



Introduction
At the end of 2019, Wuhan, the largest city in central China, was assailed by an unpredictable outbreak of a new coronavirus now known as severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2), which causes the coronavirus disease 2019 (COVID-19). Within a short time, COVID-19 spread nationwide, and when it spread worldwide was soon recognised by the World Health Organization (WHO) as a pandemic [1]. Due to the high susceptibility to infection and fast spread of COVID-19, the size of the infected population in Wuhan grew with a remarkable speed. This caused many general hospitals in Wuhan to face great challenges, especially the shortage of hospital beds and medical resources. To address this situation, 16 Fangcang shelter hospitals were built in Wuhan as a low-cost solution for shortage of hospital beds, and to quickly provide basic medical care for non-severe COVID-19 patients [Reference Chen2].
After two months of hard work in all aspects of society, the outbreak was effectively brought under control. As the number of COVID-19 cases dramatically declined, the emergency Fangcang shelter hospitals were gradually closed, and local general hospitals gradually restored normal medical order and functions. However, isolation wards were still needed to treat the remaining COVID-19 patients and to prevent outbreaks within general hospitals containing fever clinics.
A shortage of isolation wards in the fever clinic of the West Campus of Wuhan Union Hospital became an increasingly prominent problem as general hospitals without permanent fever clinics stopped treating COVID-19 patients. In order to solve the fever clinic bed shortage and to ensure that all patients with fever in the service area of the West Campus of Wuhan Union Hospital were managed effectively, an innovative concept was put into practice. A complex of mobile isolation wards was built beside the fever clinic to increase the number of beds. These mobile isolation wards have played a critical role in controlling COVID-19 in the late stages of the pandemic in Wuhan.
Establishment of mobile isolation wards at the fever clinic in the West Campus of Wuhan Union Hospital
On the basis of an order from the Wuhan COVID-19 Outbreak Prevention and Control Command, all patients with symptoms of fever must go through a process of ‘isolation, observation, screening and triage’ [3]. This process must occur within a designated hospital's fever clinic. In addition, all people who returned to Wuhan for work required COVID-19 nucleic acid and antibody tests, and a computed tomography (CT) chest scan. Those with negative nucleic acid test results could return to work. People with positive test results needed to be isolated for observation in a designated hospital's fever clinic. The fever clinic within the West Campus of Wuhan Union Hospital had only eight hospital beds for isolation and observation, which was not sufficient. Therefore, a complex of mobile isolation wards was built at the fever clinic to solve the above problem (Fig. 1).

Fig. 1. Mobile isolation wards outside the fever clinic at the West Campus of Wuhan Union Hospital (A, B, C), and one of the inside channels (D).
On 8 March 2020 most of the Fangcang shelter hospitals and isolation stations within Wuhan Economic and Technological Development Zone were closed. Simultaneously, the new mobile isolation wards at the Wuhan Union Hospital's West Campus were put into operation. The mobile isolation wards were managed by the fever clinic. By 24 March, the total number of admitted fever patients who went through the ‘screening, isolation, observation and triage’ process was 83, nine of them being COVID-19 patients. The mobile isolation wards alleviated the stress on the fever clinic by solving the patient's bed shortage. With the bed shortage solved, the hospital adequately and safely examined a large number of fever patients.
Three key characteristics of mobile isolation wards
There are three key characteristics of mobile isolation wards: (1) rapid construction with a small budget, (2) shared resources with the fever clinic and (3) a nucleic acid testing station.
The first key characteristic is rapid construction with a small budget. The construction model for the mobile isolation wards is based on a traditional battlefield hospital, which can be traced back to the Napoleonic wars [Reference King4], combined with the design of the Beijing Xiao Tang Shan hospital which was affordably, and rapidly built during the 2003 SARS battle [Reference Wang5]. The mobile isolation wards at the West Campus of Wuhan Union Hospital was built from assembled containers. These containers were identical to the mobile shelter wards in the Huo Shen Shan Hospital that was built for treating COVID-19 patients. Each assembled container is 6 m long × 3 m wide × 2.5 m high. The construction of the mobile isolation wards required little site preparation. Only the flattening and hardening of the ground where the complex was placed were of vital importance. This allowed for rapid and effective installation, so the wards could be quickly used. With the support of the local government, 25 preassembled containers were installed within 48 h. The capacity of the mobile isolation wards complex was 20 patients. The small size of the complex is more cost effective than building a new traditional general hospital or shelter hospital.
The second key characteristic of mobile isolation wards is the sharing of medical resources with the fever clinic. When faced with a large number of patients with fever, the sharing of resources with the fever clinic prevented a shortage of human resources and equipment. At the West Campus of Wuhan Union Hospital, there was a 10 000 m2 open space adjacent to the fever clinic. This area was ideal for the placement of mobile isolation wards and easily allowed for the sharing of medical resources, such as registration, sampling and CT examination with the fever clinic. The mobile isolation wards also shared the fever clinic's treatment station, medical staff office and storage room, which reduced the need for extra space.
The third key characteristic of mobile isolation wards is their use as a COVID-19 testing station. When a hospital returns to normal operation after treating only COVID-19 patients, the testing of new patients for COVID-19 antibodies and nucleic acid can be completed in these mobile isolation wards. This model was applied at West Campus of Wuhan Union Hospital. It was also effectively used by the fever clinic at the Beijing Union Hospital, where five mobile containers were assembled within 70 h for the main purpose of COVID-19 nucleic acid testing.
Essential functions of mobile isolation wards
A fever clinic is critical in the first line of defense for pandemic prevention and control. The process of ‘isolation, observation, screening and triage’ of patients with fever symptom can be completed in a one-step manner in the mobile isolation wards. Patients with fever should first be tested for new coronavirus nucleic acid, antibody, routine blood analysis and C-reactive protein and given a CT scan. The first essential function is isolation. Since these mobile isolation wards were independent of each other, isolating patients with fever within the mobile isolation wards can reduce the patient's mobility and the possibility of further spread inside the hospital. The second essential function is screening and triage. Confirmed COVID-19 patients are transferred to the proper designated hospital to receive immediate treatment. Patients with a negative nucleic acid must be tested for nucleic acid again after 24 h to ensure COVID-19 negativity. Patients with fever symptoms due to other reasons were transferred to a non-COVID-19 designated hospital to receive proper medical treatment. As a third essential function, food and basic medical care were available for the patients during the observation period in the mobile isolation wards.
The construction model of the mobile isolation wards
Layout and design
The mobile isolation wards use a layout design called ‘three zones and three channels’ (Fig. 2), which is based on a similar layout that the West Campus of Wuhan Union Hospital used to treat COVID-19 patients during earlier stages of the pandemic. These three zones were: clean zone, potential contaminated zone and contaminated zones. The three zones were completely isolated from each other and were connected with a corridor which formed a functional complex. The clean zone was located at the office area of the fever clinic which was convenient for the daily work of medical staff, so no office space was needed in the mobile isolation wards where infection risk was high. The three channels were: medical staff channel, patient channel and contaminated channel for storing medical wastes (e.g. PPE from the contaminated zone). Routes of movement for medical staff and patients were strictly separated to avoid cross-infection. The 25 preassembled containers were independent of each other. Twenty containers were used as isolation wards with basic personal effects for daily use (Fig. 3). The remaining five containers were used for medical function and technical support units: a sample room, a buffer room, a medical staff room, a duty room and a storage room (Fig. 2).
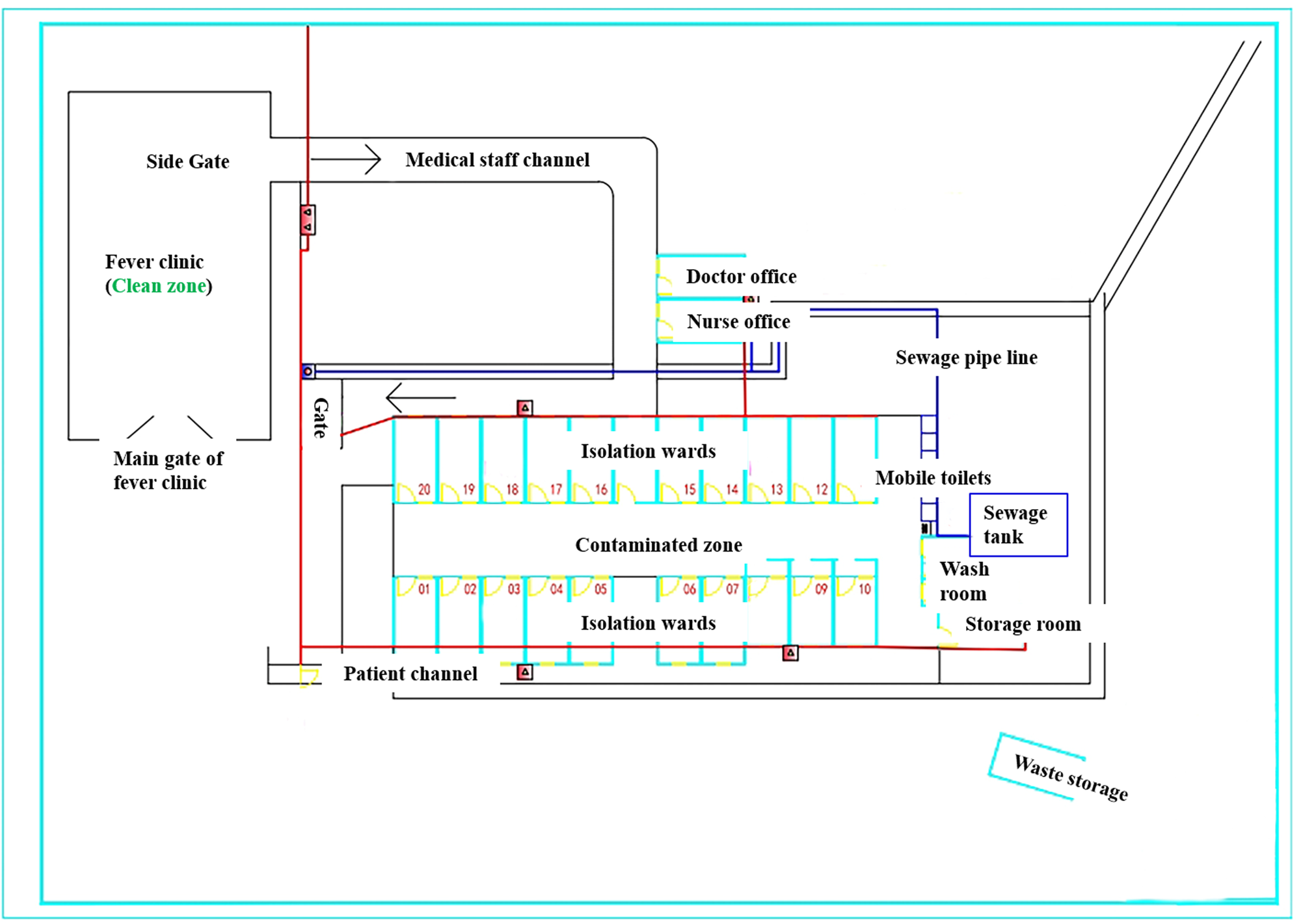
Fig. 2. Layout of the mobile isolation ward complex.

Fig. 3. The inside of a mobile isolation ward showing personal effects.
Network system
The mobile isolation wards were connected to the hospital with a high-speed network (Fig. 4), which facilitated communication between medical staffs and patients [Reference Zhou6]. When installing the network system, a local area network (LAN) access switch and a wireless router in the isolation wards were set up. The isolation wards access switch was connected to the fever clinic aggregation switch directly through a physical link to the central server. This connected the hospital information system to the mobile isolation wards. The wireless router was connected to the internet aggregation switch to achieve internet access. The mobile isolation wards were equipped with multi-angle cameras, a mobile communications system, a patient call button system and an emergency response system. An electronic access control system was also set up at key positions to prevent patients from accidentally getting in or out of the isolation wards.
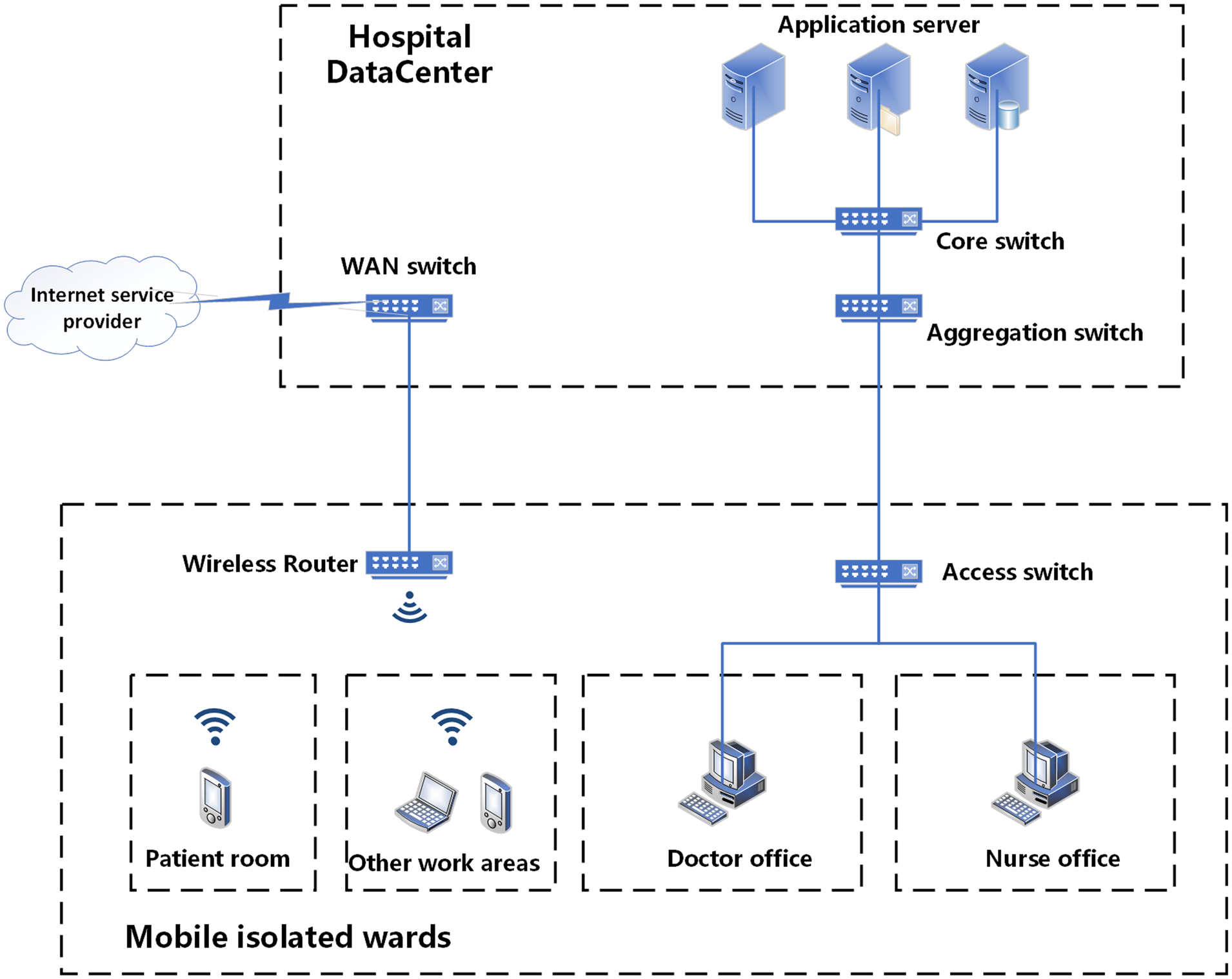
Fig. 4. 4 G network and information system in mobile isolation wards.
Water supply and drainage
To quickly put the mobile isolation wards into operation, water was only supplied to showers, toilets and the doctor and nurse offices to meet the daily need. There were two types of drainage: rain water drainage and sewage drainage. Ditches and gutters were added to discharge rain water into the municipal network. Since sewage disinfection and discharge play a key role in preventing further COVID-19 spread, sewage from the contaminated zone was gathered into a sewage tank by a sewage pipe line (Fig. 2) for special disinfection and later discharged [Reference Wang7].
Considerations for mobile infectious isolation wards
Two aspects that need to be considered when detecting and controlling infectious cases during a pandemic are outbreak stage and epidemiology.
Outbreak stage
Different stages of an infectious disease outbreak require different management strategies. Late stages can be difficult, because society is returning to normal function, but cases still exist to potentially spread infection. The mobile isolation wards were established during the late stages of the COVID-19 outbreak when the outbreak was mostly under control and the majority of the emergency Fangcang shelter hospitals were closed. The outbreak at this stage was fragmentary, but the risk of infection still existed. At this time, workers were gradually returning to Wuhan from outside of Hubei province, which presented a new concern and challenge in the battle against COVID-19. The concern was that the returning workers could cause a second outbreak. The challenge was that these workers needed to be tested, and isolated if COVID-19 symptoms were present. However, the number of hospital beds and wards in the fever clinic within the West Campus of Wuhan Union Hospital was insufficient to process tests for all of the workers sent to the hospital. Adding mobile isolation wards as an expansion to fever clinic reduced the workload of the fever clinic when it faced a large population that needed to go through the testing process.
Epidemiology
There are three essential epidemiological elements that contribute to a disease becoming a pandemic: (1) source of infection, (2) media and route of infection and (3) a population that can be easily infected. The mobile isolation wards controlled the movement of the source of infection while also cutting the routes or media of infection. This provided protection for the susceptible population by removing the source of infection.
The mobile isolation wards also facilitated the process of screening patients with symptoms of fever. For COVID-19, fever was the most common symptom. Therefore, enlarging the capacity of the fever clinic by adding mobile isolation wards increases the number of patients who can go through processing and isolation. This isolated COVID-19 patients from other people and the broader community, which prevented further spread of COVID-19.
Mobile isolation wards can also be used as the last treatment station for the final COVID-19 patients within a designated hospital in the late stage of a pandemic. Concurrently, other departments can gradually restore normal medical operation. Therefore, mobile isolation wards can provide precious time and space for a designated hospital to restore normal medical operation, while keeping COVID-19 cases isolated.
Comparison with a traditional mobile battlefield hospital and the Beijing Xiao Tang Shan Hospital
The concept and layout of the mobile isolation wards, is similar to a traditional battlefield hospital and the Beijing Xiao Tang Shan Hospital. However, mobile isolation wards are different in terms of function.
Compared to the Xiao Tang Shan Hospital, that was designed for the treatment of SARS patients [Reference Wang5] or a battlefield hospital which treats war casualties, mobile isolation wards in the West Campus of Wuhan Union Hospital were not responsible for the treatment of COVID-19 patients. The main functions of the mobile isolation wards was for triaging and observation of fever patients. Firstly, fever patients were triaged within the isolation wards with medical evaluations. Patients who had fever symptoms due to non-COVID-19 reasons were transferred to a non-designed hospital to receive proper treatment. Patients who were suspected to have COVID-19 were isolated in the mobile wards for observation purposes. Lastly, patients who had fever symptoms that were confirmed to be due to COVID-19 were separated based on the stage level of the disease (i.e. light, moderate, severe and critical). These COVID-19 patients were transferred to the designated hospitals for further treatment.
Secondly, the mobile isolation wards provide fewer beds than the Xiao Tang Shan Hospital or a battlefield hospital. A smaller facility with fewer beds allows for effective use of land compared to a battle field hospital or a Xiao Tang Shan style hospital, which requires a larger amount of space. In terms of budget, the cost is much cheaper than building a new hospital, which makes it feasible for developing countries, or third world countries.
Lastly, improvements should also be made on some aspects of the mobile isolation wards, such as how to avoid further infection [Reference Chen8], and provision of psychological therapy for patients (e.g. anxiety) therapy [Reference Li9]. Battlefield hospitals and the Xiao Tang Shan Hospital also do not usually and adequately provide these functions, which were found to be of need during the pandemic in Wuhan.
Conclusion
Within 16 days of the mobile isolation wards being functional, the total number of admitted patients with fever symptoms who went through the fever screening process that need isolation and observation was 83, with nine of them being COVID-19 patients.
The mobile isolation wards are a temporary building complex that was rapidly constructed and reduced stress on the fever clinic. They solved a series of problems during the pandemic, such as a shortage of examination rooms, medical supplies and CT and other auxiliary equipment. They also provide an orderly integration with the main fever clinic. The mobile isolation wards are still in use at the West Campus of Wuhan Union Hospital for the purpose of nucleic acid testing. Like SARS, fall and winter are generally the season for new outbreaks, so a minor outbreak, or a second wave [Reference Xu10] of the outbreak in the winter of 2020/2021 is predictable. Mobile isolation wards used as an expansion of a fever clinic can also be used as an ‘outpost’ to provide an early warning of a new outbreak or second wave. Reserving open areas beside a fever clinic for the rapid installation of mobile isolation wards is also recommended for a quick response to emergent health events.
Acknowledgements
We thank the healthcare workers and all other people working in and managing the mobile infectious isolation wards. We thank engineer Wenhua Peng of Wuhan Chedu Construction Development Co., Ltd. for issuing preliminary design and construction drawings according to the requirements of the hospital and participating in construction supervision. We also extend special thanks to Mr. Ryan James, BSc, professional biologist, from Alberta, Canada for English editing of this paper.
Author contributions
FJC conceptualised and designed the mobile isolation wards of the fever clinic within the West Campus of Wuhan Union Hospital and initiated and coordinated this study. ABC was a student of the Institute of Environmental Engineering, the University of Melbourne. He severed as a volunteer in the logistics office of the West Campus of Wuhan Union Hospital and participated in the design of channels, sewage. BZ participated in the design, construction and operation of the mobile isolation ward communication system. YG contributed to the design and implementation of mobile isolation wards of the fever clinic, and acquired key information. PS participated in the operation and management of the mobile isolation wards of the fever clinic, and acquired key information. HQ participated in the nursing management of the fever clinic, and acquired key information. ABC, YLC and FJC conceived this paper; ABC, YLC and RC wrote the draft of the paper and FJC critically revised the paper. All authors approved the final version.
Conflict of interest
All authors have no conflicts of interest to declare. No financial support was received for this research study.
Data
This paper does not contain any data.





 Open access
Open access