


The prevalence of obesity is increasing worldwide(Reference Chung Chooi, Ding and Magkos1), and nearly a third of the world population is now classified as overweight or obese(2). This increase in obesity likely results from a complex interaction between changes in the food environment, as well as physical activity (PA), socio-economic, environmental and genetic factors(Reference Chung Chooi, Ding and Magkos1). In general, a substantial proportion of young adults, in particular higher education students, follow unhealthy lifestyles(Reference Dodd, Al-Nakeeb and Nevill3,Reference Peltzer, Pengpid and Samuels4) , which gives cause for concern. Some studies observed that first year university students have significant weight gain(Reference Vadeboncoeur, Townsend and Charlie Foster5), followed by ongoing slow but steady increase in weight(Reference Gores6). Researches among university students show overweight/obesity prevalences of approximately 30 %, with rates higher for men than for women(Reference Peltzer, Pengpid and Samuels4,Reference Sira and Pawlak7–Reference Zhang, Wang and Zhao9) . In particular, the prevalence of overweight/obesity among Spanish university students is about 20 %(Reference Ruiz, del Pozo and Valero10–Reference Cutillas, Herrero and de San Eustaqui12).
Recent studies have found associations between overweight/obesity among university students and certain unhealthy lifestyle such as a high preference for high-fat and high-sugar food(Reference Jiang, Wang and Wu13,Reference Al Sabbah14) , a lack of PA and exercise(Reference Al Sabbah14,Reference Balgoon, Al-Zahrani and Alkhattabi15) , shorter sleep duration and tobacco use(Reference Pengpid and Peltzer8). These lifestyle behaviours have been reported to differ by sex(Reference Pengpid and Peltzer8,Reference Colić Barić, Satalić and Lukesić16–Reference Olfert, Barr and Charlier19) and living arrangement(Reference El Ansari, Stock and Mikolajczyk18,Reference Papadaki, Hondros and Scott20,Reference Freedman21) in university student populations. So, for example, diet quality is usually higher for women than for men(Reference Maskarinec, Namatame and Kang22) and students living away from the parental home have poorer eating habits(Reference El Ansari, Stock and Mikolajczyk18,Reference Papadaki, Hondros and Scott20,Reference Freedman21) .
Regarding diet, university student populations are widely reported to engage in unhealthy eating behaviours such as high consumption of snack foods(Reference Assaf, Brieteh and Tfaily23,Reference Schmidt24) , high consumption of fast foods(Reference Schmidt24,Reference Hultgren, Turrisi and Cleveland25) , insufficient consumption of fruit and vegetables(Reference Assaf, Brieteh and Tfaily23,Reference El Ansari, Ssewanyana and Stock26) and shift from traditional healthy diets (i.e. the Mediterranean Diet) to more unhealthy eating patterns(Reference Hadjimbei, Botsaris and Gekas27). These eating behavioural characteristics are associated with the risk of overweight/obesity. However, in this sense, beyond what to eat, where, when, how and with whom we eat are important too because not only the volume of foods but also the type and variety of foods consumed affect overweight/obesity risk(Reference Conklin, Forouhi and Surtees28). All these characteristics of diet are part of the term ‘meal pattern’ and have an important role in total energy intake and therefore in the regulation of adiposity and body weight(Reference Johnston29); however, to date, no studies have evaluated the influence of meal pattern on overweight/obesity risk in university student populations.
Behaviour acquired during young adulthood, including the stage of university studies, often lasts into adulthood(Reference Craigie, Lake and Kelly30). Therefore, this stage of life is considered a critical period to instil positive dietary and health behaviours to promote optimal health, as well as to prevent immediate health problems, such as obesity(Reference Laska, Lytle and Nanney31), and long-term health problems, such as CVD(Reference Dahm, Chomistek and Jakobsen32). Moreover, an inadequate meal pattern (e.g. characterised by no breakfast and/or the replacement of lunch with snacks) can make feel as if there are not getting enough nutrients from diet, which might be a motivation to use dietary supplements for health benefits(Reference Kobayashi, Sato and Umegaki33). Additionally, to weight loss and to obtain beauty benefits, especially in females, and to build muscle in males are factors that also lead to dietary supplement use in university students(Reference Kobayashi, Sato and Umegaki33). Several studies have estimated that more than half of university students use dietary supplements(Reference Barnes, Ball and Desbrow34,Reference Lieberman, Marriott and Williams35) , with the consequent risk of adverse effects, in particular when they are taken without a prescription(Reference Barnes, Ball and Desbrow34).
Until now, the majority of studies have focused on a single or a few health lifestyle behaviours, even though research has shown that health behaviours often coexist, interact and increase the likelihood of multiplicative illnesses in university students(Reference Dodd, Al-Nakeeb and Nevill3,Reference Bennasar-Veny, Yañez and Jordi Pericas36,Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera37) . Thus, the interactions among lifestyles related to obesity are poorly understood in this population. To our knowledge, no previous studies have analysed multiple overweight/obesity-related lifestyles, focus on the whole lifestyle rather, than a single or a few lifestyle behaviours, in university students.
The aim of the present study was therefore to investigate the prevalence and interactions of overweight/obesity-related lifestyles (specifically, examining whether subjects meet the recommended criteria), in a representative sample of students at a Spanish university, in order to identify the best strategies to combat obesity within this population. These strategies could take advantage of the naturally occurring opportunities offered by this stage of life (i.e. young adult) to induce behaviour changes. In addition, university students are likely to constitute a significant proportion of the socio-economic elite of the future; thus, their habits and behaviours are most likely to become the norm(Reference Monneuse, Bellisle and Koppert38), rendering this population interesting to investigate. Based on the literature data(Reference Dodd, Al-Nakeeb and Nevill3,Reference Pengpid and Peltzer8,Reference Colić Barić, Satalić and Lukesić16–Reference Freedman21,Reference Bennasar-Veny, Yañez and Jordi Pericas36,Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera37) , the following hypotheses were raised: unhealthy lifestyles coexist, interact and increase the risk of overweight/obesity in this population and these effects vary by sex and living arrangement.
Subjects and methods
This study is component of the EHU12/24 project, which is an observational cross-sectional study designed to assess the prevalence of excess body fat (BF) and major risk of developing overweight/obesity, following a standardised protocol and involving a representative sample of the UPV/EHU student population(Reference Telleria-Aramburu, Rocandio and Rebato39). The design, sampling and procedures of the EHU12/24 have been described in detail elsewhere(Reference Telleria-Aramburu, Rocandio and Rebato39).
Study population
Briefly, EHU12/24 project was conducted from February 2014 to May 2017 on a cohort of 603 university students (59·5 % women) aged between 18 and 28 years (with an average age of 20·9 (2·1) years). Participants were recruited using a randomised, multistage, conglomerate procedure and stratified by knowledge area (arts and humanities, sciences, health sciences, social and legal sciences, and engineering and architecture), age and sex. First, a computer randomly selects the subjects according to their knowledge areas and age, and then the subjects are distributed by sex in each knowledge area. Moreover, we assigned a weight to each participant such as that the computed statistics based on the gathered data could be more representative of the population from which the data were retrieved.
In total, 696 of the 1300 students who were invited to participate in the study gave their consent and participated, resulting in a response rate of 53·5%. To be valid for inclusion in the data analysis, the questionnaire (face-to-face) and anthropometry measurements were required. This requirement was met by 603 study participants, accounting for 46·4 % of all participants invited to participate in the research. Participants with missing data were excluded from the study.
The study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Ethical Committee on Human Research of the UPV/EHU (CEISH/193/2013/ARROYO IZAGA). Written informed consent was obtained from all subjects/patients.
The following eligibility criteria for inclusion were established to recruit a healthy population: (1) Caucasian adults (majority ethnic group in this population) aged between 18 and 28 years; (2) no current reported diseases, except for overweight/obesity (the participants could have excess BF), or conditions (such as being an athlete) that may affect the weight, height, frame size and/or body composition; (3) no relation to other participants and (4) in the case of female students, no pregnancy or breast-feeding.
Body measurements and other characteristics
A well-trained anthropometrist performed all measurements following the ISAK protocols(Reference Marfell-Jones, Olds and Stewart40). The anthropometrical measurements analysed included the following skinfold thicknesses: bicipital, tricipital, subscapular and suprailiac. Body density was calculated from the sum of the average skinfold thicknesses at each site by using the equations of Durnin & Womersley(Reference Durnin and Womersley41). The Siri–age–sex equation(Reference Siri, Brozeck and Henschel42) was used to convert density to percentage of BF (BF%). Each subjects’ BF% was classified using the criteria proposed by Bray et al.(Reference Bray, Bouchard, James, Bray, Bouchard and James43). In addition, data related to the place of habitual residence, responsibility for shopping and cooking were recorded using the questionnaires developed by Bennassar(Reference Bennassar44) and St. Jeor(Reference Scott and Sachiko45). Responsibility for shopping and cooking was multiple-answers questions.
Diet intake assessment
Diet was assessed using a face-to-face interview that includes: two meal pattern questionnaires based on validated forms(Reference Bennassar44,Reference Scott and Sachiko45) , and a short FFQ that is a modified and validated version(Reference Telleria-Aramburu, Alegria-Lertxundi and Arroyo-Izaga46). The first of them was a participant-identified approach(Reference Leech, Worsley and Timperio47) used to define eating occasions (EO), in which the participants were asked to describe how they usually ate on an ‘ordinary’ day, specifying time for meal, meal duration and choosing the type of meal best corresponding to their own meal. Two different meal types were defined: main meal and light meal/snack meal. The aim was to identify all EO, even those consisting only of a drink. In the instructions, subjects were reminded to include snacks and other light meals and that they could have several main meals during a day. All types of meals were referred to as ‘meals’ in the text. From data on time for meal and meal duration, number of EO per day and spacing of EO (mean time between meals, i.e. breakfast, lunch and dinner) were calculated. This questionnaire also included information on the presence of others at a meal (eat alone v. with others or depending on the occasion).
The second meal pattern questionnaire was a time-of-day approach(Reference Leech, Worsley and Timperio47) and was used to describe frequency of EO (less than weekly, 1–2 times/week, 3–4 times/week, 5–6 times/week, every day). This approach defines meals according to the time-of-day in which food was consumed. Explicitly, a ‘meal’ has been defined as the largest EO (breakfast, lunch and dinner), with smaller EO considered as light meals/snack meals (mid-morning, afternoon, after dinner and mid-night snacks).
A meal pattern score, incorporating the eight variables studied in this section (number of EO per day; interval between meals; breakfast skipping; eating breakfast, lunch and dinner alone v. with others; breakfast duration; and lunch/dinner duration) and assigning a score (from 0 to 1) to each one, was constructed. We used as a model two scores designed previously by other authors(Reference Romaguera, Gracia-Lavedan and Molinuevo48,Reference Sotos-Prieto, Bhupathiraju and Falcon49) . Each variable of the present score was compared with the established recommendations to prevent overweight/obesity, when these were available, or on current evidence in the general population. Detailed information on the operationalisation of our score can be found in Table 1. The total meal pattern score ranged from 0 to 8, with higher scores indicating greater concordance with the recommendations.
Table 1. Diet and lifestyle score construction

EO, eating occasions; HEI-2010, Healthy Eating Index-2010; MDS, MedDietScore; No., number; PA, physical activity.
* In the case of participants who skipped breakfast > 4 d/week, the score assigned to have breakfast alone or with others and to length of breakfast was 0.
† We used the cut-off of ≤3·3 h/d of sitting time on the basis of studies suggesting that longer duration incurred a greater risk of CVD.
In the short FFQ, the students were first asked whether they consume each specific item. If the participants affirmed consumption, they were asked about the usual frequency of consumption (daily, weekly or monthly) of one standard serving(Reference Carbajal, Sánchez-Muniz, García-Arias and García- Fernández63). The daily intakes of each food item were determined based on the average consumption frequency and the amount of each food item consumed. For items that included several foods, each food’s contribution was estimated with weighting coefficients obtained from the usual consumption data(64). Additionally, an open question was added with the objective of identifying foods that were not included in the short FFQ, such as soya products. When a food was written in the open questionnaire, we also asked how often they consumed it.
All food items that were consumed were entered into DIAL for Windows(Reference Ortega, López-Sobaler and Andrés65), a type of dietary assessment software, to estimate energy and nutrient intake (these results are part of an article under revision; unpublished results). From the data obtained on food groups, energy and nutrient intake, adherence to food-based dietary guidelines was evaluated. For this end, we used two diet quality indices: the Healthy Eating Index-2010 (HEI-2010)(Reference Guenther, Casavale and Reedy56) and the MedDietScore (MDS)(Reference Panagiotakos, Milias and Pitsavos66). The former index is a measure of diet quality used to assess how well a set of food items aligns with key recommendations of the Dietary Guidelines for Americans. Although specific to US dietary guidelines, the HEI-2010 has been widely used in European populations and even in studies involving European university students(Reference García-Meseguer, Cervera and Vico67) which allows us to compare results. We used HEI-2010 instead of HEI-2015 for many reasons. First, HEI-2010 has been applied previously with UPV/EHU students and with other university student populations(Reference García-Meseguer, Cervera and Vico67), which allows us to establish comparisons with these data sets. A second reason is that HEI-2010 includes assessment of alcohol consumption (within the ‘empty calories’ component), while HEI-2015 does not include it. The HEI-2010 consists of twelve components, including nine on adequacy and three on moderation that are scored per 1000 kcal. The theoretical range of the HEI-2010 is from 0 to 100. We scored data with the simple HEI-scoring algorithm method.
The other quality index used, the MDS is an index that estimates the level of adherence to the MD pattern and is associated with biomarkers of CVD risk(Reference Panagiotakos, Pitsavos and Stefanadis57). This score has eleven main components; each was scored separately but not by energy. For the consumption of foods considered to deviate from this dietary pattern, the scores were assigned on a reverse scale (scores 5 to 0). The total score (sum) ranges between 0 and 55. Higher values of this score indicate greater adherence to the MD pattern. These two diet quality indices were incorporated into the meal pattern score to construct the diet total score (Table 1). The weight of each index was estimated taking into account the number of items within each one (HEI-2010 consists of twelve components and MDS of eleven).
Lifestyle (different from diet)
The PA (type of activity, d/week and time/d) and sedentary behaviours (time spent sitting) related data were registered through the International Physical Activity Questionnaire in its short-form version(58). Results of PA were analysed according to the International Physical Activity Questionnaire scoring protocol(58) that establishes three categories (low, moderate and high).
The self-reported sleep duration per night was ascertained by the following question: ‘On an average school night, how many hours of sleep do you get?’(68). In addition, information about alcohol consumption was registered using the questions from the National Health Survey(68). Moreover, the short FFQ included specific questions about the frequency of intake of alcoholic beverages: beer, wine, cider, aperitif with alcohol and liquor. The alcohol consumption data are expressed as grams of alcohol and standard drink units (SDU) per week(69). In the present study, we used the SDU defined for Spain (one SDU is equivalent to 10 g of alcohol). With this information, the participants were categorised into abstemious, moderate consumption and high consumption categories according to the Spanish Society of Community Nutrition criteria, which considers moderate drinking up to one SDU per d for women and up to two SDU per d for men(61).
A lifestyle score, incorporating the five analysed variables in this section, was constructed (Table 1). Established risk factors of obesity (PA level and time spent sitting) were given more points on the score than emerging risk factors(Reference Kim70,Reference Traversy and Chaput71) . We have not included smoking habit in the lifestyle score because the relationship between smoking and obesity is confusing(Reference Healton, Vallone and McCausland72,Reference Patel, Hargreaves and Liu73) . The total score ranged from 0 to 3, with higher scores indicating greater concordance with the recommendations. Finally, a healthy lifestyle score derived from the diet total score and the lifestyle score was estimated. This last score ranged from 0 to 34 points, with the higher score reflecting adherence to lifestyles recommendations.
Statistical analysis
The data were analysed using SPSS for Windows (version 22.0, SPSS Inc.) and are reported as the mean values, standard deviation (sd) and frequencies. All analyses were conducted separately for male and female students because of their differences in lifestyle behaviours(Reference Olfert, Barr and Charlier19). All the results were weighted to ensure representativeness of the UPV/EHU university students’ population using weighting coefficients provided by the list of students enrolled in 2012/2013(74). The symmetry of the distribution of the continuous variables was determined by a Kolmogorov–Smirnov–Lilliefors test. Differences in variables were assessed with the Kruskal–Wallis H-test and associations between scores and indices with Spearman’s correlations (the variables were not normally distributed, even after logarithmic transformation, due to data being weighted and the large sampling size; thus, small deviations rendered the variables not normally distributed). Categorical variables were analysed using χ 2 tests.
Finally, to analyse the possible associations between the variables of the healthy lifestyle score and risk of excess adiposity, binary logistic regressions adjusted to age and daily energy intake were performed. The 95 % CI were calculated and Wald’s test used for comparison of the OR. All the variables of the healthy lifestyle score were dichotomised considering, on the one hand, the healthiest category and, on the other, the intermediate and the least healthy; except for ‘sitting time’ variable in which the categories were: adequate + barely adequate v. inadequate, because the frequency for the healthiest category was very low. All tests were two-tailed, and P-values <0·05 were considered statistically significant.
Results
Regarding to BF classification results, 14·4 % of the target population was classified as excessive, the prevalence of excessive BF being higher in men (16·1 %) than in women (13·3 %) (P < 0·001). On the other hand, the percentage of students who resided with parents was 53·2 %. Concerning the person responsible for food shopping and cooking, more than half of the students indicated that their parents were responsible people, 56 % for food shopping and 53·3 % for food cooking. There were sex differences in the last three analysed variables, being higher the percentage of women who lived with parents than in men (61·5 % v. 47·5 %, P < 0·001). However, women were more likely than men to be the person responsible for buying and preparing food (36·6 % v. 34·0 % for food shopping; and 38·3 % v. 35·8 % for food cooking; P < 0·001 in both variables).
Diet and lifestyle (different from diet) characteristics by sex are shown in online Supplementary Table S1. Compliance with dietary recommendations in the studied population, according to sex, is described in Table 2. Between 40·3 and 50·1 % of the participants had an adequate number of EO daily, interval between meals, time spent on breakfast and/or lunch/dinner. Sex differences were found for all these variables analysed. The percentage of men who had an adequate number of EO daily, interval between meals and never skipped breakfast was higher than in women, whereas women showed a significantly higher adequacy of time spent on breakfast and on lunch/dinner compared with men (P < 0·001).
Table 2. Compliance with dietary recommendations by sex in the population under study: students of the University of the Basque Country (UPV/EHU), EHU12/24 study
(Mean values and standard deviations, percentages)
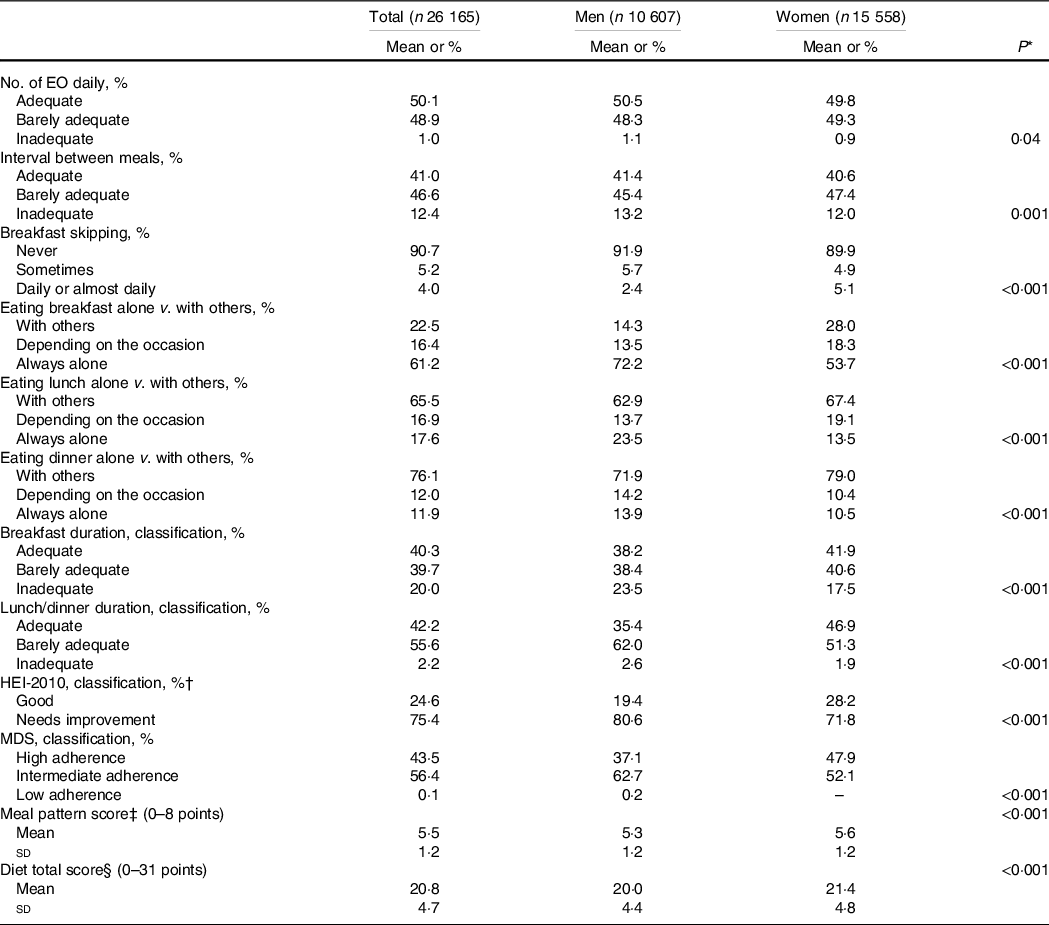
EO, eating occasions; No., number; HEI-2010, Healthy Eating Index; MDS, MedDietScore.
* Sex differences.
† None of the participants was classified as poor (<51 points).
‡ Meal pattern score included the following variables: no. of EO daily, interval between meals, breakfast skipping, time spent on breakfast and time spent on meals.
§ Diet total score: meal pattern score + HEI-2010 + MDS.
In addition, there was a significant correlation between the meal pattern score and HEI-2010 (Spearman’ rho, 0·145, P < 0·001 for the total sample; 0·161, P < 0·001 for women; and 0·114, P < 0·001 for men), and between the meal pattern score and MDS (Spearman’ rho, 0·096, P < 0·001 for the total sample; 0·149, P < 0·001 for women; and 0·089, P < 0·001 for men). Along these lines, the average scores for MDS and HEI-2010 were higher in subjects who meet the recommendations for each of the variables of meal pattern score v. those who did not (online Supplementary Table S2). In addition, the average scores for meal pattern and the diet total score were higher in students who did not live with parents than in those who live with them (meal pattern score: ‘living with parents’ 5·4 (1·1), ‘living with others’ 5·5 (1·4), P < 0·001; diet total score; ‘living with parents’ 20·7 (4·8), ‘living with others’ 21·0 (4·7), P < 0·001).
Results of compliance with lifestyle (different from the diet) recommendations in the target population are presented in Table 3. Students were characterised by having a moderate PA level, an inadequate time spent sitting, being moderate drinkers and having an adequate time spent sleeping. The percentage of men who had a high PA level and a moderate consumption of alcohol was higher than women (P < 0·001), and the average lifestyle score was higher in men than women (P < 0·001), whereas women showed a significantly higher adequacy of time spent sleeping compared with men (P < 0·001). Regarding smoking habits, 81·7 % were non-smokers/ex-smokers, the proportion of non-smokers/ex-smokers being higher for men than for women (86·9 v. 78·1 %, P < 0·001).
Table 3. Compliance with lifestyle (different from diet) recommendations by sex in the population under study: students of the University of the Basque Country (UPV/EHU), EHU12/24 study
(Mean values and standard deviations, percentages)
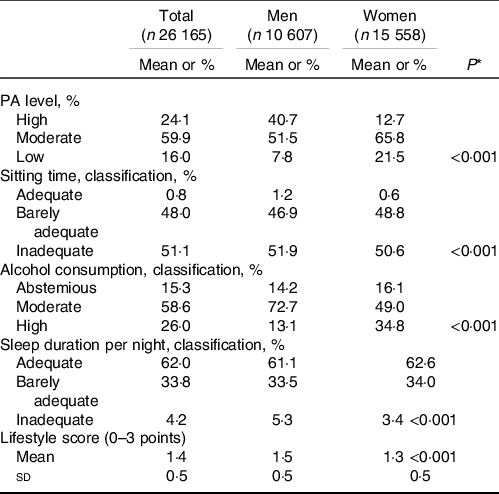
PA, physical activity.
* Sex differences.
Positive and significant correlations were found between the diet total score and the lifestyle score in the total sample (Spearman’ rho = 0·096, P < 0·001), as well as in both sexes (men, rho = 0·209, P < 0·001; and women, rho = 0·105, P < 0·001). The analysis of contingency tables between variables of the diet total score and the lifestyle score showed that students who meet the recommendations related to number of EO daily were more likely to have a high PA level (χ 2 = 413·6, P < 0·001), prolonged sitting times (χ 2 = 82·6, P < 0·001), moderate intakes of alcohol (χ 2 = 301·7, P < 0·001) and be non-smokers (χ 2 = 263·2, P < 0·001). And those who meet the recommendations for the interval between meals and for time spent on breakfast were more likely to have a high PA level (χ 2 = 45·0, P < 0·001 and χ 2 = 43·6, P < 0·001, respectively) and an optimal sleep duration (χ 2 = 593·5, P < 0·001 and χ 2 = 352·4, P < 0·001, respectively).
The mean score of the healthy lifestyle score for the total sample was 22·2 (4·8), being higher in women than in men (22·7 (4·9) v. 21·3 (4·5), P < 0·001). In addition, subjects with non-excess BF had a higher average score on the healthy lifestyle than those with excess BF (22·4 (4·7) v. 21·3 (5·0), P < 0·001). Dividing the population, according to BF% classification, there were differences in favour of those who did not have excessive BF in adequacy of number of EO daily, interval between meals and time spent on breakfast (P < 0·001) (Table 4). On the other hand, people without excess BF had higher PA level, lower consumption of alcohol, a higher adequacy of sleep duration than those with excess BF (P < 0·001) (Table 5). Analysis of lifestyle according to BF by sexes showed similar results, except for PA level, adequacy of recommendations for sitting time and the average lifestyle score among women. In relation to smoking habit, the percentage of men smokers with excessive BF% (17·3 %) was higher than those without excessive BF (12·6 %) (P < 0·001), whereas the opposite happened in women smokers (22·2 % with normal BF% v. 20·1 % with excessive BF%, P = 0·03).
Table 4. Compliance with dietary recommendations according to body fat (BF) classification in the population under study: students of the University of the Basque Country (UPV/EHU), EHU12/24 study
(Mean values and standard deviations, percentages)
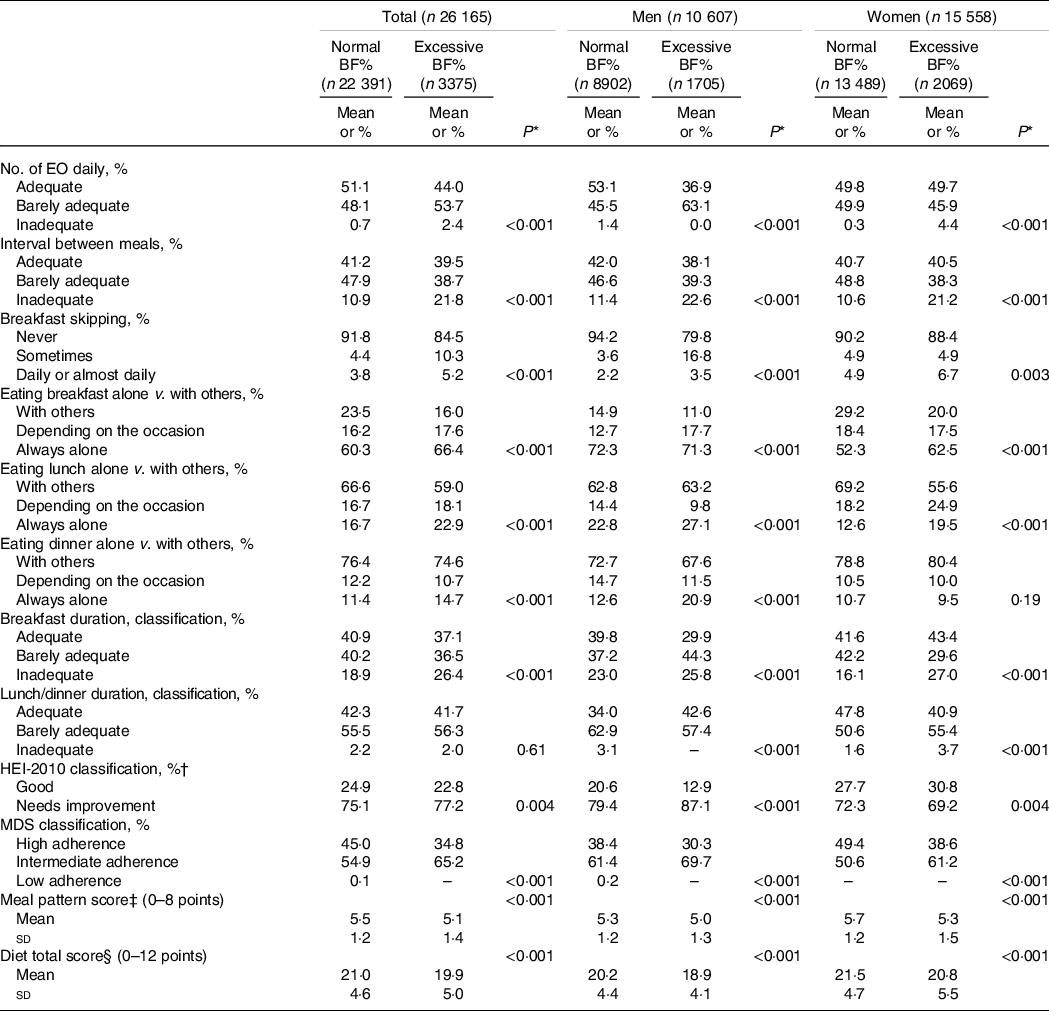
BF, body fat; No., number; EO, eating occasions; HEI-2010, Healthy Eating Index; MDS, MedDietScore.
* Differences between normal BF and excess BF.
† None of the participants was classified as poor (<51 points).
‡ Meal pattern score included the following variables: no. of EO daily, interval between meals, breakfast skipping, time spent on breakfast and time spent on meals.
§ Diet total score: meal pattern score + HEI-2010 + MDS.
Table 5. Compliance with lifestyle recommendations according to body fat (BF) classification in the population under study: students of the University of the Basque Country (UPV/EHU), EHU12/24 study
(Mean values and standard deviations, percentages)
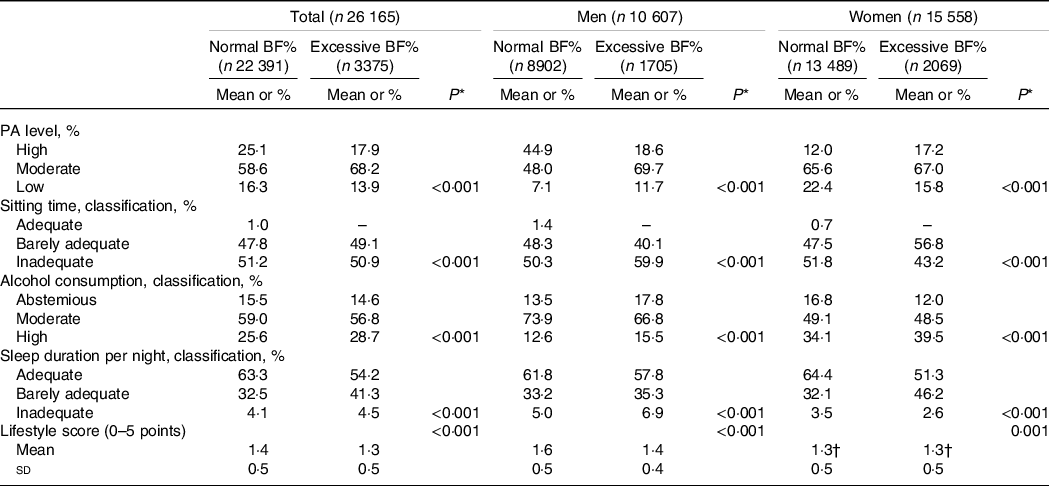
PA, physical activity.
* Differences between normal BF and excess BF.
† Differences were found between women with normal BF% and with excessive BF% (1·29 (0·46); 1·33 (0·47)).
The proportion of students with excessive BF% who did not live with parents was higher than those who live with parents, although the differences were not significant (14·7 % v. 14·2 %, P = 0·28). Among men, the following variables were associated with excess BF (from largest to smallest magnitude of effect in the model 2): a moderate/low PA level (OR: 3·77, P < 0·001), breakfast skipping (OR: 3·66, P < 0·001), a non-adequate breakfast duration (OR: 1·58, P < 0·001) and number of EO (OR: 1·43, P < 0·001), and eating breakfast alone or depending on the occasion (sometimes alone/sometimes with others) (OR: 1·37, P < 0·001) (Table 6). Among women, a low MDS, a moderate/high alcohol consumption (OR: 2·23, P < 0·001), a non-adequate sleep duration (OR: 1·72, P < 0·001), eating breakfast and lunch alone or depending on the occasion were associated with excess BF (variables ordered from largest to smallest magnitude of effect) (OR: 1·47, P < 0·001; OR: 1·42, P < 0·001, respectively) (Table 6).
Table 6. Factors related to diet and lifestyles associated with an increased risk of excess body fat (BF) in the population under study: students of the University of the Basque Country (UPV/EHU), EHU12/24 study
(Odds ratio and 95 % confidence intervals)
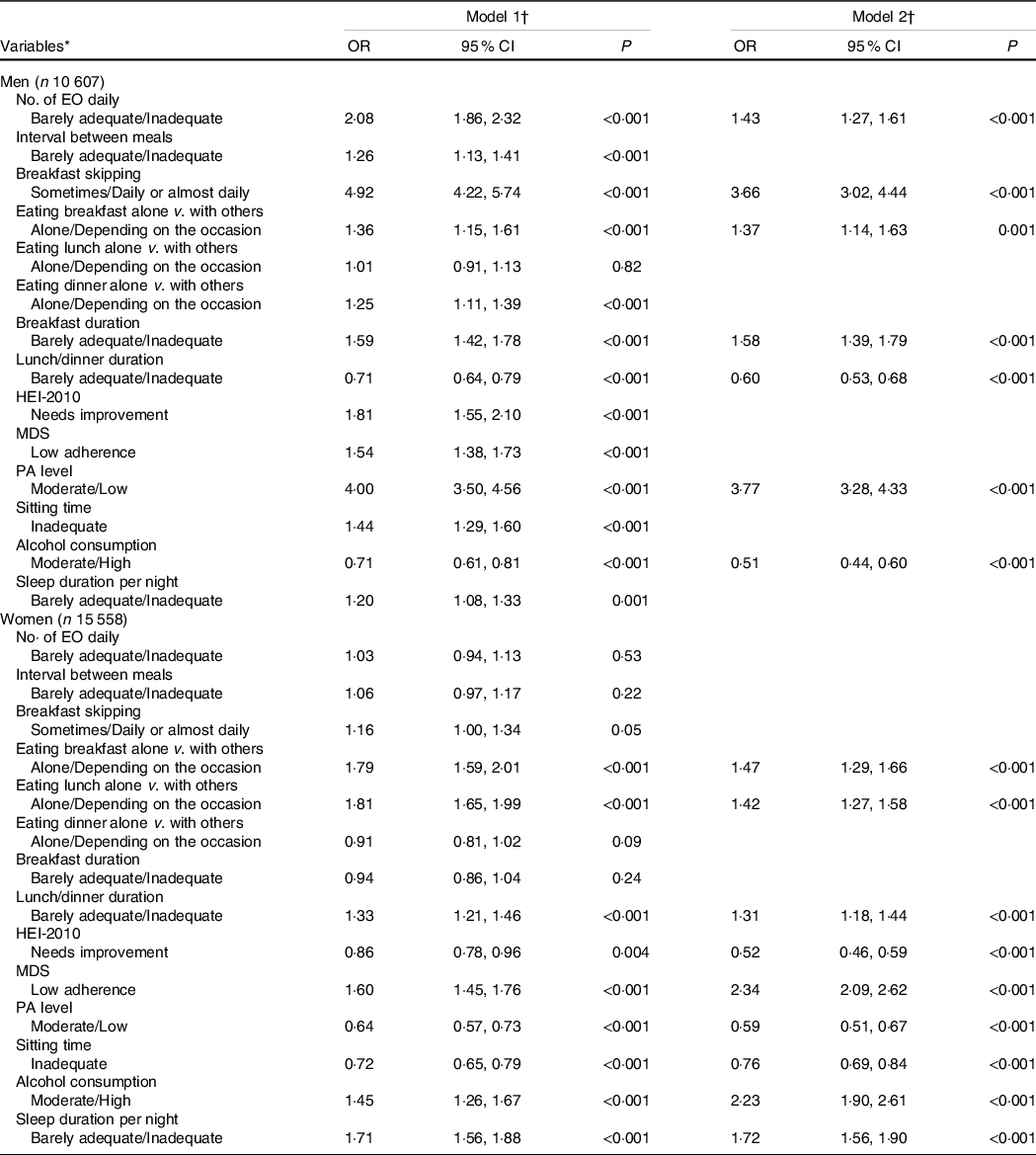
No., number; EO, eating occasions; HEI, Healthy Eating Index; MDS, MedDietScore; PA, physical activity.
* All the variables were dichotomised considering, on the one hand, the healthiest category (that is the reference category in the regression analysis), and, on the other, the intermediate and the least healthy; except for ‘sitting time’ variable in which the categories were: adequate + barely adequate v. inadequate because the frequency for the healthiest category was very low.
† Model 1: effect of each variable adjusted by age and daily energy intake (kcal/d); Model 2: multivariate Wald’s test adjusted by age and energy intake.
Discussion
In this representative sample of university students, the prevalence of overweight/obesity, according to BF%, was 14·4 %, which was lower than in other studies involving university students(Reference Peltzer, Pengpid and Samuels4,Reference Sira and Pawlak7–Reference Cutillas, Herrero and de San Eustaqui12) , but higher than those from Basque Health Survey(75). It should be noted that our study compared with those mentioned formerly used BF% as diagnostic criteria to identify cases with overweight/obesity, and thus, the results between the studies are not directly comparable. In agreement with results of the Italian(Reference Zaccagni, Barbieri and Gualdi-Russo76) and other Spanish university students(Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera37), we registered a higher prevalence of excessive BF in men than in women (P < 0·001).
Concerning the meal patterns, nearly half of the target population had an adequate number of EO daily, spacing of EO and meal duration. The average scores for meal pattern and diet total were higher than the mean value of these scales (5·5 out of 8 and 20·8 out of 31, respectively). Surprisingly, a high meal pattern and the diet total score were obtained in students who did not live with parents than those who do. However, other authors observed that students who live with their parents have healthier eating habits than those living on-campus(Reference Freedman21). Some studies have suggested that different meal patterns are related to overall diet quality, with the most consistent finding being an inverse relationship between breakfast skipping and diet quality(Reference Leech, Worsley and Timperio47). Although little research has looked at the how other variables of meal pattern influence diet quality, the findings in this work showed that all variables of the meal pattern score were associated with diet quality. A possible explanation for these results is that probably a better meal pattern implies a higher food variety and dietary diversity, together with a higher choice of healthy foods than empty foods and therefore, a higher diet quality.
On the other hand, UPV/EHU female students followed more adequate dietary habits than men, taking more time on meals, eating generally with others and having a higher quality of diet. These results are consistent with findings reported in previous studies(Reference Maskarinec, Namatame and Kang22) and probably related to the fact that women were generally more prone than men to make conscious efforts to try to eat a healthy diet(Reference Hearty, McCarthy and Kearney77). On the other hand, male students of the present study were more likely to have an adequate interval between meals, as well as an adequate number of EO/d and too usually eat breakfast, as compared with women. The sex differences in the interval between meals could be related to discrepancies in the distribution of energy intake throughout the day, as other authors have pointed out(Reference Kant and Graubard78).
In relation to lifestyles (different from diet), the population under study was characterised by having a moderate PA level, an excessive time spent sitting, being moderate drinkers and non-smokers/ex-smokers and having an adequate time spent sleeping. UPV/EHU male students had better lifestyles than women with regard to PA, drinking behaviour and smoking. However, female students presented a higher adequacy of sleeping hours compared with men (P < 0·001). The sex difference observed in the PA level was similar to that of other studies(Reference Freedman21,Reference Jaalouk, Matar Boumosleh and Helou79) . Nevertheless, sex differences in the alcohol consumption and smoking habits were not in agreement with those previously published(Reference Freedman21,Reference García-Meseguer, Delicado-Soria and Serrano-Urrea80) . These discrepancies could be due to methodological reasons and to changes in the consumption pattern by sex(Reference Davoren, Demant and Shiely81).
On the other hand, positive and significant correlations were found between the diet total score and the lifestyle score, with the most consistent finding being a direct relationship between an adequate number of EO daily and a high PA level, prolonged sitting times, moderate intakes of alcohol and being non-smokers; and between an adequate interval between meals and breakfast duration and a high PA level and an optimal sleep duration. These results agree with those of other authors(Reference Dodd, Al-Nakeeb and Nevill3,Reference Moreno-Gómez, Romaguera-Bosch and Tauler-Riera37) , who have shown that less healthy food habits are combined with a cluster of less healthy lifestyle factors (e.g. smoking, high alcohol consumption and low PA level).
In addition, subjects with excess BF had a lower average score on the healthy lifestyle scale than those with non-excess BF (P < 0·001). Students with excess BF were more likely to have an inadequate: number of EO daily, interval between meals and breakfast duration; omitting breakfast, eating alone, have a low score for MDS, meal pattern and diet total (P < 0·001). Regarding the number of EO and breakfast duration, our findings agreed with those reported by Shang et al. (Reference Shang, Zou and Guo82), who showed that eating more frequently and slowly independently leads to a lower risk of overweight/obesity.
Moreover, there is strong evidence of an association between breakfast skipping and overweight/obesity, regardless of age, sex, cultural and economic conditions(Reference Ma, Chen and Pu51). With respect to patterns of eating alone in relation to the risk of overweight/obesity, our results agree with the results of Lee(Reference Lee, Cho and Oh83). In this sense, it should be remembered that the association of social relationships with diet quality is well characterised in the literature(Reference Conklin, Forouhi and Surtees28).
Some studies have shown that, in general, people with overweight/obesity are more likely to have unhealthy lifestyles (e.g. insufficiently physically active, sedentary behaviours, binge drinking, smoking and sleeping time)(Reference Peltzer, Pengpid and Samuels4,Reference Whatnall, Patterson and Brookman84) . These results are consistent with the finding of our work, in which students with excess BF had a low-moderate PA level, a moderate-high consumption of alcohol, a higher sitting time and a lower time spent sleeping than those with a normal BF% (P < 0·001). In this study, excess BF has associated with different variables of the healthy lifestyle score in men than women. Among men, a moderate/low PA level, breakfast skipping, a non-adequate breakfast duration and number of EO and eating breakfast alone or depending on the occasion; and among women, a low MDS, a moderate/high alcohol consumption, a non-adequate sleep duration, eating breakfast and lunch alone or depending on the occasion were associated with excess BF. The largest effects (magnitudes of ORs) were found for the variables breakfast skipping and PA level in men, and for adherence to the Mediterranean diet in women.
In general, these sex differences observed here could be due to the fact that women are more likely to find healthy eating more important(Reference Holmbäck, Ericson and Gullberg85), and therefore, they followed more adequate dietary habits than men, eating a greater number of EO daily, skipping fewer breakfasts, taking more time on those meals, and they had a better diet quality, as other authors have highlighted(Reference Maskarinec, Namatame and Kang22). With respect to other lifestyles such as PA, probably cultural practices and childhood habits can be associated with a higher PA level in men than women(Reference Trost, Pate and Sallis86).
Contrary to what one might expect, UPV/EHU men students with excess BF were more likely to have an adequate lunch/dinner duration and to be abstemious and women students with excess BF were more likely to have an adequate sitting time, a high HEI-2010 and a high PA level. These results could be related to adoption of healthy behaviours for weight loss (e.g. eating less or different food, or exercising to lose weight)(Reference Haynes, Kersbergen and Sutin87). Contradictory results were obtained in women for the two diet quality indices estimated, this result could be related to discrepancies in constructs and scoring criteria of diet quality indices used.
The findings of the study should be considered within the context of its limitations. First, recall bias inherent in a convenience sample cannot be ruled out. The decision to participate or not may have been influenced by several factors, including social, educational and health conditions, which may again correlate with outcome risk factors. Second, self-reports of the behaviours may be subject to social desirability bias; thus, the findings may be under or overestimated. Despite that, previous validation studies indicate that the self-reported information, for example, those related to diet, is reported with sufficient accuracy for use in epidemiology analysis(Reference Vereecken, Covents and Sichert-Hellert88). It should be noted that we used previously well-proven or validated questionnaires. Third, the study was based on a large survey that included a face-to-face interview and anthropometric measurements; thus, the considerable length of each assessment may have influenced answers and response rate. To avoid this, the majority of assessments were conducted over 2 d to ensure adequate concentration while answering the questions and to promote the participation. Finally, fourth, the design itself was cross-sectional so causal conclusions cannot be drawn from the behaviour factors selected. In future research, a cohort of students will be followed to assess what effect the university environment has on their health behaviours.
The main strength of this work compared with other studies(Reference Bayyari, Henry and Jones89) is that we used the %BF instead of BMI as a diagnostic criterion for overweight/obesity, in order to avoid both false positives and negatives. In addition, the set of protocolised measurements used in this study generated a large amount of data regarding behavioural determinants of overweight/obesity and interrelationships among them, in a community of university students.
Conclusions
The results of this study suggest that certain unhealthy lifestyle behaviours coexist, interact and increase the risk of overweight/obesity in this population. The sex-specific differences in risk factors of excess adiposity have important implications for interventions for primary prevention of obesity within this environment. Further studies are needed to confirm the complex interconnection between underlying factors of overweight/obesity.
Acknowledgements
The authors also thank the collaboration of the participants and of the students pursuing bachelor’s and master’s degree who collaborated by performing their internships in the context of this project and contributed to the data curation.
This work was supported by grants from the UPV/EHU (EHU12/24), the Vice Rector for Innovation, Social Outreach and Cultural Activities of the UPV/EHU, funding by the contract-programme formalised with the Basque Government (code of the Campus Bizia Lab project: 17ARRO, 18ARRO and 19ARRO), the Vice Rector for Students and Employability of the UPV/EHU and Basque Government (2016); and a pre-doctoral scholarship from the Basque Language Vice-chancellor of the UPV/EHU. Neither the UPV/EHU nor the Basque Government played a role in the design, analysis or writing of this article.
The author contributions are as follows: N. T.-A. and M. A.-I. contributed to the conception and design of the research, acquired and analysed the data, interpreted the results and finally drafted the manuscript. Both authors read and approved the final manuscript.
There are no conflicts of interest.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114521001483









 Open access
Open access