

All drug use, fundamentally, has to do with speed, modification of speed … the times that become superhuman or subhuman.
After all, the world is industrial and we have to come to terms with it … Gone are the old good days of opium, heroin, gone are the young bangi¸ gone is hashish, marijuana, and geraas [weed, grass]! Now it is all about shisheh, blour and kristal and nakh. The modern people have become post-modern. And this latter, we know, it is industrial and poetical, like the God’s tear or Satan’s deceit.Footnote 1
Introduction
The election of Mahmud Ahmadinejad to the ninth presidency of the Islamic Republic asserted an anomaly within the political process of post-revolutionary, post-war Iran. After the heydays of reformist government, with its inconclusive and juxtaposing political outcomes, the 2005 elections had seen the rise of a political figure considered, up to then, as marginal, secondary, if not eclectic and obscure. Accompanied by his rhetoric, which tapped into both a bygone revolutionary era and a populist internationalist fervour, Ahmadinejad brought onto the scene of Iranian – and arguably international – politics, an energy and a mannerism, which were unfamiliar to Islamist and Western political cadres.
Considering his apparent idiosyncrasies, much of the attention of scholars and media went into discerning the man, his ideas and his human circles, with symptomatic attention to foreign policy.Footnote 2 His impact on the domestic politics of the Islamic Republic, too, has been interpreted as a consequence of his personalising style of government; his messianic passion about Shi’a revival and religious eschatology clashed with his apparent infatuation with Iran’s ancient Zoroastrian heritage;Footnote 3 and, significantly, his confrontational attitude vis-à-vis political adversaries manifested an unprecedented tone in the political script. Ahmadinejad himself contributed greatly to his caricature: his public appearances (and ‘disappearances’Footnote 4) as well as speeches, amounting to thousands in just a few years.Footnote 5 His interventions in international settings regularly prompted great upheaval and controversy, if not a tragicomic allure prompted by his many detractors. His accusations and attacks against the politico-economic elites were numerous and unusually explicit for the style of national leaders, even when compared to European and American populist leaders, such as Jair Bolsonaro, Donald J. Trump and Matteo Salvini, all of whom remain conformist on economic matters. Ultimately, his remarks about the Holocaust and Israel, albeit inconsistent and exaggerated by foreign detractors, made all the more convenient the making of Ahmadinejad into a controversial character both domestically and globally, while provided him some legitimacy gains and political latitude among hard-liners, domestically, and Islamist circles abroad. Philosopher Jahanbegloo, in his essay ‘Two Sovereignties and the Legitimacy Crisis’, describes this period ‘as the final step in a progressive shift in the Iranian revolution from popular republicanism to absolute sovereignty’.Footnote 6 Conversely, in this volume, Part Two and its three Chapters give voice and substance to this period and its new form of profane politics as they emerged after 2005. In its unholy practices, it did not produce enhanced theocracy, nor absolute sovereignty. Instead it made Iranian politics and society visibly profane, with its drug policy being the case par excellence. Jahanbegloo’s take, and that of other scholars following this line, has shed a dim light on the epochal dynamics shaping the post-reformist years (2005–13).Footnote 7 It is over this period that an ‘anthropological mutation’ took shape in terms of lifestyle, political participation, consumption and cultural order.Footnote 8 This anthropological mutation produced new social identities, which were no longer in continuity with neither the historical past nor with ways of being modern in Iran. This new situation, determined by ruptures in cultural idioms and social performances, blurred the lines between social class, rural and urban life, and cultural references among people. Italian poet, film director and essayist Pier Paolo Pasolini described the transformations of the Italian people during the post-war period – especially in the 1970s – as determined by global consumerism and not, as one would have expected, by the Weltanschauung of the conservative Christian Democratic party, which ruled Italy since the liberation from Benito Mussolini’s fascist regime in 1945. Not the cautious and regressive politics of the Catholic Church, but the unstoppable force of hedonistic consumerism represented the historical force behind the way Italians experienced life and, for that matter, politics. Taking Pasolini’s insight into historical, anthropological transformation, I use the term anthropological mutation – or, as Pasolini himself suggested, ‘revolution’ – to understand the epochal fluidity of Iranian society by the time Mahmud Ahmadinejad was elected president in 2005. It was not the reformist government alone that brought profound change in Iranian society. Reform and transformation were key traits of Ahmadinejad’s time in government. That is also why the period following Khatami’s presidency is better understood as post-reformism rather than anti-reformism.
Over this period, the Islamic Republic and Iranians all lived through the greatest political upheaval following the 1979 revolution: political mobilisation ahead of the June 2009 elections, especially with the rise of the Green Movement (jonbesh-e sabz); then state-led repression against protesters and the movement’s leaders, Mir Hossein Musavi and Mehdi Karroubi. The events following the presidential elections in June 2009 exacerbated the already tense conditions under which politics had unfolded in the new millennium. Allegations of irregularities, widely circulated in international and social media, led to popular mobilisation against what was perceived as a coup d’état by the incumbent government presided over by Ahmadinejad; then, the seclusion of presidential candidates Mir Hossein Musavi and Mehdi Karrubi, inter alios, changed the parameters and stakes of domestic politics irremediably. For the first time since the victory of the revolution in 1979, massive popular demonstrations took place against the state authorities. Meanwhile, the security apparatuses arrested and defused the network of reformist politicians, many of whom had, up to then, been highly influential members of the Islamic Republic. Echoing the words of president Ahmadinejad himself, he had brought ‘the revolution in the government’.Footnote 9
In this Chapter, I dwell on a set of sociocultural trends that unfolded during this period, progressively transforming Iranian society into a (post)modern, globalised terrain. It is important to situate these dynamics as they play effectively both in the phenomenon of drug (ab)use and the narrative of state interventions, the latter discussed in the next two Chapters. In particular, the ‘epidemic’ of methamphetamine use (shisheh), I argue, altered the previously accepted boundaries of intervention, compelling the government to opt for strategies of management of the crisis. The following three Chapters explore the period after 2005 through a three-dimensional approach constituted of social, medical and political layers. The objective is to examine and re-enact the micro/macro political game that animated drugs politics over this period. In this setting, drugs become a prism to observe these larger human, societal and political changes.
Addictions, Social Change, and Globalisation
With the rise of ‘neo-conservatives’ within the landscape of Iranian institutions, it is normatively assumed that groups linked to the IRGC security and logistics apparatuses, as well as individuals linked to intelligence services, gained substantial ground in influencing politics. The overall political atmosphere witnessed an upturning: religious dialogue and progressive policies were replaced by devotional zeal and ‘principalist’ (osulgar) legislations. Similarly, the social context witnessed epochal changes. These changes can be attributed in part to the deep and far-reaching impact that the reformist discourse had had over the early 2000s, in spite of its clamorous political failures. The seeds that the reformists had sowed before 2005, were bearing fruit while the anathema of Mahmud Ahmadinejad was in power. Longer-term processes were also at work, along lines common to the rest of the world. Larger strata of the population were thus exposed to the light and dark edges of a consumeristic society.Footnote 10 The emergence of individual values and global cultural trends, in spite of their apparent insolubility within the austerity of the Islamic Republic, signalled the changing nature of life and the public.
Family structure underwent a radical transformation during the 2000s. With rates of divorce hitting their highest levels globally and with a birth rate shrinking to levels comparable to, if not lower than, Western industrialised countries, the place of family and the individual was overhauled, together with many of the social norms associated with them (Table 6.1). The average child per woman ratio fell from seven in the 1980s to less than two in the new millennium, a datum comparable to that of the United States.Footnote 12 The (mono)nuclearisation of the family and the atomisation of individuals brought a new mode of life within the ecology of ever-growing urban centres. Likewise, the quest for better professional careers, more prestigious education (including in private schools), and hedonistic lifestyles, did not exclusively apply, as it had historically, to bourgeois families residing in the northern part of the capital Tehran. Along with Mahmud Ahmadinejad’s coming to power, rural, working class, ‘villain’ (dahati) Iranians entered the secular world of the upper-middle class, at least in their cultural referents.Footnote 13 More than ever before, different social classes shared a similar horizon of life, education being the ‘launch pad’ for a brighter career, made of the acquisition of modern and sophisticated products, such as luxury cars, expensive clothes, cosmetic surgeries, technological devices and exotic travels (e.g. Thailand, Dubai).Footnote 14 These elements entered surreptiously but firmly into the daily lexicon and imagination of working class Iranians, against the tide of economic troubles and the increasing visibility of social inequality.Footnote 15 A decade later, in the late 2010s, consumerism has become a prime force, manifested in the Instagram accounts of most people.
Table 6.1 Rates of Divorce in 2004–5Footnote 11
| Iran | Tehran | |
|---|---|---|
| Divorce during in 1393 [2004–5] | 163569 | 37976 |
| Marriage during in 1393 | 724324 | 87145 |
| Ratio of divorce per marriage | 22.6% | 37.8% |
Coterminous to this new popular imagery, the lack of adequate employment opportunities resulted from a combination of haphazard industrial policy, international sanctions and lack of investments, inducing large numbers of people to seek a better lot abroad. With its highly educated population, Iran topped the ominous list of university-level émigrés. According to the IMF report, more than 150,000 people have left the country every year since the 1990s with a loss of approximately 50 billion dollars.Footnote 16 After the clampdown on the 2009 protestors, many of them students and young people, this trend was exacerbated to the point of being acknowledged as the ‘brain-drain crisis’ (bohran-e farar-e maghz-ha).Footnote 17 A report published in the newspaper Sharq indicated that between 1993 and 2007, 225 Iranian students participated in world Olympiads in mathematics, physics, chemistry and computer science.Footnote 18 Of these 225, 140 are currently studying at top US and Canadian universities.Footnote 19 The case of the mathematician Maryam Mirzakhani, who, in 2014, was the first woman ever to win the Fields Medal (the equivalent of the Nobel Prize in mathematics), is exemplary of this trend.Footnote 20 In the words of sociologist Hamid Reza Jalaipour, ‘many left the country, and those who remained in Iran had to travel within themselves’,Footnote 21 by using drugs.
The presence of young people in the public space had become dominant and, in the teeth of the moral police (gasht-e ershad) and the reactionary elements within the clergy, exuberantly active. The fields of music, cinema, arts and sports boomed during the late 2000s and physically encroached into the walls and undergrounds of Iran’s main cities. The examples provided by Bahman Ghobadi’s No one knows about Persian cats (winner of the Un Certain Regard at Cannes) and the graffiti artist ‘Black Hand’ – Iran’s Banksy – are two meaningful cases in an ocean of artistic production of globalised resonance.Footnote 22
Considering the sharpening of social conditions, both material and imagined, there was a steady rise in reported cases of depression (dépréshion, afsordegi). Indicative of the growing mental health issue is a report published by the Aria Strategic Research Centre, which claims ‘that 30 percent of Tehran residents suffer from severe depression, while another 28 percent suffer from mild depression’.Footnote 23 Obviously, the increased relevance of depression can be attributed to a variation in the diagnostic capacity of the medical community, as well as to changes and redefinition of the symptoms within the medical doctrine.Footnote 24 Yet, the fact that depression progressively came to occupy the landscape of reference and human imagery of this period is a meaningful sign of changing perception of the self and the self’s place within broader social situations.
The lack of entertainment in the public space has been a hallmark of post-revolutionary society, but its burden became all the more intolerable for a young globalised generation, with expectations of a sophisticated lifestyle, and cultural norms which have shifted in drastic ways compared to their parents. If part of it had been expressed in the materialisation of an Iranized counterculture (seen in the fields of arts and new media), the other remained trapped in chronic dysphoria, apathy and anomie, to which drug use was often the response. The prevalence of depression nationwide, according to reports published in 2014, reaches 26.5 per cent among women and 15.8 per cent among men, with divorced couples and unemployed people being more at risk.Footnote 25 In a post-conflict context, characterised by recurrent threats of war (Israeli, US military intervention), the emergence of depressive symptoms is not an anomaly. However, as Orkideh Behrouzan argues, in Iran there is a conscious reference to depression as a political datum, manifested, for instance, in the popular expression ‘the 1360s (1980s) generation,’ (daheh shasti) as the ‘khamushi or silenced generation’ (nasl-e khamushi).Footnote 26 The 1980s generation lived their childhood through the war, experienced the post-war reconstruction period and the by-products of the cultural revolution, while at the same time gained extensive access – thanks to the unintended effects of the Islamic Republic’s social policies – to social media, internet and globalised cultural products.
An event that may have had profound effects on the understanding of depression among Iranian youth is the failure of achieving tangible political reforms following the window of reformism and, crucially, in the wake of the protests of the 2009 Green Movement. The large-scale mobilisation among the urban youth raised the bar of expectations, which clashed with the state’s heavy-handed security response, silencing of opponents and refusal to take in legitimate demands. In this, the reformists’ debacle of 2009 was a sign of a collective failure justifying the self-diagnosis of depression by the many expecting their actions to bear results.
In 2009, Abbas Mohtaj, advisor to the Ministry of Interior in security and military affairs said, ‘joy engineering [mohandesi-ye shadi] must be designed in the Islamic Republic of Iran, so that the people and the officials who live in the country can appreciate real happiness’. He then carefully added that ‘of course, this plan has nothing to do with the Western idea of joy’.Footnote 27 His call was soon echoed by the head of the Seda va Sima (Islamic Republic of Iran Broadcasting) Ezatollah Zarghami, who remarked about the urgency of these measures for the youth.Footnote 28 The government had since then relaxed the codes of expression in the radio, allowing satirical programmes (tanz), perhaps unaware of the fact that political jokes and satire had already been circulating via SMS, social media and the internet, in massive amounts. More extravagantly, the government called for the establishment of ‘laughter workshops’ (kargah-e khandeh), somehow remindful of the already widespread classes of Laughter Yoga in Tehran’s parks and hiking routes.
‘People should have real joy [shadi-ye vaqe’i]’, specified an official, ‘and not artificial joy [masnu’i] as in the West’.Footnote 29 Yet, more than ever before, Iranians ventured to trigger joy artificially, notably by using drugs, medical or illegal ones. Auto-diagnosis, self-care and self-prescription had become the norm among the population, preluding to a general discourse towards medicalisation of depression and medicalised lifestyles. With antidepressants being the most prescribed drugs and 40 per cent of Iranians self-prescribing,Footnote 30 one can infer the scope of this phenomenon and, particularly, its relevance on drug policy. The appearance of dysphoria and apathy, regardless of generational divide, is also manifested in the spectacular expansion of the professional activities of mental health workers, specifically, psychotherapists, whose services are sought by ever-larger numbers of people, although mostly belonging to the middle and upper classes.Footnote 31 Examples of depressive behaviour have often been connected to drug (ab)use. The expansion of Narcotics Anonymous (mo’tadan-e gomnam, aka NA, ‘en-ay’), and its resonance with the larger public, exemplified the transition that social life, individuality and governmentality were undergoing.
Other manifestations of this new ‘spirit of the time’ encompassed addictive behaviours more broadly. For instance, groups such the Anjoman-e Porkhoran-e Gomnam (Overeaters Anonymous Society), which appear as a meeting point for people suffering from compulsive food disorders, are on the rise with more than eighteen cities operating self-help groups.Footnote 32 Similarly, sex addiction surfaced as another emblematic phenomenon. In the prudish public morality of Ahmadinejad’s Islamic Republic, there were already medical clinics treating this type of disorder.Footnote 33 A Shiraz-based psychiatrist during the 2013 MENA Harm Reduction Conference in Beirut surprised me when he said that a large number of people had been seeking his help for their sex addiction and compulsive sex, both in Shiraz and Tehran. This, he argued, was in part caused by the increasing use of amphetamine-type stimulants, which artificially arouse sexual desire, but was also a sign for the displacement of values in favour of new models of life, often inspired by commercialised products, such as films, pornography, advertisements and social media.Footnote 34
Alcoholism, too, has been acknowledged by the government as a social problem. Today there are branches of Alcoholics Anonymous (AA) in Iran and rehab centres for alcoholism, despite alcohol remaining an illegal substance, the consumption of which is punished severely. Beyond the diagnostic reality of these claims, it is undeniable that these changes occurred particularly during the years when president Ahmadinejad and his entourage were in government. Indeed, many of the policies and laws in relation to controversial issues, such as on transsexuality and alcoholism, took form during the post-reformist years.Footnote 35 These transformations occurred not as a consequence of the government’s performance and vision, but rather as a rooting and continuation of secular, global trends, many of which began during the reformist momentum, to which, awkwardly but effectively, the populist government concurred. This was a new mode of political and social change, one that could be called reforms after reformism. Once again, a counter-intuitive phenomenon was at play.
The ‘Crisis’ of Shisheh and Its Narratives
If one combines the widespread use of antidepressant drugs with the impressive rise in psychoactive, stimulant and energizing drugs, most notably shisheh, the picture inevitably suggests a deep-seated transformation in the societal fabric and cultural order during the post-reformist era.Footnote 36
In early 2006, officials started to refer to the widespread availability of psychoactive, industrial drugs (san’ati) through different channels, including satellite TVs and the internet.Footnote 37 They said they had little evidence about where these substances originated from and how they were acquired.Footnote 38 Although ecstasy – and generally ATSs – had been available in Iran for almost a decade, its spread had been limited to party scenes in the urban, wealthy capital.Footnote 39 The appearance of methamphetamines (under the name of ice, crystal, and most notably, shisheh, meaning ‘glass’ in reference to the glass-like look of meth) proved that the taste for drugs among the public was undergoing exceptional changes, with far-reaching implications for policy and politics.Footnote 40
The most common way to use meth is to smoke it in a glass pipe in short sessions of few inhalations. It is an odourless, colourless smoke, which can be consumed in a matter of a few seconds with very little preparation needed (Figure 6.1). In one of the first articles published about shisheh in the media, a public official warned that people should be careful about those offering shisheh as a daru, a medical remedy, for lack of energy, apathy, depression and, ironically, addiction.Footnote 41 By stimulating the user with an extraordinary boost of energy and positive feelings, shisheh provided a rapid and, seemingly, unproblematic solution to people’s problems of joy, motivation and mood. Its status as a new drug prevented it from being the object of anti-narcotics confiscation under the harsh drug laws for trafficking. After all, the official list of illicit substances did not include shisheh before 2010, when the drug laws were updated. Until then the crimes related to its production and distribution were referred to the court of medical crimes, with undistressing penalties.Footnote 42

Figure 6.1 Meanwhile in the Metro: Man Smoking Shisheh.
The limited availability of shisheh initially made it too expensive for the ordinary drug user, while it also engendered a sense of classist desire for a product that was considered ‘high class [kelas-bala]’.Footnote 43 As such, shisheh was initially the drug of choice among professionals in Tehran, who in the words of a recovered shisheh user, was used ‘to work more, to make more money’.Footnote 44 Yet after its price decreased sensitively (Figure 6.2), shisheh became popular among all social strata, including students and women, as well as the rural population. By 2010, it was claimed that 70 per cent of drug users were (also) using shisheh and that the price of it had dropped by roughly 400 per cent compared to its first appearance in the domestic market.Footnote 45 It was a ‘tsunami’ of shisheh use which took both state officials and the medical community unprepared, prompting some of the people in the field to call for ‘the creation of a national headquarters for the crisis of shisheh’, very much along the lines of the ‘headquartisation’ mentality described in the early post-war period.Footnote 46 This new crisis within the field of drug (ab)use was the outcome of a series of overlapping trends that materialised in the narratives, both official and among ordinary people, about shisheh. The narrative of crisis persisted after 2005 in similar, or perhaps more emphatic, tones.

This new substance differed significantly from previously known and used drugs in Iran. In contrast to opium and heroin, which tended ‘to break the spell of time’ and diminish anxiety, stress and pain, making users ultimately nod in their chair or lie on the carpet, methamphetamines generally boost people’s activities and motivate them to move and work, eliminating the need for sleep and food.Footnote 47 In a spectrum inclusive of all mind-altering substances, to put it crudely, opiates and meth would be at the antipodes. All drugs and drug use, wrote the French philosopher Gilles Deleuze, have to do with ‘speed, modification of speed … the times that become superhuman or subhuman’.Footnote 48 Shisheh had to do with time, people’s perception of time’s flow; it was the new wonder drug of the century, with its mind-altering speed and physical rush as distinctive emblems of (post)modern consumption.
Opiates derive from an agricultural crop, the poppy, whereas methamphetamines are synthetized chemically in laboratories and therefore do not need agricultural land to crop in. Between 2007 and 2010, Iran topped the international table of pseudoephedrine and ephedrine legitimate imports, with quantities far above expected levels according to the International Narcotics Control Board (INCB).Footnote 49 Pseudoephedrine and ephedrine are both key precursors for meth production, the rest of the chemical elements being readily available in regular stores and supermarkets. With Iran’s anti-narcotic strategy heavily imbalanced towards its borders with Afghanistan and Pakistan, the production of shisheh could occur, with few expedients and precautions, ‘at home’. In fact, it did not take long before small-scale laboratories – ante tempore versions of Walter White’s one in Breaking Bad – appeared within borders, inducing the head of the anti-narcotic police to declare, ‘today, a master student in chemistry can easily set up a laboratory and, by using the formula and a few pharmaceutical products, he can obtain and produce shisheh’.Footnote 50 In 2010, the anti-narcotic police discovered 166 labs, with the number increasing to 416 labs in 2014.Footnote 51 The supply reduction operations could not target domestic, private production of meth, because this new industry was organised differently from previous illicit drug businesses and could physically take place everywhere.
The high demand for meth and the grim status of the job market guaranteed employment in the ‘shisheh industry’.Footnote 52 A ‘kitchen’ owner who ran four producing units in Southern Tehran revealed that the prices of shisheh had shrunk steadily because of the high potential of production in Iran. In his rather conventional words, ‘young chemical engineers, who cannot find a job … work for the kitchen owner at low prices’, and, he adds, ‘precursors and equipment are readily available in the capital’s main pharmaceutical market at affordable prices’.Footnote 53 The shisheh that is produced is sold domestically or in countries such as Thailand under the local name of yaa baa, or Malaysia and Indonesia, where there is high demand for meth. The number of Iranian nationals arrested in international airports in Asia hints clearly at this phenomenon.Footnote 54
Logically, shisheh and the shisheh economy appealed particularly young people, who exploited the initial confusion and lack of legislative norms. At the same time, while opium and heroin had largely remained ‘drugs for men’ (although increasing numbers of women were using them in the early 2000s), shisheh was very popular among women. For instance, the use of shisheh was often reported in beauty salons and hairdressers, allegedly because of its ‘slimming’ virtue. In similar fashion, its consumption was popular among sportsmen, both professional (e.g. football players and wrestlers) and traditional/folkloric (e.g. zurkhaneh).Footnote 55 Its consumption appealed to categories of people enchanted with an idea of life as an hedonistic enterprise often governed by the laws of social competition, something that differed ontologically and phenomenologically from Islamising principles.
Reports emerged also about the use of shisheh among students to boost academic performance. By making it easy to spend entire nights studying and reviewing, especially among those preparing for the tough university entry examination (konkur), shisheh had gained popularity in high schools and universities. The shrinking age of drug use, too, has been factual testimony of this trend.Footnote 56 In an editorial published in the state-run newspaper, a satirist announced that, in Iran, ‘the modern people have become post-modern. And this latter, we know, is industrial and poetical’ and he longed for ‘the old good days of the bangis [the hashish smoker]’.Footnote 57 Shisheh epitomised the entry into the post-modern world, an epochal, perhaps irreversible, anthropological mutation. In view of this changing pattern of drug (ab)use, the authorities realised, slowly and half-heartedly, that the policies in place with regard to treatment of injecting drug users – harm reduction as implemented up until then – had no effect on reducing the harm of shisheh. Harm reduction could not target the ‘crisis’ of shisheh, which unwrapped in a publicly visible and intergenerational manner different from previous drug crises. Its blend, in addition, with changing sexual mannerisms among the youth, aggravated the impotence of the state.Footnote 58
Sex, Sex Workers and HIV
With drug use growing more common among young people and adolescents, people acknowledged shisheh for its powerful sexually disinhibiting effects, which, in their confessions during my ethnographic fieldwork, ‘made sex [seks] more fun [ba hal] and good [khoob]’. Equally, the quest for sex with multiple partners sounded appealing to those using shisheh, engendering the preoccupation (when not the legal prosecution) of the state. With moral codes shifting rapidly and the age of marriage rising to 40 and 35 respectively for men and women, pre-marital unprotected sex became a de facto phenomenon.Footnote 59
The combination of sex and drugs resonated as a most critical duo to the ears of policymakers, one that made Iran look more like a land of counterculture than an Islamic republic. Yet, because premarital sex was deemed unlawful under the Islamic law, the issue of sex remained a much-contested and problematic field of intervention for the state. Despite the repeated calls of leading researchers, the state institutions seemed incapable, if not unprepared, to inform and to tackle the risk of pre-marital unprotected sex. This attitude accounted, in part, for the ten-fold increase in sexually transmitted diseases in the country during the post-reformist period.Footnote 60
Many believed that while harm reduction policies were capable of tackling the risk of an HIV epidemic caused by shared needles, these measures were not addressing the larger part of the population experiencing sexual intercourse outside marriage (or even within it), with multiple partners, and without any valuable education or information about sexually transmitted diseases. The director of the Health Office of the city of Tehran put it in this statement during a conference, ‘we are witnessing the increase in sexual behaviour among students and other young people; one day, the nadideh-ha [unseen people] of today will be argument of debate in future conferences’.Footnote 61 The rate of contagion was expected to increase significantly in the years ahead, a hypothesis that was indeed confirmed by later studies.
As for the risk of HIV epidemics emerging from Iran’s unseen, but growing population of female sex workers, the question was even more controversial. Sex workers, in the eye of the Islamic Republic, embodied the failure of a decadent society, one which the Islamic Revolution had eradicated in 1979, when the revolutionary government bulldozed the red-light districts of Tehran’s Shahr-e Nou to the ground and cleansed it – perhaps superficially – of prostitutes and street walkers.Footnote 62 Government officials had remained silent about the existence of this category, with the surprising exception of Ahmadinejad’s only female minister Marzieh Vahid-Dastjerdi. The Minister of Health and Medical Education broke the taboo publicly stating in front of a large crowd of (male) state officials, ‘every sex worker [tan forush, literally ‘body seller’] can infect five to ten people every year to AIDS’.Footnote 63 The breaking of the taboo was a part of the attempt to acknowledge those widespread behaviours that exist and that should be addressed with specific policies, instead of maintaining them in a state of denial.Footnote 64 The framing of the phenomenon rested upon the notion of ‘risk’, ‘emergency’ and crisis. The opening of drop-in centres for women was a step in this direction, albeit initially very contested by reactionary elements in government. In 2010, the number of these centres (for female users) increased to twelve, the move being justified by the higher risk which women posed to the general population: ‘a man who suffers from hepatitis or AIDS can infect five or six persons, while a woman who injects drugs and makes ends meet through prostitution may infect more persons’.Footnote 65
The government, however, remained unresponsive to this call. Mas‘ud Pezeshkian – former Minister of Health under the reformist government (2001–5) – commented that ‘until the profession [of sex worker] is unlawful and against the religious law [shar’] there should be no provision of help to these groups’.Footnote 66 The result of this contention was a lack of decision and coherence about the risk of an HIV epidemic. According to an official report, the majority of groups at risk of sexual contagion (e.g. sex workers, homeless drug users) were still out of reach of harm reduction services.Footnote 67 If drug users in prison embodied the main threat (or crisis) during the reformist period, the post-reformist era had been characterised by the subterfuge of commercial sex and unprotected sexual behaviour, with the incitement of stimulant drugs such as shisheh.
A study published by Iran’s National AIDS Committee within the Ministry of Health and Medical Studies – with the support of numerous international and national organisations – revealed that only a small percentage (20 per cent) of the population between fifteen and twenty-four years old could respond correctly to questions on modes of transmission, prevention methods and HIV.Footnote 68 The crisis of this era was propelled, one could say, through sex, but also based on a certain ignorance of safe sexual practices, because of unbroken moral taboos.Footnote 69
The Disease of the Psyche
The changing nature of drug (ab)use and sexual norms – in the light of what I referred to as the broad societal trends of the post-reformist years – rendered piecemeal and outdated the important policy reforms achieved under the reformist mandates. In fact, shisheh could not be addressed with the same kind of medical treatment used for heroin, opium and other narcotics. Treatment of shisheh ‘addiction’ required psychological and/or psychiatric intervention, with follow-up processes in order to guarantee the patient a stable process of recovery.Footnote 70 This implied a high cost and the provision of medical expertise in psychotherapy that was lacking, and already overloaded by the demand of the middle/upper classes. Besides, methadone use among drug (ab)users under treatment engendered a negative side effect in the guise of dysphoria and depression, which could only partially be solved through prescription of antidepressants. The recurrence to shisheh smoking among methadone users in treatment became manifest, ironically and paradoxically, as a side effect of methadone treatment and a strategy for chemical pleasure.Footnote 71
The mental hospitals were largely populated by drug (ab)users, the majority of whom with a history of ‘industrial drugs’ use, a general reference to shisheh.Footnote 72 The rise in referrals for schizophrenia, bipolar disorder, suicidal depression and other serious mental health issues needed to be contextualised along these trends. Suicide, too, remained a problematic datum for the government as it revealed the scope of social distress and mental problems emerging publicly.Footnote 73 But the increase of shisheh use markedly brought the question of drugs into the public space, with narratives of violence, family disintegration, abuse and alienation becoming associated with it. Although drug scares have always circulated in Iran (as elsewhere), they have mostly regarded stories of decadence, overdose, and physical impairment. They rarely concerned schizoid and violent behaviour in the public. With shisheh, drug use itself became secondary, while the issue of concern became the presence of highly intoxicated people, with unpredictable behaviours, in the public space.Footnote 74 As a law enforcement agent in the city of Arak confessed, ‘the heroini shoots his dose and stays at his place, he nods and sleeps; these people, shishehi-ha [‘shisheh smokers’], instead, go crazy, they jump on a car and drive fast, like Need 4 Speed,Footnote 75 they do strange things [ajib-o gharib] in the streets, talk a lot, get excited for nothing, or they get paranoid and violent’.Footnote 76 With this picture in mind, it does not surprise that Iran has had the world’s highest rate of road accidents and bad driving habits.Footnote 77 The trend of road accidents became also an issue of concern to the public (and the state), in view of investigations revealing, for instance, that ‘20 per cent of trucks’ drivers are addicted’, or that ‘10 per cent of bus drivers smoke shisheh with risks of hallucination and panic’ while behind the wheel.Footnote 78 Stories emerged also about violent crimes being committed by people on shisheh, establishing a worrying association between this substance, violent crimes (often while in a paranoid state) and, ultimately, long-term depression and mental instability.Footnote 79 More than being a sign of a material increase in violence, these stories are telling about the framing of this new substance under the category of crisis and emergency.
At the same time, shisheh became a cure for depression and lack of energy, also overcoming the urban–rural divide. I had confirmation of this more than once during my time spent in a small village in central Iran between 2012 and 2015. The shepherd known to my family since his adolescence, one night arrived in his small room, prepared some tea and warmed up his sikh (short skewer) to smoke some opium residue (shireh) which he had diligently prepared in the preceding weeks. One of the workers from a nearby farm, a young man of around twenty, came in and after the usual cordial exchanges, sat down, took his small glass pipe and smoked one sut of shisheh.Footnote 80 After their dialogue about the drop in sheep meat price in the market, the shepherd asked for some advice, ‘you see, it has been a while I wanted to give up opium, because you know it’s hard, I have smoked for thirty years now, and I feel down, without energy [bi hal am] all the time. Do you think I should put this away [indicating the opium sikh] and instead try shisheh?’.Footnote 81
In this vignette, the use of shisheh represents a response to the search for adrenaline, libido and energy in the imaginatively sorrowful and melancholic timing of rural life. Many others, unlike my shepherd friend, had already turned to shisheh in the villages, whether because of its lower price, its higher purity or opium’s adulterated state.Footnote 82 The government invoked the help of the Village Councils – a state institution overseeing local administration – in an attempt to gain control over Iran’s vast and scattered villages, but with no tangible results, apart from sporadic anti-narcotics campaigns.Footnote 83 By the late 2000s, drug adulteration (especially opium) increased substantially, encouraging drug users to shift to less adulterated substances – for example, domestically produced shisheh – or to adopt polydrug use. This caused a spike in the number of drug-related deaths, up to 2012, due principally to rising impurity (Figure 6.3).Footnote 84 The cost of using traditional drugs like opium and heroin was becoming prohibitive and less rewarding in terms of pleasure. Inevitably, many shifted to shisheh.

Figure 6.3 Drug-Use-Related Deaths
Conclusions
The phenomenon of drug use intersected over this period with long-term transformations that had bubbled below the surface of the governmental rhetoric and imagery of the Islamic Republic. Changing patterns of drug consumption, hence, was not the simple, consequential effect of new drug imports and lucrative drug networks, although these played their role in facilitating the emergence of new drug cultures. From the late 2000s onwards, drugs affected, and were affected by, broader trends in society, such as changing sexual norms, consumption patterns, social imagination, economic setting and ethical values. This represented a fundamental ‘anthropological mutation’, for it changed the way individuals experienced their existences in society and shaped their relation to the surrounding world. By this time, new cultural, ethical values gained traction, relegating to the past the family-centric, publicly straight-laced way of being in the world. The pursuit of sensorial pleasure, personal recognition and aesthetic renewal became totalizing – and totalitarian – in more rooted and uncompromising ways than the clerical ideology preached by the ruling class in the Islamic Republic. Not the ideology of the clergy, but the driving force of post-modern consumerism was the totalitarian drive of social change. To this epochal moment, the state responded haphazardly and incongruently, mostly unaware or unconcerned of what this transformation signified and in what ways it manifested new societal conditions where the old politics and rhetoric had effect. Rather than attempting a reconfiguration of the new cultural, social and ethical situation, the political order coexisted with the coming of age of new subjectivities, without recognizing them effectively.
Drugs, and shisheh in particular, were a manifestation of the profound changes taking place over this period to which the state reacted with hesitation and through indirect means. This chapter focused on social, cultural and human (trans)formations from the mid 2000s onwards, with an especial attention to the rise of shisheh consumption and its contextual psychological, sexual and economic dimensions. The next two Chapters dwell on how the state countered this changing drug/addiction phenomenon. An emblem of the anthropological mutation in lifestyle, imagery, values and flow of time, shisheh contributed to the change in political paradigm with regard the public place. It also brought about a shift in drug (ab)use and in the governance of drug disorder. Shisheh, hence, is both cause and effect of these transformations.
Introduction
One hot morning of early September 2014, Tehran’s University of Medical Sciences hosted the Eighth International Congress on Addiction Science. The venue was that of important scholarly events – the Razi (Rhazes) Conference Hall – located near the symbol of modern Tehran, the Milad Tower. A lively movement of people, mostly young students, male and female, animated the premises of the building, where the registration procedures and distribution of materials of various kinds, including breakfast, was taking place. One could tell, prima facie, that the schedule was expected to be dictated by some high-ranking, prominent participation, particularly among government officials.
The conference, an attendant involved in the organisation revealed to me, was meant to be ‘a new start’ for Iran’s drug policy and the academic community, especially in its engagement with its Western counterparts. The conference panels narrated the underlying dynamics within the policy community, in the wake of the eclipse of the post-reformist government. As such, the conference was a telling vignette of the features and apparent paradoxes of post-reformist drug policy.
At 8AM, I had successfully snuck into a panel on ‘Women and Addiction’, which occurred behind closed doors; if truth be told, I had to use my network in the UNODC to get access to the room where a female ministerial advisor did not want her statements to be reported publicly. The audience was almost entirely composed of women whose stricter type of hijab was telling of their employment post in state institutions. Despite the novelty of the issues debated in the panel, with off-the-records data being revealed, after the second presentation my attention drifted to a concomitant panel in Hall 3, titled ‘Harm Reduction among Drug Users’.
Since this panel included influential officials in the policy community and well-known advocates of harm reduction, it seemed a (political) manifestation not to be missed. I left the panel on Women and Addiction and moved to the opposite room where the panel on Harm Reduction was taking place. On this panel were prominent members of the policy community from different ministries and the DCHQ, plus a number of high-ranking officials in the audience. The presenters were Dr Ahmad Hajebi, Director of Mental Health Office at the Ministry of Health; Dr Mehdi Guya, Director of the Centre of Infectious Diseases at the Ministry of Health; and Farid Barrati-Sadeh, Director of Treatment at the DCHQ.
Despite the friendly tone of the exchanges, one could sense the latent animosity between the participants. As the panel contemplated a Q&A session, the comments remained mostly cursory, provocative and colourful. But the last speaker, Farid Barrati-Sadeh, an outspoken official with regular presence in the media, opted to use the time allocated for his presentation in order to, as he said, ‘clarify and point out some of the contradictions in the exposition of our friends’. From the very outset of his presentation, the speaker remarked that the current implementation of drug laws was not only haphazard and fragmentary, but also contradictory in itself. This, he argued, was due to the lack of interest of his ‘friends’ in the Ministry of Health, who were ‘unwilling to engage with harm reduction and keep on criticising the setad [i.e. DCHQ] for every problem in this country’. Raising the tone of his voice, he accused the other speakers who preceded him, Dr Mehdi Guya and Dr Ahmad Hajebi, ‘of refusing to adopt new protocols for the new treatment camps under the 2010 law’, a law approved by the ‘organs of the Islamic Republic and has the authoritative support of the Leader of the Revolution’, that is to say Ayatollah Khamenei. Comments of disapproval could be heard from the front line of the conference hall, where the other speakers sat. The presentation of the DCHQ official extended in a quid pro quo with the other speakers, with mutual accusations of incoherence, hypocrisy and managerial unwillingness/incapacity. It then terminated when Minoo Mohraz, Iran’s internationally prominent HIV/AIDS scholar, intervened on the panel floor, taking the microphone away from one of the speakers and, with severity, reprimanding all the panellists about their rowdy behaviour and ‘their inconclusive messiness’.Footnote 1 She then remarked that
as a person who is not ejrai [executive, i.e. a public official] – I am a scientist [adam-e ‘elmi] – I have duties towards the people, whatever you want to say and discuss about, I ask you to sit together and discuss. People cannot bear this anymore … I ask you to solve this and to support harm reduction; … use the budget to promote useful programmes, not to establish compulsory treatment camps [kamp-e darman-e ejbari].
For an external viewer, the contest might appear one centred around budgetary allocations between different state institutions entrusted with harm-reduction duties. It soon became explicit, however, that budgetary discussions were only a side note on the more equivocal and vexed page of ‘compulsory treatment’ and the ‘camps’ in general.
The 2010 Drug Law Reform
The roots of the diatribe among the panellists went back to the text of the 2010 drug law reform. This reform, approved after long and complex negotiations within the Expediency Council, emblematised the developments with regard to drug (ab)use under the presidency of Mahmud Ahmadinejad. The conference debates, although taking place after the demise of Ahmadinejad, actually concentrated on the experiences of the last government. In a way, the debate itself was taking place so overtly – and loudly – because of the political change represented by the election of Hassan Rouhani in 2014, which had resulted in a lost grip on the institutional line of command within the policymaking institutions. Criticism was accordingly welcomed as a sign of renewal, even when the people in charge at a bureaucratic level remained, largely, the same.
The 2010 law reform materialised the inherent idiosyncrasies of the politics of drugs in the twenty-first century. The law itself provides a localised example of the paradigm of government with regard to the crises that the post-reformist governments had faced. Post-reformism reflects the scenario left by the demise of governmental reformism following Khatami’s last presidential term and its unsuccessful efforts at triggering political reform. Under the umbrella of post-reformism, I indicate those attempts at governance which fall short of calling overt reforms, but which produce diffused changes within political practice. It encompasses ideologically strong administrations calling for a revolution in government while instilling a grassroots form of management of social and political conflicts (i.e. Ahmadinejad); as well as centrist, business-oriented administrations pledging moderate, slow and timidly progressive civic change (i.e. Rouhani).
The year 2010 was momentous in formulating a new approach, called post-reformism, regarding illicit drugs. Discussions of the new anti-narcotic laws were ongoing and, as the country had already built the infrastructure for large-scale interventions, the new political formula had the potential to be ground-breaking. Instead, the text of the 2010 reform of the anti-narcotic law reproduced the multiple ambiguities of harm reduction (and public policy generally) in Iran, the law itself becoming the contested ground between different governmentalities towards what was defined ‘addiction’, as partly manifested in the diatribe reported at the beginning of this Chapter. It was an oxymoronic law producing oxymoronic governance.
Apart from updating the list of narcotic drugs with the insertion of new synthetic, industrial drugs, notably shisheh, the key changes in the new texts concerned Article 15 and Article 16.
Abstract from the 2010 Drug Law Reform
Article 15 – The addict is required to refer to legitimate state [dowlati], non-state [gheyr-e dowlati], or private [khosusi] centres, or to treatment and harm reduction grassroots organisations [sazman-ha-ye mardom-nahad], so to apply to addiction recovery. The addict who enrols in one of the above-mentioned centres for his/her treatment and has obtained an identification [gavahi] of treatment and harm reduction, as long as he/she does not publicly manifest addiction [tajahor be e‘tyad], is suspended [mo‘af] from criminal sanctions. The addict, who does not seek treatment of addiction, is a criminal.
Note 2 – The Ministry of Welfare and Social Security is responsible … to cover the entire expenses of addiction treatment of destitute [bi-beza‘at] addicts. The government is required to include this in the yearly sections of the budget, and to secure the necessary financial credits.
Article 16 – Addicts to narcotic drugs and psychoactive substances, included in Articles 4 and 8, who do not have the identification mentioned in Article 15 and who are overtly addicted, must be maintained, according to the decision of the judicial authority, for a period of one to three months in a state centre licenced with treatment and harm reduction. The extension of the maintenance period is permitted for a further three months. According to the report of the mentioned centre and based on the opinion of the judicial authority, if the addict is ready to continue treatment according to Article 15, he/she is permitted to do so according to the aforementioned article.
Note 2 – The judicial authority, for one time, can suspend the sanction against the addict for a six-month period, given appropriate guarantees and the allocation of an identification document mentioned in Article 15, and can refer the addict to a centre as enunciated in this aforementioned article. The aforementioned centres are responsible to send a monthly report on the trend of treatment of the addict to the judicial authority, or to his representative …
Note 3 – Those contravening the duties enunciated in Note 2 of this article can be condemned to incarceration from one day to six months.Footnote 2
Several issues emerge from analysing these two articles. First, the 2010 reformed law legitimised harm-reduction practices applied since the early 2000s, including them in an institutional legal order. The law explicitly mentions the legitimacy of ‘harm reduction’, although it does not specify what falls under this label. Second, the law institutes centres for the implementation of harm reduction; these centres, it is spelled out, include both state centres and private clinics, as well as charitable and grassroots organisations. In other words, Article 15 of the 2010 law legitimises those agents already active in the field of drug (ab)use, explicating their social role with regard to addiction. It enshrines their function according to what I define in the Chapter 8, the governmentalisation of addiction. More crucially, the 2010 law establishes a distinction between those drug (ab)users who are willing to seek treatment and refer to a recognised institution (e.g. clinic, camp), as contemplated in Article 15, and those who do not seek treatment, who therefore become subject to Article 16. This has two main effects: on the one hand, the new law protects registered addicts since it provides them an identification card, allowing them to carry limited quantities of methadone with them – in the case of MMT patients – or to seek harm reduction treatment – in the guise of clean syringes and needles – without the risk of police arrest. On the other hand, those addicts who do not register for treatment in a recognised institution, are still liable of a crime – the everlasting crime of addiction – and could be forcibly sent to state-run compulsory camps (kamp-e maddeh-ye 16). Their crime is that of being intoxicated in a visible manner, publicly (tajahor).
Concomitant to the new law, governance of drug consumers adopted new analytical frames, which follow the logic of what I define oxymoronic governance. Drug (ab)users were now described and treated as ‘patient criminal [mojrem-e bimar]’ who, if not under treatment, ‘will be object a court ruling on compulsory treatment, to which the police will enforce a police-based treatment [darman-e polis-madar]’.Footnote 3 What was formerly a criminal – and perhaps the emblem of a criminal – the ‘addict’, is now a patient whose crime resides in his condition, his dependency to an illegal substance. This new subjectivity is the object of institutional care, not through the expertise of medical professionals alone, as would be for other patient types, and not through the whip of policemen, as would occur for simple criminals. Dealing with the drug (ab)user produces a new figure within state law and order, that of the therapeutic police, a force which treats disorder of an ambivalent kind. This enmeshment of criminalisation and medicalisation provides a cursory glance at the new governmentality under post-reformism. By adopting a medical lens, through a law-and-order approach, the therapeutic police is where policing encounters addiction. Its means are, from a practical point of view, in continuity with orthodox policing. ‘Quarantine’, used during the 1980s, came back into vogue when officials addressed the need to isolate risky groups, such as IDUs and HIV-positive individuals.Footnote 4 Quarantine, a quintessential medical practice with mandatory enforcement, was not a metaphorical hint, but an actual practical disposition. Police and medicine needed cooperation, at close range, on the matter of drugs. This new mode of intervention was rooted in the framing of the addict as a mojrem-e bimar, a ‘patient-criminal’, who needed to be countered by a ‘therapeutic police’.
In line with the post-reformist vision based on the ‘therapeutic police’ and governmentalisation of addiction, the new law contemplated direct intervention in tackling addiction, by forcing into treatment those who were reluctant, or unable, to do so. If, at the level of political discourse, the new drug law was characterised by the concomitance of insoluble traits (i.e. assistance and punishment), it did not mean that its practical effects were totally unintended. While addiction was publicly recognised as a ‘disease’ and medical interventions were legitimated nationwide through public and private clinics, the figure of the drug (ab)user remained inherently deviant and stigmatised among the official state cadre, especially when connoted with the disorderly – and dysfunctional – features of poverty and social marginalisation. The law intended to manage disorder instead of bring about order; to govern crisis instead of re-establishing normalcy, whatever the content of the latter proved to be.
The provisions of the law seem to respond, among other things, to the necessities dictated by the expanding crisis of shisheh in the public space as described in Chapter 6. Public officials during the late 2000s seemed to agree that people abusing methamphetamines could not be cured, or that a cure for them was either unavailable or too expensive to be provided on a large scale.Footnote 5 This persuaded cadres of the state to seek mechanisms of intervention that were not necessarily coherent with each other, but which, from a public authority perspective, responded to the imperatives of public order. In other words, they adopted an oxymoronic form of politics, the adoption of otherwise incompatible means.
The text of Article 16 stresses the need to intervene against ‘those addicted publicly’. It envisions public intervention vis-à-vis the manifest effects of drug use, materialised by disorderly presence in the streets, noisy gatherings of drug users, vagrancy and mendicancy.Footnote 6 This interpretation of the shisheh ‘crisis’ was rooted on a law enforcement model, updated with a new medical persuasion – that of the incurability of shisheh addiction.Footnote 7 Since methadone substitution programmes and classical harm-reduction practices (i.e. needle exchange) were inadequate to respond to the treatment of shisheh users, the state resorted to a practice of isolation and confinement, this time, however, not through incarceration in state prisons. Instead, it gave birth to a new model, that of the compulsory state-run camps, a paradigm of government of the drug crisis that exemplified, in nuce, the post-reformist governmentality on crisis.
Therapeutic Police: Compulsory Treatment Camps
Part of the diatribe portrayed in the conference vignette opening this chapter reflected the opposing views existing on the role of the therapeutic police and the status of compulsory treatment camps. Since the implementation of the 2010 reform – but to a minor degree since Ahmadinejad’s election in 2005 – the state regularly intervened to collect homeless drug users and confine them to compulsory camps, much to the astonishment of those who had worked towards the legitimation of harm reduction.Footnote 8 In reality, part of the medical community and NGO sector – notably the NGO Rebirth (Tavalod-e Dobareh) – had supported the text of the 2010 law on the basis that it recognised the legitimacy of treatment and harm reduction, as a prelude towards decriminalisation of addiction. Compulsory treatment camps, supporters of the 2010 law argued, were the necessary venue to medicalise addiction among those who could not be persuaded to seek treatment. It would be, they added, the safest and fastest way to introduce the addict into the cycle of treatment, facilitating recovery.Footnote 9 Yet, therapeutic policing relied on a system which paid little attention to recovery. Centres managed by law enforcers often unveiled situations of degradation and abuse, which prompted several officials to publicly express their opposition to this model, on the grounds that it neither brought results, nor offered humanitarian support.Footnote 10
Operating since the late 2000s, compulsory treatment camps have been active in sixteen regions. Although the media and officials refer to them as ‘camps’, the official name for them, hitherto, has been ordugah, which translates in English as ‘military camp’. One official lambasted the use of this term as ‘unappreciative’ of the government’s effort to treat drug addicts.Footnote 11 The origins of this institutional model can be traced back to the early years of the Ahmadinejad government.Footnote 12 Their purpose, however, became antithetical to the original idea. In 2007, the new head of the DCHQ, C-in-C Ahmadi-Moghaddam, already announced that ‘the addict must be considered a patient-criminal [mo‘tad-e mojrem] who, if he is not under treatment, the court will rule for him compulsory treatment [darman-e ejbari] and the police will be the executor of a police-based treatment’. He then added, ‘we have to build maintenance camps [ordugah-e negahdari]; the NAJA has already built camps for the homeless and vagrants, which in the opinion of treatment officials can be used as maintenance camps for addicts for a certain period’.Footnote 13 This announcement is an ante tempore elucidation of the 2010 law model. It coincided with the appointment of the head of the police as director of the DCHQ. The fact that, genealogically, the compulsory treatment camps were formerly camps for the internment of vagrants and homeless people, unveiled the primary concern of the state regarding the management of public order.Footnote 14
Much like the 1980s, the officials adopted a language that underlined the need to ‘quarantine’ problematic drug (ab)users.Footnote 15 Yet, this rhetoric did not prelude to a return to past forms of intervention; the post-reformist ‘quarantine’ envisaged the presence and ‘supervision of doctors, psychologists, psychiatrists and infection experts as well as social workers’ and the referral, after the period of mandatory treatment, to ‘the non-state sector, NGOs and treatment camps’.Footnote 16 The rationale, it was argued, was to introduce so-called dangerous addicts and risky groups into the cycle of treatment, the first of which was managed by the state, through the therapeutic police, while afterwards it was outsourced to non-state agents, through charities, NGOs and civil society organisations.
The government made large budgetary allocations to the NAJA in furtherance of the construction of compulsory camps. In 2011, 81 billion tuman (equivalent to ca. USD 8 million), were allocated to the Ministry of Interior, to build a major compulsory treatment camp in Fashapuyieh, in the southern area of the capital.Footnote 17 This first camp was designed to inter around 4,000 addicts in the first phase (with no clear criteria of inclusion), with the number going up to 40,000 once the entire camp had been completed.Footnote 18 Other camps were expected to be operating in major regions, including Khorasan, Markazi, Fars and Mazandaran.Footnote 19 A gargantuan project resulted from the implementation of Article 16 of the 2010 law. The deputy director of the DCHQ, Tah Taheri, announced that ‘about 250,000 people needed to be sent to the compulsory treatment camps by the end of the year’ as part of the governmental effort to curb the new dynamics of addiction.Footnote 20 The ambitious plan had the objective of unburdening the prison organisation from the mounting number of drug offenders, a move likely to also benefit the finances of the Judiciary and the NAJA, always overwhelmed by drug dossiers and structurally incapable of proceeding with the drug files.
The nature of the compulsory treatment camps resembled more that of the prison than anything else. Legislation on illicit drugs mandated the separation of drug-related criminals from the rest of the prison population. Authorities failed to implement the plan on a large scale, leaving the prisons filled with drug offenders.Footnote 21 Up to 2010, the prison population had increased to 250,000 inmates, a number that, given the state’s commitment not to incarcerate drug addicts, was symptomatic of an underlying duplicity, or ambivalence, in state intervention.Footnote 22 Mostafa Purmohammadi, a prominent prosecutor, identified ‘addicted prisoners’ as one of the main concerns of the prisons and he advised the implementation of mandatory treatment camps to alleviate the dangers and troubles of the prison system.Footnote 23 Consequently, for the first time in many decades, the prison population decreased by some 40,000 people in 2012, reaching the still cumbersome number of 210,000 inmates. This datum, heralded as evidence of success by the post-reformist government, could be actually traced back to the introduction, on a massive scale, of the compulsory camps for drug (ab)users, managed by the therapeutic police. The actual population confined in state institutions for charges of criminal behaviour (including public addiction), had actually mounted to almost double the size of prisons prior to the 2010s.
Since the establishment of the Islamic Republic, the overall number of prisoners had increased by six times, and the number of those incarcerated for drug-related charges by fourteen times, with one in three court cases allegedly being drug-related in 2009.Footnote 24 If, during the reformist period, the introduction of harm reduction had been prompted, among other things, by the HIV epidemic in prisons, the post-reformist government under Ahmadinejad reacted with outrage against the waste of money that the incarceration of drug offenders represented. An official from the Prison Organisation in 2010 outlined that ‘the maintenance of every prisoner costs 3,000 tuman per day … which is equivalent to a waste of public capital of around 450,000,000 tuman per day’.Footnote 25 Researchers from state institutions demonstrated that treating drug (ab)users would cost an average of fifteen times less than incarcerating them. In view of the ratio of drug (ab)users in prison – an astonishing 70 per cent – the creation of the compulsory treatment camps provided an alternative device for the management of a costly population.Footnote 26 The head of the Judiciary, Ayatollah Sadeq Ardeshir Amoli Larijani, leading member of the conservative faction and brother to the Parliament speaker Ali Larijani, echoed these results, asking for a swift re-settling of ‘addicted prisoners’ in the compulsory camps for the sake of treatment. Compulsory camps, rather than being under the supervision of the Prison Organisation, are managed by the DCHQ.Footnote 27
Out of the conviction that the drug (ab)user population would be relegated to the camps, the Ahmadinejad government suspended the needle exchange programmes in prisons, affirming that ‘the situation [of HIV/AIDS] was under control’.Footnote 28 The assumption among officials became that since drug (ab)users are now referred to compulsory camps, needle exchange has become irrelevant in prisons. At the same time, the government proceeded towards a significant expansion of methadone treatment, bringing more than 40,000 prisoners under treatment by 2014. Methadone, in this regard, represented an acceptable solution, as it was produced domestically, it was readily available through private and public clinics and, last but not least, facilitated greatly – by virtue of its pharmacological effects – the management of unruly subjects, such as drug users, in the problematic contexts of prisons.Footnote 29 In the account of several former drug offenders in prison, the authorities tended to encourage methadone treatment with high doses, without much scrutiny of either the side effects of excessive methadone use, or the internal economy of methadone within the prison.Footnote 30
Inspired by the relative success of its methadone programmes (in prisons, as much as outside), the DCHQ agreed to pilot methadone treatment programmes inside some of the compulsory treatment camps supervised by the NAJA. This, it seems, was identified as a productive way to introduce the highest number of drug addicts into the cycle of treatment, via less harmful drugs such as methadone. By familiarising arrested drug (ab)users to methadone, the authorities sought to maintain them off, allegedly more dangerous drugs, such as heroin. But because the number of methamphetamine users had increased significantly, methadone proved ineffective, and the authorities sought alternatives in the model of the compulsory camps. Based on forced detoxification, these camps treated all drug (ab)use without distinction. Shafaq camp embodied the new model of treatment of drug (ab)use.
In 2010, the government inaugurated the mandatory treatment camp of Shafaq in the village of Shurabad, south of Tehran. The location of this centre sounded familiar to those acquainted with Iran’s history of drugs: during the 1980s, Shurabad had been one of the major collective rehabilitation centres for drug (ab)users, one that was often given focus in media reports. In the 1990s, it was transformed into a female prison, before eventually being abandoned. Its revivification synchronised well with the post-reformist government’s call to bring back the revolutionary principles of the Islamic Revolution, in the spirit of Sadegh Khalkhali and his onslaught against drugs. However, the Shafaq centre did not resemble the old, obsolete structure of the 1980s. It was rebuilt with the objective of instituting a model for other compulsory camps as well as for other non-state rehab camps.
The target population of this camp consisted of marginal drug (ab)users, a fluid category made of poor or pauperised homeless or with instable housing, people visiting or living around the patoqs in Tehran. Shafaq’s management was initially entrusted to retired Colonel Khalil Hariri, a leading commander of Anti-Narcotic Police who had been stationed in the Sistan and Baluchistan region for nine years with the primary duty of fighting drug traffickers.Footnote 31 His appointment revealed the government’s priorities on treatment: a top security official in anti-narcotics acting as director of an addiction treatment centre. In Shafaq, the government allocated ca. 100,000 tuman (ca. USD 8) per treated addict, which officials said would cover the employment of medical and social cadres to supervise recovery, which they expected to last for a three-month period.Footnote 32
The camp of Shafaq operated from early 2010 to late 2012, when a huge scandal broke out bringing its closure. Fifty-three people, rounded up by the police because of their status as ‘public addicts’, had died of chronic dysentery after having spent a few weeks in the camp. Media reported the deaths and several journalists managed to contact people who had previously been inside the camp, unearthing dramatic accounts. The picture that emerged from the reports was gruesome: a single silo with no windows, composed of fourteen rooms on two lines, each occupying fifty beds, with no heating system installed, inadequate sanitary services and insufficient alimentary provisions, the centre soon became the symbol of the state’s inhumane treatment of drug (ab)users.Footnote 33
Overcrowded rooms and the lack of medical personnel added to the ordinary accounts of beatings, mistreatment and abuse by the personnel, including physical violence against elderly individuals.Footnote 34 The use of cages, bars and handcuffs, constant police surveillance, disciplining rules and physical violence exposed, on the one hand, the contrast with the humanitarian and medicalised precepts of harm reduction (Article 15) and, on the other hand, embodied a coercive and securitising strategy based on the management of the margins, perceived as disorderly and chaotic. Dozens of people I encountered in the drug-using hotspots – the patoq – mentioned their experience, or that of their cohorts, in the camp, remarking, not without some pride, the fact they were still alive despite what they had gone through.Footnote 35 Whether their accounts were effectively experienced or empathically imagined, scarcely mattered. In fact, the narratives of Shafaq established a shocking precedent among the population of homeless, pauperised drug (ab)users, which delegitimised governmental interventions on the problematique of addiction, while unwrapping the inconsistencies behind the state’s framing of ‘addiction’ as a medical problem.
Even the work of harm reduction organisations, which had stepped up in supporting the needs of homeless drug users, was negatively affected by the public outcry against Shafaq. Social workers operating in the patoqs had to reassure the drug-user community of their non-involvement in ‘compulsory camps’. In several patoqs, the outreach programmes had to be stopped because of the threat of violence by the patoq’s thugs [gardan-koloft, literally ‘thick-necks’], who feared that strategic information was gathered by the NGOs and sent to the police (an allegation that had some factual evidence, in fact). One man from the Farahzad Chehel pelleh (literally ‘40-steps’) patoq explained me that ‘Shafaq is a place that even the bottom line people [tah-e khatti-ha] cannot bear! And these guys [indicating the outreach team], we don’t trust them, one day they give us syringes, the other day they stare at us when the police comes and brings us to hell!’ Anathema of the homeless drug-using community in Tehran, a young interlocutor of mine would use the metaphor of barzakh to describe Shafaq: the Islamic purgatory, or limbo, whereby one could spend the eternity before the judgement at the end of times.Footnote 36 Intellectually, this image connected with the theological, eschatological meaning of ‘crisis’ as the moment of the ultimate judgment, the moment that decisions take shape regardless of established conventions.
Beside Shafaq, the compulsory treatment camps became sites of risk themselves, with the spread of HIV and other venereal diseases being reported on a number of occasions. For instance, Majid Rezazadeh, the Welfare Organisation’s head of prevention, recounted that ‘a budget for harm reduction is allocated to the compulsory camps, but these [camps] are not only unsuccessful in decreasing the rate of addiction, but they have become actual locations for the spread of the virus of AIDS in the country’.Footnote 37 Indeed, the debate about the status of these camps proceeded up to the post-Ahmadinejad period. One of the conference presenters mentioned earlier in this chapter, Ahmad Hajebi, invited the DCHQ, to pledge publicly to the definitive closure of the compulsory treatment camps, because ‘they are not places for human beings’.Footnote 38
Nonetheless, compulsory camps have been part of the political economy of addiction in the Islamic Republic: the police identified this model as an easy source of governmental funds, based on a regulation that ensured state bonuses to the NAJA for every drug offender referred to state-run camps. By collecting homeless drug users from across the cities’ hotspots on a regular basis, the police benefit from a substantial financial flow, justified by the expenses that it putatively incurs managing the camps. Given that most of the state-run camps are known for their Spartan and down-to-earth conditions, it is implied that considerable amounts of money are filling the coffers of the NAJA through addiction recovery subsidies. This also implies that the NAJA has a stake in the continuation and proliferation of the activities of the compulsory camps.Footnote 39 Although incidental to the case of compulsory camps, the rumours and accusations about the expensive cars and unchecked revenues of police officials might be a collateral effect of the compulsory camp model.Footnote 40 According to a member of the DCHQ, the municipality of Tehran spends around 400 million tuman per month on taking care of the city’s addicts, or rather for the provision of services to them.Footnote 41 Thus, the police becomes the ultimate powerbroker in drug (ab)use, especially when higher numbers of arrests contribute to a boost in budgetary allocation.
The existence of the compulsory camp model testifies to the endurance of a securitisation approach, based on law enforcement techniques, which coexists with a medicalised and managerial approach to drug (ab)use.Footnote 42 But the camps, paradigmatically, embody a new mode of law enforcement – one that, instead of contesting harm reduction, uses its rhetoric for a new purpose. Security rather than humanitarian concerns govern this model foregrounded in a management of disorderly population – one could name them the ‘downtrodden’ to use Iran’s revolutionary lexicology – through coercive mechanisms, while leaving drug (ab)users, from middle class backgrounds, unmolested.Footnote 43 While reports about Shafaq in the newspapers prompted a political reaction, bringing about the closure of the camp (and its reopening under a new management in 2014), other centres have continued to operate with similar modalities, even though with less outrageous conditions. In 2014, the director of Rebirth provocatively asked the authorities, ‘to take the addicts to prisons’ instead of the treatment camps, because at least as a prisoner the addict would have minimal support from medical and social workers.Footnote 44
Private Recovery Camps
Private rehabilitation centres have been operating legally or informally since the mid 1980s, although their veritably extra-ordinary expansion can be traced back to the early 2000s and the new politico-medical atmosphere brought in by the reformists. In particular, the coming of age of the NGO Rebirth laid the ground for a mushrooming of charitable, private rehab centres, popularly known as camps. The word camp in Persian, rather than recalling the heinous reference to the Nazi concentration camps, hints at the camp-e tabestani, ‘summer camps’, ‘holiday camps’ that had become very much à la mode among middle-class Iranians in the 1990s.Footnote 45
Born of the philosophy of Narcotics Anonymous, the equivalent of Alcoholics Anonymous for illicit drugs, and the idea of communitarian recovery, the camps are based on a detoxification process, usually based on twenty-one- to twenty-eight-day sessions, and on the self-management of daily duties by those interned.Footnote 46 As charitable institutions, they are under the supervision of the Welfare Organisation, but their most immediate relationship with the state is with the police. Regularly contacted by the police in order ‘to accommodate’ arrested drug users for rehab programmes whenever the state-run compulsory camps are overwhelmed, the camps operate on the frontier between public order and private service.Footnote 47 While people referred by the police to the compulsory camps are treated free of charge, those referred to the rehab camps are expected to pay the fees, at least partially. The camp owners admit that only in rare cases, they demand full amount and that they accept any monetary contribution the drug (ab)user, or his family, is capable of making. Most of the time, however, people referred to the private camps by the police refuse to pay and, par consequence, as a camp owner explained, ‘addicts are arrested by the police on Monday, and released by us [the camp owners] on Tuesday, because they don’t have money [to pay the fees]’.Footnote 48 This has triggered criticism of the police, especially in view of the 2010 law reform that puts emphasis on ‘the judicial supervision of the arrest, treatment and release process’, which would require a judicial dossier to be opened for every referral. The conservative newspaper Keyhan reminded the NAJA that ‘the [private] camps have no right to maintain the addicts without a ruling of the Judiciary; similarly they cannot let the addict leave the camp without approval of the judicial authorities’.Footnote 49 Both practices, as blatantly obvious from fieldwork observation, are the rule rather than the exception.
Despite the promise of monetary subsidies from the state, most of the camps exist within an economy of subsistence based on donations from local communities, recovered addicts, the mosques and a few governmental vouchers. However, the landscape of treatment camps includes also sophisticated examples, such as Rebirth’s camps of Verdij and Lavisan. Both located geographically at the north-east and north-west of Tehran, these camps are a different model of recovery, one that drastically differs from that of Shafaq and other camps.Footnote 50 In reference to these camps, several interlocutors pointed out that these places are not mardomi, popular, in the sense that ordinary, working class citizens cannot access them. They have gained credit among wealthier strata of the populace seeking recovery. In 2014, the monthly fee for a twenty-one-day period of rehab in the centre was 6,875,000 tuman [ca. USD 170], an amount the popular classes can hardly afford, although demand for access to the centres has been steady. Media reports have called these camps – somehow advertising them – as ‘a golden exile’.Footnote 51 Inside Verdij, in particular, there is a trendy coffeeshop, with a thrilling view of the forest; the people residing there can be identified as typical northern Tehranis. Some of them, it is reported by the NGO, spend up to a year in the centre, trying to find psychological tranquillity before going back to their lives.
With crippling sanctions hitting the economy in the early 2010s, however, popular classes have been unable to devote resources to sophisticated forms of treatment. Ordinary people opt for less costly options that promise better results than a twenty-one-day session in a camp. So, the panorama of private treatment camps is vast, with services that respond to middle class expectations as well as to the necessities of the popular classes. Accordingly, the conditions of the camps vary along with the costs of treatment, as for other health services.
Women in the Private Camps
Official statistics reported in newspapers in the last decade reveal that one in ten drug (ab)users in Iran is female.Footnote 52 Yet, there are also strong indications that a growing number of women are using shisheh, which would logically imply that the percentage of female users has increased in the last decade. Women represent only 5 per cent of all referrals to state institutions providing service for drug dependency, but a much higher presence is unveiled in formal and informal treatment camps.Footnote 53 The stigma for women is also more resilient and, in several cases, female treatment camps have been set on fire because they deemed these camps as immoral and a ‘nest of sexual vice’, the equivalent of a brothel in public parlance.Footnote 54
In 2011, the government approved the construction of one compulsory treatment camp for female addicts, to be located in the Persian Gulf region of Hormozgan. The site would host a multifarious category whose common feature could be identified in relation to the street (and the moral order): runaway girls trapped in drug (ab)use, streetwalkers, sex workers, female mendicants and petty drug dealers and users. All these categories blur into each other, at least if one sees like a state.Footnote 55 The location itself indicated that the site of this camp had to be peripheral; south along the coast of Hormozgan, the camp would work half as an exile and half as a refuge from the public gaze. Hormozgan itself, however, had historically been characterised by heavy drug (ab)use, including among women, a fact that perhaps further justified the location of the camp there. The particularity of this project was also its joint-venture nature between the state and a private organisation expected to manage the centre, an exception both to the 2010 law and to the practice in other camps.Footnote 56 Given the sensitivity of a female treatment camp, the authorities partly disengaged from its routine administration and partly took advantage of the existing expertise and activism of NGOs dedicated to subaltern women’s affairs. But a single female camp, located at the very periphery of Iran, could not comply with the necessities dictated by the expanding shisheh use among women. This void had been already filled by the establishment of female treatment camps, managed by private individuals or charities. I shall refer to one of them to which I was given repeated access over the course of my fieldwork in 2014. The women’s camp, situated in the city of Arak, operated under the charity organisation Wings of Freedom.Footnote 57
Operating as a sister branch of a male treatment camp, the female camp could hardly be described as a camp. It was an apartment inside a four-storey building in a formerly middle-class area (mostly inhabited by public employees), today referred generally as payin-shahr, ‘downtown’ (in Persian, it indicates ‘a popular periphery’). As I entered the gate of the apartment, I was greeted by a young woman in her twenties, who immediately mocked me because – in the scholarly enthusiasm of accessing a place otherwise forbidden to men and, even more, to male researchers – I had forgotten to take off my shoes, a gaffe which is indefensible in Iranian culture. The woman, Samira from Khorramabad, said, ‘You people go abroad for two weeks and this is the result’; I nodded, as privately I agreed with her, and I proceeded inside, not without awkwardness.
The apartment had three rooms and a small kitchen, with a long corridor used by the women as a lounge to watch satellite TV (which is formally banned according to national laws). The room where I met the director, a woman in her late thirties, was imbued with a powerful smell of cigarettes, an indication that the women, while recovering, smoked heavily. I took out my Bahman Kucik (a popular brand of cigarettes) and offered them to my interlocutors, a move that instigated another amused reaction by everyone in the room. ‘They do not smoke’, glossed the director; as I stared at her, she realised that I had understood and elaborated, ‘They cannot smoke in front of you, doctor!’ I then lit my cigarette, apologised to my interlocutors and started the conversation.
The management of the camp can indeed be problematic. In the past, the director had been assaulted by an interned woman who had threatened her with a knife while trying to escape. After having regained control of the situation, the director reacted by beating the woman who had threatened her. The director was later condemned by a judge for her violent behaviour against the patient in the camp. The camp was shut down for few months, before obtaining another licence under her husband’s organisation, which, I came to discover, is also a rehab camp for male drug (ab)users.Footnote 58 The director had access to several CCTV cameras in the apartment and she could watch the video on her laptop; she could also control the three rooms of ‘the camp’ from the desk of her office, or when she was at home, via an online application to which the CCTV camera were connected. ‘In this way’, she explained, ‘I can check on the girls when I am not here’. She argued that the camp was self-managed by the women themselves, who cook, clean and take care of the daily management of the place. They have a friendly, intimate relationship, she held, and she would like the place to be as comfortable and welcoming as possible. The door at the entrance of the apartment, nonetheless, has to remain locked at all times when she is not in, ‘otherwise the girls might run away and might go back to use drugs’. When I asked her what would happen if a person inside the apartment felt sick or needed urgent help, she justified it by saying that she could be reached at any time via mobile phone and that she checked on them regularly via the CCTV. She also relied on one of the women, Samira, who helped her doing the grocery shopping and kept an eye on the other women while she is away. Samira had been in the camp for one year and a half, since she was referred there by the women’s Prison Organisation. She had spent time in prison on several occasions for shisheh possession, aggression, armed robbery and ‘moral crimes’ (euphemism for alleged sex work). Whether institutionalisation in this private camp had produced positive effects on her life is hard to say. Certainly, I and Samira herself had the perception that her existence was suspended and that, despite having stopped using drugs, addiction was still very much present in her life. In a way, nothing extraordinary: ‘I do not smoke anymore’ or ‘I do not drink anymore’ are part of the experience of people with a dependency, of the eternally ‘recovering addict’.Footnote 59
The fee for a twenty-one-day period is of 450,000 tuman (ca. USD 110). The people coming to the camp do not live in Arak, rather, they usually come from other cities, since they want to avoid being recognised by their communities. This small apartment had two women from Khorramabad, a Kurdish woman from the Kermanshah region who did not speak Farsi, and another from northern Khuzestan. The police had sent three of the women as part of a compulsory treatment programme. Since there is just one compulsory camp for women – located approximately 120 km from Arak – the authorities rely on private camps to accommodate these women, in which case, they also pay the fees for their treatment. Generally, the director explains, the women referred by the police are more problematic, some manifesting serious health issues, while others have several criminal charges pending in their dossiers. It is not rare for these camps to refuse to take over people referred by the police, out of fear of health contagion or in order to preserve their reputation.
Most of the female treatment camps, naturally, operate at the margins of the city, or inside apartments in popular neighbourhoods, in order to pay lower rent and avoid being recognised as recovery camps. There is no overt indication outside as to the nature of the apartment and no explicit address is provided, and the referrals occur through the state line of enquiry – e.g. the police – or through informal connections. The female treatment camps operate along those margins in which state intervention is rendered more problematic by the sensibility of the gender issue, while popular resentment and stigma against them menaces their presence in public. The state, for that matter, is reticent to allocate sufficient licences for the female camps, out of concern that the mushrooming of these institutions – once they are formally recognised by the state – would stipulate a less ambiguous datum of female drug (ab)use, one which might refute the unchanging official version to which the government has hitherto pledged. In this way, it also secures flexibility in its cooperation with civil society.
This condition more evidently marks female drug (ab)users, but it does effect the phenomenon of treatment as a whole. It is no coincidence that, according to several surveys, 90 per cent of rehab camps, both male and female, are unlicensed, and operate in a starkly different environment than the examples of fancy treatment camps of Verdij and Lavisan in the North of Tehran. Indeed, to locate the political dimension of the camp, one has to investigate the phenomenon of the illicit treatment camps (kamp-ha-ye gheyr-e mojaz).
Illegal Treatment: ‘The Hand that Captures the Snake’
The phenomenon of camps suggests that these institutions, regardless of their public/private, legal/illegal status, exist on a continuum. It constitutes, in toto, a primary means of intervention – or mode of government – of addiction. It has become common knowledge – if not a joke! – that contemporary Iranian society offers a wide range of informal, illegal centres for the provision of services (e.g. retirement houses, pharmacies, education centres) and that, despite the government’s repeated calls for their closure, these enterprises continue a lucrative existence.Footnote 60 But the sheer quantitative dimension of the illegal recovery camps – nine out ten rehab camps – signifies that this category effects more largely and, perhaps categorically, the phenomenon itself. Indeed, one could say that legal treatment camps are marginalia within the pages of addiction recovery and treatment.
Already in 2007, the government warned against the mushrooming of illegal treatment camps and gave an ultimatum of three months to all camp managers to register for a licence at the Welfare Organisation.Footnote 61 The DCHQ announced that ‘by the end of the year, the problem of the camps will be solved’, yet in 2014, the number of these institutions was higher than ever, with a veritable burgeoning across the country.Footnote 62 In Tehran alone, there were more than four hundred illegal camps, while in Isfahan, out of three hundred camps, only sixteen had a licence.Footnote 63 In the city of Arak, where I conducted part of the fieldwork, there were about fifty illegal camps, located in nearby villages, main routes or in private houses.Footnote 64 These camps, prima facie, provide treatment for underprivileged people, and their families. With the burden of economic sanctions trickling down to the popular strata, treatment in these institutions represented a more affordable and realistic solution. Given the rootedness of the illegal camps, officials in the DCHQ have started to change their approach, describing the camps as ‘a positive sign, because it implies that many people in Iran seek treatment’.Footnote 65 The officials hold that, as the country’s [official] treatment capacity could not meet the demand for treatment, the camps are instrumental in this endeavour, even when they operate illegally.Footnote 66
In the management of addiction, however, their role bypasses the logic of treatment and service provision. Hamid-Reza Tahernokhost, UNODC expert, defines the illegal camps as ‘the hand that captures the snake [dast-e mar-gir]’.Footnote 67 In post-reformist governance, exclusively legal, bureaucratic or administrative means are insufficient and ineffective. To deal with crisis – and drug crisis – the state exploits the extra-legal function of the camps in areas from which the state itself had progressively disengaged, or has dissimulated its presence. In this regard, the illegal camps operate in a grey area, which qualify as Agamben’s ‘state of exception’, as I elaborate later.
The workings of the illegal camps can be sketched thus: In a situation where someone acts violently and volatilely, usually under the influence of shisheh, the family of the subject usually opts for the intervention of the camps’ personnel. This is regarded as a preferable option to the intervention of the police. By calling the illegal camp, the family avoids criminal charges, which could produce incarceration and time-consuming lawsuits, all of which cause greater economic burden to the family itself. Similarly, the intervention of the camp ‘thugs’ – the gardan-koloft – maintains a lower profile for the family than that of the police, which, especially in popular neighbourhoods, can cause rumours and aberurizi (reputation damage). Saving one’s face remains a top priority for the family as much as for the individual drug user.Footnote 68
The police, too, seems to support the illegal camp system and, at times, informs the personnel of the camps about the location of the complaint (shekayat). In this way, the camps take on the duties of the police (NAJA), with regard to drug (ab)use. A police officer confirms this informally during a conversation,
I am really happy that these camps exist; if a family calls us, instead of sending a soldier or a policeman, we call one of the people from the camps. So, if someone gets beaten, that’s the camp people, which also means that, if someone has to beat someone else, it’s always the camp people [and not the police]. Instead of taking the addict here to the police station, where he might vomit, feel sick and make the entire place dirty, he goes to the camp. Instead of coming here to shout and beat up people, or to bring diseases, HIV, he goes there. I call the camp if someone calls me.Footnote 69
The camps are an apparatus of management of social crises, in the guise of drugs addiction. De facto, most of the illegal treatment camps operate as compulsory treatment camps, because the people who are interned, for periods which vary between twenty-one days and one year, have been forced into the camps. They have not been forced by the police, but by their local communities, usually their family members. The police plays the part of the observer or the informant. It instructs the camps, in some occasions, of the location and situation of the complaint, but no formal undertaking is enacted. The camp operates in an economy of punishment and recovery of their own, autonomous but not independent from the state.
The illegal camps have become rapidly part of a mechanism of intervention, which goes beyond treatment, per se. Inside them – several personal stories disclose – the managers of the camps can adopt ‘alternative techniques’ for the treatment of addiction, the most infamous ones being kotak-darmani (‘beating-treatment’), ab-darmani (‘water-treatment’), sag-darmani (‘dog-treatment’) and zangir-darmani (‘chain-treatment’).Footnote 70 Each of these options suggest the use of an element – water, dogs, chains or punches – to inflict violence on the recovering drug (ab)user. It indicates the use of force and violence and constriction in preventing interned people from wanting to use drugs again. That occurs generally regardless of whether the person seeks to use drugs in the camp or not. It is a form of preventive measure of dissuasion and – how to say this? – a punishment for having used drugs in the first place. Although there is generally a propensity towards sensationalising these accounts – as most newspapers do on topics related to illicit drugs – the deaths of interned people are the public signature of the camps’ practice in the collective narrative.
Conversely to the state-run camps, the liability of the crime remains exclusively with the camp managers, as noted in the statement of the police officer mentioned above. The authorities severely punish casualties within the illegal camps. According to Islamic law, the judge applies qesas, retributive justice (‘an eye for an eye’). That implies the death penalty for those who are responsible for the camps where the death had occurred and was proven to be the result of the personnel’s mismanagement. (More precisely, the capital sentence is meted in cases where the family of the victim refuses to accept the diyeh, the ‘blood money’.) Although there are no clear data on the rate of deaths within the illegal camps, the reports in the newspapers suggest that the events are not sporadic.Footnote 71 Among impoverished drug (ab)users, the narratives of the camp gained solid ground and instil vivid fear, a sentiment that is somehow reminiscent of a persecution. In this way, the camps fulfil a double promise: they intervene along the problematic margins of society (its uncivil society), through the creation of extra-legal, unaccountable and, in view of their quantitative dimension, omnipresent institutions. They represent an apparatus in the management of disorderly groups and, more generally, the drug crisis. As such, they decrease the work of the police, while receiving nothing in exchange. At the same time, the camps are managed by former drug (ab)users, whose place within normative society remains unsettled. These individuals struggle to find employment in regular businesses, their housing status endures as uncertain, often relying on temporary family accommodation. The camp, hence, becomes the only stable unit in their life, functioning both as occupation and residence.Footnote 72 The heads or managers of the camps are usually also those who make the initial investment to pay the rent of the location, whether a house with garden, a flat, a silo or an abandoned compound. Two or more people, friends or family, set up the camp and employ a number of handymen who are often former ‘patients’ of the camps, now willing to help out for a small stipend or to pay their debt. In this regard, there is no substantial difference between legal and illegal camps. In this peculiar way, post-reformist governance of crisis succeeded in its quest ‘to socialise the war on drugs’ and ‘to mobilise (basij kardan)’, by other means, civil society for statist ends.Footnote 73
A public clinic manager, who also serves as a psychiatrist in a compulsory camp, explains that ‘the [illegal] camp system has successfully managed to keep the antisocial elements of society within itself: a group of antisocial people is represented by the owners of the camps, and the other group is represented by the patients, those interned in the camps’.Footnote 74 Regardless of whether the camps are constituted by antisocial groups – whatever this category signifies – the camp system functions as ‘safety valve’ for recovered drug (ab)users, whose psychological and social status is in need of a stable occupation, which would otherwise be unachievable. With the camps providing motivation and an ecosystem in which to find their place within society, the camp owners practise a system in which the phenomenon of drug (ab)use dissolves into the machinery of treatment – under the rationale of harm reduction. This system seemingly replicates itself. Former patients are employed in addiction treatment and, whether willingly or involuntarily, mistreat other drug (ab)users, perpetuating previous securitising policies.Footnote 75
This phenomenon unwraps a form of grassroots authoritarianism, whereby social elements belonging to diverse societal milieux, partake in mechanisms of control, discipline and treatment. Its relationship with the state remains, peremptorily, ambiguous, based on rhetorical condemnation, haphazard prosecution and clandestine connections, for instance, in the referral of complaints by the police to the illegal camps. Despite almost a decade of reiterated calls to close the doors of the illegal treatment camps, these institutions maintain solid roots and operate, qua rhizomes, across the margins of rural and urban Iran. Their ubiquity has given rise to the phenomenon of kamp-gardi, ‘camp-touring’, which refers to the unending journey of the drug (ab)users from camp to camp, a circumnavigation that rarely offers a way out and often leads to the individual becoming either destitute or incorporated into the activities of a particular camp.Footnote 76 Those whose experiences have been more telling are often called by the rest of the community as the ‘Marco Polo’, because they have visited as many camps as the Venetian traveller had done during his travels of the Milione.Footnote 77
An odyssey similar to that through camps, clinics and prisons goes also through other venues, such as public parks and the street where the state manages disorder differently.
A Site of Disorder: Harandi Park
In the southern district of Tehran’s Bazaar, between Moulavi Street and Shoosh Street, there are four public gardens. The biggest and most popular of these is Harandi Park, which stands at the heart of the old neighbourhood of Darvazeh Ghar. Between 2014 and 2017, Harandi Park and, to a similar extent, the other parks as well, saw large groups of drug users who camped there with tents, sleeping bags, bonfires and piles of cardboard on the ground. Over the warm seasons – between March and November – the number of street drug users residing within the perimeter of the parks and the connecting alleys reached over three to four thousand, with additional visitors towards the evening.Footnote 78
While on a stroll across the lawn in a late morning, I encountered waste collectors and gardeners working their way between groups of drug users, chatting or just passing through their circles. Every now and then, a police motorbike would ride on the main road circumscribing the park or in the middle of it, with neither the people or the police officers taking much notice. The entrance of a larger tent, close to a smelly empty pool that operated as an open-air loo, was animated by the bustling of a dozen of people. I was told later that the tent was where the main distribution of heroin (gart) and shisheh in the Harandi area takes place and that it is the centre of gravity of the park.
This is not an underground, hidden site of criminality and a marginal zone of crisis/disorder, as often described in the public imagery. The park stands in the middle of one of Tehran’s working class and poorer neighbourhoods, with a symbiotic relation to its great bazaar, located close to the main metro line (Line 1) connecting the wealthy north with the city’s southern poorer districts. In contrast to the ever-lasting declarations of the ‘War on Drugs’ and the ever-increasing number of drug arrests, the situation in Harandi casts light on a different approach based on limited tolerance of public drug use and the tacit acceptance of street hustling.
Activism among civil society groups and NGOs has attracted public attention to this place, which, by 2015, had become a leitmotif of debate around drug policy and harm reduction in Tehran. The city municipality and the mayor of the district denied their acceptance of the situation and reiterated that there is no plan to transform Harandi in a social experiment of de facto drug decriminalisation. In discussions with people in the drug policy community, the ‘Harandi model’ referred to an experience and experiment of alternative management of street drug use. An alternative to the collection plans of drug (ab)users, it refrained from incarceration or forced treatment in the compulsory camps. Instead, by having large gatherings of so-called ‘risky’ drug (ab)users concentrated in specific areas, such as Harandi Park, social workers and medical personnel could proceed to intervene with welfare services while familiarising local drug (ab)users to the options of recovery and the cycle of addiction treatment, notably methadone. The ‘dispersion of risk’ is reduced, according to public officials, who imply that, without Harandi, the whole of Tehran would be a scene of open-air drug use and drug hustling, with the spectre of HIV epidemics looming all-too-large over the populace. It would be uncontrollable.Footnote 79
That is why the neighbourhoods of this area have been provided with automatic syringe distributors, located within the reach of support centres managed by NGOs (Figure 7.1). The presence of civil society groups had, in fact, become central in this area and public attention reached its azimuth when, in autumn 2015, several groups of volunteers, humanitarian associations and philanthropic citizens started to bring cooked meals and clothes to the park and distributed them among the drug (ab)users. The provision of food had been a matter of satire amid detractors of this tolerant approach, who hold that ‘the drug addicts are no longer satisfied by bread and egg or bread and cheese, but they expect sophisticated food and are spoiled for choice’.Footnote 80 Others claimed that public attention is driven by a sentimental piety not grounded in a real understanding of the complex situation of drug addiction in this area. Philanthropic endeavours practiced, in the words reported by a piece on Sharq, ‘addict-nurturing [mo‘tadparvari]’.Footnote 81 A public official cynically suggested that the provision of food might well be a stratagem used by providers of addiction treatment (e.g. Article 15 camps) to attract people towards their facilities and, incidentally, attract public funding towards their organisations.

Figure 7.1 Automatic Syringe, Condom Distributor, Harandi Park
Although complaints against insecurity and unsafety were rife among residents of this neighbourhood, Harandi Park had by then become a spotlight for national drug policy and a site of confrontation of competing governmentalities regarding illicit drugs. On October 9, 2015, I was invited to attend the ‘First Marathon of Recovered Female Drug Addicts’ organised by the House of Sun (khaneh-ye khorshid), an event which would take place, deliberately, across the four parks of Harandi, Razi, Baharan and Shush. On the edge of Harandi Park’s southern corner, the House of Sun has been active for over two decades in providing free-of-charge services and support to female drug (ab)users and those women seeking refuge. A large crowd of women (and some men) attended the opening ceremony of the marathon and waited for the start of this seemingly sporting event. Two female players of the Iranian national football team led a collective session of gymnastic activities, a way to symbolically recover the body of the park from the sight of widespread drug consumption and destitution. Truth be told, the event revealed itself to be not a marathon – not even close – but rather a public demonstration that brought more than a thousand women and their sympathetic supporters to march inside the park and in the middle of the gathering of mostly male drug users (Figure 7.2). The term ‘marathon’, I thought, was probably used to get around the politicisation of the event in the eye of the municipality then led by Mohammad Baqer Qalibaf, which could have regarded a women-led march against drugs as too sensitive a topic (Figure 7.3).

Figure 7.2 ‘Every day 8 addict die in Iran’

Figure 7.3 Members of the National Football Team
Many of the women who took part in leading this manifestation had previous experience of life in the park and were acquaintanted with people who were still living and using there. ‘Our Iran is paradise! Don’t smoke, it’s not nice! [Iran-e ma beheshté, dud nakonid ke zeshté]’, was among the slogans that were chanted; prayers for the souls of the drug addicts were interludes between the chants and on the sides of the march, many of these women would approach people laying on the grass trying to connect with them and dissuade them from using drugs. A man, I witnessed, approached an older women and pathetically begged her to stop chanting against drug users, ‘because we are feeling ashamed and embarrassed in front of you’; others would cover their face or shout aggressively against the voyeuristic lens of the many photographers attending the event (Figures 7.4 and 7.5).

Figure 7.4 Marathon March, Tehran

Figure 7.5 ‘Give Me Your Hands, so We Can Walk in the Path of Purity’
The event resonated loudly within the drug policy community, but it also manifested some of the profound changes that Iranian society had experienced over the course of the 2010s. Women who had a history of drug abuse openly participated in the event, without hiding their immoral past and marched in the parks where they once spent their drug habit. In doing so, they also addressed drug users in the park directly and invited them to give up. The associations that participated in this manifestation were not the traditional anti-drug campaigners, but an array of harm reduction groups, users-led organisations and groups of people who had a history of drug use and were open about discussing addiction as a social dilemma. Some public officials attended the event, but, overall, it was mostly associations, grassroots groups, a few members of international organisations and social workers and activists. Leila Arshad (aka Lily), the main organiser of the event and director of the House of Sun, had long been working in this neighbourhood.Footnote 82 While those attending the marathon had gathered in the courtyard of the NGO, she held the microphone and said, ‘one of our objectives is to catch the attention of the public officials and people towards your problems [recovered female drug abusers]: lack of employment, absent housing, insurance and treatment, respect and social inclusion’.Footnote 83 Some of the volunteers catering the event were employees and volunteers of Doctor without Borders (MSF), which runs, among other things, a mobile clinic with outreach services in the area.
A few weeks following the marathon, a group of thirty or forty men raided the informal camping in Harandi Park, set fire to several tents and attacked a number of street drug users with sticks and clubs. The municipality declared that the attack was perpetrated ‘by the people’, denying any state responsibility of the authorities. Others hinted at the lack of responsiveness of the police.Footnote 84 Harandi Park, for that matter, embodied a most explicit case of the art of managing disorder in the Islamic Republic. In 2018, the municipality opted to develop the camp into a sporting area and fenced all its surroundings.
Conclusions: The Art of Managing Disorder
There is no fundamental rupture, or watershed, between the state-run compulsory camps (kamp-e maddeh-ye 16) and the informal, illegal camps (kamp-e gheyr-e mojar), or the ‘Harandi model’. Both fulfil an ultimately political prerogative in reaction to a phenomenon that has permanently been framed as a crisis. Because of that, the camps enter a field of interest to the state – one could say an expediency (Interregum) – in which the underlying rule is political management of risk, emergency, disorder and crisis. It is not, as one would expect in the Islamic Republic, a matter of moral evaluation, religious justification or variation in (post)Islamist change.
The art of managing disorder defines the governmental approach to the (drug) crisis. This art operates at the level of fabrication, make-believe and of practice, confuting the notional existence of law and the state, as seen in the case of the camps. In intervening on the phenomenon of drug (ab)use, the post-reformist state defined its modus operandi as one based on secular pillars of management. It did not thwart harm reduction practices, per se, or out of religious, moral opposition. It actually adopted the language of harm reduction, it scaled up its less contentious services (i.e. methadone and rehab camps) and, at the same time, it brought about institutionalisation of the agents under the umbrella of the state. While the state financed a significant bulk of harm reduction programmes, through the DHCQ, the police proceeded towards a securitisation of disorderly groups, based on a form of imprisonment, by other means. These means were constituted by the compulsory treatment camps, whose objective has been not to treat or reduce the harm of drug use as such, but of managing the disorderly presence of risky groups – i.e. homeless, vagrant, poorer drug users – in the public space. This process, on the one hand, secured a key role for the state under the guise of the ‘therapeutic police’, while, on the other, allowed a drastic intervention on those categories perceived as disorderly and, indeed, pathological.
The multitude of illegal treatment camps hints, instead, at another statist rationale. The state provides licences for these camps through the Welfare Organisation, but in order to do so, the government needs to guarantee minimum financial support, which, given the large number of these centres, would drain the budget from other treatment programmes, notably the compulsory treatment camps. ‘The closure of the illegal treatment camps is not part of the main policy of the state’, declared a public official in a conference, adding that ‘the existence of these camps is better than their non-existence, because their closure would mean disorder [bi-samani, also ‘instability’, ‘chaos’] among the dangerous addicts’.Footnote 85 In view of their indirect connection to the police, which sees them as a useful complement vis-à-vis problematic drug users, these institutions are part of the state effect. Despite their private and unrecognised status, they perform a public, state-sanctioned role (Table 7.1).
In doing so, camp owners and managers do not benefit, at least in most cases, from a particularly lucrative business. As confirmed both by ethnographic data and by interviews, they do not display middle class lifestyles and they mostly belong to the working class, underprivileged strata of the populace. Their income, as their status, is unstable, insecure, and exposed to several risks, including that of being closed down abruptly, or facing criminal charges for mistreatment or torture. Hence, the camps operate in an ‘in-between zone’, where they neither have actual leverage on the political mechanism of drug policy, nor do they profit from economic returns. Instead, they parallel the market of drugs with a market – which is equally illegal, yet tolerated – of treatment and recovery.
‘The condition of crime is suspended for the addicts who seek help from recognised institutions’ reads Article 15 of the 2010 drug law. This sentence is ambiguous under many points. First, what does ‘seeking help’ mean? In the Iranian legislation, it seems to signify either detoxification (‘cold turkey’) in private camps or registration to a methadone programme. Seeking help in the form of clean syringes or medical and psychological assistance of various kinds does not guarantee the suspension of the law, even in sites of disorder like Harandi Park, where the suspension is aleatory. Therefore, drug users who do not want to substitute their drug of choice with a legal substitute, e.g. methadone, or do not agree – or cannot afford – to go through rehabilitation in a private camp, are not protected by the law. They are relegated, ultimately, to an institutionalised exception exemplified by a state-run compulsory camp, an illegal camp or the public space. This ‘suspension’ lands the addict in a zone of ‘exception’. The exception is a paradigm of government of the drug crisis, which allows the coexistence of otherwise inconsistent and incompatible visions and interventions, as exemplified by the idiosyncrasies of Article 15 and Article 16 of the 2010 law. This cacophony within a single law and between the text of the law and its execution, lays, on the one hand, in the formal, de jure, insolubility of different governmentality within the state, while, on the other hand, it embodies an instrumental approach in the establishment of multiple, discontinuous responses under the art of governing crisis and managing disorder.
As in Giorgio Agamben’s State of Exception, this condition produces a ‘no-man’s land between public law and political fact, and between juridical order and life’ and it ‘appears as the legal form of what cannot have legal form’.Footnote 86 It is, in other words, an oxymoronic form of politics. To corroborate this analysis, Agamben adds:
the state of exception proceeds by establishing within the body of the law a series of caesurae and divisions whose ends do not quite meet, but which, by means of their articulation and opposition, allow the machine of law to function.Footnote 87
While categorising as criminal the multitude of drug (ab)users who do not agree to intern in a camp or substitute their drug of choice with methadone, the governmental machine has preserved its ability to ‘manage the disorder’, or to politically employ the crisis posed by massive drug (ab)use. The result is a paradigm of government – the art of managing disorder – that deals with the crisis without solving it, and therefore reconfigures the locus of harm reduction, in this case, by incorporating it in a grey area of state control/repression. Thus, the ‘caesurae’ and ‘divisions’ of the 2010 law, instead of undermining the machinery of drug laws, make it actually function, as demonstrated in the coterminous implementation of Article 15 and Article 16. This mixture of policies allows the machine of the Iranian state to function.
The role of the police is absolute in this frame; whereas one can locate the text of the law and the policies with regard to drug (ab)use, the function of the police is indeterminable and discretionary. The police is the governmental machine that enacts and reproduces the drug control in praxis and, because decisions on the political dimension of the ‘problem’ belong to the sphere of government and justice, the police acts only and exclusively on the effects of the drug problem, for instance, in the identification of temporary risky groups, or in the clearing of disorderly presences from the public space. This coexistence between insoluble, albeit instrumental to each other, ideological traits, justifies the praxis of the law – the political machinery operating on the ground. Being the administrative and enforcement tool of the politico-judicial machine, the police works on the contentious ground between what is formalised de jure and what materialises de facto. This ground is the grey zone where the rights of the drug (ab)user are at the same time enounced and violated, therefore entering the realm of an institutionalised exception, for instance, in the compulsory treatment camps, or that of a state of exception, in the illegal camps.
In this context, the status of the addict – the individual who can be object of welfare support and at the same time of criminalisation, i.e. the mojrem-e bimar (‘patient criminal’) – is exemplified by the paradigm of Agamben’s homo sacer – the person whose right to life cannot be legitimately taken, but who is contemporaneously excluded from ordinary law.Footnote 88 The legal status of the addict, within the current regime of drug control, is one of naked life, whose civil/political dimension is questioned and relegated to a grey area. Naked life is life stripped of rights. The denouement of the addicts’ rights produces political control over their life, making them a subject at the mercy of politico-juridical control, and an element in the political economy of treatment (e.g. state-run camps). Protection and punishment are two overlapping ends in the social body of the addict. A manager of a state-run clinic uses these apt words to corroborate this argument:
Those who are in the camps are in the middle between criminal and patient. They have not been accused of any crime. From a legal point of view, they have not committed a crime, … there is no legal judgement [mahkumiyat], usually there is a complaint [shekayat] about bad behaviour [bad raftari].Footnote 89
The informal nature of the ‘complaint’ produces the informal response of the illegal camps or, more rarely, that of the state-run camps. In both cases, the person who is being ‘treated’ enters a field of informality and ambiguity, as neither bureaucratic nor juridical procedures are in place. Indeed, despite the law envisioning a criminal charge against an addict who is re-arrested after a period in a compulsory camp, the police regularly refer people to the camps who had paid dozens of visit to these centres, amazingly without having a criminal record.Footnote 90 The dossier, alas!, is missing.
In the conference that opened this chapter, a presenter, much to the astonishment of the audience, remarked:
I have the feeling we are crying on a grave which is empty.Footnote 91 How many people, arrested for drug addiction and sent to compulsory camps, have actually been in front of a judge? And [if this has happened] had the judge said anything to them about treatment? I doubt that we can find ten people in the whole country who have met a judge before going to a camp, so I think the question here is something else and it is not related to compulsory treatment … The problem, it seems to me, is that the question is not medical and therapeutic, but one of social and political control.
The lack of judicial supervision and bureaucratic mechanisms is inherent to the state’s management of disorder and crisis. It is not a by-product of a lack of administrative capacity or clashing institutional interests. This coexistence of criminalisation of drug use and tolerance of the crime stems from a discretionary practice of the law. It epitomises the ‘force of the law’ in conditions otherwise unlawful. In practical terms, this makes the agenda of police officers and their immediate superiors the ‘single most important element’ in the application of the drug laws.Footnote 92
The force of the law applies materially against those more exposed in the ecology of the police: the street, parks and the public place. In this regard, the art of managing disorder applies more blatantly to the poor, the homeless, the street addict, the sex worker, while those who preserve their drug use in the private sphere do not face the force of the law. Public addiction becomes being addicted in public: homeless people are badly dressed, dirty, in other words, are living at a street level, exposed to the public gaze of the police. At this point, drugs are not the real problem. The addict in the guise of social marginalisation, moral unsettledness and class subordination incarnates the problem.
To conclude, one can infer that the framing among many public officials that addiction is a problem without solution – especially in the case of shisheh for which a substitute drug had not been viable – compelled the authorities to intervene through new techniques of political management. The compulsory state camps, in tandem with the illegal camps, have produced this governmentality. Emran Razzaghi defines the camps the number i of Iran’s drug policy equation: ‘an imaginary number that we bring in and take away later; … they don’t have a meaning in themselves but they contribute to the change of the equation’.Footnote 93 In this, they represent a primary means in the art of managing disorder of the drug phenomenon. They also confirm, together with Agamben, that ‘the true problem, the central mystery [arcano] of politics is not sovereignty, but government; it is not God, but the angel; it is not the King, but the minister; it is not the law, but the police – that is, the governmental machinery that they form and keep moving’.Footnote 94
Instead of the God-like state of the Islamic Republic, with its, prima facie, religiously inspired laws, I attempted to study the minister, the practices of the laws as much as the rhizomes of the state, all of which, I realise, form the governmental machinery of the Iranian republic.
Introduction
If the reformist period was one of ‘one crisis every nine days of government’, the post-reformist years characterised themselves for a permanent state of crisis, a status well captured by the expression ‘nine crises every day of government’.Footnote 1 Crisis was critical to the formation of Mahmud Ahmadinejad‘s vision of governance in policy and polity. Crisis remained central after Ahmadinejad, too, reigning over Hassan Rouhani’s period in power. Among these multiple crises, one can mention the following, in escalating order: the football, wrestling and judo federation crises (2012–17); the aviation maintenance crisis (2006–18); the automobile manufacturing crisis (2011); the House of Cinema crisis (2014–15); the housing bubble crisis (2010s); the market recession crisis; the inflation crisis (passim); the hydrogeological crisis (in the example of Lake Urmia, 2010–19); the Kahrizak prison crisis (2009); the 2009 election crisis; and, ça va sans dire, the nuclear crisis (2006–?).Footnote 2
The sanction regime imposed on Iran added pressure on a situation that was already deemed critical, contributing to the perception among Iranians and their political leaders, of a permanent crisis haunting the country. The first round of nuclear-related sanctions took place in 2006, when the United Nations Security Council (UNSC-1696) agreed to impose restrictive measures on Iran’s nuclear enrichment programmes. In 2010 and 2012, a second and third round of sanctions began with UNSC-1929 and was further tightened with the sanction regime imposed by the United States under Barack Obama, closely followed by the European Union. Following Donal Trump’s election, the United States withdrew from the Joint Comprehensive Plan of Action (JCPOA, aka in Iran as BARJAM) and in 2018 implemented a set of sanctions against the Iranian economy. The Islamic Republic’s isolation caused by unilateral US sanctions coupled the crises ongoing at the domestic level.
On top of all these, the drug phenomenon entered into a new dimension, one that the state had not foreseen and found difficult to deal with. The changing nature of drug (ab)use – the phenomenon of shisheh – buttressed the formation of a crisis that had been a feature of the reformist period, as described in Chapters 4 and 6.
The dynamics of post-reformist society characterised by the use of new stimulant drugs and non-traditional sexual norms, situated the post-reformist government in a paradoxical situation. The outcome of this situation was expected to be a reaction based on normativity and condemnation of new societal trends, followed by a reversal of the progressive policies, such as the controversial harm reduction legislation. Contrary to expectations, however, the Ahmadinejad government did not reverse the trend in favour of harm reduction and it generally continued the process of expansion of civil engagement in the field of drug policy. It scaled up progressive policies on addiction into a nationwide project. In view of the threat of shisheh, state representatives stressed the need to make distinctions between different substances, pointing out that the institutions should encourage shifting to less harmful drugs, such as opium.Footnote 3 High-ranking officials reiterated that ‘the management of the drug market has to be in control of the nezam [political order]’, and that the destruction of the poppy farms – successfully implemented in the 1980s – had been a strategic mistake.Footnote 4 From the second half of the 2000s onwards, officials included in their public agenda the reintroduction of poppy cultivation and other drastic reforms in the field of illicit drugs, including regulation of drug consumption.
Under Ahmadinejad, drug consumption underwent further changes. The average age of drug use dangerously decreased; more women were using hard drugs than ever before; traditional drugs were supplanted by domestically produced synthetic drugs, while the government spent considerable financial resources on drug control programmes. By 2012, according to a public survey, only 7 per cent of Iranians believed the government have been effective in dealing with the drug problem, which for 87 per cent represented the country’s main social problem.Footnote 5 Surveys revealed that people considered the police the worst-performing institutions in the ‘War on Drugs’.Footnote 6 This was despite the LEAs having arrested, over the course of three decades, more than 3.9 million people for drug crimes.Footnote 7 The compound effect of these data and the public impact of shisheh narratives (re)produced a crisis, similar to the one which characterised the initial years of the reformist government at the end of 1990s, with the HIV ‘epidemic’. However, the response of the Ahmadinejad government differed substantially from that of Khatami’s reformism, highlighting their diverging paradigms of government as illustrated in the previous chapter. In line with the style of president Ahmadinejad, the government maintained a populist approach towards drug policy, often circumscribed by an aura of secrecy and bombastic promises. In the occasion of a drug-burning ceremony, president Ahmadinejad declared ‘the problem of drugs is not only a cultural, social and economic, but it is an important political problem’, adding that only ‘the reform [eslah] of the governance system of the world [nezam-e hakem bar jahan]’ could uproot the drug problem.Footnote 8 Unlike his reformist predecessor, Ahmadinejad engaged in individual and collective meetings with recovered drug addicts, listening to their requests and recriminations. During a gathering in Tehran’s Azadi Stadium, Ahmadinejad, in front of 20,000 former drug users, said, ‘Ahmadinejad [referring to himself], like your younger brother, stands beside you in trying to solve your problems; the government is honoured to be on your side and on the side of your recovery’.Footnote 9 Significantly, the president’s reference to himself (and the government) as the younger brother was symptomatic of the vision that the post-reformist state had with regard to its role in addiction recovery and treatment. While many of the promises remained unfulfilled (e.g. priority for recovered addicts in employment), his call to adopt ‘new strategies and approaches of fighting drugs’, was the prelude to the rise of a new mode of governance, one that defied both harm reduction and prohibition alike.Footnote 10 The government played the role of the younger brother, who seeks advise from its civilian counterpart, civil society, the older brother. It acted through a modality of indirect government of the crisis. As seen in the previous Chapter, the principle modality of intervention in the post-reformist time was embodied by the art of managing disorder.
This chapter elucidates the practices born of the post-reformist moment. While in the previous chapter I discussed the on-the-ground mechanisms of management made up of informal and clandestine elements, in this section I engage with the way government and civil society cooperate in drugs politics. Here, I systematically consider the strategies of intervention within the broader scheme of the government’s approach to illicit drugs. This is produced by the institutionalisation of methadone clinics and the governmentalisation of NGOs operating in the field of addiction. Neither belong to the institutional realm of the state, but function through state subsidies, supervision and collaboration, hence materialising ‘twilight institutions’ and parastate formations. The aim is not only to illustrate how the reformist-supported policy of harm reduction metamorphosed under post-reformism, but also to connect the daily operations of public and private institutions within the broader framework of state formation and interactions between state and social phenomena.
‘A National Question, Not a Governmental Duty’
Withdrawal from formerly state-prerogative fields and the appeal for massive privatisation of non-key public assets were two key features of this era. The Constitution of the Islamic Republic, under article 44, allows privatisation of public assets, a plan that had occurred in several instances in the post-war period. Iran’s highest juridical and executive authority, Ali Khamenei, decreed in 2006 that ‘80 per cent of the public sector should be privatized’.Footnote 11 Under Ahmadinejad, about 90.5 per cent of the total value of transfers of state enterprise in the post-war period took place, a fact that is revelatory of the extent to which his government sought the lightening of state governmental duties, while promising to bring the oil money to the dining table of the populace.Footnote 12 This trend applied even more drastically to those areas of governmental action reputed burdensome and socially problematic, such as drug consumption and drug (ab)use. With the approval of harm reduction policies, the state authorised the creation of private methadone clinics (MMT), where people seeking treatment could initiate a treatment process. Methadone clinics soon became a vibrant phenomenon in the market of medical services, providing a steady source of revenue for medical practitioners, often GPs with no specialisation in addiction recovery (Figure 8.1).Footnote 13

Figure 8.1 Methadone Clinics (2009–13)
In 2009, there were about 160,000 people registered in private clinics for methadone; in 2014, the number had gone up to almost 570,000 people.Footnote 14 This astonishing increase in just a matter of five years explained the high demand for methadone among the population, but spoke also of a fundamental medicalisation of drug use among the users themselves.Footnote 15 Of the country’s 5,300 clinics, around 4,900 (95.3 per cent) belong to the private sector (Figures 8.1 and 8.2). More interestingly, while the number of public clinics has remained stable, that of private clinics has multiplied constantly up to 2014, when they allegedly reached saturation level.Footnote 16 By 2014, almost 800,000 people were registered under MMT, a figure that ranks among the highest worldwide. Drug (ab)users unable to register in private clinics, were supported through a network of state-run clinics, where the cost of methadone was heavily subsidised. These were usually connected to state-run compulsory camps under the management of the therapeutic police.

Figure 8.2 Methadone Maintenance Treatment Patients (2009–13)
The post-reformist state admitted that it needed the private sector to fulfil its governmental duties. In an interview, the deputy director of the DCHQ, Tah Taheri, stated that ‘because the government is unable to treat all the people, we rely also on the private sector. In the case of addicts who do not have enough money, we [the state] provide subsidies for them, but if their family, as usual, intervenes, the family pays for the treatment’.Footnote 17 The statement confirms that the reliance on the private sector for medical provision in the field of addiction recovery was (and is) a deliberate strategy of the state, complemented by the development of domestic methadone production. Today, Iran is self-sufficient in methadone production (Figures 8.2 and 8.3).Footnote 18

Figure 8.3 Patients in Medical Facilities for ‘Drug Abuse’ (2013)
The government’s reluctance to expand public treatment was a question of economic calculation. The diatribe about ‘addiction insurance’ (bimeh-ye e’tiyad) elucidates this aspect well. Following approval of harm reduction, public pressure mounted on the provision of insurance on addiction recovery. Often recovering in psychiatric hospitals and clinics, drug (ab)users seeking addiction recovery could not benefit from insurance coverage. Families paid the fees for those patients recovering in mental service centres, despite ‘addiction’ being acknowledged as a medical condition, ‘a pathology’, a ‘disease’. In response of this situation, the DCHQ director for treatment and social support explained that medical insurance did not cover addiction, as it involved consumption of illicit substances, and therefore fees could not be covered by public funds. Addiction remained an ambiguous pathology in the state vision; tactically, this implied that the state was not responsible for the financial coverage of costly psychiatric treatment. Given the rising numbers of shisheh users, drug policy officials scrupulously considered the likelihood of future ‘epidemics’ of mental disorder and the rising demand for psychiatric assistance. By 2015, approximately 400,000 people were known to consume methamphetamine, with polydrug use – the combination of different illicit substances – being on the rise.Footnote 19 Were the state to insure all drug (ab)users, the real number of Iranian people on drugs would be publicly visible and politically legible. This legibility risked undermining the political order and its decade-long attempt at moralising to the public. Covering the data by a thick veil of ambiguity guaranteed economic saving and political gains (Figure 8.4).Footnote 20

Figure 8.4 Number of People Admitted to Rehab Centres
One could sum up the post-reformist approach to the issue of drug (ab)use with the words of an Iranian parliament member – and staunch Ahmadinejad supporter – who said, ‘the fight against drugs and addiction is not a governmental duty, but a national question [matalebeh melli]’.Footnote 21 To be successful in the treatment of drug (ab)users, Iran needed ‘a social movement [harekat-e ejtemai, sic!]’, with the government having a ‘supervisory duty [nezarati]’.Footnote 22 The national question regarded all: public as well as private, civil society as well as institutions and agents of the state. This was a prelude, it might be argued, to the outsourcing of governmental duties to the private, or pseudo-private, sector. I shall now introduce how the machine of government reacted and what techniques of government unfolded in response to the fluid drug phenomena of the 2010s.
Harm Reduction Revisited
With the political backing for reform fading away, the new government moved towards a securitisation of social activism, especially those groups supporting reforms on civic issues. In a matter of a few years, most of the key social agents that had supported harm reduction were defused of their reformist clout. In June 2008, Iranian authorities arrested Kamiar and Arash Alaei, the two brothers who piloted the successful Triangular Clinics, on charges against the security of the state. They were accused of cooperating with foreign government to destabilise the Islamic Republic. Bijan Nasirimanesh, who operated the first DICs in Shiraz and Tehran, left the country in early 2009, while the NGO he founded continued to provide services inside Iran. In 2011, Said Madani, author of one of the first books about drug addiction in Iran, was arrested and sentenced to six years in prison and ten years of exile in Bandar Abbas for his political activities related to the Nationalist-Religious Movement.Footnote 23 Thus, the personalities and networks behind the reform were prevented from carrying on their reformist-minded plan in the field of drug policy. Besides, the post-reformist government targeted, systematically, reform-oriented academics and members of the scientific community, when in 2006 it reportedly forced numerous scientists and professors to resign from their post or to accept early retirement. By weakening the academic profile which had been behind the push for innovation and change, the government enhanced its political control and centralisation over drug policy institutions. This did not mean a setback for civil society participation in addiction recovery and drug policy. Although observers considered the coming to power of Ahmadinejad as a direct threat to the progressive harm reduction system, practices of support to drug (ab)users continued and effectively widened their quantitative scope following his election in 2005. By 2007, there were 51 government facilities, 457 private outpatient centres and an additional 26 transition centres.Footnote 24 By 2009, there were already 1,569 treatment centres, 337 government centres and 1,232 non-government centres, which have been operational throughout the country, providing services to 642,516 persons.Footnote 25 The fact that harm reduction and addiction recovery had been included in the 2010 text of the General Policies of the Islamic Republic of Iran [siyasat-ha-ye kolli-ye nezam], emanated by the Expediency Council and approved directly by the Supreme Leader, surely contributed to this process.Footnote 26
Drugs politics pursued a discontinuous, unsettled path. During his eight years of government, Ahmadinejad appointed three different directors to the highest post at the DCHQ. First, he selected Fada Hossein Maleki (2005–7), who then moved to occupy the post of special ambassador to Afghanistan, a key anti-narcotics role.Footnote 27 From 2007 to 2010, the caretaker of the DCHQ was the Commander-in-Chief of the National Police Esma’il Ahmadi-Moghaddam, who also maintained his post as head of the police. After 2010 and up to the end of Ahmadinejad’s second mandate, the president appointed his Defence and then Interior Minister Mostafa Najjar (2010–13), who also remained in charge of the ministry during his mandate at the DCHQ. Apart from the change in the directorship of the organisation, this period was characterised by a lack of direct political management in the DCHQ. The overlapping duties – as ministers and head of anti-narcotics – of the DCHQ directors meant that the DCHQ suffered from the lack of an independent strategy and scrupulous management. Internal sources to the DCHQ confirm that both the president and DCHQ directors rarely participated in the weekly meetings, leaving the organisation mostly in a state of disarray and decisional confusion.Footnote 28 Different officials brought forth conflicting policies, often resulting in an inconsistent puzzle. Loosely speaking, however, Ahmadinejad designed the post-reformist priorities in countering drug and drug (ab)use. Maleki was the exception, but both Ahmadi-Moghaddam and Najjar represented the security-oriented and policing side of drug policy. The former was Mohammad Baqer Qalibaf’s successor as NAJA commander; logically, he followed a ‘tough on crime’ line. Once appointed, Ahmadi-Moghaddam went on reassuring that the entry of the police at the head of the DCHQ did not imply that all prevention programmes will be stopped. His compromise with the medical side of the problem was taken into account, in his view, by appointing as a caretaker of the DCHQ his deputy in the NAJA, who had a previous career as a medical professional.Footnote 29
Another aspect that characterised this period is the attempt at centralisation and de-bureaucratisation of drug policy. With the involvement of the police in the daily affairs (and, hence business) of treatment, the DCHQ tended also to centralise both budget and strategic decision-making in Tehran. The charging of NAJA as supervisor of the DCHQ preluded to a process of centralisation, which was meant to quicken state response to changing drug consumption patterns, while also ensuring implementation of agreed policies. At the same time, there was a general call among state cadres to ‘de-bureaucratise’ drug policy, as institutional obstacles were considered detrimental to effective policymaking. This approach was positively attuned with Ahmadinejad’s management of governmental affairs, exemplifying a political oxymoron. Centralisation meant that the government had the authority to change direction in drug policy – as much as in other fields of interest. It helped the rise of groups and agents aligned with the vision of the ruling cadres. That also enabled a faster and controlled privatisation of welfare and social services, outsourcing them to groups that reproduced the ideology of those in power, or those holding political capital. The oxymoron of centralisation and de-bureucratisation fine-tuned this game.
Soon after his election, the president issued the order to dismantle the highly efficient and reputable Planning and Management Organisation (MPO), and to transfer its duty to the president’s office. The move was allegedly justified by the president’s call for new thinking about the economy and the budget, a reckless inspiration that left deep traces in the economy and that established a paradigm for other sectors of public policymaking. This was Ahmadinejad’s ‘revolution in government’ moment. Similarly, the DCHQ made clear that ‘the fight against drugs, at a regional and provincial level, must proceed regardless of bureaucratic administration’.Footnote 30 This statement occurred on May 2007, while Ahmadinejad’s decision to dismantle the MPO was finalised in October of that same year, a coincidence implying that centralisation and de-bureaucratisation were two mutual processes during this era. Victims of this trend were scientific and expert groups in matters of drug policy (as well as economic policymaking). The government gained greater room for manoeuvre in budgetary allocation and management, much to the advantage of the NAJA and the DCHQ. The targeting of the scientific community and the ‘experts’ was part and parcel of Ahmadinejad’s government overall anti-intellectualism and mistrust towards transnational academic networks. It also suggests that the politics of drugs went hand in hand with wider political confrontations, usually categorised under the register of factionalism.Footnote 31 While the reformist government encountered lines of opposition in its push for policy change, the Ahmadinejad government did not face serious institutional challenges, as the Parliament, the Guardian Council and the Supreme Leader’s Office expressed sympathy and alignment with the ideology and political persuasion of the new government. Instead, it was intergovernmental infighting that characterised policy implementation during this period. This is evidenced by a set of different issues, such as the contrasting statistics and data that different ministries provided on the number of drug users, the existence, or not, of drug (ab)use among students, the supervisory authority with regard to rehab camps and, most problematically, the allocation of the budget.Footnote 32 With oil prices at unprecedented heights, the budget of the DCHQ had benefitted from state largesse. In 2008, the budget allocated to the DCHQ by the Majles totalled 77,386,200 USD – with a 40 per cent increase compared to 2007 – 45 per cent of which was allocated to supply reduction activities (i.e. policing, intelligence and anti-trafficking).Footnote 33 By 2013, the budget had shrunk to 6,768,000,000 tuman (ca. 4.5 million USD) due to a combination of low oil prices and the fall of the Iranian currency.Footnote 34 With lower budgetary allocation, internecine criticism surfaced as a trait of the post-reformist period, with NGOs lamenting the lack of governmental funds for their activities.Footnote 35
During the bountiful years, the DCHQ expanded its activities to such different fields as filmmaking, cultural events, sport training and musicotherapy, without much supervision and control, despite the reiterated calls for centralisation. In line with the short-termism of Ahmadinejad’s policymaking, the budget was used to renew infrastructures, buy new cars, refurnish the buildings and invest in any sort of social activity, without coherence and objectives. Part of it was dedicated to research projects and the creation of doctoral degrees focused on drug phenomena. While research and scientific investigation were sought to support policy interventions, the content of a considerable number of these academic programmes was limited in scope and methodology, and bounded to a framing of drug issues as exclusively epidemiological or, for that matter, moralising. Abundance of research into aspects of religious exegesis and drug use is one evidence of this; endless epidemiological publications is the other side of the coin.Footnote 36 Most of it is listed under the budget of the Ministry of Education that sponsors PhD grants and other types of university research programmes (Table 8.1). By 2014, however, only 3 per cent of all research on drugs and addiction could be said to belong to the social sciences, sensu lato, most of which lacked fieldwork engagement and critical analysis.Footnote 37 No serious historical, sociological and anthropological approach was encouraged over these years.
A case in point about the lack of practical results from investments in research is given by the murky and secretive nature of drug statistics (Figure 8.5). Reiterated calls for transparent numbers about drug use led to the creation of a national committee on addiction data in 2006.Footnote 38 Although the authorities had regularly published data on drug confiscation, arrests, people under treatment and numbers of clinics, other categories have been vaguely referred to or left ambiguous. Notably, statistics with regard to drug use among students have been systematically denied by the Ministry of Physical Education and Training, while researchers have referred to this phenomenon on several occasions, prompting a journalist to publish an editorial asking, ‘In the end, are there or not addicted students?’Footnote 39 Ultimately, the DCHQ clarified that the government had data on youth addiction, but that these data were secret (mahramane) and were only available to high-ranking officials. This prompted other officials to argue that up to 30 per cent of the 3.3 million students in Iran were addicted (where ‘addicted’ meant, vaguely, hard-drug consumption).Footnote 40 Ipso facto, the creation of research units and statistics taskforces did not lead to significant development of legibility and of in-depth knowledge of the phenomenon. One reason for this is provided by the fact that the DCHQ has only disclosed fragmentary information about its epidemiological studies of drug abuse, allegedly, due to the weak methodology of the study.Footnote 41

Figure 8.5 Percentage of Drug Control Budget in 2014 (in millions of rials)
When not spent in research, DCHQ money was often mismanaged. In the words of a public official, ‘in previous years, in some cases, the money for researches in the field of drugs was even spent for aviculture and fish farming’.Footnote 42 Another official explains that ‘the Prison Organisation and the Welfare Organisation … used the money to build services which were not for addicts, but, for example, were used to build other prisons and centres of support, so we decided this time to take control of this budget’.Footnote 43 Public criticism and accusation of mismanagement and corruption were in tune with those against the rest of the post-reformist government. New cars, expensive mobile phones, unnecessary gadgets and travels, compelled the director of the DCHQ, in 2007, to make a disclaimer, refuting the idea that many had established about the DCHQ as a ‘generous charity organisation’.Footnote 44
The Plateau of Ten Thousands NGOs
The lack of a supervisory budgetary system and the negligence of bureaucratic procedures made governmental action in the field of drugs, to say the least, adventurous and haphazard. This does not signify, however, that a strategy did not exist during this period. On the contrary, the strategy for intervention occurred, even systematically, through indirect channels, intermediaries of the state and outsourcing mechanisms. Within few years into Ahmadinejad’s presidency, Iranian civil society counted more than ten thousand different NGOs/charities in the field of drug abuse and harm reduction alone.Footnote 45 Evidently, the number needs to be anatomised, as its quantitative and face value does not often match its qualitative contribution in practical terms.
The mushrooming of NGOs during this period stemmed from the same logics that determined the privatisation of addiction recovery, notably the methadone clinics. In the same way as medical practitioners opted to run methadone clinics, often with only rudimentary knowledge of drug abuse problems, charities and support groups for addiction recovery were being registered by former drug users and laypeople out of philanthropic, personal or familiar interest in the field of rehabilitation. Many also realised, perspicaciously, that the field of addiction treatment was lucrative. In Iran, most NGOs operating in the field of addiction benefit from some kind of governmental support, however limited it may be. Especially during the first years of the post-reformist government, NGOs benefited from the largesse of the DCHQ; once the generous financial support came to an end following the drop in oil prices in the early 2010s, there were considerable recriminations against the paucity of support and consequent budgetary tightening.Footnote 46 Ahmadinejad himself referred to the question of non-state organisations, pledging the government’s plan to strengthening the role of NGOs working on addiction recovery, by providing specialised public support.Footnote 47 The range of organisations covered anything from public awareness initiatives to needle exchange programmes, family support, post-incarceration assistance and other activities. The methods and philosophy of action among these NGOs differed significantly and, in some cases, rivalry between different organisations reached the point of conflict. A rather hilarious case was represented by the banner exposed by a leading NGO, Congress 60 (Figure 8.6). Out of one of the windows in its central building, which overlooked on the court of a detoxification centre of another NGO, the banner said, ‘the addict was not beaten by a snake, so you don’t need to detoxify him [‘de-poison’, samzodai]’.Footnote 48

Figure 8.6 Congress 60 weekly gathering in Park-e Taleqani
As the number of these organisations does not allow adequate and thoughtful consideration of all, or even some, of them, I shall pay heed to those more paradigmatic (Table 8.2). A unique case is represented by Narcotics Anonymous (Mo‘tadan-e Gomnam, aka NA), whose appearance and spectacular expansion encapsulates the multifaceted trends of post-reformist civil society and governance of addiction.
Table 8.2 Comparison of Drug Addiction NGOs
Narcotics Anonymous: Recovering Spirituality
Based on the frame of its mother organisation in the United States, Narcotics Anonymous is an Iranian NGO with numerous centres across all cities and villages of the country, which operates as a self-help group following the philosophy of the twelve-step programme (common also to Alcoholics Anonymous). These are accompanied by ‘12 Traditions’, which provide general guideline for the management of NA as a whole and its self-care groups. With its emphasis on God’s ultimate power over the individual and its spiritualising commitment to sincerity and mutual support, the group soon found sympathetic minds among the population. By the early 2010s, arguably, every city and many villages had at least one NA group within their districts. Although it is problematic to quantify the membership, NA followers exceeded half a million, and its self-help groups regularly met in prisons, treatment and rehab camps, and often within the meetings and spaces of other NGOs. In 2014, there were about 18,195 weekly NA meetings in Iran, with the capital Tehran also offering English-language meetings.Footnote 49 If Iranian society had among the highest numbers of drug (ab)users worldwide, it also had the highest ratio of NA members.Footnote 50
The sheer size of Narcotics Anonymous during the post-reformist period endowed it with an especial status vis-à-vis the state. At the time of its first appearance in 1994, many regarded the organisation with suspicion. Its founder Foruhar Tashvigi had come in contact with the NA system while living in the USA and, once back in Tehran, faced with friends and family members seeking support for their drug (ab)use, decided to start self-help groups in the capital.Footnote 51 These meetings soon developed into larger networks of people and became publicly prominent throughout the country. Despite NA’s adamantly non-political nature, the organisation faced backlash from the state. The conservative clergy soon prompted ideological opposition to the rituals and activities of these groups, because of the reference, typical of NA gatherings, to unorthodox spirituality, which was inconsistent with traditional Shi‘a theology and eschatology. The accusation of proselytising and staging confessions – a practice which is alien to Islamic practices and may be a derivation of Catholic rituality – were moved against the NGO, which stopped its activities for the public in 1995. During the early 2000s, NA meetings were again permitted; Christensen holds that they ‘were modified and were Iranized’ to make them more acceptable to the authorities.Footnote 52 With its persuasion for pluralistic interpretations of religion, the reformist government facilitated the expansion of NA activities, acknowledging their humanistic contribution for those seeking support. The meetings were also a steady relief for recovered drug users to whom the state could hardly provide help.
The Ahmadinejad government did not hamper NA activities either. With its priority on prayer, responsibility and aggregation, Narcotics Anonymous chartered in friendly waters with the populist, yet highly spiritualising, religiosity of the post-reformist president. Although Ahmadinejad’s rhetoric was imbued with Shi‘a messianic ecstasy, it was also deliberately folkloric and anti-intellectual in its spontaneity. Alike the prayers of NA meetings and the devotion of its members, it defied, ambiguously, the schemes of religious orthodoxy and the clergy. The accusation of proselytising, the use of Catholic-inspired confessions and admissions of guilt – all of which are alien to Islamic doctrine – did not prevent popular and traditional strata of society from joining NA meetings, much as Ahmadinejad’s religious heterodoxy was not perceived as alien or misplaced by the urban poor and the plebiean masses.Footnote 53 All of this had the potential to challenge the clerical authority over divine mediation and spiritual healing.
Personal encounters with NA members confirmed the consonance of this organisation with the broader post-reformist (govern)mentality. On several occasions, NA members asked me what I believed in. To my scepticism and temporising, one member, a fifty-year-old taxi driver, anxiously told me, ‘I believe in this one entity, which is God [khoda], no matter what God; it is energy [in English], light and it gives me the strength to be responsible of my work [mas’ul be karam]’.Footnote 54 Another explained to a journalist about the steps of his recovery: ‘the second step was when I found hope [omid] in the only and superior force of the Universe that could help me, which is God … for the third step, now, I need to be ready to entrust my will to live to this compassionate God’.Footnote 55 One element that recurred during my meetings with NA members – whose milieux included working class people such as business holders, women and men alike – was typified by the reference to the philosophy of NA as a comparative advantage in the job market. A rehab camp manager, proud of his NA membership, lamented that ‘unlike in the US, where employers prefer AA or NA members, because they are more reliable and disciplined’, Iranian employers ‘think that if you are an addict you are helpless’.Footnote 56 Self-discipline and group membership were two distinctive traits of NA to which members referred to legitimise their reliability as workers, employees and, ultimately, citizens. There are also episodes in which the NA system, through the personal network that it establishes, facilitates the life of its members, for instance, in finding a job, an accommodation or even a partner. The application of the twelve-step philosophy in the context of the Islamic Republic has given birth to a melange of universalising spiritualism with Islamic reference. By teaching, in NA words, ‘the spiritual ways [osul-e ma’navi] of sincerity [sedaqat], optimism [roushan-bini], faith [iman], positive tendency [tamayol] and humility [forutani]’, it also propagated the proper ethical lines of the post-reformist presidency, in which optimism, faith and humility have been key traits.Footnote 57 By the early 2010s, NA meetings were held in sporting centres, hosseiniyeh and locations often used for official religious gatherings.Footnote 58 None of these has precedents in Iran’s history and the language of NA spirituality is highly globalised, with its references bypassing Iran’s traditional syncretism. Ist NA nothing but a secular expression of a religious sentiment? Or is it a spiritual profession of Iranian secularity after the demise of the modernist dream, embodied in its fight against addiction?
When the Narcotics Anonymous world service in the United States was invited to visit the Iranian branch of NA, the amalgam of religious enthusiasm with mass participation astonished the US visitors. During a visit in Qom, Iran’s religious capital, a man approached the representative from the US branch and, looking into his eyes, said ‘you are my belief’!Footnote 59 The fact that this vignette occurred in Qom and during a period of high tension in US–Iran relations makes this all the more significant and illustrates the dimension and intensity of the NA phenomenon in Iran, one that truly deserves research, the scope of which bypasses this book.
From a governmental perspective, NA amalgamated, spontaneously, with the post-reformist push for entrusting social and health programmes to the drug (ab)users themselves, minimising, in one move, both financial expenditure and moral involvement in the pernicious affair of addiction. As a senior member of NA recalls, ‘[since 2005] with the spiritual help of the government, we have been active also outside rehab centres, through our meetings’ in parks, buildings, theatres and town halls. The organisation benefited from the reformist government’s spiritual support, but, based on the NA constitution, it could not accept financial aid from outside entities. The entire organisation runs with money from the members and donations from those who benefit from its meetings, a principal reason it is considered less politicised. NA distributed 1.7 million information pamphlets about drugs and addiction yearly,Footnote 60 a datum that explains the governmental role with which this NGO has been progressively entrusted. In 2013, Narcotics Anonymous was voted the top NGO by the government. Based on its status as a non-governmental entity, the prize was received by its sister NGO, Rebirth (Tavalod-e Dobareh). NA representatives take part in meetings of the DCHQ and other policy circles, but not as members of Narcotics Anonymous. Their policy branch within the civil society world is Tavalod-e Dobareh, ‘Rebirth’.
Rebirth: Grassroots Authoritarianism and Twilight Institutions
In order to strengthen therapeutic support for drug users, the founder of NA Iran created Tavalod-e Dobareh in 1999. Since then, Tavalod-e Dobareh has provided support to drug (ab)users in the guise of rehab centres, shelters for homeless drug users and counselling services. Tavalod-e Dobareh was initially conceived as a sister organisation of NA, which followed the twelve-steps philosophy. It did not seek external support and operated through a strictly non-profit vision.Footnote 61 With the approval of the harm reduction policy and its scaling up during the post-reformist period, Tavalod-e Dobareh progressively established itself as a ‘super-NGO’, with broad governmental duties and an active presence in the policymaking debate. It became a major beneficiary of public funds in the field of addiction recovery and, for that matter, drug policy. As an NGO, Tavalod-e Dobareh has a permanent seat in the Civic Participation Programme of the DCHQ, often providing on-the-ground knowledge about the state of addiction in the country, while also cooperating (and criticising), very much off-the-records, with the NAJA in its programmes of ‘therapeutic policing’ and ‘collection of dangerous addicts’ (tarh-e jam’avari). Recently, it has also started a vast, long-term programme on addiction studies, which is meant to establish the NGO as a research hub on drug abuse in the MENA region.Footnote 62
In his own words ‘a former drug addict with seventeen years of cleanness’, Abbas Deylamizadeh is the outspoken and charismatic director of Tavalod-e Dobareh, whose appearances on the national TV and interviews with local and foreign newspapers have gained him notoriety in the field and a reputation in policy circles.Footnote 63 Abbas, as most colleagues call him, stresses the importance that he gave to ‘the organisation’s academic output’, ‘collaboration with joint researches with national and foreign academic institutions’, ‘publishing in reputable and well-known journals’.Footnote 64 In one of our meetings, I had the impression, for once, of being in front of a career service panel, or a demanding supervisor, drafting the strategic vision of a research institution. Yet, this drive towards academic production does not simply concern an attempt to build public awareness or to integrate the world of policy with that of research – a mirage called also evidence-based policymaking. Infatuation with the academic world – the director read for a PhD degree in Economic Management in the island of Kish – is a common trait of policy circles where status is buttressed by titles and degrees. Research prestige goes hand in hand with the imperative of securing funding for the NGO and being competitive against other organisations. An academic profile would secure Tavalod-e Dobareh a competitive edge over other organisations, given Iran’s PhD-obsessed mentality.Footnote 65
What distinguishes this NGO from the multitude of other organisations is not its research drive, but its nationwide structure of intervention with regard to addiction recovery and its complementarity with the post-reformist governmental strategy. With this is mind, Tavalod-e Dobareh provides insight into the post-reformist management of the drug phenomenon, highlighting its ‘twilight’ nature: not a state institution, Tavalod-e Dobareh exercises both public authority and governmental duties.Footnote 66 The twilight nature of the NGO, however, does not hint at an inherent weakness of the state, as it does for twilight institutions discussed in other regional contexts (e.g. Africa by Christian Lund or the Middle East by Nora Stel). Instead, the twilight nature of Tavalod-e Dobareh unfolds how the state retreats from those spaces and situations posing a threat or challenge, or where its interference is unproductive and cumbersome.
‘With regard to the economic side of the problem of addiction’, Deylamizadeh claimed during a public speech, ‘we have to remind one point. Unfortunately our approach is that in order to deal with addiction we spend [hazineh], while we should invest [sarmayegozari]’.Footnote 67 His call for investment into treatment was a timely one. Tavalod-e Dobareh manages a large number of rehab camps and has been charged by the government with the provision of services, through DICs and shelters for homeless people. The fact that the director of this organisation speaks a language that policymakers understand – notably the language of numbers and of capital [sarmaye in Persian] – has helped Tavalod-e Dobareh gain further legitimacy. As quantitative, econometric analysis had helped the acceptance of harm reduction, the use of numbers is instrumental to justify funding requests or to point out an emerging crisis:
We have a 43% rate of success; it means that during these years, 43% of those who came to our [rehab] camps at the time of dismissal, and after, have preserved their ‘cleanness’, between two months and six months … Today 1,825,000 tuman [ca. USD 2400] is spent for one addict per year, and we don’t know if this bears results.Footnote 68
Through a mathematical calculation, the director of the NGO attempts to demonstrate that he can provide a successful method to cure a large number of people, while spending less. Where these numbers came from, I must admit, remained vague. Moreover, Tavalod-e Dobareh follows the NA philosophy and therefore its treatment facilities do not provide pharmaceutical cures, like methadone, which alone require higher expenditure. In addition, the organisation maniacally keeps track of the number of syringes that it distributes and collects, of condoms it provides during outreach programmes, of leaflets and brochures and meetings.Footnote 69 The effect is startling and enables the NGO to present itself as a highly reliable, technically sound and professionally engaged entity. Another key aspect of the rehab centres managed by the NGO is that these services, per se, function as employment venues for many former drug users. Given the difficulty for many recovering addicts to find a job in Iran’s already problematic market, the NGO plays an important part in involving former service-seekers into the management of the facilities, basically ‘keeping them busy’.Footnote 70 The creation of employment has been a long overdue task for the government, which is conscious of the fact that, without the complex network of NGO centres, many former drug users would remain unemployed, which potentially increases the risk of relapse. Yet, this form of occupation is not faultless. While visiting different centres of Tavalod-e Dobareh in Tehran, several lower-ranking members expressed their disaffection with the management as well as payment of stipends. A thirty-year-old female social worker, graduate and mother of two, who was in charge of psychological counselling, criticised the central office, pointing out that NGOs – including Tavalod-e Dobareh – have become a mechanism ‘for money making [pulsazi]’. She also added, ‘I am paid 400,000 Tuman [ca. 140$] per month and they don’t even want to cover my medical insurance … After I leave work here, I go and work in a [private] methadone clinic in another part of town, because I need to survive in this city’.Footnote 71 Another employee in charge of the kitchen of a DIC in southern Tehran confessed, ‘I earn 170,000 tuman [ca. 60$] per month and I spend every single day of the week here in the DIC. I like my kitchen and I like cooking for people, even though I can prepare only adasi [lentil soup] with the few things that are left in the cupboard’.Footnote 72
Because resources and support from the central office of Tavalod-e Dobareh are limited, the local DICs and rehab camps demand support from the community or from the families of the service-seekers, an endeavour which is made more difficult given the marginal location of these centres and the lack of family relationships among most of the people frequenting them. Indeed, few of the people who help running these centres stay longer than a few months, because the stipends they receive are too meagre. The organisation counts on the fact that many recovered addicts want to take part in the management of the activities and tend to accept little or no pay. Among the three volunteers that I met during a week spent in the Farahzad Shelter, none of them received financial support from the NGO. The shelter, located in one of the so-called risky zones of Tehran, hosted up to fifty homeless drug users every night, most of whom hung out in the nearby patoq (‘drug den’) (Figures 8.7 and 8.8). The three-man team would fulfil multiple duties, including that of outreach team providing clean needles and condoms, collecting used needles, nursing infections and scars and referring drug users to rehab and clinics.Footnote 73 Apart from physiological cigarette breaks, their work required high alert and great motivation and temper all day long, plus a set of skills in medical intervention that was beyond rudimentary (Figure 8.9).


Figure 8.8 Sanitary Intervention by Outreach Programme

Working with no money was probably a consequence of the NA ecosystem to which Tavalod-e Dobareh belonged initially. Having said that, the volunteers’ uneasiness with this system was profound, especially when faced with the sophisticated status of the Tavalod-e Dobareh’s central office. There, the personnel, most of whom had a history of drug abuse and went through the NA path, were given relatively good stipends, vouchers for lunch and transportation, and could benefit from other amenities that are part of the NGO assets.Footnote 74 By creating this model of recovery through the work of the NGO itself, Tavalod-e Dobareh promotes a vision of life in society aligned with the idea of a careerist individual, who is responsible and, hence, can ascend to professional success. This spirit was very much at the heart of the director’s solidarity to drug abusers and his desire for academic output. But it also unwrapped the ways in which the marketization of drug treatment (even when charitable and non-profit) had materialised during post-reformism. Once again, the drug market engendered a pathological marketization.
The vision behind the expansion of Tavalod-e Dobareh is that ‘every addict, regardless of his history of use and type of drugs, should enter a camp [ordugah] for addiction. Then, we call him/her a path-seeker [rahju] … But if he uses drugs while there, he is immediately sent out!’Footnote 75 This vision overlapped with the strategy that the post-reformist government had envisioned about harm reduction. In a way, the rehab camps that this NGO operated complemented the state-run camps, supplementing their organisational and logistical incapacity to address the multitude of drug (ab)users. In order to implement this strategy, Tavalod-e Dobareh had formulated a system based on ‘half-way houses’ (khane-ha-ye nime-rah).Footnote 76 In these ‘houses’, the ‘path-seekers’ find a place to stay after the twenty-eight days of mandatory recovery in the camp; they stay there for up to one year, with other people, making it ‘very similar to a student house’. The main objective of these ‘houses’ is ‘to preserve the public space from the recovering addict’, who ‘cannot get out of the house for the first three months’.Footnote 77
These plans have received support from the government of Mahmud Ahmadinejad, who identified in Tavalod-e Dobareh, a model of civil society responsive to (un)civil phenomena. Already in 2004, Ayatollah Khaz‘ali, a top cleric sitting in the Assembly of Experts, met with the founder of Tavalod-e Dobareh to congratulate his efforts, echoing the Khomeinist proverb, ‘saving one addict is saving a generation’. In the years that followed, the organisation met and lobbied among a number of prominent clerics, including Khomeini’s grandson Hasan, with the intent to gain legitimacy and support within the implementing machinery of drug policy.Footnote 78 The creation of a news agency, managed by Tavalod-e Dobareh, focused on drugs and addiction also came to play an instrumental role in the public pressure campaign of the NGO. From the late 2013 onwards, the Addiction News Agency (ADNA) became the centre of gravity of most information related to public statements and debates around drug policy reform and, although it presented conflicted opinions and different policy perspectives, it operated in order to put pressure on policymakers. In ADNA, the drug policy community displays its public face and struggle.Footnote 79
With its nationwide network of centres and a multitude of people willing to engage in its activities, Tavalod-e Dobareh had the infrastructure and means to complement the state in an area of intervention which had become troublesome ethically (e.g. harm reduction during post-reformism), and cumbersome economically (e.g. the cost of ‘free treatment’ for a multitude of people). The NGO covers also harm reduction practices across Tehran and other major cities, providing shelter facilities, mobile clinic centres in Southern Tehran, DICs as well as in-patient and detox venues of all kinds, including for younger people. It operates twelve major centres (both DICs and rehab centres) in Tehran, ten in the province of Shiraz and a dozen more across other regions. Some minor NGOs, which operate at local levels, associate themselves with this umbrella NGO, often with the purpose of increasing their chance to acquire funding, visibility and legitimacy.
But the contribution of Tavalod-e Dobareh has gone beyond these calculations. By proposing a vision based on hierarchy, self-management, quantitative results and individual responsibility, without tackling deep-seated political shortcomings, the NGO embodies an authoritarian model at a grassroots level. This model does not necessarily require adherence to ‘law and order’. Indeed, this has been opposed by Tavalod-e Dobareh rather vehemently. Instead, this model enacts strict rules of inclusion in the community – which is the NGO itself – for those individuals who wish to recover, by redeploying former drug (ab)users as working elements in the daily operations of the NGO. Without providing a path to ‘return to normal life’, recovered addicts become a self-perpetuating machine in the management of the drug crisis, by supervising rehab camps, participating in outreach programmes, taking care of administrative affairs or cooking meals in a DIC. As a confirmation of this mechanism, the director explained in a letter to the state authorities, that the weakening of harm reduction services in the DICs is problematic because these centres provide employment to the recovered addicts and involve them in social activities.Footnote 80
That Tavalod-e Dobareh acquired a governmental role within drugs politics is also confirmed by its collaboration, on a regular basis, with law enforcement units. The ‘drug addicts’ collection plans’ had been a sphere of action in which the expertise and knowledge of the NGO proved critical for the NAJA. Tavalod-e Dobareh’s access to the patoq (hotspots) gained the NGO the status of especial interlocutor. In fact, one could argue that with its involvement in arrests and referrals to compulsory camps, the NGO has defied the fundamental ethics of harm reduction, which is rooted in the absence of judgement on drug use and opposition to policing methods. Instead, it has operated as a mechanism of grassroots control, with the task of legibility, management of critical phenomenon and facilitator of state intervention. The NGO operates as a rhizome (from the Greek, mass of roots) of the state, which, instead of reproducing vertical lines of control and power relations, becomes diffused and horizontal – similar to the roots (rhizomes) of a plant. When societal control is practiced, this is cropped out through the rhizomes that stem from the horizontal roots of the state itself, camouflaged as other forms of intervention, i.e. civil society. For those arguing that post-reformist Iran witnessed increased top-down security, the metaphor of the rhizome is a reminder that power and authority operate through diffused and grassroots lines of production. This form of governance is what I define as the art of managing disorder (Figure 8.10).

Figure 8.10 Rhizomes and Grassroots Authoritarianism
Among the instances of Tavalod-e Dobareh’s collaboration with LEAs, one in particular had resonance among street drug users and the public. In the wake of the important Non-Aligned Movement Summit (NAM) of Tehran in August 2012, the authorities requested those NGOs operating in the patoqs and having knowledge about ‘street addicts’, to facilitate their collection – i.e. arrests – for the period of the meeting. A week ahead of the event thousands of street drug users, as well as large numbers of homeless vagrants, were gathered and sent to state-run rehab camps to, allegedly, be treated for addiction.Footnote 81 The obvious rationale was the cleansing of the city in view of the international meeting, which was expected to rejuvenate the NAM in the post-Arab Spring context, and show the spotless beauty of the capital.
The collaboration with the police goes beyond material support. Tavalod-e Dobareh has been discussing the possibility of taking over the management of compulsory camps – currently under the supervision of the NAJA. The NGO pledged to rehabilitate around 60 per cent of the drug abusers if given the chance to operate the facilities, a numerical data which is exponentially higher than the current official ‘rate of success’.Footnote 82 In this regard, too, the NGO is reminiscent of Ahmadinejad’s style of government, both bombastic, fictional and retracing a fundamentally populist governmentality with authoritarian overtones . One can interpret the nature of this super-NGO, through the ambiguous combination of welfare activities with a securitising persuasion. The outcome, it seems, blurs and contaminates the confines and boundaries of what is normatively regarded as the Iranian state, described as a top-down project with grassroots participation, and what is numbered under the constellation of civil society, which is hereby re-enacted as a grassroots model of authoritarianism, and not a panacea enabling democratic transition.
Conclusions
‘If we make our drug policy based only on one approach’, a state official confessed, ‘it is as if we had an economy based only on one product, which means there is a high risk of failing and ending up badly, for which there is no cure or treatment. From this point of view, the duty of the government is to support indirectly the self-help groups and the NGOs’.Footnote 83 The post-reformist language of the state has tendentiously emphasised national commitment, as opposed to governmental duty, to fight drugs and to prevent addiction – not in line with the Islamist motto: ’amr bil-ma‘ruf wa nahi ‘an-il monker, ‘commanding good and forbidding evil’. What materialised, instead, in the field of state intervention was more consonant with practices of neoliberal governance in times of crisis. The coexistence of a moralising rhetoric and securitising gaze, with a push for privatisation and outsourcing, went hand in hand as the post-reformist government sought to ease the burden of a publicly visible and financially cumbersome drug phenomenon. The field of addiction, over this period, increasingly became the turf of private clinics and, along its margins and more problematic populations, of NGOs. In this, it produced a rupture with the past.
The maintenance of a security-oriented approach was deemed necessary but not prevalent in countering drug (ab)use. The security approach (nezami), in the words of a prominent drug policy official, was required because ‘otherwise addicts are not pressured to give up’. This method, added the official, ‘has the objective of building the will [raghebsazi] of the addict … through targeted pressures’.Footnote 84 With policing methods overlapping with treatment imperatives and, as in the case of Tavalod-e Dobareh, harm reduction practices, the state pressured the marginal groups of drug (ab)users, with the prospect of institutional rehabilitation, or incarceration. While adopting a language of quantification of social phenomena, cost-and-benefit analysis and epidemiological surveys – neglecting societal and politological introspection – the state and prominent NGOs, such as NA and Tavalod-e Dobareh, worked along compatible, intertwining lines. These differed substantially from the ways civil society had engaged with the state – and vice versa – during the reformist period. At that time, mentioning critical phenomena, such as HIV epidemics, played a constructive role in formulating new approaches to drugs and drug (ab)use. Later, in the post-reformist era, the lines of enquiry insisted, on the one hand, on the return to religious-revolutionary orthodoxy as a solution to the multiple, oft-denied, crises. On the other hand, this zeal denoted a variant of neoliberalism, à la iranienne, with marketization of private treatment, governmentalisation of (un)civil society and policing of disorderly margins. The contours of state imperatives were drawn, consequently but unsystematically, by the economisation of political interventions, through a combination of medicalisation (through methadone) and harm reduction securitisation, one via clinics, the other via NGOs and charities, managing addiction recovery in the camps.
This art of governing crisis and managing disorder was distinctive to the post-reformist state, whose mechanisms of power did not arise from either strict ideological rules, nor monolith interest groups, but evolved from the confluence of multiple lines of interventions, which had the ultimate objective of containing, dispersing (also topographically) the crises. The performance of this strategy was diffused and propelled through grassroots elements, via rhizomes of authority, which operated in the twilight zone of state/society. In this example, one can find new empirical material for understanding governance under post-reformism. Thus, populism managed the crisis.
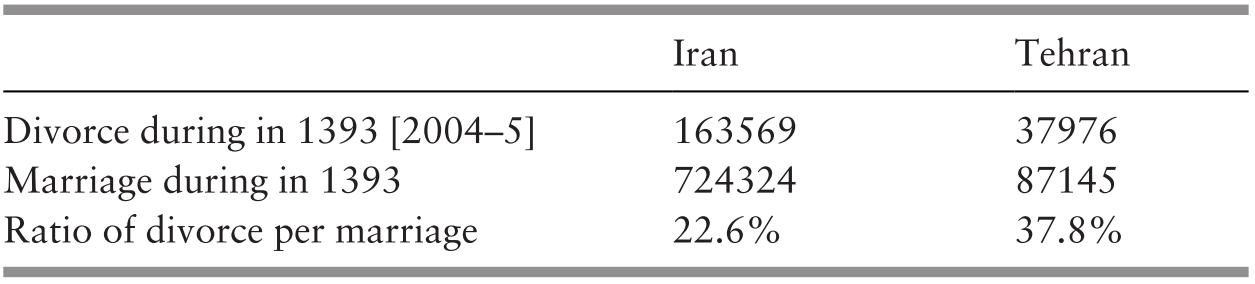






















 Open access
Open access