

Introduction
Surgeons have long told stories about themselves and their history. As Christopher Lawrence has suggested, and as we shall see in this book, these stories often reveal more about the image that their tellers sought to project of themselves and their contemporaries than they do about the various mythical, half-remembered, and stereotyped pasts they invoked.Footnote 1 This tradition of storytelling, of historicising surgery in order to understand the present, had its roots in the writings of medieval surgeons such as Guy de Chauliac (c.1300–68), but, like historicism itself, it really came to prominence at the end of the eighteenth century and beginning of the nineteenth.Footnote 2 It was in this period, or so contemporary surgeons claimed, that surgery had become a fully fledged scientific discipline that had finally distinguished itself from its traditional associations with manual craft. This story had its institutional correlate in the split of the surgeons from the Barbers’ Company (1722 in Scotland, 1745 in England) followed by the creation of the Royal College of Surgeons of Edinburgh in 1778 and the Royal College of Surgeons of London (later England) in 1800. Indeed, it was within these new institutional structures that surgery’s mythical rebirth was most frequently, and most visibly, commemorated and rehearsed.
The first part of Emotions and Surgery is concerned, in large part, with exploring the professional cultures, identities, and ideologies of a generation of British surgeons that came of age in the very late eighteenth and early nineteenth centuries: a generation of Romantic surgeons. Perhaps the most prominent claim that this generation made for the transformation of their art in the fifty or so years prior to 1800 was its increasing scientific sophistication: the re-founding of surgical practice on the basis of sound anatomical knowledge, rather than mere empiricism. If the humanist surgeons of the sixteenth century had struggled to wrest learned surgery from the intellectual domain of the physician, then surgeons of the later eighteenth century had, it was claimed, made anatomical and physiological learning their own.Footnote 3 In fact, they had, to a significant degree, made medical knowledge their own. The eighteenth century produced a number of surgeons whom posterity would venerate as exemplars of this new-found theoretical and operative self-confidence. These included men such as William Cheselden (1688–1752) and Percivall Pott (1714–88).Footnote 4 However, by far the most iconic figure, and the man who, as Lawrence observes, would be ‘shaped into the “father of scientific surgery”’, was John Hunter.Footnote 5 It was Hunter whose name would, in 1813, be immortalised in the form of an annual oration at the Royal College of Surgeons of London, and it was his likeness, in the shape of Henry Weekes’ (1807–77) statue of 1864, that would take pride of place in the College’s Museum.Footnote 6 As Lawrence suggests, while English surgeons made Hunter their own, those in Scotland told a different story (somewhat ironically, given that Hunter was a Scot).Footnote 7 For Edinburgh chroniclers writing in the mid-nineteenth century, it was John Bell who was celebrated as ‘the best surgeon that Scotland had then produced’Footnote 8 and ‘the reformer of Surgery in Edinburgh, or rather the father of it’.Footnote 9 Indeed, the prowess of Scottish surgeons in the early to mid-nineteenth century, including the brothers John and Charles Bell, as well as Robert Liston and James Syme, allowed their contemporaries to imagine that Scottish surgery had initiated a revolution all of its own. Writing to his uncle from Edinburgh on New Year’s Day 1833, the young Cumbrian surgical pupil Andrew Whelpdale spoke of ‘the beauty of the modern School of Medicine in Edinbro [sic]’. ‘I can assure you’, he wrote, ‘that there is as much difference between a surgeon of the Old School and one of the New as you can possibly imagine. We have here one of the best operators in the world Liston – A pupil of his is almost the equal, and indeed is far superior in some things to a practised surgeon of the old school’.Footnote 10
In praising the ‘new school’ of Edinburgh surgery, founded by John Bell and raised to greatness by Liston, Whelpdale mocked the pretensions of the physician and asserted the claims of surgery to be the superior science. ‘To shew you the contempt in which the Doctors are held by the great men here’, he wrote, ‘I will relate a story about Liston’. This story, which involved Liston asking his students whether they thought ‘there existed any one more ignorant than a Doctor?’, was doubtless apocryphal. But Whelpdale also confided that his personal tutor in anatomy, the celebrated (and infamous) Robert Knox (1791–1862), had told him that he ‘is sorry he graduated himself [i.e. became a physician] & would not let a son of his graduate’. ‘Besides’, Whelpdale concluded, ‘no one gets on now but general practitioners. The surgeons seldom call in a Physician’.Footnote 11
Whelpdale’s letters nicely capture the sentiment, prevalent in the early nineteenth century, that the traditional balance of power between surgery and medicine was beginning to shift. Indeed, it is notable that he referred to this new ‘School of Medicine’ in purely surgical terms. This accords with an established historical narrative. Numerous historians have argued that it was during the nineteenth century that surgery came to prominence as a profession, eventually displacing medicine in the hierarchy of social and intellectual prestige. Indeed, within the historiography of medicine, surgeons are, like the middle classes of old, perpetually rising.Footnote 12 And yet, aside from a few examples, there is surprisingly little scholarship on what this process actually looked like or how it shaped British surgical culture.Footnote 13 This is certainly true when compared to the well-established historiography on the rise of surgery in France, which traces its influences through the eighteenth century to the clinical revolution of early nineteenth-century Paris.Footnote 14 Emotions and Surgery is not intended to function as a political history of surgical professionalisation in Britain, at least not as conventionally conceived. What it does seek to do is to provide a cultural historical account of nineteenth-century British surgery through a fine-grained analysis of surgical performance and identity at a time of remarkable transformation.
Emotions, this book contends, are critical for understanding nineteenth-century surgical culture, and they played an especially vital role in shaping Romantic surgical practice, experience, and identity. In his Illustrations of the Great Operations of Surgery (1821), Charles Bell claimed that ‘it depends on the conduct of those who are now entering their Profession, whether Surgery will continue to be confounded with meaner arts, or rise to be the very first in estimation’. As we shall see in Chapters 2 and 3, he, like many of his contemporaries, framed the ‘knowledge’, ‘honour’, and ‘abilities’ of surgeons largely in terms of their capacity to act with, as well as to manage and manipulate, feeling.Footnote 15 This first chapter argues that one of the key features of the epistemic transformation that characterised the inheritance of Romantic surgery, namely a greater knowledge of human anatomy, was an increasing emphasis upon operative restraint and a caution against radical, dangerous, or so-called heroic procedures deemed likely to produce excessive suffering or even death to the patient. It is important to see this transformation not simply as an objective, epistemological phenomenon, but also as a subjective, ideological one. The deprecation of unnecessary or rash surgical intervention was the product not only of greater anatomical knowledge, but also of social and cultural change, the corollary of an emotional regime founded upon the values of sensibility, sentiment, and sympathy. As we shall see in successive chapters, these values had a profound impact on surgical identity and practice, as well as on patient experience. In this chapter, however, our focus is on their implications for the literal performance of surgery, for the manual skills and bodily dispositions deemed necessary for the cutting of one’s fellow creatures: the ‘hexis’ and ‘habitus’, as it were, of Romantic surgery.Footnote 16 Thomas Schlich is one of the few historians of surgery to consider the place of manual skill and styles of operative performance in the shaping of surgical culture and identity.Footnote 17 Like other commentators, such as Peter Stanley, he characterises the early nineteenth century as an era defined largely by speed, something that was not only deemed necessary for the mitigation of pain, but also became central to the ‘mystique of the heroic surgeon’.Footnote 18 Both Stanley and Schlich point to the existence of other operative ideals, notably grace, composure, and caution.Footnote 19 Moreover, Schlich rightly suggests that operative styles ‘needed to be controlled by a moral framework to make sure that the surgeon’s performance stayed within the limits of his patients’ best interests’.Footnote 20 This chapter corroborates that suggestion but endeavours to go further, underscoring the moral complexity of Romantic surgical performance by suggesting that speed was far from being the principal attribute for which surgeons of the period were admired. Indeed, it argues that a new-found emphasis upon restraint actually had deeply ambiguous implications for the place of manual dexterity and operative flair in contemporary surgical culture and identity. On the one hand, physical dexterity and operative ‘boldness’ were praised as both practical necessities and signifiers of manual and mental aptitude, but, on the other, surgical commentators of the period increasingly expressed distrust of excessive flamboyance and self-regard, which they came to see as the expression of an inauthentic surgical persona.
With the expansion of hospital-based teaching in the late eighteenth and early nineteenth centuries, operations were performed with increasing frequency in front of sometimes large audiences of students and fellow practitioners. Schlich and others have suggested that such public performances encouraged surgical ‘showmanship’.Footnote 21 As we shall see, especially in Chapter 4, surgeons were indeed scrutinised and judged for their operative performance, sometimes quite harshly. However, surgical performance in the Romantic operating theatre involved more than the mere display and evaluation of style and skill. The operating theatre was, in fact, a complex political and emotional space that required careful moral management.
If the performative dimensions of Romantic surgery were complex and ambivalent, then those qualities can be said to have crystallised in the form of one of the Romantic era’s most celebrated operators, Robert Liston. Liston’s renown as perhaps the greatest operative surgeon of the 1830s and 1840s was spread by contemporaries such as Andrew Whelpdale and has been sustained by subsequent generations of historians. And yet, while Liston is famed as a bold and skilful operator, and as the first surgeon to perform an operation under anaesthesia in Britain, he is often represented, especially in more sensationalist accounts of the history of surgery, as the last of the surgical old guard, a speed-obsessed showman whose rashness hints at the cruelty and brutality of the pre-anaesthetic era.Footnote 22 In her account of John Elliotson’s (1791–1868) mesmeric demonstrations in the operating theatre at University College Hospital, Alison Winter remarks that ‘insufficient historical study has been undertaken to recover the kinds of surgical displays that made Liston so immensely effective as a surgical performer’.Footnote 23 As we shall see in the final section of this chapter, the solution to that riddle is not necessarily straightforward. For one thing, Liston’s performances, and their reception, were shaped by the twin demands of care and cure, demands that were not always easily reconcilable. Moreover, his reputation as an operator was not simply an objective corollary of his abilities, but was formed by a variety of complex social and political factors, not the least of which were the factious cultures of medical reform and the occasionally antagonistic relations of Anglo-Scottish surgery.
Anatomy, Science, and the Decline of Heroic Surgery
In order to understand how the notion of operative restraint became central to Romantic surgical identity, it is first necessary to consider how it came to be tied to a customary narrative of social, intellectual, and epistemological self-improvement. Surgeons of the period were profoundly conscious of their historically questionable status and of their associations with empirical, rather than scientific, practice. However, in their writings and lectures, they crafted a narrative of surgery as risen to respectability from humble origins in less than a hundred years. Speaking to his St George’s Hospital class in 1820, Benjamin Brodie (1783–1862) claimed:
In this and in many other Countries where surgery was first pursued as a separate profession, it was held in low estimation. Even in the beginning of the last century, the Surgeon was a subordinate person, who Trepanned and performed amputations, under the direction of the Physician. But since that time, our profession has made rapid strides towards its present dignified and honourable station. It has been adorned in this Country by Cheselden, Hunter, and Pott, and we may safely say, that at the present day, the Surgeon in the Metropolis, ranks in public estimation, at least as high as the Physician.Footnote 24
As a lecturer at St George’s, Brodie may have had good reason to single out William Cheselden and John Hunter as pioneers of modern surgery, as both men were closely associated with that hospital. Brodie’s teacher, and fellow St George’s Hospital surgeon, Everard Home (1756–1832) certainly had especial reason to celebrate the latter, as he was Hunter’s brother-in-law and his former pupil, as well as the joint executor, together with Hunter’s nephew Matthew Baillie (1761–1823), of his estate. Moreover, he was the direct inheritor of Hunter’s intellectual legacy and benefited greatly from the association, although his reputation was tainted by his subsequent destruction of Hunter’s personal papers, an act that gave rise to inevitable suspicions of plagiarism.Footnote 25 In 1811, some twelve years prior to this fateful decision, Home gave a series of lectures to his students at the Great Windmill Street Anatomy School, founded by John’s older brother, William Hunter (1718–83); he chose to open in customary (and self-serving) fashion with some moral and historical instruction. ‘It is usual in beginning a course of lectures wither [sic] on Medicine or Surgery’, he announced, ‘to read an introductory Lecture, in which is given a short history of the art, its excellencies pointed out, & the sources from which the teacher derived his knowledge detailed’. He continued:
In the earlier times of physic, the art of Surgery was low and confined to the performance of manual operations, which were determined by the Physician. As the physicians professed no accurate knowledge of the structure of the human body, it was impossible that the art could be advanced under their direction. Surgery could not be improved till the practitioners had become acquainted with the different parts of the body; their use & connection with one another. With the progress of Anatomical Knowledge is to be traced the advancement of Surgery.Footnote 26
Surgery’s professional and social subordination was, then, according to Home, a direct product of the physician’s ignorance of anatomy. However, even if the necessity of anatomical knowledge for improved surgical practice had long been acknowledged, ‘the prejudices of mankind against dead bodies made it necessary that Anatomical pursuits should be followed in secret in the first instance’. This only began to change in the eighteenth century, Home alleged and, in a narrative that would become a staple of later hagiographic accounts, he held the personal achievements of the Hunters responsible for a greater national renewal:
In England, before the time of Dr Hunter, Anaty [sic] was superficially taught, & improvements in it confined to France. To the late Dr Hunter England is indebted for the rapid advancement she has since made in the Practice of Surgery. Dr Hunter not only made himself master of the anatomy of the human body but every thing concerned with that study by diligence & unwearied perseverance. His merit to his country however extended beyond these narrow limits. With infinite difficulty, notwithstanding the professional prejudices against it he instituted a practical School for Anatomical Dissections. He was hence not satisfied with being eminent himself, but desirous of making his pupils as capable as their master.Footnote 27
Home’s implication about the equivalence of master and pupil was clear enough. However, in case anyone in his audience had missed it, and to ensure that he caught the full light of the Hunters’ reflected glory, he added that his testimony was ‘a just tribute to the memory of that great man who erected the walls by which we are now surrounded & it was from him that I received my first lesson’.Footnote 28
While Home may have had a particularly close personal connection to William and John Hunter, he was far from alone in claiming a unique place for the brothers in the history of anatomy and surgery. As his lecture implies, William’s contributions to anatomical study were widely recognised by Romantic surgeons, but it was his younger brother John who, as the surgical sibling, was most commonly singled out for praise. Indeed, Stephen Jacyna has argued that he was deified by later eighteenth- and early nineteenth-century surgeons to an extent rivalled only by Isaac Newton’s (1642–1727) idolisation in natural philosophical circles.Footnote 29 According to Jacyna, unlike Newton, or indeed other celebrated figures in the history of medicine such as William Harvey (1578–1657) and even his own erstwhile apprentice, Edward Jenner (1749–1823), Hunter did not lend his name to a single discovery or therapeutic innovation. Instead, his fame rested on his wholesale transformation of surgery from a manual occupation to a scientific one.Footnote 30 As the Guy’s Hospital surgeon Astley Cooper pithily put it to his students, ‘Surgery before his time was good mechanical but after it good scientific’.Footnote 31
The principal locus for the mythologisation of John Hunter and the celebration of scientific surgery in the nineteenth century was the Hunterian Oration to the Royal College of Surgeons, established by Home and Baillie in 1813. This provided an opportunity for leading surgeons of the day to rehearse their history, and to cement Hunter’s place in it as the man who transformed surgery into a science. What is important to note is that these orators, and others who lauded Hunter’s legacy, did not celebrate the cultivation of scientific anatomy for its own sake. In a remarkable claim that swept away the achievements of Andreas Vesalius (1514–64) and Ambroise Paré (1510–90) among others, William Norris (1757–1827) stated:
since the time of the Greeks, very many ponderous volumes, of pompous title and bombastic promise, on the subjects of Anatomy and Surgery have been published; but they contained little that was of any value, save what was purloined or imperfectly translated from their predecessors. The surgery therefore which prevailed in this country, even at the beginning of the eighteenth century, except in the treatment of a few diseases, could hardly be said to be an improvement upon that of Hippocrates, 2,200 years before!Footnote 32
What was different about Hunter and his contemporaries, Norris and others proposed, was that their knowledge of anatomy and pathology was fundamentally applicable to practice. This was not the classical anatomy of the physician, concerned predominantly with structure and form, but rather a surgical anatomy, which enabled the surgeon to treat disease and injury with greater confidence and with better results for the patient. According to Norris:
This preliminary knowledge necessarily produced a more rational pathology; and that the comforts and safety to mankind from thence derived became apparent, and were properly appreciated, is seen by the high degree of estimation in which those who exercised the Art and Science of Surgery were held. The easy and effectual method of restraining haemorrhage by the ligature – the general adoption of simple and superficial applications to wounds and sores – the practice of saving as much skin as possible in operation – and even the bringing into contact the divided muscles from the opposite sides of a stump immediately after amputation, so that they occasionally unite by the first intention, are a few of the very many improvements that had taken place.Footnote 33
As we have suggested, if John Hunter became the model of the scientific surgeon for London’s practitioners in the early nineteenth century, the picture in Edinburgh was somewhat different. The reception of Hunter’s legacy in Scotland in general, and Edinburgh in particular, is a topic that invites further study. Despite being a Scot, Hunter moved to London at an early stage in his career and stayed there until his death. As such, he remained indelibly associated with England’s capital. Moreover, both brothers were born in Lanarkshire and had close ties to Glasgow. The latter was especially true of William, who studied at the university there, and it was to that institution that he left his anatomical collections after his death. Both men were therefore outside of the orbit of the Edinburgh medical and surgical elite, and neither could be comfortably assimilated into a collective narrative of Scottish surgical self-improvement.
If there was no one figure of equivalent stature to John Hunter in early nineteenth-century Edinburgh, there were a number of individuals associated with the development of surgical anatomy in that city. In his historical account of the Edinburgh anatomical school, published in 1867, John Struthers (1823–99) opens with the three generations of the Monro family who occupied the chair of anatomy at the University of Edinburgh between 1725 and 1846.Footnote 34 Alexander Monro primus (1697–1767) studied at Leiden, but did not take a degree and only received an honorary MD from Edinburgh in 1756.Footnote 35 By contrast, his son Alexander Monro secundus (1733–1817) and grandson Alexander Monro tertius (1773–1859) were both physicians and taught anatomy in a classical manner, predicated on medical rather than surgical requirements.Footnote 36 Indeed, Monro secundus actively opposed the Royal College of Surgeons’ attempts to institute a professorship of surgery, thereby ‘preventing the establishment of a course of surgery in Edinburgh for thirty years’.Footnote 37 For Struthers, then, the true ‘father’ of surgical anatomy in Edinburgh was John Bell. As he writes:
Among the crowd of students in Mono’s class-room, there was one remarkable for his keen eye, intelligent countenance, and small stature. It struck this youth that, although Monro was an excellent anatomist and teacher, the application of anatomy to surgery was neglected. He saw this opportunity and took his resolution accordingly. This was John Bell […] As Monro had never been an operating surgeon, the deficiency in his teaching would, we might suppose, be evident enough; but the merit of John Bell’s early surgical discrimination is appreciated only when we remember that there was no surgical anatomy, as now understood, in the Edinburgh school till he introduced it by himself.Footnote 38
Bell explained, in his own words, the inadequacy of a classical anatomical education for the practising surgeon:
It is an actionable and most dangerous occupation, to attempt to benefit the human race by acquiring skill, or learning anatomy, on any thing but CORK and WOOD! unless it be upon LIVING BODIES. In Dr Monro’s class, unless there be a fortunate succession of bloody murders, not three subjects are dissected in a year. On the remains of a subject fished up from the bottom of a tub of spirits, are demonstrated those delicate nerves, which are to be avoided or divided in our operations; and these are demonstrated once at the distance of one hundred feet! nerves, and arteries, which the Surgeon has to dissect, at the peril of his patient’s life.Footnote 39
Bell began lecturing in 1786, first at the College of Surgeons and then, from 1790, at his own purpose-built anatomical school in the college grounds; he soon became one of the most popular extra-mural teachers in Edinburgh. According to Struthers, ‘the position which John Bell exemplified and defended, was one which no man will now venture to dispute, that surgery must be based on anatomy and pathology, a doctrine for which there was at that time, in “the windy and wordy school of Edinburgh”, neither acceptance nor toleration’.Footnote 40 As Bell himself put it, ‘ANATOMY serves to a Surgeon, as the sole theory of his profession, and guides him in all the practice of his art’.Footnote 41
John Bell is a central figure in the development of Romantic surgery, not least, as we shall see, because he was the most articulate advocate for a surgical identity founded upon sensibility and compassion and rooted in the embodied experience of operative practice.Footnote 42 For our immediate purposes, what is important to note is that Bell’s scientific surgery, like that of John Hunter, was not only said to have transformed surgical practice in terms of its sophistication and efficacy. It was also said to have made surgeons more cautious, encouraging them to adopt a less heroic and interventionist approach to operations. Indeed, Bell, like many of his contemporaries, castigated the surgery of the past as rash and cruel, precisely because of its relative ignorance of human anatomy and pathology:
We have now leisure to observe, how slowly diseases have been understood, or operations invented or improved; we can remark how slowly and imperfectly anatomy has been applied even to this day; at this moment we are employed in rooting out the prejudices and barbarous practices of those Gothic times! For the practice of the older surgeons was marked with all kinds of violence; and indifference about the simple cure of diseases; and a passion for operations, as the cutting off of limbs, the searing of arteries, the sewing of bowels, the trepanning of sculls [sic] round and round, and all the excesses and horrors of surgery.Footnote 43
In this new age of scientific surgery, it became increasingly common for practitioners to trust to the curative powers of nature. In a lecture to his St Bartholomew’s Hospital class in October 1818, for example, John Abernethy (1764–1831) considered the treatment of inflammation:
The Question then comes, should I open the abscess? – What would be the use of it; nature is her own Surgeon, and knows better how to do it than any of us, she removes the superincumbent parts and sets up such disorder in them that they are the last to heal – but if we stick in our knives, in a short time the wound becomes united and this is the way to make a Fistula by interfering with natures [sic] processes.Footnote 44
Of course, such a transformation did not happen overnight, and many surgeons doubtless continued to intervene while others were inclined to watch and wait. ‘The truth is’, Bell wrote, reiterating his earlier point, ‘that the practices and the prejudices of the old times mix themselves with the more orderly and perfect operations of the present day’.Footnote 45 Even so, by the early decades of the nineteenth century it had become commonplace for surgeons to deprecate what Robert Liston called the ‘old meddlesome surgery’, the ‘eternal pokings and probings of wounds, abscesses, and sinuses’. ‘Nature’, he argued, ‘well and judiciously assisted, instead of being thus thwarted, tampered, and interfered with […] will generally bring matters to a speedy and happy conclusion’.Footnote 46
This increasing emphasis upon operative restraint was not simply a consequence of greater anatomical and pathological knowledge; it was also an expression of surgery’s growing professional self-confidence and of the kinds of culturally resonant identities that Romantic surgeons sought to craft for themselves. For one thing, from the later eighteenth century onwards, what Owsei Temkin famously called ‘the surgical point of view’ had become increasingly central to the ways in which medical practitioners as a whole thought about the body and disease.Footnote 47 The effects of this were felt most powerfully in France, where the Parisian clinical ‘revolution’ of the early nineteenth century was predicated on a surgical sensibility that saw disease as located in the anatomical structures of the body, and where the traditional hierarchies of medicine, which placed the physician above the surgeon, were collapsed into the figure of the officier de santé.Footnote 48 In Britain, the manifestations of this process were not quite so dramatic, but they were no less transformative. After all, the notable expansion of the medical market in this period took place not so much among the ranks of the physician as among those of the surgeon-apothecary or general practitioner. These men may have been of lower status than the physician or the ‘pure’ surgeon, and many may have endured economic insecurity, but they were, in many ways, the vital force of early nineteenth-century medicine and, as Andrew Whelpdale’s letter quoted earlier suggests, they commanded an increasing share of the market for medical services. What was notable about these men is that they were trained not as physicians, but rather as surgeons; they therefore viewed the diseased body, and the world it inhabited, through the eyes of the surgeon, albeit one acutely conscious of his subordination to the Council of the Royal College.Footnote 49
In light of this, many surgeons were increasingly overstepping the traditional boundaries of their practice.Footnote 50 This was true not simply for general practitioners, but also for those among the surgical elite. John Abernethy, for example, was celebrated as a surgical lecturer but was, by all accounts, an indifferent operator. Astley Cooper, who otherwise regarded him as ‘an amusing companion’ with ‘an excellent private character’, stated that he ‘would have made a good physician, but never was a perfect surgeon, and never would have been, had he lived a hundred years’.Footnote 51 Even his own biographer admitted that ‘we have very little desire to rest any portion of his reputation on this branch of our duty’, adding that as Abernethy ‘advanced in life, his dislike to operations increased’.Footnote 52 We shall come to consider the reasons why Abernethy so disliked the operative aspects of surgery in Chapter 2. For the moment, it will suffice to observe that his aversion to the knife may have influenced the nature of his practice, which, in line with Cooper’s observation, was very similar to that of a fashionable metropolitan physician.Footnote 53 Though his biographer was at pains to deny it, Abernethy’s lectures speak to the fact that he saw the health of the digestive system as being at the root of many disorders, and it was this belief that led him to concoct his ‘blue pill’, something that Cooper believed ‘did him harm’.Footnote 54 Even so, it would be inaccurate to conceive of Abernethy’s practice purely in terms of his praxial limitations or intellectual idiosyncrasies. Rather, his reluctance to regard surgery ‘merely as an operative art’ was part of a broader ideological commitment to uniting medicine and surgery in the management of disease.Footnote 55 Never a political radical, Abernethy nonetheless invoked the radicalism of French medicine when he famously told his students that ‘surgery and medicine are essentially, what the French Republic was declared to be, “one and indivisible”’.Footnote 56 ‘The physician must understand surgery and the surgeon the medical treatment of disease’, he informed the audience at his Hunterian Oration of 1819.Footnote 57
Even if the desire to stress competencies other than the manual can be seen as part of Romantic surgery’s designs on the sphere of medicine, it might nonetheless appear odd that surgeons of the early nineteenth century sought to distance themselves from the one aspect of their practice that rendered them unique. After all, from the middle decades of the nineteenth century onwards, surgeons were apt to emphasise their physical capacities as heroic men of action, and by the later decades, operative surgery had become, in the words of Thomas Schlich, the ‘technological fix’ for the ills of the modern body.Footnote 58 In order to make sense of this rhetorical and political strategy, it is important to reiterate that it did not constitute a wholesale repudiation of embodied skill per se. Rather, it deprecated the kind of rash and heedless operative intervention that was represented not only as the marker of a more ignorant past, but also, on occasion, as the preserve of other surgeons whose abilities and temperament one might seek to call into question. Take, for example, John Bell’s attack on the System of Surgery (1783–8) of the (unrelated) Edinburgh surgeon Benjamin Bell (1749–1806), written under the pseudonym ‘Jonathan Dawplucker’:
The difference betwixt your description and that of a bold operator, is just that which distinguishes an assassin from a brave man! You write bloodily, though not boldly: you speak not like a regular surgeon […] but like a desperate man, careless of everything, and afraid only of being affronted, or, in other words, “embarrassed” in the midst of a public exhibition! You write like one who had been often caught and entangled in difficulties from which he had no other way of disengaging himself than by a slap-dash stroke of the knife […] You are enfuriated [sic] by opposition! the words adhesion, stricture, gut, and sac, excite proportioned fury! and you exclaim, tear, cut, clip, destroy – Tear the adhesions, cut every thing; - surgery consists in cutting! and the best surgery is to cut every thing!!!Footnote 59
As this quotation suggests, Bell sought to represent his rival as a man whose operative ‘boldness’ was in actual fact a cover for vanity, anger, and incompetence. His implication was not that operative skills were unimportant; far from it. Rather, as we shall now see, Bell and others were beginning to suggest that not only were exquisite manual skills and a deep knowledge of anatomy essential to the effective practice of surgery, but so too was a particular kind of emotional disposition. Shaping a professional identity within the emotional regime of Romantic sensibility, these men sought to craft an image of the modern surgeon not simply as a cerebral and scientific practitioner, but also as a moral one: self-confident, composed, and utterly dedicated to his patient’s safety and well-being.
Embodied Knowledge, Dexterity, and the Moral Surgeon
Speaking to his surgical class at St Thomas’ Hospital in 1815, Astley Cooper defined the embodied qualities of the surgeon in a phrase that would become a veritable cliché in later years. ‘With regard to operations’, he stated, ‘a few acquisitions are necessary. It has been said that an Operator should have a[n] Eagle’s eye, a Lion’s heart and a Lady’s hand’.Footnote 60 This common proverb can be found as early as the mid-eighteenth century and, doubtless, has its origins even further back than that.Footnote 61 Even so, among his students and acolytes at least, it became closely associated with Cooper, a man widely regarded as the greatest English surgeon of the early nineteenth century and, alongside Liston, possibly the best operative surgeon of the pre-anaesthetic era. The phrase is remarkable for a number of reasons, not least the framing of haptic skill as feminine. As we shall see in Chapter 2, the culture of sensibility allowed for a more fluid gendering of surgical skill than was common in the latter part of the century, although surgery remained a resolutely masculine practice until that time.Footnote 62 What is also suggestive about it is the insight that it provides into the habitus of the Romantic surgeon: the melding of perceptual, physical, and emotional/affective qualities. We shall explore the emotional/affective aspects shortly, but first it is necessary to consider the other two dimensions.
It is notable that, in introducing these necessary qualities, Cooper refers to them as ‘acquisitions’, suggesting that they were things that could be taught and learned. This is not an unproblematic assumption. If we are to take his animal metaphor seriously, we might question whether the lion learned to be courageous or whether the eagle acquired excellent eyesight. It would surely be more accurate to suggest that these qualities (even as culturally constructed) are innate to those creatures. Certainly, there was a good deal of debate in this period about whether the true surgeon was born or made. According to an anonymous correspondent to The Lancet, the public, thinking surgery a
mere mechanical operation […] conclude that frequent practice, with a proper knowledge of anatomy, must make them perfect performers:- but this is not the case; daily practice upon a musical instrument will never make some people good players […] nor will all the opportunities of operating in an [sic] hospital make a good operator of the man who has neither the eye […] nor the dexterity of finger which are the necessary prerequisites for such a performer.Footnote 63
The St Bartholomew’s Hospital surgeon Frederic Skey (1798–1872) likewise maintained that the ‘dexterity of hand’ or ‘the power of entire command over its movements, which should be at the same time firm, but light and graceful […] can only prevail in perfection, in men naturally gifted by its possession’.Footnote 64 And yet there were few surgeons indeed who would have claimed to be perfect operators. Even Astley Cooper admitted that he was ‘never a good operator where delicacy was required’ and that ‘for the operation of cataract he was quite unfitted by nature’.Footnote 65 Cooper’s reference to surgical dexterity as being akin to the ‘lady’s hand’ offers a suggestion as to how this paradox concerning nature and nurture might be resolved. After all, it was generally assumed in this period that women had an innate propensity for delicate handicraft. And yet, women’s education (across the social spectrum) still put great store by cultivating and honing those skills.Footnote 66 By the same token, it might be assumed that an aspirant surgeon, even one possessed of the natural gifts of good eyesight and dextrous hands, would still need to be trained in order to realise their potential. As John Bell put it, ‘Though the qualifications of a surgeon are not to be acquired, yet assuredly they may be improved’.Footnote 67
Unfortunately for the historian, the sources of embodied surgical education are not readily accessible, and it remains difficult for us to fully grasp, using the conventional materials of historical research, the exquisite haptic repertoire of Romantic surgical performance, or the ways in which those skills were inculcated in the novice. As Mark Jenner and Bertrand Taithe have argued, ‘Professional historians are deeply suspicious of modes of representation based upon bodily practices such as those followed by re-enactment societies’ and ‘rarely seek theatrically to recapture and master the manipulative techniques, the precision of hand, and other non-verbal embodied skills which were at the core of much medical practice’.Footnote 68 However, if many of the praxial dimensions of surgical education remain lost to posterity (at least in terms of their depth and sophistication), we can nonetheless appreciate something of the importance of manual training to surgical practice through what textual forms are available to us. After all, most surgeons offered at least some basic advice in their lectures on the correct way of handling the knife, and of making incisions. It should perhaps come as no surprise, given his reputation in the operative dimensions of surgery, that one of the fullest such accounts can be found in the works of Robert Liston, notably his Practical Surgery (1837). This offered a reasonably compressive guide to operative technique, even within the constraints of the textual form (Figure 1.1).
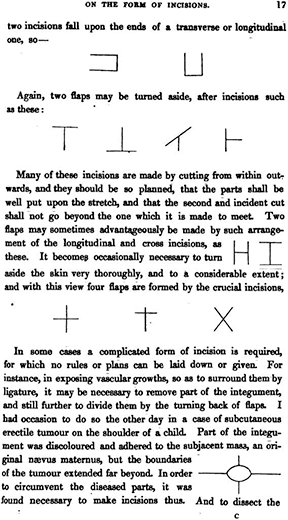
Figure 1.1 Haptic hieroglyphics: Robert Liston’s guide to incisions from his Practical Surgery (London: John Churchill, 1837), p. 17.
Nevertheless, the principal lesson that such written accounts taught the student of surgery was that operative skills could be acquired only by doing, not reading. According to Charles Bell, ‘words alone will never inform the young Surgeon of the things most necessary to a safe operation’.Footnote 69 For Astley Cooper, then, ‘the first object to become a good Surgeon is anatomy’, for ‘a person may operate well without it, but it is only by chance’.Footnote 70 In order to learn anatomy, as we have heard, students conventionally attended lectures in which the forms and functions of the body might be elucidated, either through illustrations and preparations or the dissection of a corpse by an anatomical demonstrator (Figure 1.2). However, by the early nineteenth century the dictates of surgical anatomy, such as practised by John Bell in Edinburgh and in the private medical schools of London, ensured that students were increasingly provided access to their own (often illicitly acquired) corpses.Footnote 71 Such forms of hands-on dissection were deemed increasingly essential to the training of operative surgeons, and specialist publications such as The London Dissector (1811) sought to guide the student through the process. ‘Dexterity in the manual operation of dissection’, it argued, ‘can only be acquired by practice’:
This species of knowledge will afford him the most essential assistance in his future operations on the living subject; in which indeed it is so necessary that we are perfectly astonished to see persons rash enough to use the knife without possessing this information; but we view the hesitation, confusion, and blunders by which such operators betray their ignorance to the bystander, as the natural result, and the well-merited but too light punishment, of such criminal temerity.Footnote 72
By dissecting the dead human form, then, aspirant surgeons might familiarise themselves not only with the anatomy of the body, but also with its haptic presence, the resistance provided by flesh and bone to knife and saw. They might also guard against future disgrace. Dissection, according to John Bell,
gives a dexterity of hand, and acuteness of sight; a manner of searching for and seizing, with the most delicate of hooks and other instruments, parts almost invisible to one not trained to dissection: And that dexterity and acuteness of sight, gives presence of mind in the moment of operation […] [it] renders scenes of danger familiar by anticipation; and inspires by degrees that address and courage, which enables a Surgeon to bear up undismayed, against alarms and accidents, when his own reputation is at stake; and, what is more distracting, while the life of a fellow-creature is endangered: Of a fellow-creature who has, at his suggestion, submitted to a dangerous operation, and is fainting in his hands, from pain and loss of blood.Footnote 73

Figure 1.2 Robert Blemmel Schnebbelie, A Lecture at the Hunterian Anatomy School, Great Windmill Street, London, watercolour (1839).
Bell’s comments, and those of the London Dissector, are notable for their deployment of emotion: their evocation of the tribulations and anxieties of operative surgery, and of the personal costs of failure, especially in front of an audience. This should come as little surprise. After all, while it might promote familiarity with the intricacies of the human frame and the use of surgical instruments, the dissection of a dead body (or even ten dead bodies, for that matter) could never truly prepare the student for the realities of operating upon a living, breathing, writhing patient. Surgical pupils were therefore encouraged to attend operations by eminent practitioners and become acquainted with the realities of operative practice. For example, Home stated that the student ‘should add to his own information by the practice of others. Public Hospitals are so many Seminaries for this part of Education, whose Operations are performed under all circumstances & varied according to the Knowledge & dexterity of the Surgeons’.Footnote 74 Students might even gain direct personal experience by paying to assist in operations, a position known as a ‘dresser’. Nonetheless, it was perfectly common to qualify as a surgeon without ever having performed an operation, let alone a capital procedure such as amputation or lithotomy.
In her ethnographic study of contemporary American surgical education, Rachel Prentice states that ‘Surgeons must teach both skills and meaning’. Most of the surgeons she worked with spoke of technical skill as constituting a mere 20 per cent of surgical education, ‘falling lower in importance than difficult-to-quantify qualities of wisdom, judgement and experience’.Footnote 75 Such was also the case for the early nineteenth century. Indeed, confronted by the prospect of a sentient patient in extraordinary pain, such considerations were even more important. Thus, Astley Cooper claimed that ‘the quality which is considered of the highest order in surgical operations, is self-possession; the head must always direct the hand, otherwise the operator is unfit to discover an effectual remedy for unforeseen accidents that may occur in his practice’.Footnote 76 Over thirty years later, Frederic Skey’s advice was similar: ‘He should possess great firmness of purpose […] to be acquired only by previous thought and preparation, and a self-possession which no accident, however unlooked for, can disturb or alienate’.Footnote 77
At one level, this emphasis upon self-possession was a reaction to the practical challenges of pre-anaesthetic surgery. But it was also much more than this. In the early nineteenth century, surgical lecturers increasingly emphasised the moral and emotional aspects of the surgical persona, in contradistinction to the traditional emphasis on manipulative skill and operative dexterity. ‘If I were to judge of a Surgeon’s abilities’, Cooper told his students, ‘I would not judge him by his manner of performing the operation for the stone or the amputation of a limb, but would form my opinion of him according as he possesses a power of encountering unexpected dangers with calmness. It is this quality above all others […] which you should endeavour to make yourselves masters of’.Footnote 78 In delivering his Hunterian Oration in 1826, meanwhile, the Westminster Hospital surgeon Anthony Carlisle (1768–1840) argued that ‘The operative practice of surgery is a mere mechanical art’ and that ‘if it be exercised with daring temerity, unchecked by moral or by scientific reflection, it becomes a desperate if not a mischievous calling’. The ‘vain pretender brandishing his knife over the affrighted victims of his violence, may become a popular surgeon’, he claimed, ‘and by early good luck may reach his way to vulgar fame; but his career is most dangerous, and the result unenviable’.Footnote 79
Frederic Skey was similarly sensitive to this delicate balance between the moral and manual qualities of surgery. ‘To write a work on Operative Surgery, which should consist of merely mechanical rules for the performance of an amputation’, he observed:
would be to leave the work more than half unfinished, simply because the knowledge, which determines the necessity of the undertaking is far more valuable […] than that which is required to qualify a surgeon for its performance. The one qualification involves both the moral feeling and intellect of the surgeon. The other demands the exercise of his physical functions onlyFootnote 80
This ‘moral feeling’, Skey maintained, ‘is more involved in the establishment of a just reputation than the world at large imagines’.Footnote 81 This was because the operating surgeon was ‘not a mechanic, but the agent through whose instrumentality is carried into action the highest principles of scientific medicine’.Footnote 82 Skey’s sense of the primacy of ‘moral feeling’ over manual skill was such that, even in a book dedicated to the subject of operations, he proclaimed:
I have endeavoured as an English metropolitan surgeon to carry into execution at least one primary object, viz., to strip the science of Operative Surgery of a false glare, mistaken by the ignorant for the brightness of real excellence, to check a spirit of reckless experiment and to repress rather than encourage the resort to the knife as a remedial agent.Footnote 83
Operative Surgery (1850) was published only a few years after the introduction of ether and chloroform, but it was fundamentally a product of the pre-anaesthetic era; Skey had studied under John Abernethy and his career had been forged in the 1820s. Indeed, Skey’s distrust of what he called the ‘brilliancy’ and ‘éclat’ of operative performance had deep roots in the cultures of Romantic surgery, which can be traced back to John Bell. Bell’s elaboration of a Romantic surgical persona at the turn of the nineteenth century was shaped by contemporary anxieties about the dangers of artifice and the importance of emotional sincerity and personal authenticity.Footnote 84 For Bell, the truly authentic surgical man of feeling rejected ostentation, artifice, and self-promotion in favour of a selfless and compassionate dedication to his patient’s well-being. Thus, in his Principles of Surgery (1801) he argued that ‘boldness is a seducing word, and the passion of acquiring character in operations is surely full of danger’. ‘We are but too apt’, he continued, ‘to allow the audax in periculis [boldness in danger] to be the character of a good surgeon. But this is a temper of mind and a line of conduct which can benefit nothing but the character of the surgeon himself; for as to his patient, this shameless thirst of fame! this unprincipled ambition, is full of danger’. In place of such self-centred exhibitionism, Bell proposed the following:
Should not then the present suffering of the patient, and sense of his own duty, and above all the trust that is reposed in him, occupy the surgeon’s mind too much to leave room for vain or selfish thoughts? Yet we every day see surgeons cutting out harmless tumours with affected and cruel deliberation, and in the same hour plunging a gorget among the viscera with unrelenting harshness.
Believe me, those qualities which relate to operations and other public exhibitions of skill, are of a very doubtful kind, while the duties of humanity and diligence are far more to be prized; they are both more amiable and more useful.Footnote 85
According to Bell, then, operative flair was not simply an affectation that, in many cases, concealed as much as it revealed; it was a morally repugnant act that put the practitioner’s desire for esteem ahead of his patient’s interests. Charles Bell certainly inherited his brother’s sensibility in this, as in many things, writing that ‘Any thing [sic] like a flourish on such an occasion, does not merely betray vanity, but a lamentable want of just feeling. It is as if a man said – Look at me now – see how unconcerned I am, while the patient is suffering under my hand!’Footnote 86 Moreover, John Bell’s arguments had a lasting impact far beyond his own family. John Struthers praised the Principles of Surgery as an ‘undying book’, while The Lancet claimed that it ‘may be fairly considered the most interesting, if not the most useful, that has ever appeared on the subject of surgery […] a work which may make a man proud of his calling’.Footnote 87 Indeed, if Skey’s comments suggest something of Bell’s influence, in other cases the intellectual inheritance was even clearer. For example, in lecturing to his students at the Aldersgate Street Medical School in the early 1830s, James Wardrop (1782–1869) quoted directly from the above passage of ‘the late Mr John Bell’ before adding his own coda:
Some of you may have heard of instances where surgeons, in other respects deservedly eminent, forgetting the duties of civilized life, have attempted a kind of theatrical effect in performing operations, for no other purpose than to give bystanders a false impression of their dexterity, coolness, and presence of mind […] that affectation of dexterity, or doing operations quickly, is but a pitiful ambition in those who use it […] but you will invariably observe that none except those who are deficient in moral courage […] find it necessary to resort to such conduct; and that a man who feels himself equal to the task he undertakes proceeds deliberately and calmly, steadily bearing in mind the grand object – relief to the patient.Footnote 88
Clearly, then, Romantic surgical culture militated against the idea of excessive, ostentatious, and unrestrained operative display. However, the very fact that surgical writers and lecturers of the early nineteenth century felt the need to caution against flamboyance and theatricality hints at another important dimension of operative practice. We have already heard from publications such as The London Dissector that surgery was often performed in front of an audience and that surgical skill was increasingly subject to scrutiny. Now we shall discover that this ‘public’ quality had profound implications for surgical performance, both literal and metaphorical.
The Operating Theatre as Performative and Emotional Space
The nineteenth-century Scottish author John Brown (1810–82) is now not much remembered. But in his lifetime he was a celebrated essayist and man of letters and was invariably mentioned in conjunction with his most well-known story, Rab and His Friends (1859). Essentially a paean to the nobility of dogs, this is a semi-autobiographical work in which surgery plays a central role.Footnote 89 Brown studied surgery in Edinburgh in the late 1820s, was apprenticed to James Syme, and served as a dresser and assistant at Syme’s Minto House Hospital.Footnote 90 The story begins in 1825 with Brown as a teenage boy witnessing Rab, a large grey mastiff, kill a crazed bull terrier on the Cowgate. It resumes six years later with Brown a student at Minto House. He is now close to Rab and is acquainted with the dog’s owner, a simple carter by the aptronymous name of James Noble. One day, James brings his wife, Ailie, to the hospital with what he refers to as ‘trouble in her breest [sic]’. On examination, her breast is found to be ‘hard as stone, a centre of horrid pain’, and Syme opines that the advanced nature of the cancer means that she must be operated on urgently.Footnote 91
The operation takes place the following day and the students, eager to witness the procedure, rush into the theatre. ‘Don’t think them heartless’, Brown cautions his readers; ‘they are neither better nor worse than you or I; they get over their professional horrors, and into their proper work – and in them pity – as an emotion, ending in itself or at best in tears […] lessens, while pity as a motive is quickened’. ‘The operating theatre is crowded’, he continues;
much talk and fun, and all the cordiality and stir of youth. The surgeon with his staff of assistants is there. In comes Ailie: one look at her quiets and abates the eager students. That beautiful old woman is too much for them […] These rough boys feel the power of her presence […] The operation was at once begun; it was of necessity slow; and chloroform – one of God’s best gifts to his suffering children – was then unknown. The surgeon did his work […] [Finally] it is over: she is dressed, steps gently and decently down from the table, looks for James; then turning to the surgeon and the students, she courtesies, – and in a low, clear voice, begs their pardon if she has behaved ill. The students – all of us – wept like children.Footnote 92
Brown’s story provides a linking thread between the conventions of Victorian sentimentality and those of Romantic sensibility, linkages that are now increasingly recognised by historians.Footnote 93 Even so, it explicitly represents a pre-anaesthetic emotional regime in which the sufferings of the patient constituted a moral drama at the heart of surgical performance. Brown begins by asking his readers not to judge his fellow students for their enthusiasm or jocularity, suggesting that emotional restraint is a central aspect of surgical character and education. And yet, when confronted by the nobility of this woman, they are moved, ultimately, to tears. Neither is it just the students who express emotion. Syme himself is recorded as addressing Ailie in ‘a kind way, pitying her through his eyes’.Footnote 94 This is not incidental. Such affective engagement is central to the story’s purpose, for as Brown notes, ‘there is a pleasure, one of the strangest and strongest in our nature, in imaginative suffering with and for others’.Footnote 95
As we shall see, Brown’s representation of the emotional and moral politics of the pre-anaesthetic operating theatre was an idealised one. Nevertheless, it captures something vital about this space as one of noise, confusion, and occasionally irreverence, which had, somehow, to be managed and disciplined. It also reminds us of the theatrical aspects of surgery in this period. Romantic surgery was not only an intense drama, it also often had a stage and actors, as well as an audience. In Chapter 4, we shall consider in more detail the ways in which a theatricalised sensibility shaped the radical scrutiny of surgical practice. For the moment, we are concerned with the general cultures of the operating theatre and its impact on surgical performance.
Before considering the theatrical dimensions of Romantic surgery, it is important to note that many operative procedures in this period were undertaken in private residences by fee-paying patients. Aside from the occasional textual reference, or images such as the well-known 1817 watercolour of an operation to remove a tumour, undertaken in the otherwise salubrious surrounds of a Dublin drawing room (Figure 1.3), we know relatively little about how such homes were arranged, or rearranged, for the purposes of medical and surgical procedure. By contrast, we know rather more about how the operative spaces of public institutions were appointed. Most hospitals, including small provincial ones, had some kind of discrete space for the performance of operations. With the expansion of surgical education in the later decades of the eighteenth century, however, teaching hospitals, such as those in London, built larger rooms to accommodate students. Few operating theatres from this period survive. The best example in Britain is that of the old St Thomas’ Hospital, originally built in 1822 before being rediscovered and partially reconstructed in the late 1950s. From this survival, as well as from contemporary sources, we know that operating theatres of the period traced their spatial lineage back to the anatomical theatres of the Renaissance.Footnote 96 The oldest of these was built at Padua in 1594, followed by a similar structure at Leiden in 1596 (Figure 1.4). As Jonathan Sawday observes, these spaces ‘combined elements from a number of different sources, drawing together different kinds of public space in order to produce an event that was visually spectacular’. ‘In the construction of these theatres’, he states, ‘we can discern outlines of the judicial court, the dramatic stage, and, most strikingly, the basilica-style church or temple’.Footnote 97 What is perhaps most characteristic about these structures is their steep terraced sides, often with a balustrade and handrails to allow the audience to gain as unobstructed a view as possible. Enhancing the visuality of the proceedings was not simply about observation, however. The spatial arrangement of the theatre also focused the audience on the moral dimensions of the performance. In her work on the anatomical demonstrations of Alexander Monro primus, Anita Guerrini coins the term ‘moral theatre’ to describe the ways in which anatomical dissection functioned as a ‘public performance intended to induce in its audience such emotions as awe, fear, and compassion – emotions similar to those provoked by religious practices’.Footnote 98

Figure 1.3 ‘A surgical operation to remove a malignant tumour from a man’s left breast and armpit in a Dublin drawing room’, watercolour (1817).
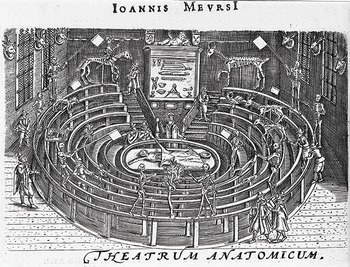
Figure 1.4 Leiden anatomical theatre (1596), from Johannes van Meurs, Athenae Batavae (1625).
However, while the operating theatre of the early nineteenth century had its antecedents in the anatomical theatres of the Renaissance, they were not identical structures. Most operating theatres built in this period had a more proscenium than amphitheatrical quality, with the audience facing the ‘stage’, so to speak, more or less front on (Figure 1.5). In part, this reflected wider shifts in theatrical architecture, but it also coincided with a fundamental shift in purpose. Early modern anatomical dissection was, to a great extent, a public spectacle. Artists attended to view the form and articulation of the body, while others sought spiritual succour in the wonders of divine creation. By the early nineteenth century, however, routine public anatomical demonstrations had all but died out. Such practices increasingly moved behind closed doors as their rationale shifted from quasi-religious revelation to utilitarian medical education. The same is true of the operating theatre. These spaces were located in hospitals, which, during the course of this period, were transitioning from quasi-public civic spaces into professional institutions dedicated to the construction and dissemination of medical knowledge.Footnote 99 Members of the public occasionally continued to attend operations in the first half of the century, but there was a growing consensus that these were professional spaces that should be accessible only to practitioners and students.

Figure 1.5 F. M. Harvey, The Old Operating Theatre at The London Hospital, Demolished in 1889 (1889), oil on canvas.
To say that the early nineteenth-century operating theatre was a more tightly policed space than its forebears is not to say that it was any less moral or dramatic. Indeed, one might say that, as the space was shorn of its spiritual connotations, it became ever more akin to a theatre in the literal sense. In almost all the hospitals of the metropolis, it was necessary to be either a practitioner, or a student in possession of a ticket, in order to attend an operation. The behaviour of this audience also resonated with the experience of play-going. The St Thomas’ Hospital surgeon John Flint South recalled that, as a young student:
The operation day was Friday, and in the earlier part of my hospital life it was very rare to have less than two or three operations. The operating theatre was small, and the rush and scuffle to get a place was not unlike that for a seat in the pit or gallery of a dramatic theatre; and when one was lucky enough to get a place, the crowding and squeezing was oftentimes unbearable, more especially when any very important operation was expected to be performed.Footnote 100
Chaotic though such scenes might appear, there was, in principle at least, a semblance of order. Generally speaking, the space immediately around the table was occupied by the surgeon, his assistants, and dressers. The seats closest to the front were reserved for the house surgeons and eminent visitors, while those behind were taken up by fee-paying students. Other, less prestigious visitors, meanwhile, were relegated to the back. These arrangements were subject to a delicate politics. In 1844, for example, Joseph Rogers (1820–89) decided to attend an amputation of the thigh undertaken by James Moncrieff Arnott (1794–1885) at his alma mater, the Middlesex Hospital. On entering the theatre, he ‘walked into the front row, where I found two old pupils, like myself’ and was reassured by a notice ‘to the effect that former house-surgeons, old pupils who came as visitors, and the dressers to the other surgeons, were allowed to stand there’. However, on entering the theatre, Arnott ‘turned upon me, saying […] “You have no business here – go out”’. Humiliated, Rogers ‘withdrew, (observing as I went, “I am an old pupil”,) and then took my station at the top of the theatre, amidst the tittering of the students who doubtless thought me an intruder’.Footnote 101
In many ways, the atmosphere of the operating theatre was in keeping with the broader cultures of medical student life, as described by Keir Waddington and Laura Kelly.Footnote 102 Concern about student behaviour, according to Waddington, ‘fed on a rich vein of anxiety about moral decay, crime, and intemperance associated with urbanization […] [and] its visible display of playhouses, pleasure gardens [and] prostitutes’.Footnote 103 For the most part, however, it resembled little more than schoolboy pranks or the limited licence of the apprentice. Thus, in 1823 a former Edinburgh student complained to The Lancet about the conduct of those awaiting Astley Cooper’s lecture at St Thomas’ Hospital. ‘What an interesting spectacle’, he wrote, ‘to see a body of young men assembled for the purpose of acquiring professional knowledge, actively engaged in discharging masticated paper and apple into each other’s faces; or employed in the no less intellectual occupation of twirling around the Lecturer’s table, or sprinkling dirt on the heads of those who happen to sit under them’.Footnote 104 At other times such rowdiness could serve more political ends, as students sought to defend their perceived rights and interests. This was especially notable in the aftermath of the acrimonious collapse of the so-called United School of Guy’s and St Thomas’ in 1825.Footnote 105 Bransby Cooper (1782–1853), Astley Cooper’s nephew and protégé, had been appointed professor of anatomy to the new school at Guy’s and when he attempted to attend a lithotomy at St Thomas’, undertaken by Joseph Henry Green (1791–1863), he was forced ‘out again immediately, several of the pupils having expressed their disapprobation of his presence by hisses’.Footnote 106
Much of the time, the disordered scenes in metropolitan operating theatres were merely the product of students endeavouring to get the best possible return on their fees. In 1828, a pupil at St George’s Hospital wrote to The Lancet complaining that
I have heard, occasionally, the voice of the surgeon as he addresses the patient; I have seen, occasionally, the gleam of the knife in the operating theatre of this establishment, and have been electrified by the scream of the patient, and edified by the remonstrating voice of the surgeon; but I have rarely seen or heard more […] I have never had a fair and distinct view of an operation on the regular day of operating, since I have had the happiness of being attached to this establishment. That portion of the theatre where the patient is placed, is, upon the arrival of the operating surgeon, instantly filled by friends, dressers, surgeons, house surgeons, etc.; all these literally club their sagacious heads together, and – but need I say more? the pupils in the first row endeavour to overtop them, those in the second or third row follow their example, and the rest are under the necessity of standing on the rails, bars, posts, etc. to obtain a casual glance at what is going forward.Footnote 107
With its reference to the electrifying ‘scream of the patient’, this letter reminds us of the intense pathos at the heart of such scenes. Likewise, another correspondent evoked the ‘weeping and cries’ of Mary Hayward, a 25-year-old woman who had come to St Bartholomew’s to have a tumour removed from her knee. In the midst of the procedure she pleaded with the operator, imploring him to ‘“let it alone, let it alone! don’t pull it about any more […] plaster it up! I won’t let you cut it any more, I won’t, I won’t, I won’t”’. These expressions were combined with ‘cries of “heads! heads!”’ from the back of the theatre as the students endeavoured to catch sight of proceedings, followed by hisses when their requests were ignored. It was, according to the correspondent, an unedifying scene that ‘entirely did away with the ordinary view and benefit derived from the performance of operations in this theatre’.Footnote 108 Needless to say, many commentators were aware that such an atmosphere can have done little to improve the patient’s emotional state. Writing to The Lancet in 1827, for example, a student at the Borough hospitals of Guy’s and St Thomas’ argued that ‘The mode in which operations were conducted at both hospitals was shameful’ and that ‘during the performance of the operation there was a continual cry of “hats off, heads”, etc., which was not only annoying to the more gentlemanly students, but also tended to render the patient more fearful’.Footnote 109
We shall see in Chapter 2 how surgeons sought to render the experience of operations more emotionally palatable to the patient, and in Chapter 4 we will consider the political consequences of their failure to do so adequately. For the moment, however, it is important to recognise that the atmosphere of the operating theatre also had a profound impact on surgical conduct. For one thing, the audience members did not always limit themselves to watching the procedure or interacting only with each other. As with the contemporary dramatic theatre, which had yet to be ‘rationalised’ by the efforts of reformers and the effects of the Theatres Act of 1843, there was often a permeable boundary between ‘pit’ and ‘stage’.Footnote 110 In an incident at St Bartholomew’s in 1834, for example, Eusebius Lloyd (1795–1862) and William Lawrence (1783–1867) were tying an arterial aneurysm when they were surrounded by several other surgeons, one of whom ‘actually took the knife and forceps from MR. LLOYD’S hand and proceed coolly to satisfy his doubts by actual dissection’.Footnote 111 Such direct interference was rare and greatly frowned upon. Nonetheless, the routine throng of participants and observers could be intensely distracting, as in the case of Mary Hayward’s operation, where the crowd around the operator was such that he was forced to ‘raise his head and shoulders above those of others (thus indecorously conducting themselves) to perform parts of the operation with his arms completely extended before him’, or in another instance at Guy’s where an actual fight broke out between a pupil and a dresser over the former’s obstructed view.Footnote 112
In light of this, it is perhaps unsurprising that the Romantic ideal of operative performance should involve calm and considered deportment. Surgery was always a challenging affair, full of risks and unforeseen eventualities, but in as intense an atmosphere as the hospital operating theatre, there was all the more necessity to practice with a focused precision, unperturbed by the goings-on around. Moreover, one’s actions were subject to constant scrutiny by the audience, even down to the smallest gesture. As such, operators were discouraged from talking to their assistants unless absolutely necessary, directing their actions with nothing more conspicuous than a discreet glance or motion of the hand. At one level, while it might not necessarily accord with the conventional image of the pre-anaesthetic surgeon as a flamboyant showman, this cool-headedness was, as Stephanie Snow has suggested, a form of showmanship in itself:
By the late 1840s, ‘modern’ surgeons had constructed their professional identity upon attributes such as coolness and decisiveness. It was an image with elements of showmanship; the surgeon was the oasis of authority among the bodily confusion of severed flesh and bones, and the disarray of minds.Footnote 113
There is much truth in this statement, but there is also much more to be said, for, as we have suggested, by practising with a self-contained composure, operative surgeons not only demonstrated their intellectual and praxial authority, they also set a moral example, disciplining and ennobling their audience through calm and measured dedication to the patient’s well-being. As John Bell argued earlier in the century:
A man of science never proceeds without due reflection: The whole plan of his operation is perfect in his own mind: He communes with his assistant rather by signs than words, and his manner commands that stillness which is due to a moment of suffering, and essential to his self‐possession and success: He is formed by education, and qualified, from the first moment in which he takes those public duties upon him, to give impressive lessons to the younger members of the profession: They are awe‐struck with the first horrors of incisions and blood, but depart with gratified feelings, when they see the scene closed with entire relief to the sufferer, and happy prospect of success; and they learn to love and respect their profession, and to study it with emulation.Footnote 114
In this way, even the conventional signifiers of public and professional approbation were to be discouraged. In 1835, for example, The Lancet, commenting on the lithotomy of a 6-year-old child at Westminster Hospital, stated:
We are sorry to have to animadvert on the bad taste which has lately been frequently exhibited amongst the visitors at this theatre, and exemplified in the highly injudicious practice of applauding the operator in the course or at the conclusion of his labours […] Even putting out of sight the inhumanity of such demonstrations at a time when the patient is writhing in acute agony, the ill effect which any expression of feeling by an assembly must produce upon the nerves of the most intrepid surgeon at a critical moment, must be obvious to every reflecting mind, superadding, as it does, to the natural difficulty of the surgeon’s duty, the intense excitement of a public exhibition.Footnote 115
On occasion, the surgeon was even required to exercise a vocal emotional and moral authority over the space of the operating theatre. Generally speaking, surgeons were discouraged from addressing the audience, or offering instruction, until after the operation was over and the patient removed. A remarkable exception to this took place at St Bartholomew’s where William Lawrence, having amputated the cancerous penis of a 60-year-old man, ‘turned his back to the patient, and immediately began dissecting the part that had been removed’. Upon this, ‘the poor man raised himself up, took the handkerchief from his eyes, and was permitted to sit looking over the dissector’s shoulder for four minutes’. ‘At length’, the patient requested to know ‘what was to be the fate of this once important part’, to which Lawrence replied, ‘“Oh! It shall be taken care of, my friend, it shall be taken care of”’, a comment that ‘occasioned much laughter throughout the theatre’.Footnote 116
Doubtless, on this occasion the degree of jocularity permitted to Lawrence and his audience stemmed from the patient’s age and gender, as well as his active participation in the process. But in other instances, where the politics of sensibility demanded due reverence to suffering, especially that of women and children, the ‘voice of the surgeon’, as the St George’s correspondent quoted earlier put it, was to be edifying and remonstrative. In 1831, for example, during an operation to remove a tumour from the neck of a young boy, Joseph Henry Green admonished his rowdy audience at St Thomas’, telling them that ‘I am astonished that any set of persons calling themselves gentlemen should pass their jokes in this place, especially when a human being is suffering, putting myself out of the question, though I am not likely to perform a nice and delicate dissection the better by hearing such noises’.Footnote 117 Likewise, in 1840, Robert Liston had just commenced an operation to remove a piece of necrosed bone from the heel of a child at University College Hospital when
a person in the theatre, because the poor little sufferer began to cry, burst out into a loud laugh; whereupon Mr. LISTON instantly turned round, and asked, “if the offender belonged to that hospital?” He then remarked that “such unfeeling conduct was disgusting and disgraceful in the extreme.” The honourable gentleman also alluded, in strong terms of reprehension, to a similar exhibition of cruel misbehaviour a few days since […] This well-timed and excellent rebuke appeared to give great satisfaction to the gentlemen present. The operation was quickly executed, in Mr LISTON’S admirable and unrivalled style.Footnote 118
While this scene offers a stark contrast to Brown’s idealised representation of the emotional dynamics of the operating theatre in Rab and His Friends, it nonetheless presents Liston as a model of the Romantic surgeon, performing with great skill while also exercising moral authority and demonstrating a compassionate concern for his patient’s well-being in the face of callous indifference to suffering. However, as we shall see in the final section of this chapter, Liston’s reputation was not always so straightforward and serves as a reminder of the complexity and ambiguities of Romantic surgical culture.
Robert Liston: The Making of an Ambivalent Icon
In 1912, the American-born pharmaceutical entrepreneur Henry Wellcome (1853–1936) commissioned the Bristol artist Ernest Board (1877–1934) to paint twenty-six images of important events from the history of science and medicine. One of these images portrays Robert Liston performing the first operation carried out in Britain under inhalation anaesthesia at University College Hospital on 21 December 1846 (Figure 1.6). That Wellcome should have chosen this event is testament to its mythic place in the history of British surgery. As we shall discover later in this book, by the time Wellcome commissioned these paintings the introduction of anaesthesia was well established in professional and popular consciousness as a pivotal moment in the shift from a squalid, barbaric past to a clean, pain-free surgical modernity. But if the value of that particular historical moment was, and remains, largely unquestioned, the identity of its key protagonist was, and still is, less clear-cut. Though indelibly identified with the first use of ether in Europe, Robert Liston is something of a liminal figure, standing at the threshold of this new age while never being truly a part of it. To a large extent this is due to the fact that he died of an aneurism of the aorta less than a year later, at the peak of his career. But it also derives from his rootedness in the operative cultures of the pre-anaesthetic era. Indeed, within the historiography he is often portrayed as the literal embodiment of the physical prowess, manual dexterity, and, most especially, operative speed that came to prominence in the decades immediately before surgery’s supposed transfiguration. However, as if to serve as a cautionary exemplar of the horrors of surgery’s ancien régime, this operative celerity is frequently represented as both ‘a gift and a curse’.Footnote 119
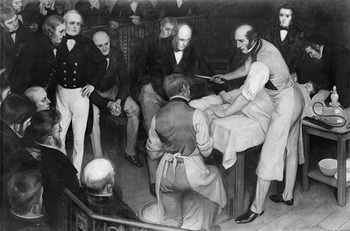
Figure 1.6 Ernest Board, Robert Liston Operating (1912).
The roots of Liston’s modern representation as an ‘incorrigible bustler’ are readily traced and demonstrate the ease with which spurious anecdote can pass into historical fact.Footnote 120 Take, for example, Lindsey Fitzharris’ popular history of Joseph Lister, The Butchering Art (2017); her reference to Liston as ‘the fastest knife in the West End’ and her account of an apocryphal operation in which his obsession with speed supposedly led to the deaths of the patient, an assistant, and a bystander are taken, virtually word for word, from a book written by the anaesthetist and Doctor in the House author Richard Gordon (1921–2017).Footnote 121 This book, Great Medical Disasters (1983), which contains a brief three-page sketch of the man, is the source of much modern Liston folklore. For example, Gordon’s claims that Liston ‘sprung across the bloodstained boards upon his patient like a duelist [sic], calling “Time me gentlemen, time me!”’ and that ‘To free both hands, he would clasp the bloody knife between his teeth’ are often repeated in popular accounts.Footnote 122 Gordon’s sources, other than his own imagination, are two articles in the University College Hospital Magazine, one of which is a general biographical account of Liston, written by Percy Flemming (1863–1941) in 1926.Footnote 123 This is the principal source for the assertion that Liston would hold the knife between his teeth.Footnote 124 Flemming likewise maintains that Liston ‘would begin an operation by exclaiming, “time me, gentlemen, time me”’.Footnote 125 In turn, this claim is an extrapolation from the second of Gordon’s sources, an account of Liston’s first use of ether, written by F. William Cock (1858–1943) and published in 1911.Footnote 126 A contemporary article in The Lancet states that ‘Dr Cock’s restrained, but vigorous, writing invests the narrative with due fascination’.Footnote 127 Meanwhile, Flemming refers to the events of 21 December 1846 as having been ‘graphically described by my old friend F. W. Cock’.Footnote 128 Indeed, on inspection it is clear that Cock’s article is largely a work of fiction, embellishing the known details of the operation with imagined dialogue, including Liston’s request to be timed.Footnote 129 It is also one of the principal accounts to claim that Liston referred to anaesthesia as a ‘Yankee dodge’ that ‘beat mesmerism hollow’.Footnote 130 Despite Alison Winter’s attribution of this quotation to Liston’s assistant William Squire’s (1825–99) account of the operation published in The Lancet in 1888, there is no evidence of such a phrase, either in this article or in his later recollections published in the British Medical Journal in 1896.Footnote 131 It is true that, in an account published at the end of the nineteenth century, John Russell Reynolds (1828–96) claimed to remember Liston uttering these words ‘as if it were yesterday’, but it is odd that no such phrase appears before around 1872, some twenty-six years after the fact.Footnote 132 Indeed, what is consistent in Squire’s reports, and in most other first-person accounts, is that Liston either made ‘few remarks’ or said ‘nothing’, as he was so struck by the effects of ether on the patient that ‘he could scarcely command himself sufficiently to address even a few words to the spectators’.Footnote 133
While Liston’s ambivalent historical reputation, awkwardly poised between hero and villain, is largely a product of the early twentieth century and owes little to his contemporary public and professional identity, the irony is that his place within the cultures of Romantic surgery was no less ambiguous or contingent. He was, by almost all accounts, a somewhat difficult man who lacked the easy manner and social graces of Astley Cooper, a surgeon who, as we shall see in Chapter 2, conformed more readily to the culturally resonant ideal of the man of feeling. Even Liston’s obituary in The Times notes that ‘His manner in ordinary society was sometimes complained of as harsh or abrupt’ and that he was ‘rather backward or indifferent in his address’.Footnote 134 In this sense, he more closely resembled John Abernethy, who was said to have been occasionally rough in his manner, or John Bell, who, despite his literary appeals to sensibility, had a dubious interpersonal reputation, even within his own family.Footnote 135 Certainly, Liston’s directness, rudeness even, is evident in his correspondence with his former assistant, James Miller (1812–64).Footnote 136 However, his obituary was at pains to aver that, despite this, he was still a man of tender compassion, claiming that ‘in the chamber of the sick – he was gentle as he was resolute’, and that ‘into the scene of suffering he never brought a harsh word or an unkind look and the hand which was as hard as iron and true as steel in the theatre of operation, was soft as thistledown to the throbbing pulse and aching brow’.Footnote 137 As this quotation suggests, if Liston’s professional character and demeanour were ambiguous, then much of that ambiguity centred, then as now, on his operative performance. And in its reference to ‘thistledown’, it also indicates how much of this ambiguity also derived from his identity as a Scot practising in the English metropolis.
As we have suggested in the case of the Edinburgh student Andrew Whelpdale, Liston’s fame in the early nineteenth century was spread, in part, by his pupils and acolytes. But it was, at a fundamental level, made by an expanding and increasingly vital medical press. There is a growing body of literature on the culture and politics of the early nineteenth-century medical press, but if there is one journal that has received the greatest attention, it is The Lancet, founded in 1823 by the radical surgeon Thomas Wakley.Footnote 138 The Lancet was significant not simply because it was one of the first journals to be published weekly, nor simply because it had by far the largest circulation of any medical journal, but also because of its literary style, which, by embracing the radical conventions of ‘democratic celebrity’, played a vital role in the making and unmaking of medical and, more especially, surgical reputations.Footnote 139
Nowhere was the role of The Lancet in shaping surgical reputations more obvious than in the case of Robert Liston. One of his earliest appearances in its pages was in connection with an operation performed by his cousin, friend, and soon to be bitter rival, James Syme, in 1823. This procedure, the amputation of the leg at the hip joint, undertaken on a 19-year-old by the name of William Fraser, was what Syme called ‘the greatest and bloodiest operation in surgery’ and had yet to be performed in Scotland.Footnote 140 Liston assisted in the operation, covering ‘the numerous cut arteries with his left hand and compress[ing] the femoral in the groin by means of his right’.Footnote 141 The Lancet reprinted the Edinburgh Medical and Surgical Journal’s initial report in early February 1824 without comment.Footnote 142 At the end of the month, however, it ran a highly critical editorial on the (ultimately fatal) procedure. Wakley was enraged by the idea that ‘the northern [i.e. Scottish] journals’ sought to use the incident ‘for the purpose of casting a shade upon the splendour of London surgery’, particularly in the way they ‘sarcastically compared the time occupied by Mr. SYMES [sic] to that occupied by Sir A. COOPER when he recently performed a similar operation at Guy’s Hospital’. Whereas Cooper ‘required twenty minutes to remove the limb’, Syme ‘according to his own account, was contented with ONE minute’.Footnote 143 As we shall see in Chapter 4, Wakley and The Lancet were nothing if not London centric, and the journal’s attitude towards Scottish (and Irish) medicine was deeply ambivalent. Moreover, Cooper had been Wakley’s tutor at St Thomas’ and so he was doubtless jealous of the great man’s reputation, as much for his own sake as for that of London surgery. Thus, rather than ‘throwing scandal upon the operation of Sir ASTLEY’, Wakley suggested that such reports seemed ‘to inculcate the pernicious principle that manual dexterity is the most important desideratum in the performance of surgical operations’. That the amputation was ‘performed with expertness, all must readily admit’, he claimed; ‘but that it was executed with judgement will be universally denied’. ‘We sincerely hope that MR. SYMES [sic] will never expose a patient to similar risk, nor himself to a repetition of such dreadful anxiety’, he concluded. As for Liston, who had ‘grappled with and squeezed the arteries […] this circumstance is so truly ludicrous and anti-surgical, we are almost inclined to believe that the assistant operator was Mr. LISTON of Drury-lane theatre’.Footnote 144
The Lancet’s comments on this matter, including its reference to the celebrated actor John Liston (c.1776–1846), illustrate the ways in which that journal would frequently characterise Edinburgh surgery as theatrical, self-promotional, and heedlessly ostentatious, in contrast to the more considered and humane surgery of the metropolis. And, as Edinburgh surgery’s leading light, as well as a man whose 6 ft 2 in. frame and physical strength shaped his identity as a surgeon, these associations stuck most closely to Liston. For example, in a quite remarkable ‘sketch’ written by ‘Scotus’ in 1830, Liston is characterised as a man ‘whose brains are obviously not contained in his cranium, but, by original conformation have been deposited, or what perhaps is more probable, have been transuded into his muscular system, by virtue of that physiological law which apportions energy to parts according to the demands of exercitation’. ‘Scotus’ figures Liston as a man utterly defined by his physicality and almost entirely lacking in sensibility and compassion: ‘He has brought [to the practice of surgery] a breadth of shoulder, muscularity of arm, and a merciful indifference to the tortures of the knife, seldom, if ever equalled by the coolest and most corpulent cultivators of that sanguinary art’. In the public space of the operating theatre, ‘Scotus’ claims, this all-consuming physicality allows for an effortless, yet inherently cynical, display of coolness:
His entrance into this arena of his most favourite avocations, is never marked by those concomitants of perturbed expression, which characterise the appearance of his contemporaries […] Instead of that self-collected contour, or compound expression of difficulty, arrangement, and responsibility of serious undertaking, which the workings of the mind impress on the countenance on those occasions, Mr. Liston’s muscular system alone evinces symptoms of emotion. A sort of vermicular movement is quite obvious throughout his prehensile apparatus, which is busily engaged in knotting his apron-strings, adjusting his sleeve wrists, manipulating some instrument, as if familiarising his fingers with the peculiarities of its form and extent of its mechanical powers; or his brawny arms and shoulders are thrown into repeated preparatory contractions, as if measuring their strength, or modulating their tone to the present undertaking. Now and then, indeed, a half-suppressed smile of self-complacency plays around his lips […] It could not be well expected that one who reserves his services for more important objects to the patient, should waste any portion of his useful energies in empty condolence; Mr. Liston consequently seems to take little interest in the feelings of those upon whom he operates, and reduces the reluctant and refractory to obedience, more by his cool, commanding and confident demeanour, than by the persuasive eloquence of compassionate address.Footnote 145
There is much in here to sustain extended analysis. For one thing, it speaks to Thomas Dixon’s observations about changing ideas of the emotions in the early nineteenth century: about what they were and where they resided.Footnote 146 It also has much to tell us about developing ideas of physicality within a culture of Romantic sensibility and its relationship to professional identities. At a time when surgeons were seeking to obvert their historical association with manual trade, it seems hardly surprising that such profuse physicality would be construed as problematic. And yet there is ambivalence here, for while Liston is represented as incapable of care, in terms of compassion at least, he is nonetheless physically capable of cure. Thus, ‘his incisions are invariably steady, rapid, and scientifically directed, costing the subject of them as little suffering as is, perhaps, consistent with the necessity of their performance’. The question of whether this Liston is a good or a bad surgeon is not entirely clear, but the overall perception is certainly negative. Hence, while ‘Mr. Liston’s merits […] are of the first order of excellence’, they are ‘degraded by a mannerism bordering on buffoonery’. Moreover, they are critically undermined by his self-conscious theatricality, for ‘[e]ven with the scalpel in his hand, his vanity of his own qualifications is putting forth its tenacula in a thousand impertinent fopperies, to receive the laudatory alms of the spectators on which it feeds’.Footnote 147
The literally monstrous figure ‘Scotus’ conjures is an extreme, yet entirely consistent, example of The Lancet’s representation of Liston during the 1820s and early 1830s. The occasional piece published in this period might allude to his operative skills. Nevertheless, most other editorials and articles either refer to him, in the characteristic language used by Wakley to describe office holders and ‘monopolists’, as ‘the northern BAT’, criticise him for his conceit and ‘indifference to the vulgar notion, of the difficulty of the operation’, or sarcastically characterise his tenure at the Edinburgh Royal Infirmary as one of callous indifference, where ‘the patients (or sufferers) are treated with great mildness and humanity; the infliction of a few blows to render them docile, obedient, and quiet during painful operations being intended and calculated for their benefit’.Footnote 148
All this was soon to change, however. In 1833, Liston’s rivalry with Syme reached its peak as the latter was appointed to the Chair of Clinical Surgery at the University of Edinburgh, Liston having refused to pay the incumbent, James Russell (1754–1836), the £300 a year he had stipulated.Footnote 149 As a result, Liston left Edinburgh for London in 1834, having accepted the post of surgeon to the newly founded North London Hospital (soon to be University College Hospital). The following year, he was also appointed Professor of Clinical Surgery at its parent institution, London University (soon to be University College London). As Adrian Desmond has shown, London University was a Benthamite project, headed by the leading Scottish Whigs, James Mill (1773–1836) and Henry Brougham (1778–1868). As such, it drew heavily upon the rationalist traditions of Scottish medical and scientific education and consciously imported many of its leading lights from north of the border. For its conservative critics, this was yet another example of ‘“Scotch” jobbery’.Footnote 150 But even for those attached to the institution it could cause tensions. This was notable in Liston’s fractious relationship with his fellow surgeon Samuel Cooper (1780–1848), but more especially so after Liston’s death, when the appointment of Syme as his successor led to Cooper’s resignation in the face of hostility from the Scottish Professor of Anatomy and Physiology William Sharpey (1802–80) and the Irish Professor of Descriptive Anatomy Richard Quain (1800–87). On that occasion, Wakley and The Lancet were trenchant in their opposition to the ‘Scottish influence’ at University College London, but on the appointment of Liston in 1834/5 they were surprisingly tight-lipped, especially given their previous criticisms.Footnote 151
By the end of 1835, moreover, something remarkable had occurred. Its first flowerings are evident in an editorial concerning Charles Bell’s appointment as Chair of Surgery at the University of Edinburgh, in which Wakley expressed his pleasure that Liston had not accepted the offer himself, claiming that ‘Within the short space of time that he has already resided in the Metropolis, Mr. LISTON has succeeded in establishing here a reputation equally well founded with that which he had previously acquired by the exercise of his scientific attainments in Edinburgh’.Footnote 152 However, it only came into full bloom following Liston’s attendance, together with Wakley, at a meeting of the medical students of London, held on 18 January 1836, calling for the formation of a ‘Central Students Association’ and a change to the way in which candidates were examined for medical licences and degrees. ‘Mr. LISTON’, the report in The Lancet observed, ‘was the only hospital surgeon in London who supported the cause of the students’. More than this, he and Wakley volunteered to lead the deputation sent to the Chancellor of the Exchequer to pass the resolutions of the meeting to government.Footnote 153
From this point on, and with his radical credentials secured, Liston could, in the eyes of Wakley and The Lancet at least, do no wrong. Indeed, in its annual ‘Account of the London Hospitals and Schools of Medicine’ in 1836, The Lancet claimed that Liston ‘has for some time been renowned as the first operator among British surgeons’ and that ‘If the justly-distinguished, and far-famed ASTLEY COOPER is ever to have a successor, in this metropolis, Mr. LISTON will be that man’.Footnote 154 Thus, while in 1824 Liston’s operative style had been derided as ‘ludicrous and anti-surgical’ and actively contrasted with Cooper’s, by the mid-1830s it was presented as the latter’s rightful inheritor. Indeed, what is remarkable about The Lancet’s volte-face with regard to Liston is the fact that the very qualities of boldness and operative dexterity that had initially rendered him problematic now functioned as the grounds on which his fame and reputation were most vigorously defended. For example, in November 1836 The Lancet reported on the case of Mary Ann Griffiths, a 20-year-old woman suffering from a horribly disfiguring tumour of the superior maxillary bone (Figure 1.7). It described Liston’s excision of the bone and its tumour, which took only seven minutes and twenty seconds, as ‘one of the most splendid triumphs that operative surgery has ever achieved’.Footnote 155 Meanwhile, within the very same month, it reported on a similar, though more tragic, case of a 24-year-old shoemaker, known simply as ‘W. B.’, whose face had been injured by a blow from a cricket ball and who had likewise developed a tumour of the superior maxilla bone. In this instance, however, the patient died several hours after the operation. Though the case ‘was unfortunate with regard to the suffering patient’, the report claimed that it ‘furnishes a useful lesson to young practitioners’ that ‘success after operations cannot be ensured’. Moreover, it ‘must prove of still greater value for Mr. LISTON himself’:
The reputation of that gentleman as an operator stands unrivalled, and the dexterity which he possesses is a subject of astonishment with surgeons who have visited the continental hospitals. The public, therefore, on discovering that an operation may occasionally be followed by fatal consequences even when it is performed by the most distinguished of our surgeons, will shrink in dismay from the thought of entrusting their lives […] to half-instructed bunglers, who, under the system of nepotism, obtain the office of surgeon in our old endowed hospitals. The issue of the case of the patient E. B. [sic], proves, beyond question or dispute, that capital operations in surgery cannot be undertaken, with safety to the reputation of the practitioner, unless by such a man as Mr. LISTON, – a surgeon of undoubted skill and established fame.Footnote 156
Here, then, The Lancet sought to use Liston’s failure to further illuminate his reputation and castigate the shortcomings of others. Such rhetorical contortions were not lost on Wakley’s opponents. The moderate reforming journal the Medico-Chirurgical Review claimed that ‘a more bungling attempt to protect a friend could scarce be made’. Questioning the wisdom of Liston’s actions in both cases, it maintained that ‘The day indeed for flashy operations is gone by. The refinement of our manners is disgusted at the exhibition of what wears more the aspect of clever butchery than science’. This was especially true, it argued, of those operations that, like that upon W. B., are of ‘so disgusting and revolting an appearance, that an eye-witness declares that of “upwards of two hundred spectators present, many became faint, and some were carried out of the theatre – such was the scene”’.Footnote 157

Figure 1.7 Mary Ann Griffiths, The Lancet 27:688 (5 November 1836), p. 237.
While the Medico-Chirurgical Review thought Liston’s propensity to operate an unseemly instance of ‘clever butchery’, a correspondent to The Lancet signing himself ‘A WELLWISHER TO TALENT AND TRUTH’ endeavoured to refute its imputations. Though he denied that ‘therein lies his forte’, this correspondent acknowledged that Liston’s operative dexterity was ‘naturally the most striking’ aspect of his surgical identity ‘and the first to be canvassed’. He claimed that most of Liston’s critics were ‘envious spirits’ who ‘strive to represent the matter to others in a disparaging point of view’ and argued that, if by ‘flashy’ the Review meant ‘tinsel, a gaudy, empty show’, then they were correct, for ‘this is not the time for such displays’. However, if by that word they meant to impugn all surgical novelty, then they were mistaken. Moreover, he challenged the idea that Liston’s actions were inhumane, asking
is not the surgeon who dextrously and safely removes a hideous swelling […] and thereby restores his patient to health, comfort and happiness […] better ‘informed’ and more ‘humane’ than the surgeon who […] with a wide shrug of the shoulders, and a scientific shake of the head, expresses pity for the suffering of the patient, but leaves the disease to run its course unmolested, and the fellow-being unassisted, to drag out a miserable existence, harassed by his fell destroyer.Footnote 158
Not all were convinced by such protestations. In particular, the conservative London Medical Gazette, Wakley’s bête noire, thought that it detected more than a little favouritism in The Lancet’s reporting of Liston. Contrasting Liston’s hallowed status with that of Wakley’s former friends and allies, John Elliotson, Professor of the Principles and the Practice of Medicine at University College London, and William Lawrence, the former radical and Lancet contributor turned conservative ‘placeman’, it wrote:
Mr Liston, the present idol of Wakley’s attachment is, we believe, the only person of any standing in the profession in London, who is desirous of the good opinion of the honourable member for Finsbury [Wakley was MP for Finsbury from 1835]; he has not been ashamed to be present at, and to take part in, meetings where Wakley has been prominent: hence, naturally, the reciprocal feeling on the part of the latter. The great attraction now at the North London Hospital is Mr Liston: Mr Liston is all in all, just as it used to be with Dr Elliotson, who at present seems to be completely thrown over-board. Why is this? […] Are we right in attributing it to the mortal hatred that subsists between Dr Elliotson and the great surgeon of the North? […] Mr Liston is held up as the model of surgeons – the greatest after Sir Astley Cooper, and so forth. How is this, when we have Mr Lawrence still amongst us in all his pristine vigour and ability […] But Mr Lawrence shook off the patronage of Wakley, and hence the rival that has been set beside his throne.Footnote 159
Conclusion
The case of Robert Liston clearly demonstrates that Romantic surgical identities were shaped not simply by words and deeds, but also by the politics of representation. Likewise, it suggests that issues such as manual skill and operative dexterity, as well as compassion and humanity, could be used to both sustain and undermine surgical reputations. Indeed, what is perhaps most evident from Liston’s fame (and infamy) is that Romantic surgical identities were dependent on a delicate balance between physicality and sensibility, action and judgement. While some might question Liston’s decision to proceed with a ‘disgusting and revolting’ operation, even if it was ‘not one which [he] undertook from choice, but on account of the urgent solicitations of the patient’, others clearly thought that trusting to nature in a case where death was almost certain was no more compassionate or humane than resorting to the knife.Footnote 160
This balance between doing and thinking, force and feeling, was not unique to the practice of surgery; nor was it static. As Joanne Begiato has argued, while masculinities are always determined by a combination of these qualities, the Romantic era saw a particularly acute set of tensions develop between them. If the age of sensibility and the deprecation of artifice created the conditions for the Romantic man of feeling, open to the authentic emotions of embodied experience, then the shadow of war and revolution also demanded virile male bodies capable of violence.Footnote 161 Even so, if surgery was not alone in this regard, it nonetheless provided a particularly vital arena for the playing out of these issues. After all, surgeons of the early years of the nineteenth century were acutely aware of the need to divest themselves of their traditional associations with brute physicality and shape identities as gentlemen of refined sensibility. By the 1830s and 1840s, on the other hand, it was perhaps becoming somewhat easier to combine physicality and vigour with morality and emotion.Footnote 162 Thus, Liston’s body could become a site of conflict not simply for competing political agendas but also for changing social attitudes, as the image of a showy and vulgar physicality depicted by ‘Scotus’, which allowed no room for sensibility, gave way to ‘Wellwisher’s’ man of action for whom pity and sympathy were not enough. Without wanting to push our analysis too far, we might even conceive of Liston as a metonym for Scottish national identity more generally, in its shift from ‘savage’ warriors, though Enlightenment men of feeling, to the ‘heroic’ warriors of the Victorian imagination.
While such semiotic considerations are clearly vital to understating his place in the cultures of Romantic surgery, it is important to note that Liston’s own relationship with the knife was equally complex, ambivalent, and conditional. Thus, in his Elements of Surgery (1831), he dismissed healing by what he called ‘the pure force of surgery’, asking: ‘Who will question, that there is more merit in saving one limb by superior skill, than in lopping of a thousand with the utmost dexterity?’ Despite his occasional representation as a rough handler of patients, he also maintained that ‘It is of utmost importance to attend to the state of the patient’s mind and feelings’.Footnote 163 By the time of his Practical Surgery (1837), however, he was perhaps more confident with his operative reputation, claiming that ‘a dexterous surgeon, like a man skilful in the use of weapons, will not enter rashly into difficulties, but being engaged from conviction, will bring himself through with courage’. He even took a swipe at the Medico-Chirurgical Review, arguing that while surgeons ‘are too often asked to admit, that operations are the opprobria of their art […] it is unjust to sneer at this department of the profession, as is done by some, affecting to consider the dexterous and successful operator as little better than a “clever butcher”’.Footnote 164 And yet, two years later, he wrote to James Miller telling him that he was engaged in ‘lots of cutting at present’, adding ‘awful I am sick of it. Operations every day at the Hospital – 4 or 5 for today – amputations – 2 thighs – arm and great toe […] also disarticulation of the jaw in very pretty young woman’.Footnote 165 Meanwhile, in another letter sent the following month, he questioned his public and professional reputation, writing that ‘They begin to find that I am not as much given to cutting as they thought’.Footnote 166 Such comments are suggestive, for as we shall see in Chapters 2 and 3, emotions were no mere counterpoint to operative performance; rather, they shaped the very experience of surgery for surgeon and patient alike.








 Open access
Open access