Burns are defined by the WHO as ‘an injury to the skin or other organic tissue primarily caused by heat, radiation, radioactivity, electricity, friction or contact with chemicals’(Reference Greenhalgh and Saffle1). Despite significant advancements in techniques to prevent burn incidences, severe burn injuries remain the most catastrophic damage that can be survived, and they pose a global public health concern(Reference Wischmeyer2–Reference Berger, Binz and Roux4).
Severe burns lead to serious pathophysiological stress reactions and drastically incremented metabolic rate, which might be long lasting(Reference Clark, Imran and Madni5). Moreover, severe catabolic state leading to reduced body mass, negative nitrogen balance and whole-body protein breakdown, similar to acute severe malnourishment, can happen when more than 20 % of the total body surface area is involved(Reference Prelack, Dylewski and Sheridan6).
Managing the nutrition of patients who have suffered from severe burns can be a challenging task for healthcare professionals, including physicians and dietitians. Considering the risky hypermetabolic response, intensified losses and requirements, as well as changed glucose metabolism following burn injury(Reference Clark, Imran and Madni5,Reference McClave, Taylor and Martindale7–Reference Williams, Branski and Jeschke11) , nutritional interventions depending on the areas of burn, risk of malnutrition or any other concomitant disorders are vital factors for the treatment of patients with severe burns, along with prominent outcome effectors(Reference Clark, Imran and Madni5,Reference Natarajan12) . Thus, understanding the beneficial effects of nutritional interventions is vital because this could result in better patient outcomes, including reduced length of hospital stay, as well as mortality. Fortified oral diets, complementary beverages and enteral or parenteral nutrition are some ways in which this support could be provided(Reference Tan, Danilla and Murray13). Also, arginine, glutamine and n-3 fatty acids are among the dietary agents that have been considered for patients with severe burns(Reference Heyland, Wibbenmeyer and Pollack14).
Despite numerous systematic reviews and meta-analyses (SRMA) of intervention trials on the impact of various nutritional interventions in patients with burn injury, the findings about the effectiveness of each nutritional intervention remain varied, and the quality of studies has not yet been assessed. For instance, regarding enteral nutrition, one SRMA found no considerable impact on the length of hospital stay and ventilation day(Reference Pham, Fang and Vrouwe15); however, one SRMA indicated a substantial improvement in mortality(Reference Pu, Doig and Heighes16). Moreover, regarding glutamine supplementation, three SRMA did not reveal any significant effect on outcomes(Reference Ortiz-Reyes, Lee and Lew17–Reference Yue, Wang and Zeng19); however, two SRMAs showed beneficial effects(Reference Lin, Chung and Yang20,Reference Mortada, Alhindi and Abukhudair21) . Considering the value of improving burn-related outcomes in adults and the ambiguity regarding which kind of nutritional interventions are helpful, a thorough umbrella review is required to provide information about effective interventions to improve outcomes in patients with burn injuries. Therefore, this review aimed to assess the impact of various nutritional interventions in patients with burn injuries and rate the certainty of evidence gathered.
Methods
According to the Cochrane Handbook for Systematic Reviews, this umbrella review was conducted(Reference Higgins, Altman, Higgins and Green22). The study followed the guidelines of the ‘Grading of Recommendations Assessment Development, and Evaluation’ handbook(Reference Page, Moher and Bossuyt23) and the ‘The Preferred Reporting Items for Overviews of Reviews’ statement(Reference Gates, Gates and Pieper24) (online Supplementary Table S1). The PROSPERO website registered the protocol of this study (CRD42024496620).
Search strategy and eligibility criteria
A search was conducted on PubMed/Medline, Science direct, Scopus, Web of Sciences and Embase databases of systematic reviews from 1990 to August 1, 2024, to locate meta-analyses of intervention trials (online Supplementary Table S2). No language restriction was applied. Removal of duplicates was carried out after importing the identified articles to EndNote.
Eligibility criteria study selection
To be included, the studies met the following criteria: meta-analyses of randomised controlled trials (RCT) investigating associations with seven nutritional interventions (early enteral nutrition, combined immunonutrition, glutamine, branched-chain amino acids (BCAA), fish oil, ornithine α-ketoglutarate and trace elements) among adults with complication-related burn injury, including overall mortality, length of hospital stay, sepsis, pneumonia, overall infection, wound infection and ventilation day. Two reviewers (F.N. and A.H.) conducted independent screening of titles and abstracts to determine relevance and selected studies after reviewing the full text of potentially eligible articles. Any discrepancies were resolved by discussion with the third reviewer (H.M.). We excluded articles that did not have full text, reviews or meta-analyses of studies with different designs and those that did not include a control group.
Data extraction
The task of data extraction and quality assessment was carried out independently by two reviewers (M.R. and S.H.) and then reviewed by two other reviewers (F.N. and S.Z.M). Consensus was reached to resolve discrepancies. The meta-analyses of eligible systematic reviews provided information on various aspects including trial and participant numbers, study duration, effect sizes for clinical outcomes, heterogeneity, publication bias risk, population and intervention characteristics and outcome certainty level. We prioritised effect sizes from the meta-analysis with the most RCT if it included an RCT in multiple meta-analyses on the same outcome. The study presents effect sizes along with their corresponding CI and P values.
Assessment of methodological quality
We used the A Measurement Tool to Assess Systematic Reviews tool to assess the methodological quality of the systematic reviews(Reference Shea, Reeves and Wells25). It contains sixteen questions. The Cochrane risk-of-bias tool was used to evaluate the methodological quality of the RCT included in the meta-analysis (online Supplementary Tables S5)(Reference Higgins, Altman and Gøtzsche26). The quality assessments were conducted by two independent investigators, S.T. and S.Z.M. A third author was involved in reaching a consensus to resolve any disagreements (H.M.).
Data synthesis and statistical analysis
We included all relevant RCT with data on a clinical outcome for the quantitative synthesis, regardless of their inclusion in any reviews. Then, we obtained effect sizes and 95 % CI from the original studies in the largest systematic review. To account for within- and between-study heterogeneity, we applied a conservative random-effects model to recalculate the mean differences or relative risks for each meta-analysis, along with their corresponding 95 % CI(Reference DerSimonian and Laird27). Because of heterogeneity of the included studies in terms of study population and study design, random-effect model was used to homogenised the data for meta-analysis. The I2 statistic was used to assess and report heterogeneity quantitatively, and a χ 2 test for homogeneity was conducted (P heterogeneity > 0·10). According to the Cochrane Handbook guidance, we interpreted the I2 values as follows (0–40 %, might not be important; moderate heterogeneity may be represented by a range of 30–60 % and the range of values, from 50 % to 90 %, indicates potential heterogeneity; 75–100 %, may represent considerable heterogeneity)(Reference Cumpston, Li and Page28). Publication bias was evaluated through visual inspection of funnel plots and using P values from the Egger test(Reference Egger, Smith and Schneider29).
Grading of the evidence
We used the GRADE criteria to evaluate evidence quality in a meta-analysis, considering five domains: (1) individual study bias, (2) inconsistency, (3) indirectness, (4) imprecision and (5) publication bias(Reference Langendam, Akl and Dahm30). We applied the GRADE criteria to evaluate the evidence quality per effect in a meta-analysis, focusing on five domains.
Results
The flow diagram of literature search in electronic databases is indicated in Fig. 1. Following a comprehensive search and after excluding duplicate papers, we recognised 2363 articles, of which 2342 were removed at the titles/abstracts stage screening. Of twenty-one articles that went through full-text reviewing, ten were excluded due to the outlined following reasons: Systematic review without meta-analysis (n 1); unavailable full text (n 1); no relevant intervention (n 4); no relevant outcome (n 1); different study design (n 1) and duplicate (n 2) (online Supplementary Table S3). Finally, eleven meta-analyses were selected for inclusion in our review.

Fig. 1. Literature search and review flow diagram for selection of studies.
Thirty-three original intervention trials from eleven meta-analyses have been included in our umbrella review. Overall participants and follow-up length were spanned from twenty to 1399 participants (median = 244), as well as 11 d to 24 weeks. The publication year of our selected intervention trials were between 1990 and 2022. The original intervention trials recorded in the eligible reviews entered seven different types of nutritional interventions (early enteral nutrition, combined immunonutrition, glutamine, BCAA, fish oil, ornithine α-ketoglutarate and trace elements). In addition, the outcomes examined in adult patients with burn injury involved overall mortality, length of hospital stay, sepsis, pneumonia, overall infection, wound infection and ventilation day.
The effect of nutritional interventions on overall mortality
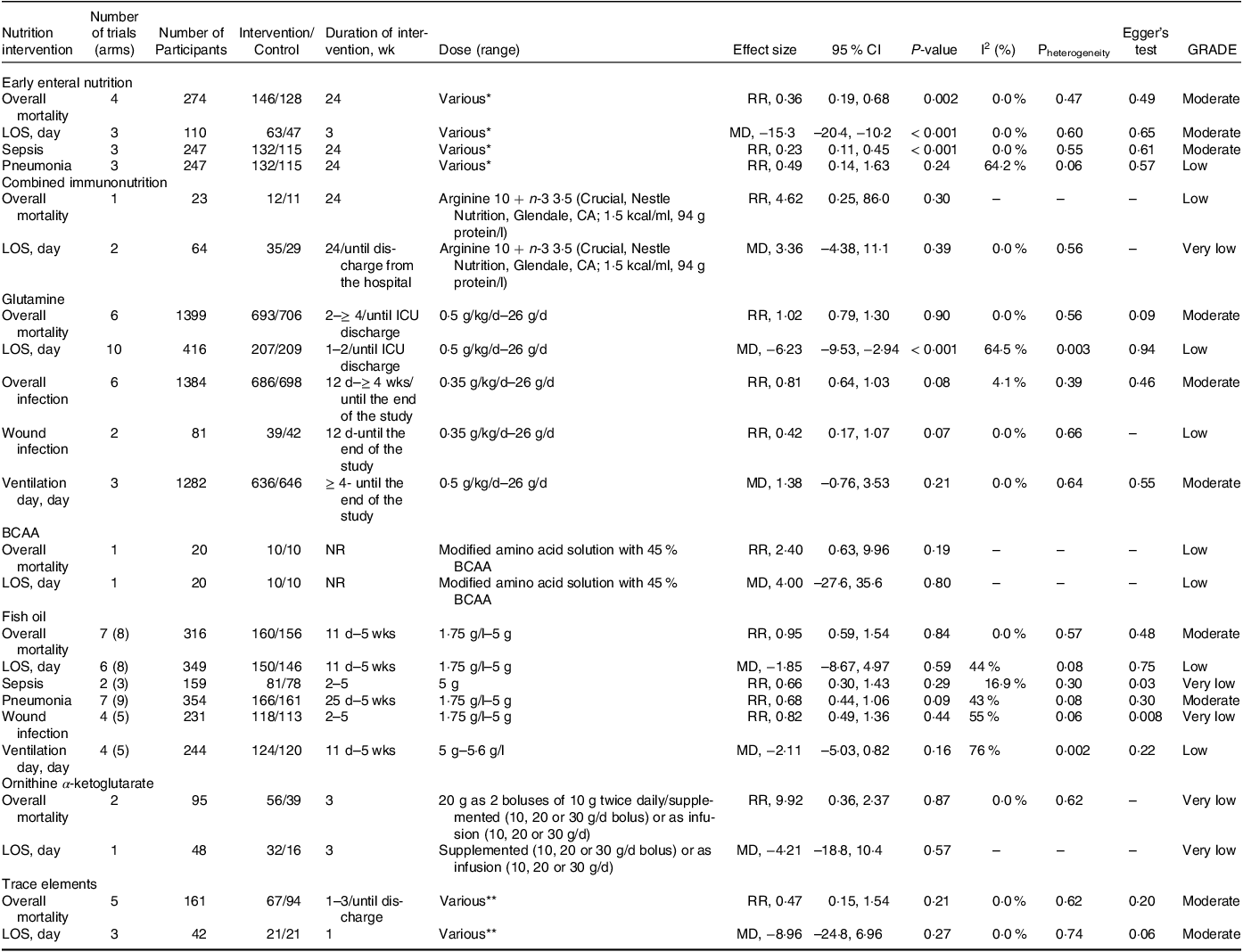
All nutritional interventions examined their impacts on the incidence of overall mortality. In burn patients, early enteral nutrition has been found to significantly reduce the incidence of overall mortality (RR: 0·36, 95 % CI: 0·19, 0·68, I2 = 0·0 %; moderate evidence certainty; n 4 trials). However, other interventions, including combined immunonutrition (RR: 4·62, 95 % CI: 0·25, 86·0), glutamine (RR: 1·02, 95 % CI: 0·79, 1·30), BCAA (RR: 2·40, 95 % CI: 0·63, 9·96), fish oil (RR: 0·95, 95 % CI: 0·59, 1·54), ornithine α-ketoglutarate (RR: 9·92, 95 % CI: 0·36, 2·37) and trace elements (RR: 0·47, 95 % CI: 0·15, 1·54) did not show a significant impact (Table 1), with moderate to very low GRADE evidence. All intervention trials showed no significant publication bias (Table 1).
Table 1. The effects of nutritional interventions in burn patients

BCAA, branched-chain amino acids; CI, confidence interval; d, day; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; LOS, length of hospital stay; MD, mean difference; NR, not reported; RR, relative risk; wk, week.
* As soon as possible after ICU admission: 500 kcal provided in the first 24 h of ICU stay, then increased to reach at least 75 % of calculated targets in the next few days (Goals set by the Curreri formula) or within 24 h of burn injury: EN commenced at 20 ml/h in adults. Rate increased every 6 h as tolerated until goal reached (Goal set using Harris-Benedict) or Within 4 h after admission: 25 ml/h EN via NJT infused by pump during the daytime for 12–16 h over 3–5 d or Within 6 h after injury: 100–125 ml/h via NJT, providing 2000 kcal in the first 24 h. Increased to 4000 kcal over the next 2–3 d or Immediately after admission: 50 ml/h ‘homemade’ EN (1900 kcal/l and 79 g protein/l) via NGT increasing over 3–4 d. Goal set with Curreri formula. Rate did not exceed 150 ml/h.
** 2·4 mg Cu, (15·04 µmol Cu) 82 µg Se, (0·434 µmol Se) 26·5 mg Zn (194·44 µmol Zn) or Cu (40·4 µmol), Se (2·9 µmol), Zn (406 µmol) or 59 µmol Cu, 4·8 µmol Se, and 574 µmol Zn or 15 mg elemental Zn or 75 mg/d Zn.
The effect of nutritional interventions on length of hospital stay
All nutritional interventions were examined for their impacts on the length of hospital stay. In burn patients, early enteral nutrition (MD: −15·3, 95 % CI: −20·4, −10·2, I2 = 0·0 %; moderate evidence certainty; n 3 trials) and glutamine (MD: −6·23, 95 % CI: −9·53, −2·94, I2 = 64·5 %; low evidence certainty; n 10 trials) have been found to significantly reduce the length of hospital stay (Table 1). In contrast, with moderate to very low GRADE evidence, other interventions included combined immunonutrition (MD: 3·36, 95 % CI: −4·38, 11·1), BCAA (MD: 4·00, 95 % CI: −27·6, 35·6), fish oil (MD: −1·85, 95 % CI: −8·67, 4·97), ornithine α-ketoglutarate (MD: −4·21, 95 % CI: −18·8, 10·4) and trace elements (MD: −8·96, 95 % CI: −24·8, 6·96) revealed no considerable impact on the length of hospital stay (Table 1). All intervention trials revealed no considerable publication bias (Table 1).
The effect of nutritional interventions on sepsis and pneumonia
Two nutritional interventions, early enteral nutrition and fish oil, were studied for their impact on the incidence of sepsis and pneumonia. While neither intervention significantly reduced the risk of pneumonia, early enteral nutrition significantly reduced the risk of sepsis (RR: 0·23, 95 % CI: 0·11, 0·45, I2 = 0·0 %; moderate evidence certainty; n 3 trials).
We also found considerable publication bias for pooled trials that compiled data on the risk of sepsis following fish oil intervention (Pegger = 0·03) (Table 1).
The effect of nutritional interventions on infection
Two nutritional interventions, glutamine and fish oil, were studied for their impact on the incidence of overall, as well as wound infection. With low to very low GRADE evidence, glutamine (RR: 0·42, 95 % CI: 0·17, 1·07) and fish oil (RR: 0·82, 95 % CI: 0·49, 1·36) interventions had no significant impact on improving the risk of wound infection (Table 1).
We also found considerable publication bias for pooled trials that compiled data on the risk of wound infection following fish oil intervention (Pegger = 0·008) (Table 1).
The effect of nutritional interventions on ventilation day
Two nutritional interventions, glutamine and fish oil, were studied for their impact on the ventilation day. With moderate to low GRADE evidence, glutamine (MD: 1·38, 95 % CI: −0·76, 3·53) and fish oil (MD: −2·11, 95 % CI: −5·03, 0·82) interventions had no significant impact on reducing the ventilation day (Table 1). Moreover, all intervention trials revealed no considerable publication bias (Table 1).
Methodological quality
Findings of quality assessment of entered reviews are revealed in online Supplementary Table S5. Evidence quality of entered reviews are ‘high’, ‘low’ and ‘critically low’ at 45·5 %, 9 % and 45·5 %, respectively.
Discussion
The results of the present umbrella review study showed that among the nutritional supplementation effects on patients with burn, with moderate evidence certainty, early enteral nutrition could significantly reduce the overall mortality, length of hospital stay and risk of sepsis. Also, with low certainty of evidence, glutamine supplementation has been shown to improve the length of hospital stay significantly. However, other interventions, including combined immunonutrition, BCAA, fish oil, ornithine α-ketoglutarate and trace elements, had no special effects on clinical outcomes.
The positive changes in clinical results shown in this study align entirely with the physiological reasoning provided to endorse early enteral nutrition in prominent clinical practice guidelines(Reference Rousseau, Losser and Ichai8). Early enteral nutrition helps preserve the immune function of the intestinal mucosal barrier, consequently minimising consequences associated with bacterial translocation(Reference Pu, Doig and Heighes16). The digestive system is widely recognised as the most responsive organ to reduced blood flow. For example, in people with good health who engage in light exercise for some time every day, it causes splanchnic hypoperfusion(Reference Luo, Tan and Peng31,Reference Van Wijck, Lenaerts and Van Loon32) . This condition undermines the integrity of epithelial cells, resulting in heightened permeability and the triggering of neutrophils. Shortly following a severe burn injury, individuals are recognised to experience alterations in the gastric and duodenal mucosa, indicative of ischaemic damage(Reference McClave and Heyland33). These changes may advance to ulcerative erosions, leading to the presence of hidden blood in stools or, in extreme cases, posing a risk of life-threatening bleeding(Reference Kumar and Sudhakar34).
Moreover, these ischaemic alterations in the intestines undermine the immune function, permitting the movement of bacteria from the intestinal tract to other parts of the body(Reference Fayazov and Akhmedov35). Apart from raising the likelihood of infectious side effects, the excess presence of gut bacteria stimulates leucocytes and macrophages specific to certain tissues. This activation triggers an inflammatory sequence that sets off subsequent organ failures and contributes to the clinical manifestation of sepsis(Reference Corcione, Lupia and De Rosa36,Reference Earley, Akhtar and Green37) .
It has been reported in some of the cohort and cross-sectional studies among the participants hurt by the burn that those who are administered early enteral nutrition had significantly lower odds of gastrointestinal haemorrhage(Reference Mosier, Pham and Klein38–Reference Lam, Tien and Khoa40). Animal samples subjected to fluid resuscitation demonstrate that, regardless of cardiac output, the provision of early enteral nutrition leads to a notable rise in blood flow to different parts of the digestive system following a significant burn(Reference Inoue, Lukes and Alexander41). The maintenance of blood flow through early enteral nutrition sustains the immune function of the gut’s physical barrier, leading to a considerable reduction in measurable bacterial translocation(Reference Kurmis, Nicholls and Singer42,Reference Shahi, Skillman and Phillips43) . The provision of early enteral nutrition also lowers the measurable presence of endotoxin in the bloodstream, dampens the exaggerated cortisol reaction to burn injuries, diminishes tumor necrosis factorα and improves the host’s capability to eliminate translocating bacteria(Reference Lu, Huang and Yu44,Reference Morvaridzadeh, Nachvak and Agah45) . Preserving the immune function of the digestive system through early enteral nutrition emerges as a likely phenomenon behind the significant clinical effects observed in our study. This maintenance of gut integrity results in a decreased damage to the digestive system, reduced infectious side effects, a lowering of subsequent organ failures and a diminished likelihood of sepsis onset(Reference Parsi, Torkashvand and Hajiani46,Reference Wu, Liu and Jin47) . The collective advantages of these outcomes contribute to enhanced patient survival and a shorter hospital length of stay.
In the present study, we found that glutamine supplementation significantly reduced the length of hospital stay. However, we could not find any significant improvement in the overall mortality, duration of ventilation and wound infection. In a meta-analysis study by Ortiz-Reyes et al., they showed that glutamine demonstrated a notable decrease in both mortality and instances of infectious complications in one-centre trials, although this effect was not observed in trials conducted across multiple centres(Reference Ortiz-Reyes, Lee and Lew17). In terms of mechanisms, adding glutamine helps reduce inflammation originating from the gut, sustains immune functions, shields against burn-related myocardial injury, preserves muscle metabolism and safeguards cells from injury(Reference van Zanten, Dhaliwal and Garrel18,Reference Heyland, Wischmeyer and Jeschke48,Reference Rahimlu, Shab-Bidar and Djafarian49) . Specific research findings indicated that glutamine exhibited the most significant impact in reducing damage to the intestinal mucosa(Reference Zhang, Yan and Lv50). Diamine oxidase (DAO) is an enzyme that removes amino groups from histamine and polyamines, reaching its peak activity in the intestinal mucosa across various mammalian species, including humans(Reference Sun, Wang and Zhou51). DAO is primarily located in the small intestine, and its function is strongly linked to the synthesis of nucleic acid and protein in the intestinal tract. The levels of DAO in the bloodstream correspond to the content of DAO and structural alterations in the intestinal mucosa(Reference Sun, Wang and Zhou51). Studies have demonstrated that plasma DAO activity accurately mirrors changes related to mucosal injury in severe trauma cases. Some studies showed a notable rise in DAO activity following burn injuries, and following a 7-d regimen of glutamine treatment, there was a significant reduction in DAO levels(Reference Sun, Wang and Zhou51–Reference Hashemi, Rahimlou and Baghdadian53).
In this umbrella review study, we could not find any significant effects of other nutritional interventions, including fish oil, combined immunonutrition, BCAA, ornithine α-ketoglutarate and trace elements on other burn-related outcomes. The results of other meta-analysis studies investigating the effect of n-3 supplementation in enteral nutrition in critically ill patients have shown that n-3 supplementation had no significant effect on outcomes such as mortality or length of hospitalisation(Reference Koekkoek, Panteleon and van Zanten54).
Based on our knowledge, the present study was the first umbrella review study that examined the effects of different nutritional interventions among patients with burns. However, some limitations in the present study should be considered. First, there were disparities in how metrics and clinical outcomes were reported across studies. Furthermore, most of the meta-analyses incorporated in the study did not assess the severity of burn injuries, including factors like burn depth, baseline organ dysfunction degree or the Nutrition Risk in the Critically Ill Score(Reference Ortiz, Jiang and Turgeon55,Reference Ostadrahimi, Nagili and Asghari-Jafarabadi56) . Consequently, these aspects could not be analysed in our research. Third, the studies did not consider baseline concentrations of some nutrients, such as glutamine. Fourth, not considering lifestyle modification like dietary intakes and level of physical activity in most of the included studies should be considered as one of the important limitations of the present research. Finally, the certainty of the evidence was weak for some findings in the present study.
Conclusion
In conclusion, our umbrella review comprehensively assessed the impact of various nutritional interventions on clinical outcomes in patients with burn injuries. Early enteral nutrition emerged as a significant contributor, demonstrating a substantial reduction in overall mortality, length of hospital stay and the risk of sepsis. Additionally, glutamine supplementation showed a notable decrease in the length of hospital stay. However, other nutritional interventions, including combined immunonutrition, BCAA, fish oil, ornithine α-ketoglutarate and trace elements, did not exhibit significant effects on the assessed clinical outcomes. Despite some limitations, our study provides valuable information for clinicians and researchers, highlighting the potential benefits of early enteral nutrition and glutamine supplementation in improving outcomes for patients with burn injuries. Further well-designed research addressing the identified limitations such as consideration of lifestyle modification like dietary intakes and level of physical activity of study participants could enhance our understanding of nutritional interventions in this population.
Acknowledgements
We thank Tehran University of Medical Sciences for its financial support.
All authors conceptualised and designed this review. F. N. and A. H. conducted a literature search. M. R. and S. H. collected the data, and S.Z-M. performed analysis. M. R., S. M. and S. Z-M. wrote the first draft. H. M. contributed to critically revising and interpreting the data. All authors read and confirmed the final manuscript.
All authors declare that they have no conflict of interest.
Data described in the manuscript will be made available upon request pending.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114524002344