



Introduction
Research on subjective age has shown consistent discrepancies between one's chronological age and one's younger reported age (Rubin and Berntsen, Reference Rubin and Berntsen2006; Montepare, Reference Montepare2009; Kotter-Grühn et al., Reference Kotter-Grühn, Kornadt and Stephan2016), and this discrepancy increases as people grow older (Kornadt et al., Reference Kornadt, Hess, Voss and Rothermund2018). Similarly, individuals provide high ratings of their subjective health (Sperlich et al., Reference Sperlich, Tetzlaff and Geyer2019), and remain optimistic about their health despite normal age-related decline in physical abilities (Chipperfield, Reference Chipperfield1993). To feel younger and healthier, individuals must compare themselves to others, but it is unclear who these others may be. The current study examines which social comparisons older adults make spontaneously when they are asked to assess their subjective age and their health. In addition, we examine the effects of experimentally manipulated social comparisons on the assessment of subjective age and health.
Social comparison theory (Festinger, Reference Festinger1954) suggests that people have an innate drive to evaluate themselves, often in comparison to others. There are three types of social comparisons: downward, upward and lateral (Gerber, Reference Gerber, Zeigler-Hill and Shackelford2018). Downward comparisons involve looking down on someone who is worse off. Upward comparisons involve looking up to someone who is better off (Taylor et al., Reference Taylor, Neter and Wayment1995). Lateral comparisons involve a choice of individuals who are perceived as similar to the person who makes the comparison (Ben-Zur, Reference Ben-Zur2016; Gerber et al., Reference Gerber, Wheeler and Suls2018). It has been shown that downward comparisons contribute to positive self-perceptions in old age (Heckhausen and Brim, Reference Heckhausen and Brim1997), while lateral comparisons are important in making older adults realise that age-related change is normal (Ferring and Hoffmann, Reference Ferring and Hoffmann2007).
One way to study social comparison is through studies in which participants report to whom they compare themselves or provide assessments of themselves relative to others. A meta-analysis of 55 studies that included participants from a wide age range has shown that 46 per cent of the participants preferred to make an upward comparison, 36 per cent preferred a downward comparison and only 18 per cent preferred a lateral comparison (Gerber et al., Reference Gerber, Wheeler and Suls2018). This analysis did not focus on the effects of ageing on social comparisons, and the literature on older adults provides evidence for slightly different findings. For example, Cheng et al. (Reference Cheng, Fung and Chan2007) had younger (<60) and older adults (⩾60) assess whether statements about health described them as well as someone else of the same age. Older participants consistently perceived their own physical health as better than the health of others. The authors concluded that older adults maintain a positive view of their physical health through downward comparisons to others who are worse off. In another study, Ferring and Hoffmann (Reference Ferring and Hoffmann2007) asked 2,129 participants aged 50–90 to think of another person of their same age and to use a five-point Likert-scale to rate their own physical fitness, mental fitness and psychological resilience relative to that person. The results demonstrated that most participants used lateral comparisons, followed by upward comparisons, while downward comparisons were least frequent. The authors proposed that lateral comparisons helped older adults normalise the perceived effects of age. The discrepancy between the conclusion of the meta-analysis and the studies that focused specifically on older adults suggests that we do not know which social comparisons older adults make in their assessment of the effects of age.
Another way to study social comparisons is to examine participants’ reaction to different social comparisons. In such studies, the manipulation involves feedback that leads participants to compare themselves to others, and the reaction to feedback is the dependent variable (Gerber et al., Reference Gerber, Wheeler and Suls2018). These studies show that downward comparisons make older adults feel better. For example, Pinquart (Reference Pinquart2002) randomly assigned 100 participants aged 60–94 into two groups. In the experimental group, participants received negative information about old age (e.g. the elderly are a real nuisance), while in the control group, participants received neutral information (e.g. old people think about many things in a different way from young people). Participants who received negative information reported better self-perception following the manipulation relative to participants who received neutral information. Similarly, Frieswijk et al. (Reference Frieswijk, Buunk, Steverink and Slaets2004) exposed 455 participants aged 65–98 to a fictitious interview with a frail person (downward comparison) or to an interview with an independent senior-home resident (upward comparison). Exposure to a downward comparison led participants to feel more satisfied with their lives than did exposure to an upward comparison.
Only a few studies have examined the effect of social comparisons on subjective age. Stephan et al. (Reference Stephan, Chalabaev, Kotter-Grühn and Jaconelli2013) had adults aged 52–91 report how old they generally felt, and then measured their handgrip. Following the handgrip task, half of the participants were told that they performed better than most of their same-age peers, while the other half received no feedback. Participants who received positive feedback reported a younger subjective age following this procedure relative to their own report prior to the procedure, whereas participants who received no feedback showed no change. In another study, Shao et al. (Reference Shao, Xiao, Zhang and Xin2020) asked participants aged 60–84 to report their subjective age, perform a memory task and then report their subjective age again. Following the memory task, participants received feedback that their performance was better than that of same-age peers (positive feedback), received feedback that their performance was equivalent to that of their peers (neutral feedback) or received no feedback. Participants in the positive feedback group felt younger after receiving the feedback than before, whereas participants in the other two groups either showed no significant change in subjective age or felt older. These studies suggest that feedback about other individuals of the same age who are worse off has a positive effect on people's assessment of subjective age. However, the effects of a comparison to younger people remain unknown.
Social comparisons can also have a positive effect on self-rated health, although little experimental attention has been devoted to these effects. Spini et al. (Reference Spini, Clémence and Ghisletta2007) asked individuals aged 80–84 to rate their health. Participants were also asked to compare themselves to other people of the same age, and report whether their health was better, worse or the same. Those who selected ‘better’ provided higher ratings of their health over time. The authors argued that downward social comparisons help individuals maintain positive perceptions of their health. However, the sample included only very old participants, who may have demonstrated a greater effect due to their more immediate expectation of declining health. In addition, this study did not examine whether experimentally manipulated feedback affects self-rated health in older adults.
In light of the inconsistency in the literature with regard to the social comparisons that older adults make, and the lack of clarity about the impact of such comparisons on the perception of subjective age and health in the older population, we set out to conduct two studies that investigated these questions. In Study 1, we asked participants to report to whom they compared themselves when assessing their subjective age or health. In Study 2, we provided feedback that compared participants to younger people or to their peer group. We then examined whether the feedback affected the assessment of subjective age and health.
Study 1: Selection of a social comparison group
This study aimed to explore which spontaneous social comparisons older adults make when they are asked to assess their subjective age and their health. Lateral comparisons allow older adults to determine their self-esteem and to settle age-related changes (Ferring and Hoffmann, Reference Ferring and Hoffmann2007). Thus, older adults might compare themselves to their peer group when making spontaneous social comparisons. Nevertheless, because older people report younger subjective age relative to their chronological age (Kotter-Grühn et al., Reference Kotter-Grühn, Kornadt and Stephan2016) and because they evaluate their health as relatively good (Sperlich et al., Reference Sperlich, Tetzlaff and Geyer2019), it is possible that they would also compare themselves to younger people or to themselves when they were younger. Study 1 examines these possibilities.
Method
Participants
The sample included 146 Israeli participants (100 women, 46 men) between the ages of 60 and 89 (mean = 71.25, standard deviation (SD) = 6.06); their mean number of years of formal schooling was 16.37 (SD = 2.74). Recruitment used snowball sampling among community-dwelling volunteers. The study received approval from the Ethics Committee of The Open University of Israel.
Tools
Subjective age
Participants provided a number in years that reflected their subjective age, after reading the following sentence: ‘Many people feel older or younger than they actually are. What age do you feel most of the time?’ (e.g. Hughes and Lachman, Reference Hughes and Lachman2018). The participant's chronological age was subtracted from the reported age, and the result was divided by the participant's chronological age to allow for proportional discrepancy scores.
Self-rated health
Participants were asked to rate their health on a five-point Likert scale (1 = not good at all; 5 = very good).
Social comparison
Participants were asked to report to whom they compared themselves when they provided their assessment of subjective age and health. They could select one comparison group from four alternatives: (a) other people of the same age; (b) people 10 years younger than myself; (c) my younger self; and (d) people 10 years older than myself.
Assessment of expectations regarding ageing (ERA)
As subjective age assessment is assumed to incorporate expectations regarding ageing (Diehl et al., Reference Diehl, Wahl, Brothers and Miche2015), we also included an evaluation of these expectations. Participants were asked to report their expectations regarding ageing, using the ERA 12-item questionnaire of Sarkisian et al. (Reference Sarkisian, Steers, Hays and Mangione2005). Two independent translators translated the questionnaire into Hebrew, and any disagreements were resolved through discussion. The items in the questionnaire targeted physical health (e.g. ‘When people get older, they need to lower their expectations of how healthy they can be’), mental health (e.g. ‘I expect that as I get older, I will spend less time with friends and family’) and cognitive function (e.g. ‘I expect that as I get older I will become more forgetful’). Each statement appeared together with a four-point Likert scale (1 = strongly disagree, 4 = strongly agree). To compute the total score, we used the formulation of Sarkisian et al. (Reference Sarkisian, Steers, Hays and Mangione2005) that converted scores to a 0–100 range, with lower scores representing an expected decline in health and functional status, and higher scores representing better outcomes in older age. Cronbach's α coefficient in our sample was 0.846.
Procedure
All questionnaires were presented through Qualtrics (Provo, UT). Participants received an email with an invitation to complete an online survey. Within the survey, participants first provided demographic information (chronological age, gender, number of years of formal schooling). Next, participants assessed their subjective age and their health, and selected a comparison group that referred to the relevant subjective measure. Finally, participants filled in the ERA questionnaire. The entire survey lasted approximately 10 minutes.
Results and comment
We omitted five participants whose subjective age score exceeded three standard deviations from the mean score of the entire sample. Table 1 presents the distribution of comparison groups that participants selected after providing their assessment of subjective age and self-rated health.
Table 1. Distribution of comparison groups that participants selected, by type of assessment
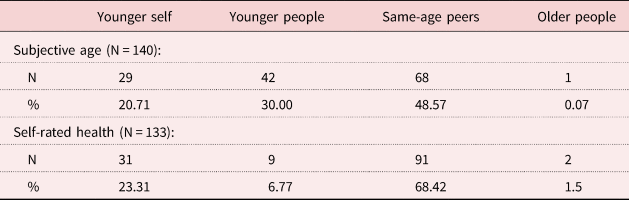
Note: The number of participants differs across comparisons because some participants were excluded due to outlier or failed to select a comparison group after one of the assessments.
Because the number of participants who compared themselves to people who were 10 years older than themselves was negligible, we excluded these respondents from all further analyses. We then combined participants who compared themselves to people who were 10 years younger and participants who compared themselves to their younger selves, as these two groups did not differ in any of the parameters reported below. Exclusion of participants based on subjective age ratings, comparison to older adults and failure to select a comparison group after one of the assessments left 131 participants in the sample. An exact McNemar test revealed a statistically significant difference in the selection of comparison groups (younger versus same age) while assessing subjective age or self-rated health (McNemar χ2 = 15.02, p < 0.001). Thus, more individuals compared themselves to younger people when they reported their subjective age relative to the proportion of people who did so when they rated their health.
Next, we examined whether participants who reported that they compared themselves to younger people differed from participants who reported that they compared themselves to people of their same age. A one-way analysis of covariance (ANCOVA) examined the difference between participants who selected younger comparison groups and participants who selected same age when assessing their subjective age, while controlling for gender and education. These analyses showed significant differences in subjective age, F(1, 135) = 21.10, p < 0.001, $\eta _p^2 = 0.135$ , in self-rated health, F(1, 130) = 8.19, p = 0.005, $\eta _p^2 = 0.059$
, in self-rated health, F(1, 130) = 8.19, p = 0.005, $\eta _p^2 = 0.059$ , and in ERA, F(1, 128) = 5.98, p = 0.016, $\eta _p^2 = 0.045$
, and in ERA, F(1, 128) = 5.98, p = 0.016, $\eta _p^2 = 0.045$ . In all cases, participants who reported that they compared themselves to younger people fared better than did participants who reported that they compared themselves to people of the same age (see Table 2). An equivalent ANCOVA that controlled for gender and education showed no differences between participants who selected younger comparison groups and participants who selected same age when assessing their self-rated health: subjective age, F(1, 127) = 2.19, p = 0.141, $\eta _p^2 = 0.017$
. In all cases, participants who reported that they compared themselves to younger people fared better than did participants who reported that they compared themselves to people of the same age (see Table 2). An equivalent ANCOVA that controlled for gender and education showed no differences between participants who selected younger comparison groups and participants who selected same age when assessing their self-rated health: subjective age, F(1, 127) = 2.19, p = 0.141, $\eta _p^2 = 0.017$ , self-rated health, F(1, 127) = 1.08, p = 0.308, $\eta _p^2 = 0.008$
, self-rated health, F(1, 127) = 1.08, p = 0.308, $\eta _p^2 = 0.008$ , and ERA, F(1,127) = 1.36, p = 0.245, $\eta _p^2 = 0.011$
, and ERA, F(1,127) = 1.36, p = 0.245, $\eta _p^2 = 0.011$ (see Table 2). That is, selection of a comparison group following health ratings was not related to participants’ perceptions.
(see Table 2). That is, selection of a comparison group following health ratings was not related to participants’ perceptions.
Table 2. Means and standard deviations (SD) of subjective age, self-rated health and expectations regarding ageing (ERA) scores in Study 1, by assessment and selected comparison group
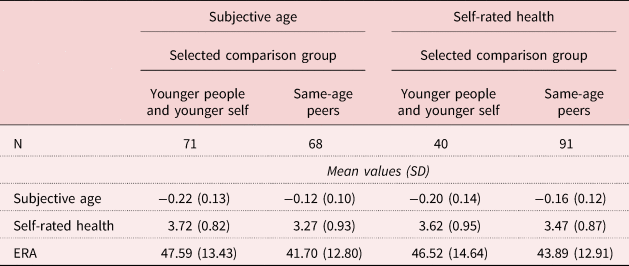
Note: Smaller (more negative) proportional subjective age scores indicate younger subjective age.
The results show that older adults compared themselves primarily to their peer group when assessing both their subjective age and their perceived health. In addition, more participants compared themselves to younger people when assessing their subjective age than when assessing their health. Participants who compared themselves to younger people when assessing their subjective age felt younger and healthier and had more positive expectations regarding ageing than participants who compared themselves to their own age group. In contrast, the selection of social comparison group had no effect when it referred to self-rated health.
Study 1 examined which social comparisons older adults make spontaneously when they assess their subjective age and their health, demonstrating that some older adults select a younger comparison group, and that such comparisons may have beneficial consequences. Study 2 further investigates these findings by examining reaction to experimentally defined comparisons.
Study 2: Reaction to social comparison
To examine reaction to social comparison feedback, we used a vocabulary test, and gave participants feedback about their performance on the test. We chose to use a vocabulary test because it has been shown that such a test has no effect on the assessment of subjective age, unlike other cognitive tests (e.g. Hughes et al., Reference Hughes, Geraci and De Forrest2013). Feedback conditions manipulated the age of the comparison group. Following feedback, participants assessed their subjective age (Study 2a) or their self-rated health (Study 2b).
Study 2a: Assessment of subjective age following social comparison feedback
The purpose of Study 2a was to examine whether social comparisons influence subjective age. Based on our findings in Study 1, we hypothesised that comparison to younger adults would lead participants to report a younger subjective age relative to comparison to same-age peers.
Method
Participants
The sample included 50 participants (25 women, 25 men) between the ages of 60 and 87 (mean = 70.28, SD = 7.30), who were born in Israel and were native Hebrew speakers; their mean number of years of formal schooling was 16.16 (SD = 3.76). Participants were randomly assigned to one of two experimental conditions (for full demographic details, see Table 3). Recruitment used snowball sampling among community-dwelling volunteers. There were no significant differences in age, t(48) = 0.77, p = 0.44, d = 0.21, or in education, t(48) = 0.74, p = 0.45, d = 0.21, between the two experimental conditions. The proportion of females was lower in the compare-to-young group relative to the compare-to-same age group, χ2(1, N = 50) = 6.48, p = 0.011. The study received approval from the Ethics Committee of The Open University of Israel.
Table 3. Sample characteristics in Studies 2a and 2b, by experimental condition
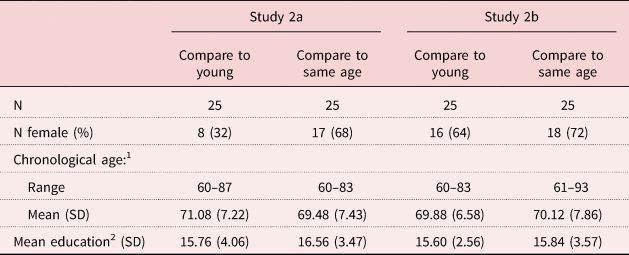
Notes: 1. Number of years. 2. Number of years of formal schooling. SD: standard deviation.
Experimental conditions
Participants received two types of feedback concerning their performance on the vocabulary test.
Compare to young
In this condition, the feedback compared participants to younger people, saying: ‘You completed the task successfully. Your performance was similar to the performance of young people.’
Compare to same age
In this condition, the feedback compared participants to people of the same age, saying: ‘You completed the task successfully. Your performance was similar to the performance of people your age.’
Measures
Vocabulary test
We used a 12-item multiple-choice vocabulary test (Kavé et al., Reference Kavé, Sapir-Yogev, Zamsh and Waintraub2022), in which each item includes a target word and four alternative responses of either one word or a short phrase. Participants were asked to mark the correct interpretation by clicking on it. A preliminary study that included 50 native Hebrew speakers (mean = 68.59, SD = 7.58, range 60–83) showed that participants who completed the vocabulary test were similar to those who did not complete the vocabulary test in subjective age, t(48) = 1.12, p = 0.26, d = 0.32, and in self-rated health, t(41) = 1.16, p = 0.25, d = 0.35. Thus, the test itself had no effect on these measures.
Subjective age
Participants provided a number in years that reflected their subjective age, after reading the following sentence: ‘Many people feel older or younger than they actually are. What age do you feel most of the time?’ (e.g. Hughes and Lachman, Reference Hughes and Lachman2018). The participant's chronological age was subtracted from the reported age, and the result was divided by the participant's chronological age to allow for proportional discrepancy scores.
Procedure
Participants received an email with an invitation to complete an online survey. Within the survey, they first provided demographic information (e.g. chronological age, gender, number of years of formal schooling), and then they completed the vocabulary test. After the test, they received feedback on their performance and then assessed their subjective age.
Results and comment
We omitted one participant whose subjective age score exceeded three standard deviations from the mean score of the entire sample. Table 4 shows success rate on the vocabulary test.
Table 4. Means and standard deviations (SD) of subjective age, self-rated health and vocabulary success rate, by study and experimental condition
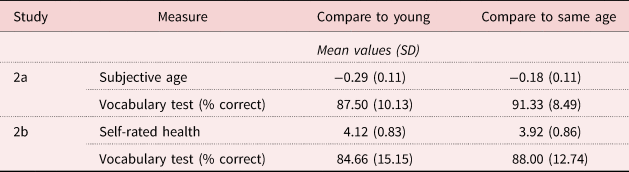
Note: Smaller (more negative) proportional subjective age scores indicate younger subjective age.
Participants on the two feedback conditions did not differ in their performance on the vocabulary test, t(47) = 1.43, p = 0.15, d = 0.41. Participants who received feedback that compared them to younger people assessed their subjective age as younger than did participants who received feedback that compared them to people of the same age, F(1, 47) = 10.33, p = 0.002, $\eta _p^2$ = 0.18. An ANCOVA that controlled for gender, years of schooling and actual performance revealed the same group difference in subjective age, F(1, 44) = 6.45, p = 0.015, $\eta _p^2$
= 0.18. An ANCOVA that controlled for gender, years of schooling and actual performance revealed the same group difference in subjective age, F(1, 44) = 6.45, p = 0.015, $\eta _p^2$ = 0.128.
= 0.128.
The results suggest that participants who received feedback that compared their performance to the performance of younger adults reported younger subjective age than did participants who received feedback that compared their performance to that of their same-age peers. Thus, individuals who were led to compare themselves to younger people felt younger than those who were led to compare themselves to older people.
Study 2b: Assessment of self-rated health following social comparison feedback
The purpose of Study 2b was to examine whether social comparisons influence self-rated health. Based on the findings of Study 1, we hypothesised that the type of social comparison would not affect self-rated health as it affected subjective age.
Method
Participants
The sample included 50 participants (34 women, 16 men) between the ages of 60 and 93 (mean = 70.00, SD = 7.18) who were born in Israel and were native Hebrew speakers; their mean number of years of formal schooling was 15.72 (SD = 7.17). Recruitment to Study 2b used the same procedure as in Study 2a, and randomisation of condition assignment took place for the two studies together (for full demographic details, see Table 3). There were no significant differences between the two conditions of Study 2b in age, t(48) = 0.11, p = 0.90, d = 0.03, education, t(48) = 0.27, p = 0.78, d = 0.07, or gender distribution, χ2(1, N = 50) = 0.368, p = 0.544. In addition, there were no significant differences in either age, t(98) = 0.19, p = 0.84, d = 0.03, education, t(98) = 0.63, p = 0.52, d = 0.12, or gender distribution, χ2(1, N = 100) = 3.38, p = 0.067, between individuals who participated in Study 2a and those who participated in Study 2b. The study received approval from the Ethics Committee of The Open University of Israel.
Procedure
The procedure was identical to that of Study 2a, except that participants were asked to assess their health instead of their subjective age. We used the same self-rated health item that appeared in Study 1, and feedback compared participants to younger people or to same-age peers as in Study 2a.
Results and comment
Participants on the two feedback conditions did not differ in their performance on the vocabulary test, t(48) = 0.84, p = 0.40, d = 0.23 (see Table 4). There was no difference in self-rated health between the two feedback groups, F(1, 48) = 0.69, p = 0.40, $\eta _p^2$ = 0.01, and controlling for gender, years of schooling and actual performance in an ANCOVA did not change this result, F(1, 45) = 1.17, p = 0.284, $\eta _p^2$
= 0.01, and controlling for gender, years of schooling and actual performance in an ANCOVA did not change this result, F(1, 45) = 1.17, p = 0.284, $\eta _p^2$ = 0.025.
= 0.025.
The results of Study 2b strengthen the findings of Study 1 in showing that social comparisons do not affect participants’ assessment of their health.
General discussion
We conducted two experiments in which participants over the age of 60 were asked to report to whom they compared themselves when they assessed their subjective age or their health, and received feedback that made them compare themselves to either younger people or to their same-age peers.
Study 1 shows that the distribution of comparison groups is different for the assessment of subjective age and for the assessment of self-rated health, so that more individuals compare themselves to younger people when they report their subjective age relative to the proportion of people who do so when they rate their health. However, for both types of assessments, participants compared themselves to their peer group more often than they compared themselves to any other group. These findings strengthen the argument that social comparisons in older age serve the need for accurate self-assessment as well as the need for normalising age-related changes (Ferring and Hoffmann, Reference Ferring and Hoffmann2007). Thus, comparing oneself to others of the same age may reflect a lateral or a downward comparison, whose main motive is to feel better. Indeed, older adults felt generally younger than their chronological age and rather healthy, even when comparing themselves to their peers.
Yet, comparison to same-age peers could serve more than one function. A lateral comparison involves a comparison to others who are perceived as similar in the examined ability (Gerber et al., Reference Gerber, Wheeler and Suls2018). In this sense, selecting same-age peers as a comparison group means that participants conduct a lateral comparison. Since this lateral comparison resulted in younger subjective age relative to chronological age, we believe that the comparison to one's peer group is actually a downward comparison. The purpose of this comparison is to distance oneself from the negative perception of old age. This argument is in line with earlier research that demonstrated that older adults who were exposed to negative stereotypes about ageing reported a younger subjective age compared to those who were not exposed to negative stereotypes (e.g. Kotter-Grühn and Hess, Reference Kotter-Grühn and Hess2012; Weiss and Lang, Reference Weiss and Lang2012).
Study 1 further suggests that some participants compared themselves to younger age groups. When assessing subjective age, participants who compared themselves to younger people reported a younger subjective age, better self-rated health and more positive expectations of ageing than those who compared themselves to their peers. This comparison may represent an upward comparison or a lateral comparison. Upward comparisons involve looking up to someone who is better off (Taylor et al., Reference Taylor, Neter and Wayment1995). A comparison to younger people, who are perceived as better than older adults in various aspects, may thus reflect an upward comparison. However, it is also possible that those who feel younger select a younger comparison group because they feel that they belong in that group, thus making a lateral comparison.
Furthermore, it is possible that some participants compared themselves to younger people due to their self-ageism. That is, participants who fear the implications of growing old, such as the loss of good health, independence, usefulness and, ultimately, life (Sargent-Cox, Reference Sargent-Cox2017), may wish to distance themselves from older adults even when they are old themselves. Although ageism may refer to how others view older adults, it is also relevant to how older adults feel about their own group (Bodner et al., Reference Bodner, Cohen-Fridel and Yaretzky2011). In fact, research suggests that older people internalise the attitudes that prevail in society concerning old age (Ayalon and Tesch-Römer, Reference Ayalon and Tesch-Römer2018), and that ageist attitudes affect subjective age ratings (Bodner et al., Reference Bodner, Shrira, Hoffman and Bergman2021). Unfortunately, we did not ask our participants explicitly whether they were attempting to distance themselves from negative stereotypes of ageing. It remains to be seen whether such explicit distancing mediates the effects of social comparisons on subjective age.
Study 2 demonstrates that participants who received feedback that compared their performance to the performance of younger people reported younger subjective age than did participants who received feedback that compared their performance to their peers. Previous reaction studies have pointed out two main patterns: assimilation and contrast (Gerber, Reference Gerber, Zeigler-Hill and Shackelford2018). Assimilation occurs when the comparison makes people feel closer to the target of comparison, whereas a contrast occurs when people shift away from the target (Wheeler and Suls, Reference Wheeler and Suls2007). According to Collins (Reference Collins1996), an upward comparison could lead to either of these two main patterns, depending on whether the comparison is construed as indicating similarity to the comparison target or difference from this target. Since people may expect some similarity to any comparison target who is within their own range of ability, a certain degree of assimilation will occur in almost all cases. The effect of contrast is generally stronger than the effect of assimilation, and thus it often masks the effect of assimilation. In some contexts, the expectation of similarity becomes stronger, thus leading to a stronger assimilation effect (Collins, Reference Collins1996). We propose that receiving feedback that compares the performance of older adults to the performance of younger adults made participants embrace group similarities. Thus, participants might have viewed themselves as part of a younger age group, and consequently reported younger subjective age. This argument fits well with the conclusion of Gerber et al. (Reference Gerber, Wheeler and Suls2018) that in instances of assimilation, the comparer's self-evaluation moves towards the comparison target.
Both Studies 1 and 2 suggest that social comparison is differentially related to the assessment of subjective age and to the report of self-rated health. In Study 1, participants who assessed their health and compared themselves to younger people and those who compared themselves to their peers did not differ in subjective age, self-rated health and expectations regarding ageing. In Study 2, participants who received feedback that compared them to either younger or older adults did not differ in their assessment of their health. There could be several explanations for these findings. First, previous studies have shown that individuals provide high ratings of subjective health (Sperlich et al., Reference Sperlich, Tetzlaff and Geyer2019), and remain optimistic about their health despite normal age-related decline in physical abilities (Chipperfield, Reference Chipperfield1993). Indeed, our participants reported good self-rated health (approximately 4 on a 1–5 scale). This ceiling effect in self-rated health could have affected our analyses. Second, while subjective age may be subject to a range of situations and daily changes (Geraci et al., Reference Geraci, De Forrest, Hughes, Saenz and Tirso2018; Bellingtier and Neupert, Reference Bellingtier and Neupert2020; Bodner et al., Reference Bodner, Shrira, Hoffman and Bergman2021), longitudinal studies usually report that self-rated health is rather stable over time (Spini et al., Reference Spini, Clémence and Ghisletta2007). Thus, it is possible that individuals have a stable perception of their health that cannot be easily manipulated experimentally. Third, subjective age is always examined against chronological age, which is an objective measure. In contrast, the self-rated health measure that we used was not calculated relative to any other objective health measure. It is possible that a health measure that would be calculated more similarly to the calculation of the subjective age measure would lead to different results.
In conclusion, the current findings may help explain why older adults feel younger and healthier than they actually are. We propose that they do so because they select social comparisons that help them protect their self-image from the negative perceptions of ageing. Future research should examine whether these conclusions are also relevant for the many dimensions of the subjective age construct (as defined by Kastenbaum et al., Reference Kastenbaum, Derbin, Sabatini and Artt1972), and whether social comparisons can be helpful in interventions that attempt to affect older adults’ general feelings towards their age.
Data
Data will be made available to other researchers upon request from the corresponding author.
Acknowledgement
The study was not preregistered.
Financial support
This work was supported by the Open University of Israel.
Conflict of interest
The authors declare no conflicts of interest.





 Open access
Open access