



Background
Epidemiological studies suggest that up to 5% of the population will experience an eating disorder over the course of their lives.Reference Treasure, Claudino and Zucker1 Eating disorders are often accompanied by complex physical and psychiatric comorbidity, and have high mortality rates.Reference Treasure, Claudino and Zucker1 Despite their severity, only a small proportion of individuals with eating disorders seek and obtain help,Reference Solmi, Hatch, Hotopf, Treasure and Micali2 medical students still receive minimal training on these conditionsReference Ayton and Ibrahim3 and research funding for eating disorders remains limited.4 Despite being a cardinal element of successful public health campaigns, compared with other disorders mental health literacy around eating disorders has received little attention.Reference Bullivant, Rhydderch, Griffiths, Mitchison and Mond5 Therefore, it is possible that stigma towards eating disorders arising from low levels of mental health literacy around these conditions could account for low levels of help-seekingReference Griffiths, Mond, Murray and Touyz6 as well as the above-mentioned limited research investment and visibility in medical curricula.
Compared with other mental illnesses, studies show that eating disorders are more commonly viewed as less severe, self-inflicted and under an individual's control.Reference Mond, Robertson-Smith and Vetere7,Reference Ebneter and Latner8 Crucially, studies have shown these beliefs are held by professionalsReference McNicholas, O'Connor, O'Hara and McNamara9 as well as the public. To date, only a limited number of studies have investigated stigmatising attitudes towards people with eating disorders. To the best of our knowledge, all existing studies have used convenience samples, which are likely to be unrepresentative of the general population. In the UK, the Office of National Statistics (ONS) has collected data on stigmatising views held by the public towards seven different mental health conditions in 1998, 2003 and 2008, as part of the Royal College of Psychiatrists’ campaign ‘Changing Minds: Every family in the land’, aimed at reducing stigma towards mental illness. Two previous studies have described findings from the 1998 and 2003 surveys;Reference Crisp, Gelder, Goddard and Meltzer10,Reference Crisp, Gelder, Rix, Meltzer and Rowlands11 however, no studies have investigated changes in stigmatising beliefs towards eating disorders over time using the most recent data available (i.e. 2008), or their association with sociodemographic characteristics of respondents controlling for potential confounders in order to identify specific predictors of stigmatising beliefs.
Aims
Researching the associations of stigmatising beliefs and sociodemographic characteristics may provide evidence of which groups in society to target, given limited resources. The aim of this study was thus to use data from the first and last ONS surveys to investigate whether attitudes towards individuals with eating disorders have changed over time, how these compared with other mental health conditions, and whether stigmatising attitudes are associated with specific sociodemographic characteristics, including gender, ethnicity, age and socioeconomic status. Based on findings from the 2003 survey, we hypothesised that men and those from more deprived socioeconomic positions would endorse more stigmatising beliefs and that the latter would have remained relatively stable over time.Reference Crisp, Gelder, Goddard and Meltzer10
Method
Participants
We used data from the July 1998 and July 2008 ONS Omnibus Opinion Surveys. The sampling frame for these surveys were UK postal sectors stratified by region and by: proportion of households renting from local authorities, and the proportion in which the head of household was in socioeconomic groups 1–5 or 13. Thirty households were randomly selected in each postal code and, for each household, one adult aged 16 years or over was chosen at random. Participants answered questions on sociodemographic factors by questionnaire, and interviewers asked questions on stigma and mental health aided by the use of flashcards.
Measures of stigma
The survey asked about participants’ views on eight topics that a previous reviewReference Hayward and Bright12 had identified as representing core stigmatising beliefs around people with mental illnesses. These were: being dangerous; being unpredictable; being difficult to talk with; having only themselves to blame; being able to pull themselves together; having a poor outcome and responding poorly to treatment. Existing research suggests that these questions have a three-factor structure, consisting of: negative stereotypes, patient blame and perceived inability to recover.Reference Wood, Birtel, Alsawy, Pyle and Morrison13
For the purpose of this study, we concentrated on the latter two: patient blame (comprising the statements that people with mental illnesses ‘only have themselves to blame’ and ‘could pull themselves together if they wanted to’), and inability to recover (comprising the statements that people with mental illnesses ‘will never recover fully’; and ‘will not improve if given treatment’). We chose not to focus on negative stereotypes (i.e. beliefs that people with mental illness are ‘dangerous to others’ and ‘unpredictable’) as it was previously shown that a much smaller proportion of respondents endorsed these beliefs with regards to eating disorders compared with other conditions under study.Reference Crisp, Gelder, Goddard and Meltzer10 Each statement was scored on a five-point scale ranging from ‘completely disagree’ to ‘completely agree’.
For all questions, greater scores indicate greater agreement with the statement, for example, placing greater blame on the person or believing that individuals with a given condition have lower ability to improve. We interpreted high scores on questions about blame as representing more stigmatising beliefs around individuals’ responsibility for their illness. Questions on ability to recover are thought to tap into respondents’ mental health literacy surrounding treatment and also beliefs around severity and chronicity of these conditions. Literature suggests that people with mental health conditions that are perceived as chronic and with poorer prognosis are more likely to be stigmatised and socially rejected.Reference Hayward and Bright12 Therefore, high scores on these questions could identify this type of stigmatising attitudes. However, we also hypothesised that low scores on these questions could index a different type of stigma, for instance, if a certain condition is seen as easier to recover from because it is not considered to be as severe as others. This type of belief might be particularly relevant for conditions that are typically considered as self-inflicted.
In order to understand the nature of, as well as trends in, stigmatising beliefs towards eating disorders, we compared scores of questions relating to individuals with eating disorders with those relating to individuals with depression and alcohol dependence as, based on previous findings, these disorders appeared more comparable with eating disorders than schizophrenia and dementia.Reference Crisp, Gelder, Goddard and Meltzer10,Reference Crisp, Gelder, Rix, Meltzer and Rowlands11
Sociodemographic characteristics
We investigated the following sociodemographic characteristics as potential predictors of stigmatising views: a continuous indicator of participants’ age; gender (male/female), education level (compulsory, i.e. age 16 years/ non-compulsory); social class (manual/non-manual); housing tenure (owning versus renting a house); and ethnicity (White British/ Black, Asian and other minority ethnic groups).
Data analysis
We described participants' characteristics using means (with standard deviations) and frequencies (with proportions). To describe cross-sectional differences across psychiatric conditions by stigma domain, we used mean scores (with 95% confidence intervals) across stigma domains by psychiatric condition (i.e. eating disorders, depression, alcohol dependence) and calendar year (1998, 2008).
To investigate sociodemographic factors associated with stigma, for each stigma domain we first ran univariable linear regressions, modelling the outcomes (individual stigma domains) as a function of each individual sociodemographic factor. To test for changes in stigma scores between 1998 and 2008, we further included the variable ‘year’. We present univariable models in the supplementary material for completeness. In our main analyses, we entered all sociodemographic factors simultaneously in a multivariable model, with stigma domains as the outcome. We did not limit the number of variables in the multivariable model to those with low P-values in the univariable model for two reasons. First, if one uses only variables with a P-value below a predefined threshold there is a risk of excluding variables that are negatively confounded by other variables subsequently included in the model. Second, we wanted our models to be comparable across conditions. Analyses were based on participants with complete cases and conducted in Stata 15.
Results
Participants
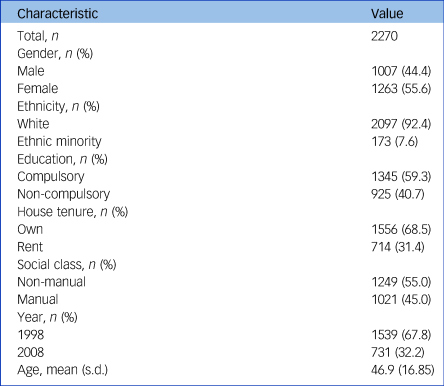
A total of 2854 individuals took part in the surveys in 1998 and 2008 and, of these, 2270 (79.5%) had complete data on all the variables included. We provide a flow chart of study participation in Fig. 1. The majority of the participants were female and of White ethnicity; had only completed compulsory education; had a non-manual occupation; and owned their house (Table 1). The mean age of the sample was 46.9 years (s.d. = 16.9). Participants who were older, were from a minority ethnic background, had a non-manual occupation and had only completed compulsory education were more likely to have some missing data (Supplementary Table 1 available at https://doi.org/10.1192/bjp.2021.175). Individuals who took part in the 2008 survey were also more likely to have missing data.
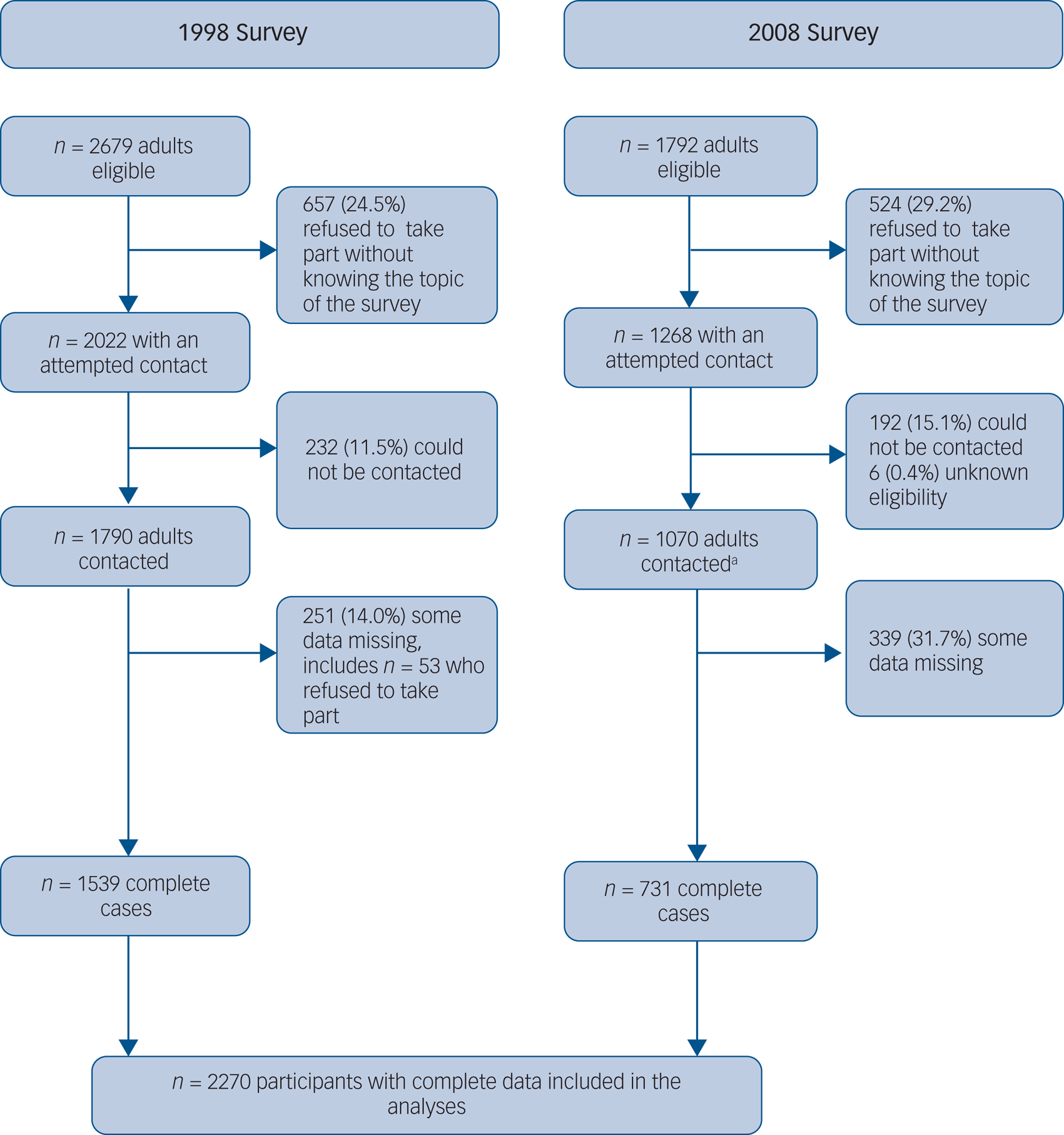
Fig. 1 Flow chart of study participation.
a. Actual data-set included 1064 participants.
Table 1 Sociodemographic characteristics of the participants
Trends and predictors of stigmatising beliefs around recovery
In both 1998 and 2008, mean scores for questions relating to whether participants thought that individuals ‘would not improve if given treatment’ and ‘will never recover fully’ were lower for eating disorders than severe depression or alcohol dependence (Fig. 2 & Supplementary Table 2):
(a) eating disorders: ‘improvement’ question 1998 mean 1.99 (95% CI 1.94–2.06), 2008 mean 2.10 (95% CI 2.02–2.18); ‘recovery’ question 1998 mean 2.26 (95% CI 2.20–2.31), 2008 mean 2.46 (95% CI 2.38–2.54);
(b) severe depression: ‘improvement’ question 1998 mean 2.25 (95% CI 2.19–2.31), 2008 mean 2.33 (95% CI 2.24–2.42); ‘recovery’ question 1998 mean 2.78 (95% CI 2.72–2.84), 2008 mean 2.92 (95% CI 2.84–3.00);
(c) alcohol dependence: ‘improvement’ question 1998 mean 2.16 (95% CI 2.11–2.23), 2008 mean 2.34 (95% CI 2.25–2.43); ‘recovery’ question 1998 mean 2.81 (95% CI 2.76–2.88), 2008 mean 2.92 (95% CI 2.82–3.02).
This suggests that responders believed recovering from eating disorders is easier than recovering from the other conditions. For all three conditions stigmatising beliefs decreased in 2008 compared with 1998 (Fig. 2).
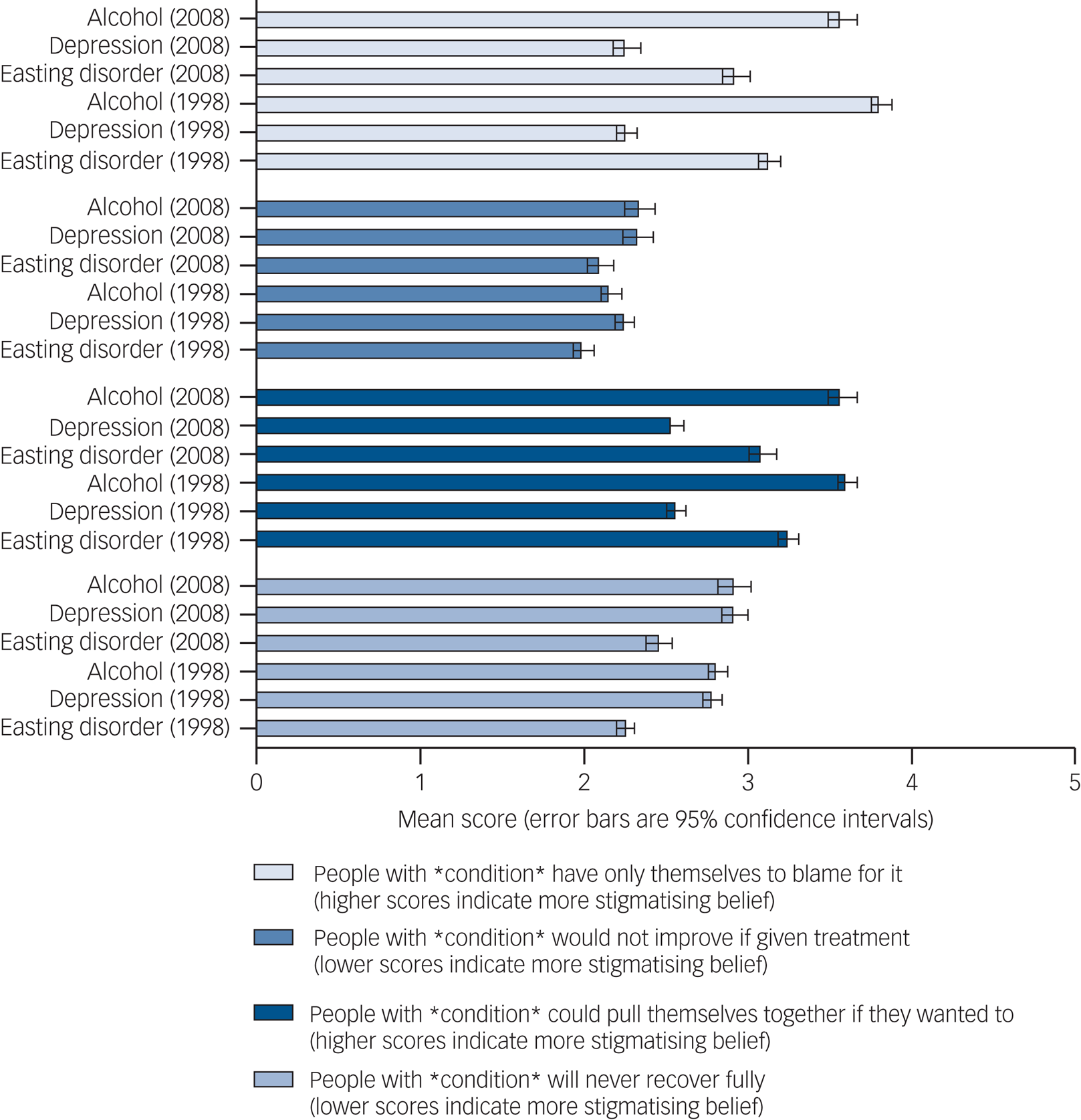
Fig. 2 Mean item score (with 95% confidence interval) by survey year and psychiatric condition (n = 2270).
With respect to predictors of these beliefs, we present results of univariable models in Supplementary Table 3 and the main multivariable model in Table 2.
Compared with women, men were more likely to think that people with eating disorders could recover fully (mean difference: −0.18, 95% CI −0.28 to −0.08) and improve with treatment (mean difference: −0.08, 95% CI −0.18 to 0.01) although for the latter association evidence was weaker. We observed a similar pattern for alcohol dependence (not improve with treatment mean difference: −0.11, 95% CI −0.21 to −0.01; not recover fully mean difference: −0.10, 95% CI −0.22 to −0.01), but not depression, for which there was no difference between males and females’ beliefs.
Older participants believed that recovery was unlikely across all three mental illnesses. Compared with participants with only compulsory education, those with non-compulsory education more frequently thought that those with depression (mean difference: −0.23, 95% CI −0.35 to −0.11) and alcohol dependence (mean difference: −0.12, 95% CI −0.24 to −0.01), but not those with eating disorders (mean difference: −0.07, 95% CI −0.17 to 0.04) could recover if given treatment. Participants who rented their accommodation more commonly believed that those with eating disorders could not improve if given treatment (mean difference: 0.14, 95% CI 0.03–0.24). The same belief was shared among those with non-manual compared with manual occupations for all three conditions, although evidence was weaker for alcohol dependence. There were no differences in these beliefs by ethnicity.
Trends and predictors of stigmatising beliefs around blame
In both 1998 and 2008, when participants were asked whether they believed that individuals ‘have only themselves to blame for their condition’ and ‘could pull themselves together if they wanted’, they scored eating disorders higher than depression, but lower than alcohol dependence (Fig. 2 and Supplementary Table 2):
(a) eating disorders: ‘blame’ question 1998 mean 3.13 (95% CI 3.07–3.20), 2008 mean 2.93 (95% CI 2.85–3.02); ‘pull together’ question 1998 mean 3.25 (95% CI 3.19–3.31), 2008 mean 3.09 (95% CI 3.01–3.17);
(b) depression: ‘blame’ question 1998 mean 2.26 (95% CI 2.20–2.32), 2008 mean 2.26 (95% CI 2.18– 2.35), ‘pull together’ question 1998 mean 2.56 (95% CI 2.51–2.62), 2008 mean 2.53 (95% CI 2.45– 2.61);
(c) alcohol dependence: ‘blame’ question 1998 mean 3.81 (95% CI 3.76–3.88), 2008 mean 3.57 (95% CI 3.49–3.67), ‘pull together’ question 1998 mean 3.60 (95% CI 3.55–3.67), 2008 mean 3.54 (95% CI 3.46–3.63).
This indicates that respondents believed that people with eating disorders are more to blame for their condition than those with depression, but less than those with alcohol dependence. However, as shown in Fig. 2 (and Supplementary Table 2), compared with 1998, in 2008 stigmatising views towards eating disorders and alcohol dependence improved in these domains. By contrast, for severe depression scores remained similar.
Table 2 shows factors associated with stigmatising views around blame. Compared with women, men expressed more agreement with the idea that people with eating disorders are to blame for their condition (mean difference: 0.24, 95% CI 0.13–0.35), with a comparable association observed for depression (mean difference: 0.25, 95% CI 0.15–0.35). Men were also more likely than women to think that people with all three mental illnesses could ‘pull themselves together’ if they wanted to, with the greatest difference observed when referring to people with eating disorders (mean difference: 0.37, 95% CI 0.27–0.47), compared with depression (mean difference: 0.24, 95% CI 0.14–0.34) and alcohol dependence (mean difference: 0.20, 95% CI 0.10–0.31). Older participants believed that people with eating disorders (but not those with depression or alcohol dependence) were to blame for their disorder (mean difference 0.09, 95% CI 0.03–0.17). Older participants also though that people with an eating disorder (mean difference: −0.07, 95% CI −0.13 to −0.01) and those with alcohol dependence (mean difference: −0.12, 95% CI −0.18 to −0.06) could not ‘pull themselves together’ they wanted to.
Table 2 Multivariable linear regression models for the associations between sociodemographic characteristics and stigmatising beliefs, by condition (eating disorders, depression, alcohol dependence)a
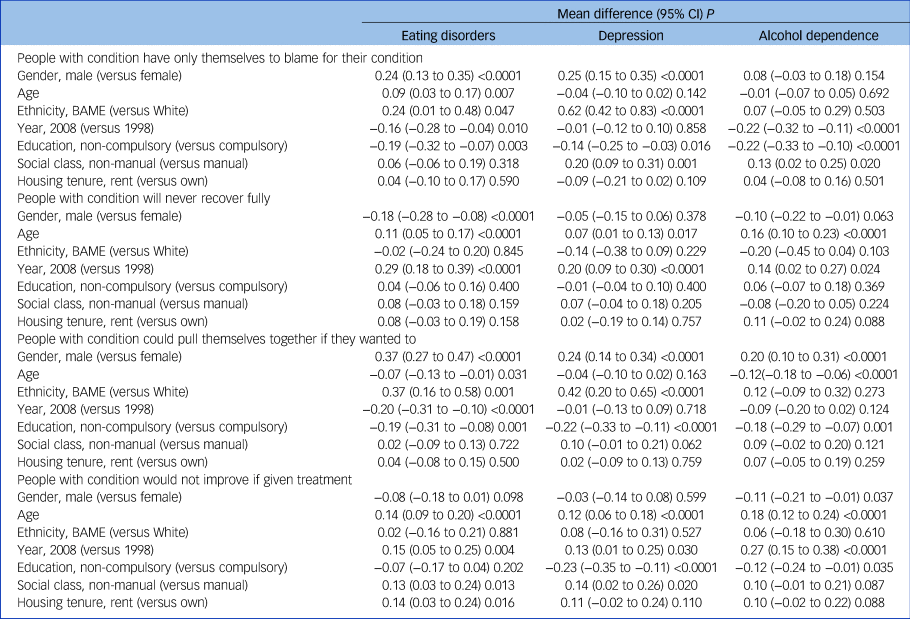
BAME, Black, Asian, Minority ethnic.
a. Complete case analyses, n = 2270.
Participants from minority ethnic backgrounds, compared with White participants, were more likely to think that those with eating disorders (mean difference: 0.24, 95% CI 0.01–0.48) and depression (mean difference: 0.62, 95% CI 0.42–0.83) were to blame for their conditions and that they could ‘pull themselves together’ if they wanted to (eating disorders mean difference: 0.37, 95% CI 0.16–0.58, depression mean difference: 0.42, 95% CI 0.20–0.65). Compared with those with only compulsory levels of education, participants with higher levels of education were less likely to blame individuals for their mental illness (eating disorders mean difference: −0.19, 95% CI −0.32 to −0.07; depression mean difference:−0.14, 95% CI −0.25 to −0.03; alcohol dependence mean difference: −0.22, 95% CI −0.33 to −0.10) or think that they could ‘pull themselves together’ if they wanted to (eating disorders mean difference: −0.19, 95% CI −0.31 to −0.08; depression mean score: −0.22, 95% CI −0.33 to −0.11; alcohol dependence mean difference: −0.18, 95% CI −0.29 to −0.07).
Discussion
Main findings and comparison with the existing literature
In this study we investigated patterns of stigmatising beliefs towards people with eating disorders, depression and alcohol dependence, how these have changed over 10 years (1998–2008), and how they are associated with sociodemographic factors.
In both 1998 and 2008, respondents thought that people with eating disorders were to be blamed for their conditions more than people with depression, but not more than those with alcohol dependence. Participants also believed that it would be easier to recover from an eating disorder or improve if given treatment, than it would be to recover from either depression or alcohol dependence. These results possibly reflect the widespread belief that eating disorders are under one's control and could be easily recovered from, as previously reported.Reference Mond, Robertson-Smith and Vetere7,Reference Ebneter and Latner8
However, we also found that, over the 10-year period studied (1998–2008), these stigmatising views towards eating disorders decreased across the board, which was contrary to our hypothesis. This had not been the case when the 1998 results were compared with the results of the 2003 survey (as these only reported improvement on the two ‘recovery’ questions)Reference Crisp, Gelder, Goddard and Meltzer10 and was not observed to the same extent for the other two comparator conditions. This trend is encouraging and is in line with global literature showing improvements in stigma towards mental health diagnoses. Nevertheless, to date this research has primarily focused on depression and schizophrenia and largely overlooked eating disorders, hence comparisons of our findings with those of other countries is difficult.Reference Angermeyer, Matschinger and Schomerus14
Finally, we observed that stigmatising views towards people with eating disorders were more common among certain groups, which was broadly in line with our hypothesis. Males, participants who were older or from minority ethnic backgrounds, and those with lower levels of formal education were more likely to attribute blame to people with eating disorders; this pattern was also observed across the other conditions. Older participants were more likely to think that people with eating disorders, as well as other conditions, will never recover fully even if given treatment. On the other hand, compared with women, men were more likely to believe that it was possible to recover from eating disorders and alcohol dependence, but their views did not differ from those of women when considering depression. Previous studies using 1998 and 2003 ONS data found largely similar patterns, although these did not disaggregate between different stigma domains and did not mutually control for sociodemographic factors.Reference Crisp, Gelder, Goddard and Meltzer10,Reference Crisp, Gelder, Rix, Meltzer and Rowlands11 Our study therefore offers a more granular understanding of the relationship between different sociodemographic characteristics and specific stigma domains.
Strengths, limitations and direction for future research
This study has a number of strengths. We used nationally representative general population data spanning a decade, thus avoiding selection biases associated with the use of convenience samples (for example college students). We compared eating disorders with two conditions that are often comorbid with eating disorders and share similar epidemiological profiles (depression) and that we hypothesise would have similar stigma profiles (alcohol dependence), as opposed to disorders that have different stigma and epidemiological profiles, for example dementia or schizophrenia.Reference Hudson, Hiripi, Pope and Kessler15 We measured our outcomes using continuous scores rather than dichotomising answers, allowing us to investigate our outcomes on a continuum of severity while also achieving good statistical power. Finally, this was the first study to investigate sociodemographic characteristics associated with individual stigma domains and using regression models to control for confounding, thus ensuring robustness of findings.
Despite these strengths, a number of limitations should also be acknowledged. One limitation, as with all large population-level surveys, is that there was some selective attrition that became more prominent in the most recent survey. Although we included predictors of attrition in our analyses, we cannot exclude the possibility that selection bias could have occurred if survey participation was conditional upon certain sociodemographic characteristics, for instance female gender or White ethnicity both of which appear to be over-represented compared with 2011 ONS census figures.16 We did not adjust regression models for multiple comparisons as, given some groups were small (for example ethnic minority participants), attempting to avoid a false positive would have increased the risk of false negatives. Instead, we interpreted the strength of the evidence based on effect size and 95% confidence intervals, and the majority of the associations observed had very small P-values, which suggests there was strong statistical evidence to support a difference.
The survey asked about ‘eating disorders’ without differentiating between bulimia nervosa, anorexia nervosa or binge eating disorder. As there is some evidence that these conditions may have different stigma profiles,Reference Griffiths, Mond, Murray and Touyz6,Reference Ebneter and Latner8 future studies should aim to include questions on individual eating disorders. The survey also asked about ‘severe depression’ as opposed to ‘depression’ but did not include any indications of severity for any of the other conditions, which may have biased participants’ responses if individuals, or specific sociodemographic groups, perceived this condition as being more severe than the others. The questions around ability to recover did not directly ask about respondents’ beliefs around severity of each condition under study and could have measured knowledge around availability of effective treatment options. The lower scores we observe on these questions could have therefore indexed better mental health literacy and fewer stigmatising beliefs. However, we propose that the latter is unlikely as we do observe marked differences between depression and eating disorders, for instance, despite the fact that evidence around effective treatments for eating disorders is weaker than that around effective treatments for depression. Hence, we believe these questions are likely to capture underlying beliefs around severity. Nevertheless, future surveys and studies should include more explicit questions around severity in order to tease apart these two important domains. They should also include questions on participants’ weight to explore how the latter might influence people's views on eating disorders.
Although few have addressed eating disorders specifically, in recent years there have been more public health campaigns to increase mental health literacy and decrease stigma,Reference Bullivant, Rhydderch, Griffiths, Mitchison and Mond5 also helped by public figures talking more openly about their mental health. Although some of the improvement in stigmatising beliefs that we observed could have been because of specific campaigns, our design could not test this, as participants were not asked whether they had been exposed to any specific campaign and, despite covering a 10-year time frame, the data is no longer current. It is therefore important that such surveys continue to be repeated and that evaluation of the effectiveness of anti-stigma and mental health literacy campaigns is embedded in their design in order to understand the impact of anti-stigma and awareness-raising campaigns on trends in mental health stigma. Finally, our results are specific to the UK and might not be generalisable to other countries. It is therefore important that data on mental health stigma is more widely collected so that cross-country comparisons can be conducted.
Implications of our findings
The finding that males and ethnic minority participants held more stigmatising views towards people with eating disorders has important clinical and research implications. Eating disorders are often framed in the media as White women illnesses. Men who experience these conditions are portrayed as ‘atypical’ and ‘less of a man’.Reference MacLean, Sweeting, Walker, Patterson, Räisänen and Hunt17 These negative views could be responsible for the greater levels of stigmatising beliefs we observed in our study and greater internalised stigma seen in males with eating disorders compared with females, which have been reported by previous studies.Reference Griffiths, Mond, Murray and Touyz6 However, we found that males had more stigmatising views towards depression and alcohol dependence as well, and this has also been previously observed.Reference Oliffe, Ogrodniczuk, Gordon, Creighton, Kelly and Black18 Feelings of shame around experiences of mental illness in males have been shown to hinder help-seeking behavioursReference Griffiths, Mond, Li, Gunatilake, Murray and Sheffield19 and are thought to be one of the reasons behind their increased risk of suicide.Reference Rasmussen, Hjelmeland and Dieserud20
General population studies suggest that the prevalence of eating disorders and disordered eating in the UK population does not differ across ethnic groups.Reference Solmi, Hatch, Hotopf, Treasure and Micali2 However, there is evidence that individuals from Black and Asian minority backgrounds are systematically under-represented in eating disorder services.Reference Abbas, Damani, Malik, Button, Aldridge and Palmer21 This could be explained by lower rates of help-seeking, failure to identify eating disorders in these populations in primary care, or both. Qualitative studies have highlighted that lower mental health literacy and greater stigma towards mental health conditions are barriers towards help-seeking for eating disordersReference Wales, Brewin, Raghavan and Arcelus22 and mental health problems in general in minority ethnic communities.Reference Memon, Taylor, Mohebati, Sundin, Cooper and Scanlon23 Interventions aimed at increasing mental health literacy could therefore have multiple benefits – from encouraging greater help-seeking to reducing internalised stigma and improving people's quality of life. For instance, a recent systematic review found that interventions that focused on biological explanations of eating disorders, as opposed to sociocultural ones, were more successful at reducing stigma towards these conditions.Reference Doley, Hart, Stukas, Petrovic, Bouguettaya and Paxton24 However, the same review also cautioned against excessive reliance on biological explanations as these might give rise to deterministic beliefs around the difficulty of recovering from or preventing an eating disorder.Reference Doley, Hart, Stukas, Petrovic, Bouguettaya and Paxton24 Our study suggests that, increasing public understanding that eating disorders also affect males and people from ethnic minority backgrounds as part of anti-stigma campaigns could help de-stigmatise them in these groups. It is therefore important that public health campaigns aimed at improving mental health literacy are inclusive and target diverse groups.
In conclusion, we found that although stigmatising views towards eating disorders had improved in 2008 compared with the late 1990s, core differences vis-à-vis other conditions, remained. Although new surveys presenting more current data are needed, our study still provides useful insights on which aspects of eating disorder mental health literacy might need to be addressed by future anti-stigma and mental health literacy campaigns, and which groups might benefit from the latter. Such interventions should be considered a key priority alongside other public health strategies as they are likely to promote greater help-seeking behaviours, improve individuals’ well-being and lead to greater investment in research and clinical services, ultimately leading to improved prognosis and opportunities for prevention.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1192/bjp.2021.175
Data availability
The data-sets used in this study are available free of charge on the https://ukdataservice.ac.uk/ website.
Author contributions
F.S. formulated the research question and designed the study with input from all authors; F.S. analysed the data; J.G. and F.S. drafted the manuscript. All authors contributed to interpreting the results and revising the manuscript.
Funding
F.S.. is funded by the Wellcome Trust (Sir Henry Wellcome Fellowship; grant code: 209196/Z/17/Z). This research is also supported by the UCLH NIHR Biomedical Research Centre.
Declaration of interest
The authors declare that they have no conflict of interest







 Open access
Open access
eLetters
No eLetters have been published for this article.