



CLINICIAN’S CAPSULE
What is known about this topic?
Gathering visual information effectively is an important task of a physician leader when managing a resuscitation case.
What did this study ask?
Are there particular visual information-gathering patterns associated with performance in simulated resuscitation scenarios?
What did this study find?
Certain visual patterns (e.g., focusing on case-specific clinically relevant stimuli) are associated with better performance in a simulated resuscitation setting.
Why does this study matter to clinicians?
The ability to characterize physician visual patterns across a competence continuum has implications for trainee assessment and medical education.
INTRODUCTION
Successful management of a medical emergency demands effective crisis resource management (CRM) skills.Reference Kim, Neilipovitz, Cardinal, Chiu and Clinch1, Reference Watkins, Roberts, Boulet, McEvoy and Weinger2 Physicians skilled in CRM are usually easily identifiable by their peers, but describing specific behaviours that make them successful in crisis settings is difficult, even for physicians themselves.Reference Szulewski and Howes3 A reason is that high-level CRM skills are automatized over many years as a result of deliberate practice and become second nature.Reference Ericsson, Krampe and Tesch-Römer4 This tacit knowledge is subsequently difficult to describe explicitly and teach.Reference Kaufman, Arocha, Patel, Sternberg and Horvath5, Reference Szulewski, Brindley and Van Merrienboer6
Tacit knowledge poses particular challenges to medical educators who are tasked with preparing and assessing learners in routine and emergent medical cases. It follows that the more that is known about expertise development in the management of medical emergencies, such as resuscitation and CRM, the more likely it will be that both can be taught and assessed effectively and efficiently. Moreover, by triangulating novel objective measures of learner performance with traditional assessment, educators can calibrate both modalities and increase the validity of both subjective and objective means of trainee assessment. This would improve the granularity of resuscitation assessment, with decreased risks to patients, a need that will only increase as medical schools shift to competency-based medical education (CBME).
One commonly used approach to teaching CRM skills well suited to integrating CBME is simulation-based training.Reference Gaba, Howard, Fish, Smith and Sowb7 High-fidelity medical simulation-based training improves learning by providing a forum for feedback, integration of curriculum, and an opportunity for repetitive practice for routine cases, as well as variability of practice for non-routine cases.Reference Issenberg, McGaghie, Petrusa, Lee Gordon and Scalese8-Reference Seppänen and Gegenfurtner10 Formative and summative assessments in simulation are also gaining popularity,Reference Gegenfurtner, Quesada‐Pallarès and Knogler11 especially in postgraduate medical education in which assessment tools are being developed and optimized.Reference Hall, Dagnone, Lacroix, Pickett and Klinger12-Reference Bick, Demaria and Kennedy14
It is difficult to glean a comprehensive view of expertise development in resuscitation medicine using traditional observational research methods. A novel method of studying resuscitation medicine and CRM expertise is with the use of mobile gaze-tracking technology. Gaze-tracking data can provide new insights into clinician behaviour and performance and may lead to improved patient safety practices.Reference Henneman, Marquard, Fisher and Gawlinski15 Mobile gaze-tracking glasses are worn like a pair of eyeglasses that record both a video of a participant’s first-person point-of-view and track the participant’s eye movements, superimposing a gaze indicator on the first-person video, revealing where the participant is looking in real time. Based on data that show what a physician “sees,” inferences can be made on the differences between novices and experts with respect to their visual attention, situational awareness, and ability to manage competing interests.Reference Szulewski, Roth and Howes16
Visual expertise research has shown that there are measurable visual differences between novices and experts in numerous domains that can be quantified using gaze-tracking technology.Reference Bick, Demaria and Kennedy17, Reference Henneman, Marquard, Fisher and Gawlinski18 Experts can selectively ignore irrelevant information, recognize patterns rapidly, and select appropriate diagnostic schemata to fit what they see.Reference Gegenfurtner, Kok and van Geel19 With practice, individuals become better, more efficient interpreters of their surroundings. They are better able to prioritize what is important while simultaneously deprioritizing what is not. Analyzing eye movements in a non-medical field, Haider and FrenschReference Kok, de Bruin, Robben and van Merriënboer20 termed this phenomenon the “information-reduction hypothesis,” and Kok et al.Reference Kok, de Bruin, Robben and van Merriënboer21 hypothesized that there may be parallels to be drawn in medicine.
Gaze-tracking technology has also been used to determine the feasibility of studying physician behaviours during simulated medical emergencies, and it has been shown that this technique is practical and useful in this setting.Reference Szulewski and Howes3 However, little is known about whether physicians’ expertise in the complex environment of resuscitation medicine can be accurately assessed by studying their visual patterns.
Building on this research, this study explored the information-gathering techniques of residents by analyzing their initial visual fixation patterns in a simulated resuscitation environment. Specifically, we were interested in uncovering particular gaze patterns used by physicians that are associated with better exam performance. The objectives of this study were to: 1) examine the relationship between initial visual patterns and performance scores; and 2) explore if these patterns varied in different simulation scenarios.
METHODS
Study design and participants
A convenience sample of emergency medicine (EM) residents at one training site were invited to participate in two exams, each comprised of two simulated scenarios.
The first two scenarios (S1, diabetic ketoacidosis; and S2, bradycardia secondary to beta-blocker overdose) were conducted in February 2014; the second two scenarios (S3, ruptured abdominal aortic aneurysm [AAA]; and S4, metabolic acidosis caused by antifreeze ingestion) were conducted in August 2014. The scenarios and their associated assessment tools were developed through an iterative process that consisted of a template-based scenario development tool. At least three expert EM physicians reviewed each case for clinical fidelity. A previous study of EM residents, using similar scenarios developed in this manner, demonstrated excellent reliability (as determined through a G-study analysis).Reference Hall, Dagnone, Lacroix, Pickett and Klinger12 The study took place during regularly scheduled biannual simulation-based objective structured clinical exams (OSCEs). Participants had previously participated in similar OSCEs and were familiar with the assessment environment and format; however, the scenarios used in this study were novel to each participant. Participants did not receive any incentives to participate. The study was approved by the Research Ethics Board at Queen’s University (EMED-162-11).
Experimental design
Residents were fitted and calibrated with a mobile gaze-tracking device (Tobii Glasses Eye Tracker, Danderyd, Sweden). After reading a case stem, they entered the high-fidelity simulation lab as the leader of a team comprised of a registered nurse (RN) actor and respiratory therapist (RT) actor. Simulation rooms were organized to mimic the resuscitation bay in the emergency department (ED). The RN and RT began the scenarios in the same locations in the room; however, they were free to move around the room based on instructions given by the resident. Participants completed two 10-minute scenarios. Audio and video data from three (non-gaze-tracking) cameras were also recorded (Kb Port, Allison Park, PA). These videos were subsequently used by the blinded external reviewers to score participant performance.
Analysis
The gaze-tracking device recorded first-person audio and video data and gathered information on pupil position and glint location at a rate of 30 Hz. Using these data, a dynamic gaze indicator was superimposed on the first-person video by computer software (Tobii Studio Pro). This video was used in the analysis to compute the gaze-tracking variables and fixation areas listed in Table 1. Figures 1 and 2 show static representations of the data generated by the software. In this study, fixations referred to instances when the gaze indicator stopped scanning the environment and landed on an area of interest. The frequency and duration of the residents’ gazes were scored independently by two trained individuals who manually analyzed each first-person video. Human raters were used in this study to count fixations, as computer technology that can accurately triangulate eye-tracking data with three-dimensional positional data in a resuscitation room with dynamic areas of interest (where individuals and equipment move) is still under development. The dichotomous actions and visual propensities of the participants were captured (see Table 1), and Pearson correlation coefficients were used to determine whether associations existed with performance. These areas of interest were defined a priori based on their potential clinical relevance and input from local medical experts. We focused this analysis on the first 60 seconds of each scenario, as we were mostly interested in how residents’ initial information-gathering patterns correlated with performance scores. Furthermore, our previous experience suggested that most relevant visual fixations occur early in simulated scenarios and that there is increased variability and noise in gaze patterns as the simulations progress.
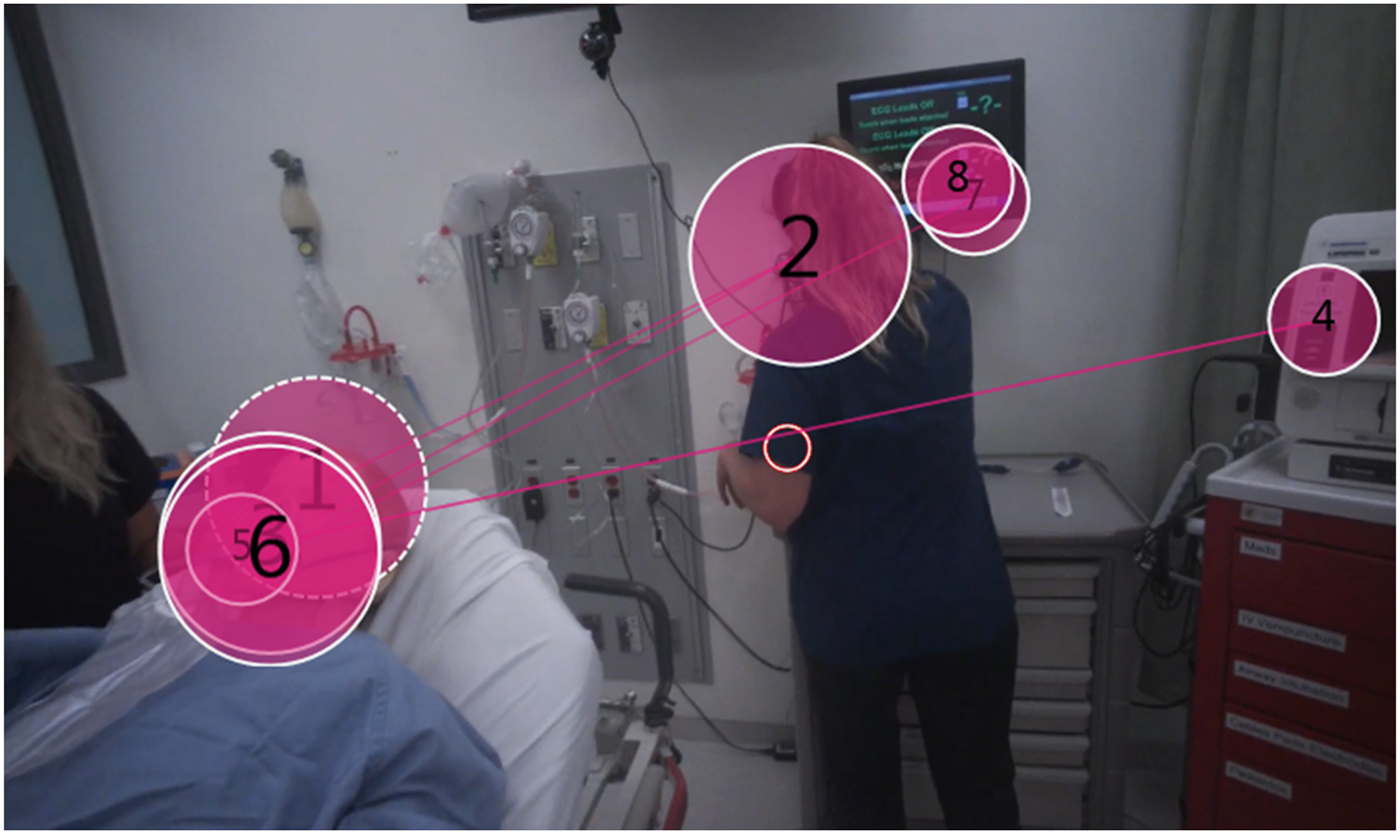
Figure 1 A third year resident’s gaze fixations within the first minute of a simulation. The numbers represent the order in which the resident looked at each area of interest and the size of the circle represents the relative time spent fixating on each of these points.

Figure 2 A third year resident’s gaze fixations within the first minute of a simulation. The colours represent a heat map, where red represents more fixations for a longer duration, followed by yellow and green areas, which represent fewer fixations.
Table 1. Measured gaze-tracking fixation areas
ECG=electrocardiogram; RN=registered nurse; RT=respiratory therapist.
Inter-rater reliability between the two individuals tabulating eye-tracking variables and the expert performance assessors were determined by calculating intraclass correlation coefficients (ICC). For each eye-tracking video, an ICC for aggregated fixation times (total fixation time and time until first vital signs check) and the net number of object fixations in the first 60 seconds were calculated. Two independent undergraduate reviewers used video time stamps and systematic video pausing to record the total gaze duration and frequencies. Reliability was calculated separately for S1 and S2, as well as S3 and S4, as only five participants were involved in all four scenarios.
Performance of the residents was assessed by external attending emergency physicians who were blinded to the participants’ identity and level of training. The Queen’s Simulation Assessment Tool (QSAT) was used for assessment by the physicians after their review of the non-gaze-tracking recordings. The raters had previous experience and training on using the QSAT in this context. The QSAT has been previously shown to discriminate simulation-based OSCE performance with a similar cohort of EM residents within a CRM context.Reference Hall, Dagnone, Lacroix, Pickett and Klinger12 The QSAT (see Appendix 1) assessed residents on a five-point Likert scale from inferior to superior across four categories (primary assessment, diagnostic actions, therapeutic actions, and communication), as well as overall performance.
A factorial analysis of variance (ANOVA) was conducted to determine if score differentials were only a function of training level or if gaze-tracking data provided information on the level of experience that extended beyond the level of training. Grouping of residents by experience in S1/S2 and S3/S4 differed because of uneven numbers of participants across postgraduate years (PGY). Of note, CCFP (PGY-3) residents were considered independent of Fellow of the Royal College of Canada (FRCPC) PGY-3 residents.
RESULTS
Participants
As for participation, 13 and 29 residents took part in the S1/S2 and S3/S4 exams, respectively (five completed both exams). One participant declined to consent to gaze tracking (but still completed the exam). Because of poor data quality and technical errors, the results from three cases in the first OSCE and three cases in the second were excluded. Therefore, a total of 78 cases were subsequently analyzed. Participants were EM residents enrolled in the College of Family Physicians of Canada (CCFP) and the Royal College of Physicians and Surgeons of Canada (RCPSC) programs (see Table 2) at one EM training site (mean age 30.0 years, standard deviation [SD] 2.91, and 48% were female residents).
Table 2. Number of participants by level of training and simulated case for the analyzed data
AAA=abdominal aortic aneurysm; CCFP=College of Family Physicians of Canada; PGY=postgraduate year.
* A total of six cases were excluded because of poor data quality and technical errors.
Gaze-tracking data
Appendix 2 outlines the average fixation data for the scenarios. An acceptable average ICC was found for the fixation time ratings between the two individuals who analyzed the gaze-tracking videos in S1 and S2 (ICC=0.87, p<0.001, 95% confidence interval [CI] 0.15–0.97); however, an unacceptable ICC was found for S3 and S4 (ICC=0.39, p<0.001, 95% CI −0.22 to 0.71). An acceptable average ICC was found for the net number of object fixations (first 60 seconds) for S1 and S2 (ICC=0.67, p<0.032, 95% CI −0.03 to 0.90]) and S3 and S4 (ICC=0.82, p<0.001, 95% CI 0.59–0.92). Fixation time ratings were thought to be unsatisfactory largely because of the difficulty of manually recording the time and number of gazes. The future development of automated tracking processes would be beneficial to the accuracy of tracking.
Performance scores
The calculated ICC was very good between the two expert assessors in S1 (ICC=0.85, p<0.01, 95% CI 0.45–0.96) and S2 (ICC=0.87, p<0.001, 95% CI 0.02–0.97). Only one external blinded assessor reviewed S3 and S4. Assessors scored participants across four categories for a total score, in addition to an overall impression score. A two-way mixed ICC was calculated for absolute accuracy between the raters for the total and overall scores. The findings showed acceptable reliability between the total and overall scores for S1 (ICC=0.933, p<0.001, 95% CI 0.65–0.98]), S2 (ICC=0.987, p<0.001, 95% CI 0.95–0.99), S3 (ICC=0.95, p<0.001, 95% CI 0.86–0.98), and S4 (ICC=0.87, p<0.001, 95% CI 0.70–0.94). Because of the congruency between the total and overall scores and between assessors, an average was taken between the percent total and overall scores for each scenario to create a new average score. This final score was used for subsequent analyses (see Appendix 3). After checking for normality, correlations were computed to determine associations between the data points in Table 1 and simulation performance scores.
Relationship between the level of training and performance
In S1 and S2, residency years were separated into three categories: PGY-1 to PGY-4 (mean or M; M S1 =0.57, S2=0.60), PGY-5, (M S1=0.90, S2=0.93), and CCFP (PGY-3) (M S1=0.58, S2=0.56). A significant difference was demonstrated regarding the main effects between groups for S1 (F statistic or F;F[2, 8]=5.32, p=0.03, β=0.67) and S2 (F[2, 9]=4.90, p=0.04, β=0.65). There were significant differences between PGY-5 and CCFP PGY-3 residents (p=.034) in S1. No significant differences were found among the groups in S2. In S3 and S4, residency years were separated into three categories: PGY-1 and PGY-2 (M S3=0.64, S4=0.59), PGY-3 to PGY-5 (M S3=0.75, S4=0.63), and CCFP (PGY-3) (M S3=0.66, S4=0.57). No detectable significant difference was demonstrated between residency groupings in S3 (F[2, 25]=1.65, p=0.2, β=0.32) and S4 (F[2, 25]=0.14, p=0.86, β=0.07). Because of differences in the number of participants and spread of the residents’ level of training between S1/S2 and S3/S4, the groupings could not be consistent. Independent t-tests were used to determine the ordering effects across scenarios. No effects of ordering were found (p>0.4). A sample size calculation was not performed, as we maximized the number of residents who were available to participate. Instead, we have provided statistical power calculations (β).
Relationship between gaze tracking and performance
The observed correlations between the gaze-tracking variables and average performance score are shown in Tables 3–5 (Please see Appendix 4 for the complete correlation tables). Significant correlations in S1, S3, and S4 indicated that visually fixating on particular people and objects was correlated with performance.
Table 3. Correlations between selected gaze indicators and the average score in S1 (diabetic ketoacidosis)
RT=respiratory therapist.
*p<0.05.
Table 4. Correlations between selected gaze indicators and the average score in S3 (ruptured AAA)
ECG=electrocardiogram; RN=registered nurse.
*p<0.05, †p<0.01.
Table 5. Correlations between selected gaze indicators and the average score in S4 (metabolic acidosis)
*p<0.05.
DISCUSSION
Residents’ gaze-tracking patterns were found to be significantly correlated with objective performance in the simulation-based resuscitation examinations. Because of the number of participants and array of data, correlation was used to elucidate patterns and associations. Given that this was a pioneering study on the use of gaze analytics to establish patterns associated with performance, these results have not been put forward as definitive findings; rather, they lay the groundwork for future study in this novel area.
In S1 (unstable patient with diabetic ketoacidosis), performance was strongly and positively correlated with decreased latency in checking the patient’s vital signs, a task-relevant stimulus (Pearson’s r 0.70, p<0.05). The number of times a participant looked at the RT was negatively correlated with performance (Pearson’s r − 0.65, p<0.05). In this case, the RT did not provide any useful clinical information and also did not have a predefined script. In addition, the patient did not require any advanced airway intervention and did not have any increased work during breathing; therefore, it is plausible that increased views were not only task irrelevant but also potentially associated with help seeking or other attempts at social validation.
In S2 (beta-blocker overdose), there were no statistically detectable correlations identified. This is likely a result of multiple factors. First, the scenario and corresponding assessment tool were unable to discriminate by the level of training. Anecdotally, it seems that there was malalignment between the scenario design features and expected trainee behaviours. For example, many senior trainees did not perform transcutaneous pacing and focused instead on applying antidotes and medical management immediately for beta-blocker toxicity. Retrospectively, this was not an unreasonable management decision. However, raters were informed that transcutaneous pacing was an important therapy for this patient and likely rated these performances with a lower score.
In S3 (patient with a ruptured AAA), we found that visual fixations on task-irrelevant stimuli such as the laboratory values, electrocardiogram (ECG), and nurse were all strongly and negatively correlated with objective performance (Pearson’s r −0.50, −0.39, and −0.46, respectively; p<0.05). A physician who made a diagnosis of a ruptured AAA should be primarily focused (after initial stabilization) on transporting the patient to the operating room for life-saving surgery. On video review, it was observed that higher performers expedited patient transfer by concentrating on contacting the vascular surgeon, calling the operating room charge nurse, and ensuring that the patient was on portable monitors and ready for rapid transfer. We did not tabulate these areas of interest in the data collection, as these tasks were not predicted to be relevant a priori.
In S4 (patient with metabolic acidosis caused by antifreeze ingestion), participants needed to provide primary resuscitation and appropriately manage a patient with an undifferentiated metabolic acidosis. The number of times a participant fixated on the medication list was correlated with poorer performance (Pearson’s r −0.48, p<0.05). These low-performing participants tended to assume that a medication overdose was the cause of the patient’s condition and overlooked clues that pointed to ingestion of another toxic compound (antifreeze in this case). Those who performed better identified the appropriate agent and spent less time viewing the patient’s medication list.
As in clinical practice, each scenario was different from the others and required medical learners to focus their attention on differentiating stimuli to be successful. Because these visual patterns differ from scenario to scenario, it would be difficult for a learner to feign superior visual behaviours without having the requisite knowledge and experience of a high-performing medical learner.
These findings can be considered within the context of the information-reduction hypothesis. This hypothesis submits that as people gain experience and improve their performance, they are better able to identify (and rapidly deprioritize) task-irrelevant stimuli quickly, while appropriately prioritizing task-relevant stimuli.Reference Haider and Frensch20, Reference Haider and Frensch22 Further, improvement in speed and performance on a task are partially because of a reduction in the amount of information that an individual processes at the perceptual level. Newer eye-tracking research adds evidence to this theory, as domain experts have been found to have more fixations of a longer duration on task-relevant information and fewer fixations of a shorter duration on task-irrelevant information.Reference Gegenfurtner, Lehtinen and Säljö17
The decreased ability to appropriately shift visual attention away from task-irrelevant stimuli may be related (at its extreme) to the concept of “helmet fire.” In helmet fire, an overload of stimuli overwhelms the working memory resources of a (usually) more inexperienced physician when tasked with the management of a sick patient under high-stress conditions. Helmet fire decreases task performance and is observed in many novices in both simulation and clinical practice when managing a situation beyond their comfort level.
In our study, candidates were not specifically presented with task-irrelevant information. Task-irrelevant stimuli could be seen by some as distractors that may artificially inflate difficulty. The authors argue that, in the future, adding realistic distractors may increase the opportunity to observe discriminating behaviours that are indicative of expertise.
It may have been expected that we would have identified more positive correlations with task-relevant areas, as well as negative correlations with task-irrelevant areas. A possible explanation was found on video review. While expert avoidance of task-irrelevant stimuli is striking, consistency in viewing task-relevant data is much less obvious and systematic. Experts may take different paths to get to the same diagnostic and therapeutic destinations, and, thus, do not have chronologically consistent viewing patterns. It is also plausible that much of what makes experts proficient is their ability to effectively process information cognitively that may be challenging to discern accurately with gaze tracking.
Our study had certain limitations. As a correlational study with multiple comparisons, results should be interpreted as hypothesis generating. As a result, we limit our interpretation of this data to the general observation that higher performing residents were better able to appropriately prioritize relevant information while deprioritizing irrelevant information in simulation-based examinations. We propose that future studies design scenarios to incorporate (a priori) realistic task-irrelevant stimuli to more accurately simulate the clinical environment and better elucidate discriminating behaviours that might be indicative of expertise. These studies should utilize an experimental design to allow for causal conclusions about gaze tracking and performance to be made. Further, we observed poor ICC and inter-rater reliability between the two individuals tabulating the results and only included one external blinded assessor for performance scores for S3 and S4. Future studies that use automated computer software (as it becomes readily available) to define exactly what constitutes a visual fixation should improve the accuracy of results and speed of data generation. Finally, the authors had to make assumptions about what participants perceived based on what they looked at, without truly knowing whether their attentional resources had attended to these stimuli. Future studies could employ a mixed methods approach with post-scenario interviews to enrich the interpretation of the data.Reference Gegenfurtner, Kok and van Geel19 Finally, our study was conducted in the simulation laboratory; therefore, we could not make conclusions on information-gathering patterns in clinical situations.
CONCLUSIONS
The study results suggest that there are certain visual behaviours in resuscitation-based simulations that are predictive of performance. These visual behaviours vary between cases because certain visual stimuli may be relevant in one patient presentation but irrelevant in another. Individuals who performed better appeared to have an improved ability to deprioritize task-irrelevant information appropriately and selectively process task-relevant information. Gaze tracking may provide educators new insights into the visual processing patterns of medical learners in simulated environments.
Acknowledgements
The authors thank Dr. Melanie Walker for her help with proofreading this manuscript.
Competing interest
The authors would like to acknowledge the Kingston Resuscitation Institute for providing funding for the research assistants and access to the eye-tracking device used in this study. None declared.
SUPPLEMENTARY MATERIAL
To view supplementary material for this article, please visit https://doi.org/10.1017/cem.2018.391









