and valued aspect of my own professional development. In fact, as another instance of parallel process, writing the original version of this chapter with someone who was an advanced graduate student at the time who was learning to supervise in our academic training clinic pushed me to crystallize my thinking about the process and to familiarize myself with the classic and current supervision literature. In terms of specific recommendations for faculty supervisors, I would encourage the incorporation of direct observation of the therapy sessions that are being supervised by the supervisor in training and, when possible, the direct observation of a supervisory session. It is interesting to note that a survey of internship training directors revealed a stronger consensus regarding supervision competencies than there is on effective training models or methods (Reference Rings, Genuchi, Hall, Angelo and CornishRings et al., 2009), suggesting that while there is theory and research to draw from, as a field we have not yet identified a specific and preferred training model for learning to be an ethical and competent supervisor. Hopefully this chapter will provide useful strategies for you to consider as you begin your training in this realm.








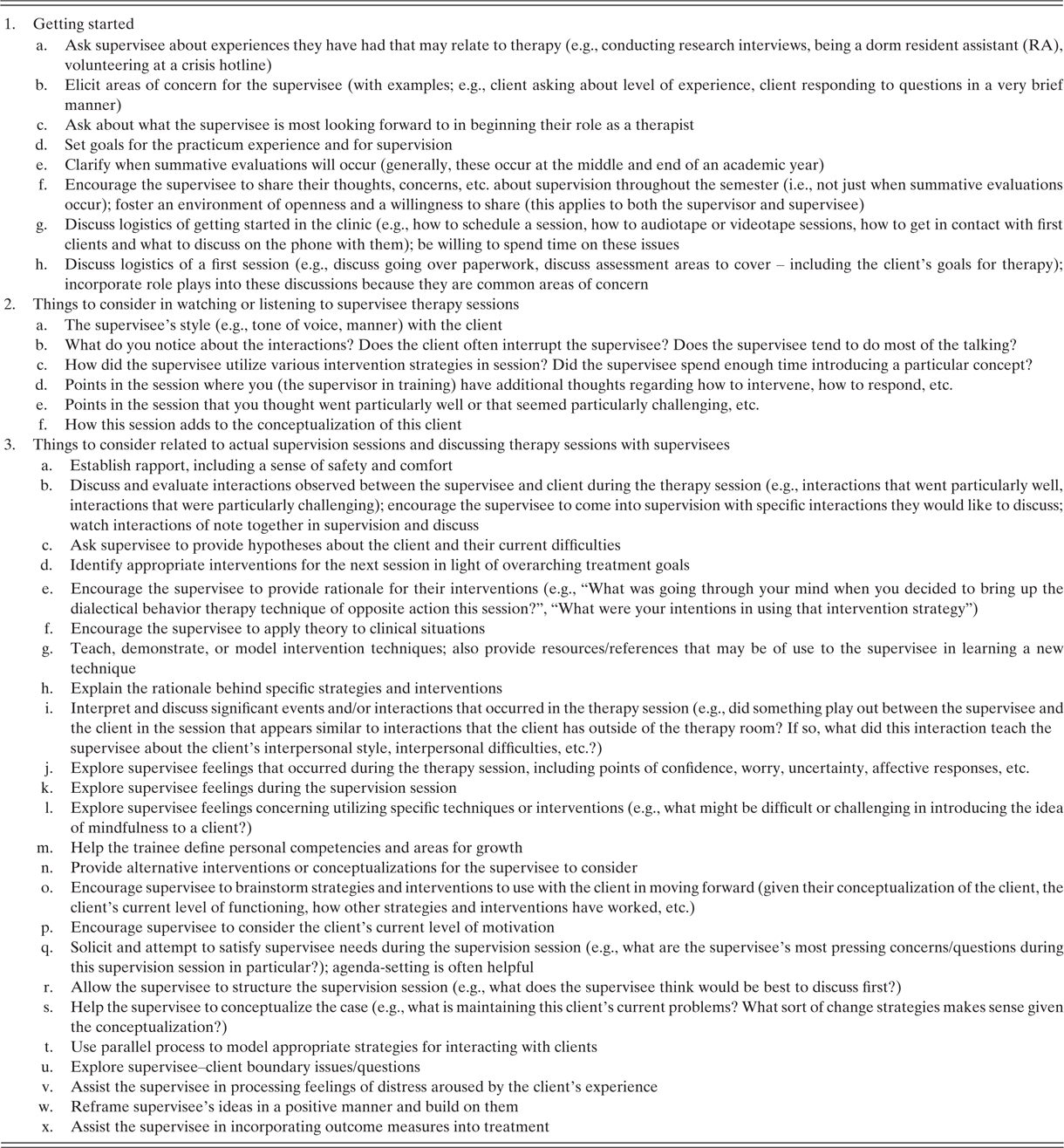

 Open access
Open access