


Introduction
Anorexia nervosa (AN) is a severe mental illness whose sufferers present poor quality of life, relevant psychological and physical sequelae [Reference Treasure, Zipfel, Micali, Wade, Stice and Claudino1], and high mortality [Reference Arcelus, Mitchell, Wales and Nielsen2]. Body image disturbances are a hallmark of this disorder [3] and the overevaluation of shape and weight and their control has been proposed as the “core psychopathology” of clinical eating disorders [Reference Fairburn, Cooper and Shafran4]. Mirroring other fields of psychiatry, also in AN, body image has been conceptualized as a multifaceted construct in which affective, cognitive, and behavioral components coexist [Reference Marzola, Cuzzolaro and Abbate-Daga5]. Relatedly, body shape is a valuable way to effectively capture body image concerns in keeping with Cash’s definition [Reference Cash6] of (dis)satisfaction and salience dimensions in body-related concerns. Different standpoints have been adopted to the body shape examination in AN. For example, neuroimaging studies showed alterations of the parietal cortex in AN sufferers [Reference Vocks, Busch, Grönemeyer, Schulte, Herpertz and Suchan7] while other lines of research highlighted the role of negative emotions in eliciting the experience of a distorted body shape in AN [Reference Espeset, Gulliksen, Nordbø, Skårderud and Holte8]. Still, some studies deepened the role of the behavioral component of body shape disturbances [Reference Legenbauer, Martin, Blaschke, Schwenzfeier, Blechert and Schnicker9,Reference Shafran, Fairburn, Robinson and Lask10] while very few investigated its changes after treatment [11–Reference Mountford, Brown, Bamford, Saeidi, Morgan and Lacey13]. Taken together, these findings confirm the relevance of body shape disturbances in AN and their complexity alike.
Also, from a clinical standpoint, the assessment of body shape is multidimensional. In addition to the well-known distressing weight and shape concerns, patients with AN tend to show obsessive and perfectionistic traits [Reference Kaye, Wierenga, Bailer, Simmons and Bischoff-Grethe14] that may be involved in the drive to constantly check their body, aiming to find respite from the fear of being “fat.” In fact, body checking (e.g., measuring the circumference of arms, thighs, etc.) can be frequent in AN [Reference Shafran, Fairburn, Robinson and Lask10,Reference Calugi, Grave, Ghisi and Sanavio15]. In contrast, patients tend to avoid to measure their body (e.g., not looking themselves in the mirror [Reference Bamford, Attoe, Mountford, Morgan and Sly16]), because this behavior could represent a painful trigger of body-related anxiety and dysphoria. A novel line of research showed these components as differentiating phenotypes of eating disorders [Reference Legenbauer, Martin, Blaschke, Schwenzfeier, Blechert and Schnicker9] but only few data are currently available.
Very few data exist on body shape perceptions in inpatients with severe AN, possibly because the primary aim of hospitalization is usually to minimize patients’ life-threatening conditions rather than working on body-related concerns [Reference Marzola, Delsedime, Scipioni, Fassino and Murray17,18]. Notwithstanding, dissatisfaction with one’s own body is a well-known element influencing prognosis of AN treatment [Reference Schlegl, Diedrich, Neumayr, Fumi, Naab and Voderholzer19] so it could be of clinical relevance to take it into account also in the hospital setting. Also, it could be interesting to analyze the body shape scenario of patients admitted through an emergency hospitalization, as a proxy for severe AN condition.
In fact, the literature poorly measured the trajectory of body shape concerns during hospitalization and some data are available only for those hospital interventions, which are focused on cognitive–behavioral therapy [11–Reference Mountford, Brown, Bamford, Saeidi, Morgan and Lacey13]. Also, in this light, it could be noteworthy to measure the changes in body perception during hospitalization when a multimodal intervention (e.g., weight restoration, pharmacotherapy, individual psychodynamic psychotherapy, psycho-education) is usually delivered to patients. Moreover, some data rely on mixed samples or on patients with mild AN (e.g., Body Mass Index [BMI] over 17.5) [Reference Morgan, Lazarova, Schelhase and Saeidi12,Reference Gailledrat, Rousselet, Venisse, Lambert, Rocher and Remaud20]; still, the body checking versus body avoidance components of body shape have been rarely measured in inpatients. Lastly, from a clinical standpoint, the analysis of inpatients’ changes in body shape disturbances during hospitalization is also needed. In fact, earlier literature on inpatients showed that body-oriented therapy (including bodily expression and relaxation therapy) was effective at reducing body shape concerns in inpatients with EDs, with maintenance of such results at the 1-year follow-up assessment [Reference Danielsen, Rø and Bjørnelv21].
Therefore, grounded on every-day clinical practice and in order to bridge these gaps in the literature, with this study we aimed: (a) to ascertain as to whether hospitalization following emergency admission could effectively reduce body shape difficulties in patients with severe AN; (b) to multidimensionally consider body shape concerns, investigating not only body shape concerns but also body avoidance and body checking; (c) to investigate as to whether diagnostic subtypes differ in body shape both at baseline and after hospitalization; and (d) to ascertain the potential impact of body-related concerns (e.g., body shape, avoidance, and checking difficulties) on clinical improvement upon discharge. We expected to find an improvement in body shape concerns after hospitalization in both body avoidance and body checking; also, we hypothesized to find differences between subtypes of AN in the improvement of body-related dimensions grounded on the “real world” observation that those with a binge-purging subtype tend to show greater clinical severity [Reference Brown, Cusack, Anderson, Trim, Nakamura and Trunko22]. Finally, we raised the hypothesis that more severe body shape concerns could impact on inpatients’ clinical trajectory during hospitalization.
Materials and methods
Participants
One hundred and fifty-five women hospitalized at the Eating Disorders Center of the University of Turin, Psychiatry ward of the “Città della Salute e della Scienza” hospital of Turin, Italy, were consecutively enrolled from December 2016 to October 2018. Inclusion criteria were: (a) diagnosis of AN (both subtypes) as assessed with the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [Reference First23] by an experienced psychiatrist; (b) female gender; (c) age ranging from 16 to 50; and (d) no psychotic-spectrum disorders. However, 14 patients did not complete all assessments and 2 refused to provide their written informed consent. Finally, 139 inpatients with AN were included in this study with no dropouts. This study was approved by the Ethical Committee of the Department of Neuroscience of the University of Turin, Italy. All patients were voluntarily admitted to the hospitalization program and provided written informed consent for this study.
Treatment
All patients were voluntarily admitted, although through the emergency room in a very acute phase. Patients were provided with individualized treatment plans [18] aimed to engage them as effectively as possible in treatment. They were offered an integrated and multidisciplinary intervention, including psychiatrists, clinical psychologists, nurses, dietitians, and internal medicine physicians. Blood tests and electrocardiogram were strictly monitored according to individual needs. The main goal was the normalization of eating patterns and the improvement of motivation to undergo the next steps of treatment. Parenteral and enteral nutrition was provided when required by clinical condition. Five structured meals were offered (breakfast, half‐morning snack, lunch, mid‐afternoon snack, and dinner) under dietitian’s supervision. Patients received psychiatric visits in addition to daily individual motivational and supportive psychodynamic sessions and weekly psycho-educational groups. No body-focused formal groups with mirror exposure were provided because body shape interventions available in the literature were not deemed appropriate for patients with extreme AN (i.e., BMI < 15) and hospitalized because of an emergency condition. In fact, when patients are highly emaciated contraindications for such an intervention exist [Reference Morgan, Lazarova, Schelhase and Saeidi12,Reference Mountford, Brown, Bamford, Saeidi, Morgan and Lacey13]. Mirror exposure has been introduced by Key et al. [Reference Key, George, Beattie, Stammers, Lacey and Waller24] as a sensitization and habituation technique subsequently incorporated in treatments with a cognitive–behavioral framework [Reference Vocks, Wächter, Wucherer and Kosfelder25]. It can be imaginal or in vivo and is usually delivered in a group format; patients are asked to look at themselves in a mirror and to work in treatment on all the possible negative cognitions and emotions triggered by their perceived image.
Materials
Clinical characteristics were measured upon hospital admission (T0) and discharge (e.g., end of treatment [EOT]). A trained nurse measured height and weight at both time points in order to calculate BMI.
All participants were asked to complete the following assessments at T0 and EOT:
1. Eating Disorder Examination Questionnaire (EDE‐Q; [26–28]): the Italian version of a 28‐item self‐report questionnaire that provides measures of clinical characteristics of the eating disorder in a total score and four subscales: restraint, eating concern, shape concern, and weight concern. Patients with eating disorders score significantly higher on the global EDE-Q and subscales than healthy controls. Internal consistency (Cronbach’s α = 0.79 for the global EDE-Q and subscale scores) and test–retest reliability (r = 0.80) are strong [Reference Calugi, Milanese, Sartirana, El Ghoch, Sartori and Geccherle28].
2. Body Shape Questionnaire (BSQ; [Reference Cooper, Taylor, Cooper and Fairbum29]): a 34-item self-report questionnaire evaluating body image and body dissatisfaction. Using a six-degree scale, participants have to respond to items referring to how they have felt about their body shape in the last weeks with higher scores denoting greater levels of body dissatisfaction. The Cronbach’s α values are between 0.82 and 0.89 and test–retest reliability has been evaluated as good (r = 0.97) [Reference Franko, Jenkins, Roehrig, Luce, Crowther and Rodgers30].
3. Beck Depression Inventory (BDI; [Reference Beck and Ward31]): the validated Italian version [Reference Baggio, Ferrari, Partinico and Vidotto32]) of a 13-item self-report questionnaire used to measure self-report depressive symptoms. Scores from 0 to 4 indicate minimal depressive symptoms, scores of 5–7 indicate mild depression, scores of 8–15 indicate moderate depression, and scores of 16–39 indicate severe depression. BDI internal consistency has a mean coefficient α of 0.86 for psychiatric patients and 0.81 for nonpsychiatric individuals. Test–retest reliability ranged from 0.73 to 0.96 [Reference Wang and Gorenstein33].
4. State Trait Anxiety Inventory (STAI; [Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs34]: the validated Italian version [Reference Lazzari and Pancheri35] of a 20-item instrument to self-report state anxiety, a temporary condition experienced in specific situations, and trait anxiety, a general tendency to perceive situations as threatening. All items are rated on a four-point scale. Total scores for each section range from 20 to 80, with higher scores meaning greater levels of anxiety. Internal consistency (Cronbach’s α) varies from 0.86 to 0.95; test–retest reliability coefficients from 0.65 to 0.75 over a 2-month interval [Reference Spielberger, Gorsuch, Lushene, Vagg and Jacobs34].
5. Body Checking Questionnaire (BCQ; [Reference Reas, Whisenhunt, Netemeyer and Williamson36]): a validated Italian version of the BCQ was used [Reference Calugi, Grave, Ghisi and Sanavio15]. The BCQ is 23 items test that evaluate body checking behaviors including question about measuring, controlling or watching one’s body, or seeking feedback from others. Higher scores indicate higher frequency of checking (total scores range from 23 to 115). The test–retest reliability has been described as high (r = 5.90) with good internal consistency (Cronbach’s α = 0.66–0.92) [Reference Calugi, Grave, Ghisi and Sanavio15,Reference Bamford, Attoe, Mountford, Morgan and Sly16,Reference Reas, Whisenhunt, Netemeyer and Williamson36].
6. Body Image Avoidance Questionnaire (BIAQ; [Reference Rosen, Srebnik, Saltzberg and Wendt37]): the Italian version of BIAQ [Reference Riva and Molinari38] has been used. BIAQ is a 19-item self-report test evaluating the avoidance of body image-related experiences, which may increase dissatisfaction or distress. It evaluates four areas: clothing (disguising or covering up the body), social activities (avoidance of eating in public or displaying one’s figure), restraint (i.e., diet), and grooming/weighing (checking behaviors and weighing). All items are scored on a 6-point scale according to the frequency of engagement in the behavior, from never (0) to always (5) with higher scores indicating higher avoidance. Internal consistency reliability (Cronbach’s α = 0.64–0.89) and test–retest reliability (r = 0.64–0.87) vary across studies [38–Reference Maïano, Morin, Monthuy-Blanc and Garbarino41].
Statistical analysis
The SPSS 24.0 statistical software package (IBM SPSS Statistics for Windows, version 24.0; IBM Corp., Armonk, NY) has been used for data analysis. Student’s t test for independent samples has been used to evaluate the differences between R-AN and BP-AN groups at hospital admission. A paired sample t test has been then run to analyze patients’ changes between baseline and EOT. Cohen’s d effect sizes [Reference Cohen42] were calculated as well; differences are defined as small (≥0.2 and <0.5), medium (≥0.5 and <0.8), and large (≥0.8).
A repeated measures ANOVA has been performed to investigate any differences between R-AN and BP-AN over time, between hospital admission and discharge. The effect size was measured with the eta-squared (η 2). According to Cohen’s work [Reference Cohen42], the effect size can be assessed as small η 2 = 0.01–0.06; moderate η 2 = 0.06–0.14; or large η 2 > 0.14.
Pearson’s correlations have been used to analyze the correlations between changes in body shape concern and clinical variables and eating and general psychopathology as measured upon admission and discharge.
A formal staging in AN is lacking [Reference Maguire, le Grange, Surgenor, Marks, Lacey and Touyz43]; so, based on clinical variables, we defined patients with a clinical significant reduction of AN symptomatology as improved if upon discharge they showed: (a) change in BMI ≥ 0.7 (i.e., over the 50°percentile of BMI improvement reported by the whole sample) and (b) EDE-Q total score within 1 SD from norms (i.e., cutoff at 2.5 [Reference Calugi, Milanese, Sartirana, El Ghoch, Sartori and Geccherle28]).
Multiple logistic regression (namely controlling for age, duration of illness, BMI, BDI, STAI-S, STAI-T, and EDE-Q total score at baseline) has been run in order to see as to whether baseline variables of body shape, checking, and avoidance could be associated with clinical improvement at hospital discharge. Body shape scores were considered as independent variables and clinical reduction of AN symptomatology as a dependent variable.
Results
Participants clinical features at baseline
Patients with both subtypes of AN were included in this study so the sample was composed by 139 inpatients. Participants were subgrouped as follows: 96 (69.1%) patients were affected by restricting-AN (R-AN) and 43 (30.9%) by binge-purging AN (BP-AN). The vast majority of patients were Caucasian (n = 137). Patients’ mean age was 24.7 ± 9.5 years, mean duration of illness was 7 ± 8.7 years, and mean BMI was 14.2 ± 1.9. The number of previous inpatient treatments was 1.32 ± 2.38 and hospitalization lasted 36.1 ± 17 days. One hundred and twenty patients (87.6%) were on medications, mostly SSRIs or SSRIs coupled with atypical antipsychotics at a low dose (mostly olanzapine or aripiprazole). Enteral nutrition—although delivered for a limited period of time—was required for 46 patients.
Diagnostic subtypes of AN differed in BMI, duration of illness, BSQ, eating psychopathology, and anxiety (Table 1).
Table 1. Baseline differences between inpatients with restricting (R-AN) and binge-purging subtypes of AN (BP-AN)
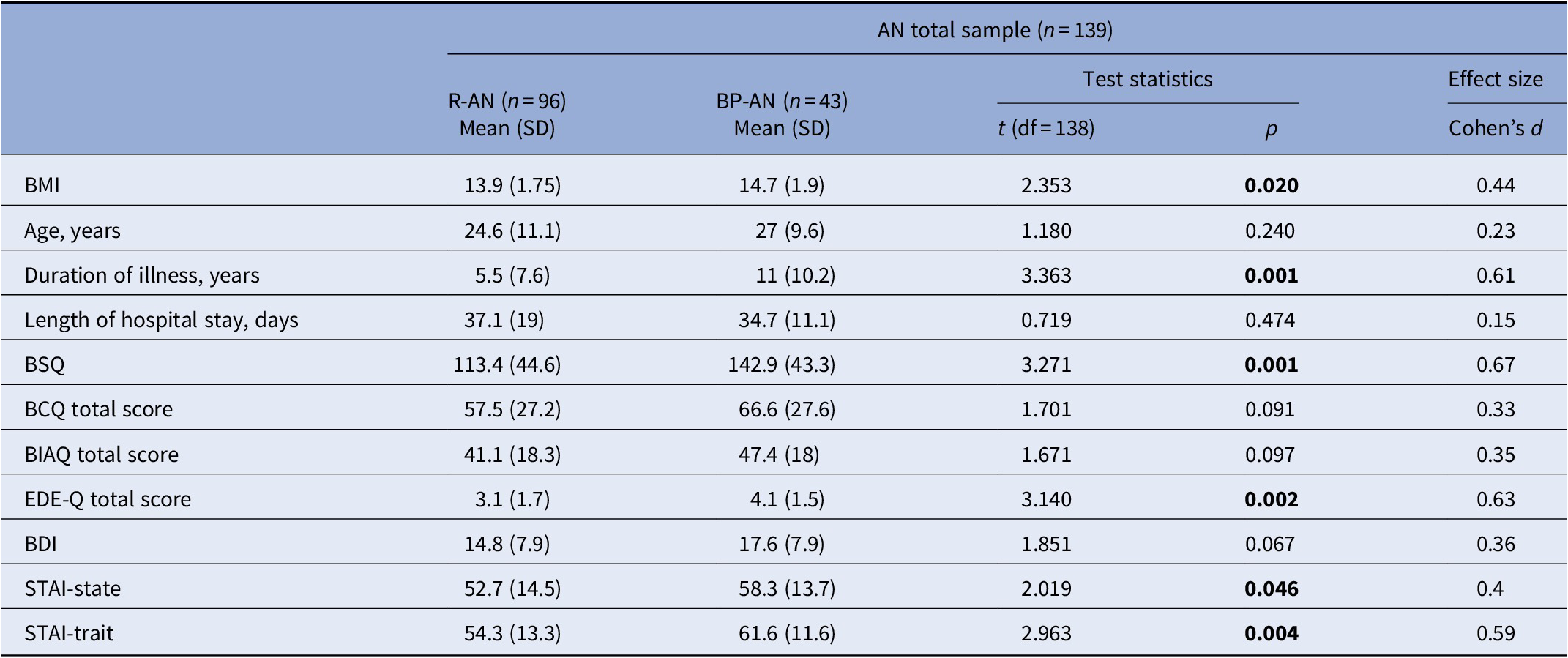
Abbreviations: BCQ, Body Checking Questionnaire; BDI, Beck Depression Inventory; BIAQ, Body Avoidance Questionnaire; BMI, Body Mass Index; BSQ, Body Shape Questionnaire; EDE-Q, Eating Disorders Examination-Questionnaire; STAI, State Trait Anxiety Inventory.
Cohen’s d effect sizes: small (≥0.2 and <0.5), medium (≥0.5 and <0.8), and large (≥0.8).
statistical significance (p < 0.05) has been highlighted in bold.
Outcome of hospitalization
BMI, eating, and general psychopathology
As shown in Table 2, patients showed significantly improved BMI, binge-purging episodes, and eating psychopathology at EOT, as measured by the EDE-Q. Nevertheless, many patients (69.8%) required to be stepped-down to nutritional rehabilitation facilities or to a day treatment intervention. Data on the latter can be found in earlier research from our group [Reference Abbate-Daga, Marzola, Gramaglia, Brustolin, Campisi, De-Bacco, Amianto and Fassino44,Reference Abbate-Daga, Marzola, De-Bacco, Buzzichelli, Brustolin, Campisi, Amianto, Migliaretti and Fassino45]. Also, a significant improvement was found on measures of depression and anxiety.
Table 2. Sample differences between hospital admission (T0) and EOT in BMI, eating and general psychopathology
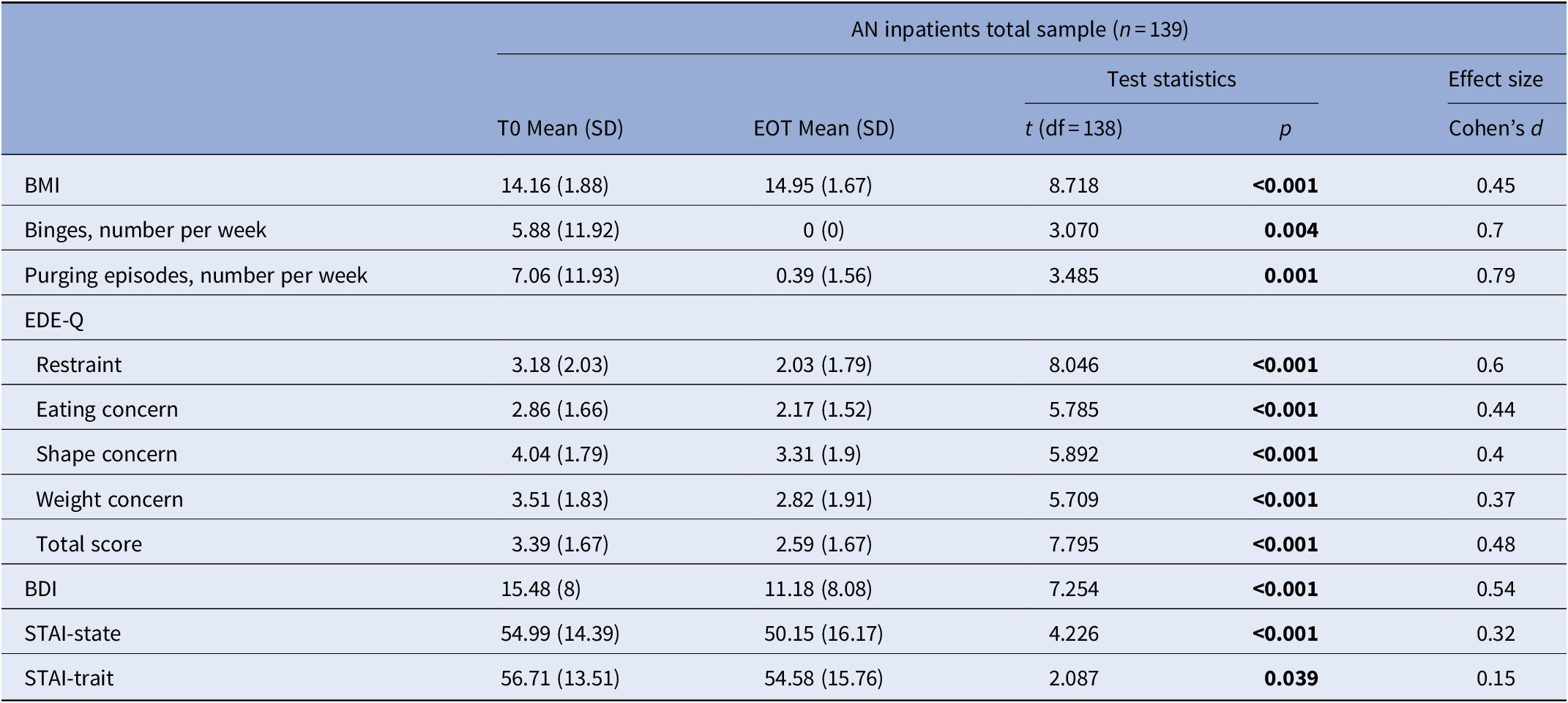
Abbreviations: BDI, Beck Depression Inventory; BMI, Body Mass Index; EDE-Q, Eating Disorders Examination-Questionnaire; EOT, end of treatment; STAI, State Trait Anxiety Inventory.
Cohen’s d effect sizes: small (≥0.2 and <0.5), medium (≥0.5 and <0.8), and large (≥0.8).
statistical significance (p < 0.05) has been highlighted in bold.
According to the aforementioned outcome criteria (see “Methods” section), 97 patients (69.8%) were classified as reporting significant clinical reduction of AN symptoms while 42 did not report such an improvement (30.2%) upon discharge.
Body shape
With regard to body shape, BSQ significantly improved as well as the total score of the BIAQ and the vast majority of its subscales. In contrast, body checking as measured by the BCQ did not significantly improve after hospitalization (Table 3).
Table 3. Sample differences between hospital admission (T0) and EOT in body-related dimensions
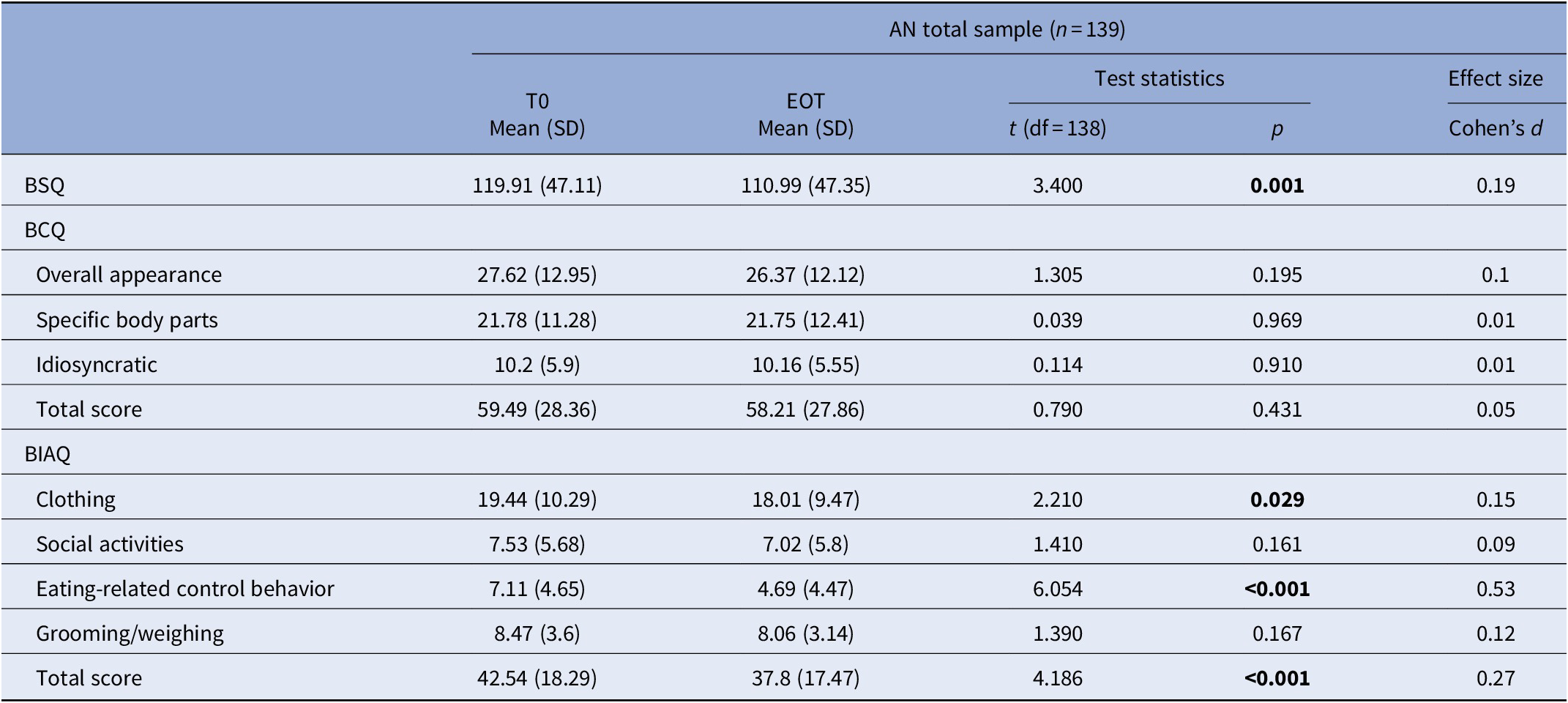
Abbreviations: BCQ, Body Checking Questionnaire; BIAQ, Body Avoidance Questionnaire; BSQ, Body Shape Questionnaire; EOT, end of treatment.
Cohen’s d effect sizes: small (≥0.2 and <0.5), medium (≥0.5 and <0.8), and large (≥0.8).
statistical significance (p < 0.05) has been highlighted in bold.
Those who achieved a meaningful clinical reduction of AN symptoms reported significant lower scores than those who did not report such an improvement on all body shape scales at baseline (BSQ: clinically improved = 82.6 ± 39.9, clinically nonimproved = 137.3 ± 38.7, t (138) = 7.15, p < 0.001; BCQ: clinically improved = 35.9 ± 13.9, clinically nonimproved = 70.1 ± 25.5, t (138) = 7.78, p < 0.001; BIAQ: clinically improved = 29.3 ± 15.1, clinically nonimproved = 48.1 ± 17, t (138) = 5.7, p < 0.001).
Diagnostic subtypes of AN had an impact only on body shape concerns, with BP-AN reporting worse baseline scores and greater improvement than R-AN at EOT (Table 4).
Table 4. Differences between R-AN and BP-AN between hospital admission (T0) and EOT in body-related concerns
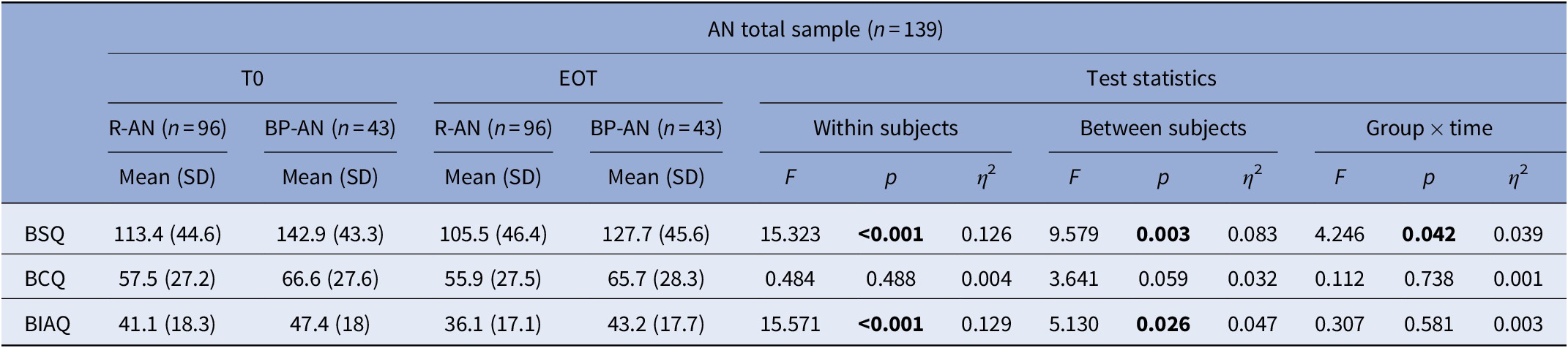
Abbreviations: BCQ, Body Checking Questionnaire; BIAQ, Body Avoidance Questionnaire; BSQ, Body Shape Questionnaire; EOT, end of treatment; η 2, eta squared.
0.01–0.06 = small effect; 0.06–0.14 = moderate effect; >0.14 = large effect.
statistical significance (p < 0.05) has been highlighted in bold.
Associations between body shape variables and clinical outcome
The differences in BSQ and BIAQ reported after hospitalization were found to correlate with changes in eating and general psychopathology. Changes in BCQ correlated with eating psychopathology and state anxiety but not with strait anxiety or depression. Differences in BMI and binge-purging symptomatology did not correlate with any measures of body shape concern (data not shown).
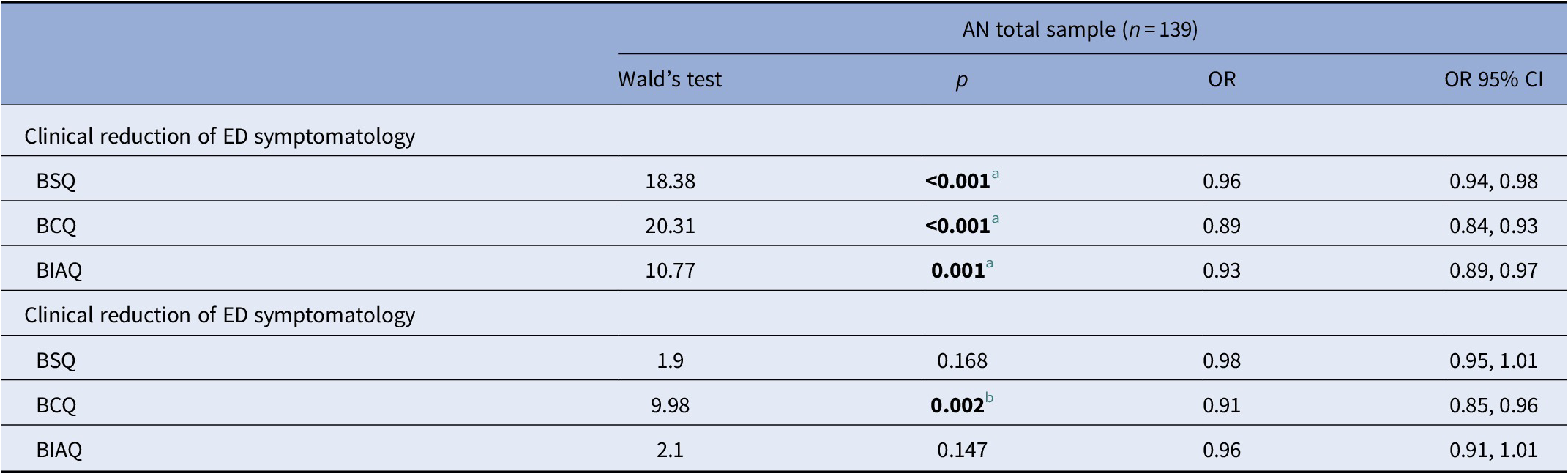
When logistic regression was performed in order to ascertain as to whether body shape, avoidance, and checking were associated with clinical improvement, BSQ, BCQ, and BIAQ resulted as negatively associated with clinical reduction of the AN symptomatology after controlling for age, duration of illness, and BMI, BDI, STAI-S, and STAI-T at baseline (Table 5). In other words, each point of BSQ, BCQ, and BIAQ decreases the odds to achieve clinical reduction of the AN symptomatology. When baseline EDE-Q total score was added to the model, only BCQ remained significant; therefore, the higher the BCQ score, the lower the odds to clinically improve upon discharge (Table 5).
Table 5. Association between baseline body-related variables and clinical outcome
Abbreviations: BCQ, Body Checking Questionnaire; BIAQ, Body Avoidance Questionnaire; BSQ, Body Shape Questionnaire; ED, eating disorder.
a p < 0.05 when controlling for age, duration of illness, BMI, BDI, STAI-S, and STAI-T at baseline.
b p < 0.05 when controlling for age, duration of illness, BMI, BDI, STAI-S, and STAI-T, and EDE-Q total score at baseline.
statistical significance (p < 0.05) has been highlighted in bold.
Discussion
Five main findings emerged from this study. First, inpatients with severe AN, even if hospitalized because a life-threatening condition in an acute phase of their illness, reported improved body shape concerns after treatment. Second, inpatients with severe AN described significant changes in body avoidance (including eating-related control behaviors) but not body checking after hospitalization. Third, diagnostic subtypes reported significanly different (i.e., higher for BP-AN) body shape concern at baseline but comparable levels of body avoidance and checking. Fourth, diagnostic subtypes had an impact on the improvement in body shape, with BP-AN improving more on the BSQ than the R-AN group, but not on body avoidance and checking. Lastly, body shape, avoidance, and checking measured upon admission impacted on clinical outcome even after controlling for age, duration of illness, BMI, depression, and anxiety at baseline. In other words, higher scores on all measures of body shape concern decreased the odds for clinical reduction of AN symptomatology. However, when eating psychopathology (i.e., EDE-Q total score) was added to the model as a confounder, only body checking resulted to be associated with inpatients’ clinical reduction of the AN symptomatology. These are novel findings, since to date body shape concerns have not been deepened in the literature on inpatients with severe AN, mostly with those patients who required an emergency hospitalization.
Per international guidelines [18], hospitalizations for AN are mainly focused on weight restoration and improvement of life-threatening clinical conditions, even more so with patients who are hospitalized because of an emergency. In spite of baseline clinical severity, the inpatient treatment resulted effective in improving not only clinical and eating-related difficulties but also body shape concerns. The latter are of particular interest because they are not so commonly investigated in the acute setting although they represent well-known risk factors for relapse [Reference Danielsen, Rø and Bjørnelv21].
According to our a priori hypothesis, body avoidance improved during hospitalization. This finding was expected because working in treatment on patients’ body is somehow intertwined with refeeding and weight restoration, hallmarks of the inpatient intervention. When hospitalized, patients are engaged in an active work on themselves from multiple standpoints (e.g., nutritional, psychotherapeutic, psycho-educational); as a result, patients reported to be less avoidant regarding their body and looking at themselves. When considering the relevance of avoidance behaviors in AN [Reference Bauer, Schneider, Waldorf, Cordes, Huber and Braks46] and their reciprocal relationships with patients’ inner states [Reference Haynos, Crosby, Engel, Lavender, Wonderlich and Mitchell47], this result is of particular interest for both clinical and research settings and future studies are warranted to confirm these novel data. In the same vein, avoidance is a factor related to response to treatments [Reference Marzola, Panepinto, Delsedime, Amianto, Fassino and Abbate-Daga49] and to duration of illness [Reference Marzola, Panepinto, Delsedime, Amianto, Fassino and Abbate-Daga49]; therefore, the modification of this behavior is particularly useful from a clinical standpoint.
In contrast, inpatients’ body checking scores improved without reaching statistical significance. It is difficult to compare our findings with earlier literature because data on body checking have been scarcely reported on inpatients with severe AN hereinbefore. However, it can be raised the hypothesis that a lack of cognitive–behavioral interventions could be called into question when reading this result also in the light of recent literature [11–13], showing that patients receiving CBT-E [Reference Fairburn50] during hospitalization improved significantly their body checking as well as those patients who received specific body-focused interventions like mirror exposure [Reference Morgan, Lazarova, Schelhase and Saeidi12,Reference Mountford, Brown, Bamford, Saeidi, Morgan and Lacey13].
As a third result, we found R-AN and BP-AN groups differing in body shape but not in body avoidance and checking at baseline, although those with BP-AN reported higher scores than R-AN in both behaviors. This is a novel datum because earlier literature compared different diagnoses rather than diagnostic subtypes [Reference Legenbauer, Martin, Blaschke, Schwenzfeier, Blechert and Schnicker9,Reference Mountford, Haase and Waller51]. However, two debated approaches have been adopted so far in literature to the eventual relevance of body avoidance and checking behaviors with respect to diagnosis. In fact, previous data showed on one hand that different diagnoses of eating disorders differ in body checking [Reference Legenbauer, Martin, Blaschke, Schwenzfeier, Blechert and Schnicker9] but on the other hand it has been found that body checking cognitions and behaviors are best understood not only with regard to diagnostic category but also to symptom presentation [Reference Mountford, Haase and Waller51]. When analyzing this result, it is of note that the BP-AN group showed greater overall severity on several clinical and psychopathological parameters so the difference in BSQ could mirror the overall more marked severity of this diagnostic subtype, consistently with earlier literature [Reference Brown, Cusack, Anderson, Trim, Nakamura and Trunko22]. However, other uncontrolled variables may play a role in generating this difference so future studies are warranted on this topic.
Nevertheless, the diagnostic subtype impacted on body-related changes during hospitalization only with respect to body shape rather than specific behaviors like avoidance and checking. In fact, those with BP-AN improved more their body and shape concerns, as measured by the BSQ, than the R-AN group. At first, it could have been hypothesized a link between the improvement in both body and weight concern and binge-purging symptomatology. Nevertheless, the correlation analysis did not confirm this hypothesis, so only further investigations will eventually confirm this novel finding.
Finally, baseline low scores on the three assessments of body shape concerns were associated with a greater chance to achieve AN symptom reduction upon discharge, independently of age, duration of illness, BMI, depression, and anxiety, as measured upon admission. This is in line with earlier literature in the eating disorders field [Reference Shafran, Fairburn, Robinson and Lask10], on the prognostic value of body shape concerns; notwithstanding, for the first time, this was found to be true also for severe inpatients with AN. Therefore, psychopathology of the body is confirmed to be a key-aspect in maintaining AN [Reference Calugi, El Ghoch and Dalle Grave11,Reference Stanghellini, Castellini, Brogna, Faravelli and Ricca52] and should be considered more in treatment. Still, when eating psychopathology was added to the regression model, only baseline body checking remained significant. This finding generates some hypotheses. First, body dissatisfaction and body avoidance are intertwined with eating psychopathology. This would fit well with our data because shape and avoidance improved while body checking did not: in fact, emergency hospitalizations are primarily aimed to patients’ clinical safety (i.e., minimizing life-threatening AN risks), weight restoration and eating psychopathology. It is therefore suggestive to propose that patients’ improved eating symptomatology and psychopathology could impact on body shape concerns and avoidance and vice versa but not body checking. In fact, the latter would seem a more distinct aspect of eating psychopathology and its nuances. Second, it could be also hypothesized that body checking could be less modifiable and requesting, as stated earlier, more focused and protracted interventions. Taken together, these data highlight the need for addressing body shape concerns in treatment given their impact on patients’ short-run improvement, also in the acute/emergency setting.
Conclusions
In closing, with this work we found that patients with severe AN reported improved body shape concerns after hospital treatment with significant changes in body avoidance but not in body checking. Diagnostic subtypes of AN reported dissimilar body shape scores at baseline and R-AN and BP-AN groups resulted to have an impact on the improvement in body shape concerns, but not on body avoidance and checking. Finally, baseline body shape concerns, mostly body checking, were found to influence inpatients’ clinical improvement.
These findings are relevant because few data are available on inpatients with AN whose severity required an emergency hospitalization although it is well-known that body shape distortions play a role in treatment outcome [Reference Schlegl, Diedrich, Neumayr, Fumi, Naab and Voderholzer19]. Relatedly, data on the behavioral component of body shape are welcome from a clinical perspective because body-related behaviors are not only a key-element of body shape disturbances, but are also involved in the maintenance of the eating disorder [Reference Shafran, Fairburn, Robinson and Lask10,Reference Vossbeck-Elsebusch, Waldorf, Legenbauer, Bauer, Cordes and Vocks53].
Therefore, some interesting clinical implications emerge from this study: in fact, it could be necessary—even at an early stage, like during hospitalizations required by an acute clinical condition—to work in treatment on body shape-related aspects, with a specific focus on body checking, in the light of its impact on clinical outcome. This is even more true when considering that even after controlling for baseline BMI body shape concerns were still found to be associated with inpatients’ clinical reduction of AN symptomatology. Also, differences between diagnostic subtypes should be taken into account.
However, in spite of interesting findings on body shape in acute severe inpatients with AN, some limitations should be acknowledged as well: the sample could be larger and a follow-up after hospital discharge is lacking. Nevertheless, these are “real world” findings that could be a starting point for other studies further deepening the role of hospitalization on body shape disturbances in AN. Also, it should be borne in mind that, given patients’ severity, the main goals of hospitalization were medical stabilization and improving motivation for the next steps of care rather than actively working on body shape concerns (e.g., body checking). Notwithstanding, treatment was effective in improving the core aspect of body shape in AN and future research is warranted to investigate if different clinical approaches could be suitable for inpatients with severe AN.
Conflict of Interest.
The authors declare no conflict of interest.






 Open access
Open access
Comments
No Comments have been published for this article.