


Introduction
Improving tobacco dependence interventions remains a global public health priority (World Health Organization, 2015). The most effective tobacco interventions use a combination of pharmacotherapy and behavioural components to mitigate withdrawal symptoms, boost motivation to quit and facilitate coping skills. High rates of relapse following smokers’ cessation attempts continue to push researchers to test innovative treatment strategies. Recent behavioural intervention trials reveal a resurgent interest in cue exposure strategies (Germeroth et al., Reference Germeroth, Carpenter, Baker, Froeliger, LaRowe and Saladin2017; Xue et al., Reference Xue, Deng, Chen, Zhang, Wu and Huang2017). Interventionists consider cue exposure strategies to facilitate extinction learning during cessation treatment. Extinction is observed as the weakening of one's conditioned response (e.g., smoking urge) over time following repeated exposures to conditioned stimuli, or cues (e.g., smoking paraphernalia) across non-reinforced contexts (situations in which a smoker avoids or is prevented from self-administering nicotine and experiencing drug-related reinforcement).
The theoretical and empirical basis for utilising cue exposure treatment (CET) methods for smoking cessation centres on evidence that (a) cue-elicited reactivity (e.g., elevated urge) relates to relapse risk (e.g., Payne, Smith, Adams, & Diefenbach, Reference Payne, Smith, Adams and Diefenbach2006; Waters et al., Reference Waters, Shiffman, Sayette, Paty, Gwaltney and Balabanis2004) and (b) CET facilitates extinction of cue reactivity (e.g., Collins & Brandon, Reference Collins and Brandon2002; Collins, Nair & Komaroff, Reference Collins, Nair and Komaroff2011). Similarly, Lam et al., Reference Lam, Robinson, Versace, Minnix, Cui and Carter2012 showed that elevated negative affect following smoking cue exposure was associated with greater risk for smoking relapse (Lam et al., Reference Lam, Robinson, Versace, Minnix, Cui and Carter2012). CET trials have also demonstrated the potential utility of cue exposure in promoting longer periods of abstinence compared to standard control or relaxation (Drummond & Glautier, Reference Drummond and Glautier1994; Hartwell et al., Reference Hartwell, Hanlon, Li, Borckardt, Canterberry and Prisciandaro2016; O'Connell, Shiffman, & DeCarlo, Reference O'Connell, Shiffman and DeCarlo2011).
Cue-elicited urges/cravings to smoke continue to be considered key factors related to continued smoking, (Tiffany & Wray, Reference Tiffany and Wray2009) difficulty initiating a quit attempt (Orleans, Rimer, Cristinzio, Keintz, & Fleisher, Reference Orleans, Rimer, Cristinzio, Keintz and Fleisher1991) and difficulty maintaining abstinence after quitting (Bagot, Heishman, & Moolchan, Reference Bagot, Heishman and Moolchan2007; Shiffman, Reference Shiffman1991; Tiffany, Reference Tiffany1990; Wray, Gass, & Tiffany, Reference Wray, Gass and Tiffany2013), even though smoking can occur in the absence of antecedent urges to smoke (Tiffany, Reference Tiffany1990). Research on the association between smoking cue reactivity and relapse is mixed, and evidence exists that some smokers do not respond to CET (Perkins, Reference Perkins2012; Wray et al., Reference Wray, Gass and Tiffany2013). However, these mixed results could be attributed in part to the wide range of cross-study exposure methods (e.g., guided imagery; visual slide presentation of cues; actual drug paraphernalia) and reactivity measures (e.g., self-reported urge, negative affect, heart rate) as well as to evidence that individual differences exist across smokers’ conditioning histories. These individual differences influence the degree to which a smoker may respond to specific individual cues or complex contextual cues (Collins et al., Reference Collins, Ibrahim, Hovell, Tolley, Nair and Jaffe2010; Perkins, Reference Perkins2009; Shadel et al., Reference Shadel, Niaura, Abrams, Goldstein, Rohsenow and Sirota1998; Unrod et al., Reference Unrod, Drobes, Stasiewicz, Ditre, Heckman and Miller2014). Moreover, there may exist a number of contexts and individual difference moderators that influence variability in urge response and whether urges lead to relapse or interfere with completion of substance dependence treatment (Collins & Brandon, Reference Collins and Brandon2002; Kavanagh, Andrade, & May, Reference Kavanagh, Andrade and May2005). Therefore, more research is needed to better understand the potential influence of individual difference characteristics, behavioural repertoires, or ‘traits’, that may contribute to variability in response to cue exposure procedures and CET outcomes.
We assert that persistence is a behavioural repertoire that could relate not only to one's response to CET procedures, but also to one's ability to maintain abstinence and manage cue-elicited reactivity (e.g., urges) after a quit attempt. Operationalised in Clonginger's theory of personality (Cloninger, Svrakic, & Przybeck, Reference Cloninger, Svrakic and Przybeck1993) and the theory of learned industriousness (Eisenberger, Michael Kuhlman, & Cotterell, Reference Eisenberger, Michael Kuhlman and Cotterell1992), persistence can be described as a relatively stable, but modifiable trait observed as the ability to maintain goal-directed effort in contexts that present mental or physical demands, or that elicit frustration or fatigue. During CET, individuals with higher trait persistence compared to those with lower persistence may respond more favourably to the demands of exposure procedures and unpleasant experience of conditioned reactivity, thereby increasing the likelihood of extinction learning.
The basis for this assertion is grounded in theory: Compared to individuals with a history of reinforcement for low effort in aversive contexts (e.g., challenging tasks and unpleasant situations), learned industriousness theory posits that individuals rewarded for high effort in aversive contexts are more likely in the future to persist in those contexts and experience their effort as less aversive over time. Smokers attempting to quit must exert high effort to avoid smoking while tolerating unpleasant nicotine withdrawal or during situations that elicit urges to smoke. Thus, greater persistence in maintaining abstinence when experiencing withdrawal or strong urges may facilitate extinction learning and, in turn, reduce relapse risk (Quinn, Brandon, & Copeland, Reference Quinn, Brandon and Copeland1996).
More recent studies show that persistence is associated with longer abstinence after a quit attempt in both retrospective (Brown, Lejuez, Kahler, & Strong, Reference Brown, Lejuez, Kahler and Strong2002; Steinberg, Williams, Gandhi, Foulds, & Brandon, Reference Steinberg, Williams, Gandhi, Foulds and Brandon2010) and prospective smoking intervention studies controlling for other factors associated with relapse (Brandon et al., Reference Brandon, Herzog, Juliano, Irvin, Lazev and Simmons2003). However, despite growing evidence of the predictive validity of persistence in smoking intervention research (Steinberg et al., Reference Steinberg, Williams, Gandhi, Foulds, Epstein and Brandon2012), results across studies show varying strengths of association between persistence and long-term smoking cessation outcomes (e.g., Brown et al., Reference Brown, Lejuez, Strong, Kahler, Zvolensky and Carpenter2009; Etter, Reference Etter2010; Kalman, Hoskinson, Sambamoorthi, & Garvey, Reference Kalman, Hoskinson, Sambamoorthi and Garvey2010). This inconsistency may be attributed, in part, to the differential use of self-report vs. behavioural task measures of persistence. Within Cloninger's typology and self-report measurement, persistence may represent one's cognitive appraisal of their ability to maintain engagement in aversive contexts. Alternatively, behavioural measures of persistence that require effortful performance with a challenging task appear to additionally capture variability in individuals’ emotional experience (e.g., frustration) arising from task demands. These observations have lead some researchers to consider that behavioural measures of persistence overlap with the construct of distress tolerance (Brandon, Vidrine, & Litvin, Reference Brandon, Vidrine and Litvin2007; Karekla, Champi, Panayiotou, & Collins, Reference Karekla, Champi, Panayiotou and Collins2015; Steinberg et al., Reference Steinberg, Williams, Gandhi, Foulds and Brandon2010). Thus, inconsistencies across self-report and behavioural studies may reflect what Kalman and colleagues (Reference Kalman, Hoskinson, Sambamoorthi and Garvey2010) suggest is the measurement of related, but different constructs: the construct of trait persistence as measured via self-report and the more emotion-based construct, distress tolerance, observed in behavioural tasks and characterised as one's perceived ability to endure distress during effort (Leyro et al., Reference Leyro, Zvolensky and Bernstein2010).
Despite previous inconsistencies between measures of persistence in predicting long-term cessation outcomes, there is growing evidence that trait-type persistence may be associated with decreased urges in both smokers and individuals with other addictions. For example, Zilberman, Tavares, & El-Guebaly (Reference Zilberman, Tavares and El-Guebaly2003) found that among treatment seeking women with substance-related disorders, greater persistence was associated with less craving. Etter's (Reference Etter2010) results suggest that, compared to current smokers, persistence is higher among former smokers who have achieved long-term abstinence perhaps because ex-smokers have had greater opportunity for reinforcement of their efforts to maintain abstinence across multiple urge-eliciting contexts. More recent studies expand evidence of the persistence-urge link: Panayiotou and colleagues (Karekla et al., Reference Karekla, Champi, Panayiotou and Collins2015; Panayiotou, Karekla, Champi, & Collins, Reference Panayiotou, Karekla, Champi and Collins2014) demonstrated that smokers reported greater urge reactivity following sustained effort with a stress inducing task (PASAT; Lejuez, Kahler, & Brown, Reference Lejuez, Kahler and Brown2003). Reactivity was mediated by increased negative affect during the task, and moderated by gender, such that increased negative affect appeared to be a more important catalyst to smoking urge among men compared to women.
Based on theory and collective evidence, persistence may be an important individual difference characteristic that differentiates smokers’ ability to tolerate urge-related consequences of abstinence. Therefore, persistence may be a relevant factor contributing to extinction learning, and help explain why some smokers experience habituation or extinction of cue reactivity more quickly than others in urge-eliciting situations during abstinence.
Aims
The goal of our study was to explore the association between abstinent smokers’ self-reported, trait-like persistence and urge reactivity across repeated cue exposure trials. The cue exposure procedures served as an analogue of a high relapse-risk, urge-eliciting situation with common smoking cues present. This study represents a secondary analysis of data from a previous study examining the role of negative affect on cue reactivity (Collins, Nair, & Komaroff, Reference Collins, Nair and Komaroff2011) which demonstrated a gender × time interaction with males reacting with significantly greater initial and sustained urge compared to women – results consistent with evidence of the moderating effect of gender on smoking cue reactivity (e.g., Perkins, Epstein, Grobe, & Fonte, Reference Perkins, Epstein, Grobe and Fonte1994). Given this evidence, the present study tested the hypothesis that low persistence would relate to greater sustained urges over time (resistance to urge extinction) and that within our cue exposure paradigm, the effect of persistence would be greater among men than women.
Methods
All procedures were approved by the institutional review board. The overarching design and methods for this study followed the parent study (Collins, Nair, & Komaroff, 2010). We recruited participants using print advertisements. Male and female current smokers and recent quitters with 6–12 months of abstinence were recruited to pilot test procedures and explore gender differences in urge reactivity across repeated trials. Participants were eligible if they were over 18-years old and had smoked more than 10 cigarettes daily. Ineligible participants reported a history of cardiac or pulmonary disease, current severe psychopathology (e.g., psychotic disorders), or current use of other tobacco products, nicotine replacement therapy, or psychotropic medication. Participants were instructed to maintain abstinence overnight and eat breakfast prior to their morning session and were excluded if pre-session CO was greater than 10 ppm. After completing informed consent, current smokers (not ex-smokers) were provided with 14 mg patch, thereby increasing the opportunity for observing conditioned urge responding not attributed to nicotine withdrawal. All participants waited in a lounge for 45 minutes to complete baseline assessments prior to cue exposure procedures described next.
Cue Exposure
Participants sat in a comfortable chair for procedural overview: the experimenter showed participants a partitioned, remote-controlled turntable used for cue presentation, describing that cues could include common objects (e.g., pen and paper) or smoking-related objects. Participants learned that audio instructions would guide them to use the objects and demonstrated how to light a cigarette without putting it in their lips. They were told that smoking was not permitted and that the experimenter would monitor their adherence during the session and test their CO after the session to verify sustained abstinence.
To habituate to the setting, participants completed a 15-minute resting baseline trial. Before each subsequent exposure trial, the experimenter set up the turntable and, 60 seconds later from the observation room, remotely rotated it to present cues while starting the audio instructions. The first minute of instructions guided participants to imagine using the items on the turn table. The remaining 4 minutes guided the participant to handle the objects and attend to specific features of the objects. Urge measures were obtained at the end of each trial.
For the first two exposure trials, participants were presented with neutral cues (paper and pencil) or smoking cues (a pack of the participant's brand of cigarettes, lighter, ashtray) in counterbalanced order. After these trials, the experimenter led participants to the research suite where they were invited to use the bathroom and instructed to drink one ounce of water. Participants then returned to the testing room to complete the remaining 5-minute trials. There were 12 total, consecutive smoking cue exposure trials using identical structure, timing, and materials. Participants imagined smoking, then were instructed to engage in a series of motor behaviours associated with smoking after lighting the cigarette while attending to the sight, smell, and tactile sensations related to the cigarette and smoke. After the fourth smoking cue trial, participants received a 30-minute break in the lounge with a standardised snack and one ounce of water. After the eighth trial, participants had a 5-minute stretch break with one ounce of water. At the conclusion of the last exposure trial, participants were debriefed and study compensation was offered.
Measures
Baseline assessments included questions related to participant characteristics and smoking history. All measures were chosen based on their psychometric strengths with a preference for shorter measures to reduce participant response burden.
Dependent variable: Self-reported urge to smoke was assessed as a repeated measure after each exposure trial using a single item on a 10-point Likert scale (0 = no urge at all to 9 = very strong urge). A single item scale was used to minimise participant burden across repeated exposure trials. Single item scales, including visual analogue scales are valid methods for assessing self-reported smoking urge (Ussher, Beard, Abikoye, Hajek, & West, Reference Ussher, Beard, Abikoye, Hajek and West2013; West & Ussher, Reference West and Ussher2010). To address convergence and interpretational difficulties that occurred using urge as a continuous dependent variable, urge was dichotomised at the median and modelled as a binary random variable with predicted values plotted as lines across trials.
Independent variable: Persistence was assessed at baseline using the five-item persistence dimension of the temperament personality questionnaire (a subset of the temperament and character inventory – version 9) (Cloninger, Przybeck, & Svrakic, Reference Cloninger, Przybeck and Svrakic1991; Cloninger, Przybeck, Svrakic, & Wetzel, Reference Cloninger, Przybeck, Svrakic and Wetzel1994). The scale is derived from Cloninger's neuro-psychological theory of personality traits which includes four inheritable dimensions of temperament: novelty seeking, harm avoidance, reward dependence and persistence (Cloninger et al., Reference Cloninger, Svrakic and Przybeck1993). Internal consistency of this scale with this sample (α = 0.725) suggested acceptable reliability.
Controlling covariates: Negative affect was assessed using the 20-item positive and negative affect schedule (PANAS; Watson, Clark, & Tellegen, Reference Watson, Clark and Tellegen1988b). Items are scored on a five-point Likert scale (1= very slightly or not at all to 5= extremely). Both positive and negative affect scales are internally consistent and demonstrate good convergent and discriminant validity (Crawford & Henry, Reference Crawford and Henry2004; Watson, Clark, & Tellegen, Reference Watson, Clark and Tellegen1988a). Nicotine withdrawal symptoms ratings were obtained using the Minnesota Withdrawal Symptom Checklist (WSC; Cappelleri et al., Reference Cappelleri, Bushmakin, Baker, Merikle, Olufade and Gilbert2005; Hughes & Hatsukami, Reference Hughes and Hatsukami1986) along with eight additional items that assessed physical symptoms. Items were rated on a four-point scale from ‘not present’ to ‘severe’. For the purpose of this study, we examined withdrawal-related symptoms other than urge, including ‘other physical symptoms’ (e.g., sweating, nausea), ‘energy’ (e.g., drowsiness, fatigue), and ‘hunger’. Smoking status differentiated between participants who enrolled as current smokers agreeing to be abstinent during procedures vs. recent quitters. Baseline smoking urge was assessed prior to the first smoking cue exposure trial.
Analysis
The sample size was too small to compare group differences between abstinent current smokers and recent quitters. The entire sample was used to facilitate power to test the study hypothesis. To characterise differences in urge that could be attributed to gender and persistence across trials, multilevel logistic growth curve models (Raudenbush & Bryk, Reference Raudenbush and Bryk2002) were developed with PROC GLIMMIX in SAS v9.2 (Littel, Stroup, Milliken, Wolfinger, & Schabenberger, Reference Littel, Stroup, Milliken, Wolfinger and Schabenberger2006). Because our previous analysis demonstrated significant effects of gender and time (and gender by negative affect by time) on smoking urge across trials (Collins, Nair, & Komaroff, Reference Collins, Nair and Komaroff2011), this analysis tested whether the probability of ‘above average urge’ (urge > 2 in this sample) could be modelled with an interaction by time, gender and persistence, after adjusting for baseline urge, smoking status and negative affect. Time was parameterised as an ordinal variable corresponding to trials. To model the theoretically predicted initial increase and subsequent decrease in urge, time was entered as a second-order polynomial. Baseline urge was group centred at the mean and included in the model to equate for any inter-individual differences in initial urge. Negative affect, defined as each subject's mean score on the PANAS across all data collection points, was dichotomised at the median and entered in the model as an indicator (0/1) covariate. The same approach was used for persistence with a median split to characterise high or low persistence. The initial steps involved in building the models are detailed previously (Collins et al., Reference Collins, Nair and Komaroff2011). Based on those previous results, we entered gender as a main effect as well as an interaction effect with linear and quadratic time. To determine if persistence moderated gender effects in initial trajectories (increase) of urge as well as later trajectories (decrease/extinction effect), persistence by gender was entered as an interaction with the linear and quadratic terms for time after adjusting for baseline urge, smoking status and negative affect.
Results/Findings
Forty-three participants, including thirty-three abstinent current smokers and ten recent quitters, completed the massed extinction trial session. One eligible smoker was not included in the analyses because of voluntarily withdrawing from the study after Trial 4. The final sample included 51% male, 54% African American, and 51% unemployed participants with a mean age of 49 ± 11-years old. Participants smoked for an average of 20.56 ± 10.83 years, and had a mean, baseline negative affect score of 17.44 ± 5.96. There were no significant differences between males and females on smoking status, psychosocial, or demographic variables except that males, on average, were older than females (t = 2.56, p < 0.02). There was no change in total WSC scores between the first and last smoking cue exposure trials. Table 1 displays mean age, cigarettes smoked per day (prior to cessation in the ex-smoker group) and percentage of ex-smokers and abstinent current smokers. There were no significant differences in these characteristics across the four subgroups of participants.
Table 1 Baseline age, cigarettes smoked, and smoking status by gender and persistence

In Table 2, ‘fixed effects’ represent overall beta coefficients and ‘variance components’ represent the variation (and covariation) in the random effects. Examination of the random effects revealed an extremely wide 95% confidence interval for the quadratic random effect (0.000397 to 31,082,743), thus was eliminated from the model. The final model demonstrates a significant persistence × gender × time interaction in the linear trajectories representing the initial increase in reactivity (p = 0.041) with a three-way quadratic interaction, representing change in reactivity trajectory, that approaches significance (p = 0.067) (see Table 2).
Table 2 Gender × persistence effects on change in urge trajectory across massed trials: Logistic growth curve modelling variance components
The individual slopes in the table and Figure 1 reveal that female trajectories were relatively flat (did not change with time or persistence), whereas the males had a significantly steeper linear effect corresponding to increasing urge. Moreover, males with high persistence demonstrated extinction in urge response (reduction in cue reactivity) compared to males with low on persistence, who demonstrated sustained smoking urge across trials. Table 3 further illustrates the group differences in urge by showing the mean peak urge by group midway through procedures and on the last trial. These data illustrate the gender difference, and the greater sustained urge reactivity among the low-persistence males vs. high-persistence males.
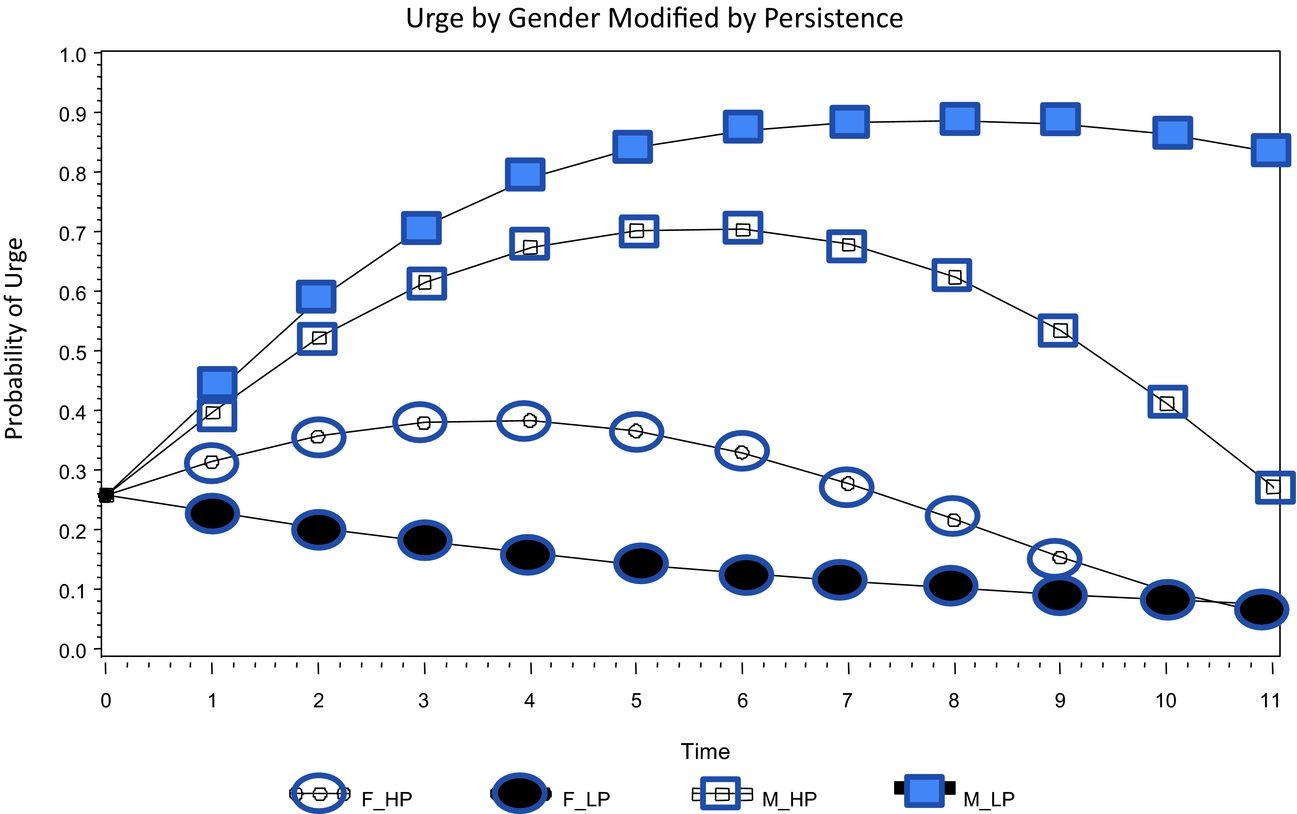
Figure 1 Probability of above average urge across cue exposure trials.
Table 3 Mean urge at peak reactivity and last extinction trial (Gender × persistence)

Note: Peak urge is the highest mean urge midway through exposure procedures (T4-6).
Conclusions
This study is the first to demonstrate the relation of persistence to the change in smoking cue reactivity (urge to smoke) across massed exposure trials. These results add to growing evidence that individual difference characteristics may influence smoking cue reactivity, and they expand our understanding of how persistence may relate to cue reactivity during abstinence. These results could inform future clinical trials and interventions that use cue exposure methods to promote extinction learning.
In this study, the gender by persistence interaction over time bears out a persistence-urge association among men, not women, when participants are exposed to a context that includes smoking cues proximally associated with nicotine self-administration. Specifically, this context presented smoking paraphernalia, the sight and smell of tobacco and smoke, branding from participants’ preferred cigarettes, and motor behaviours mimicking smoking. Abstinent male smokers with higher persistence trait scores demonstrated an initial increase in cue reactivity followed by extinction (reduction in urge). In contrast, men reporting lower persistence demonstrated greater, sustained urge reactivity during the session, suggesting they may be at greater risk for relapse in similar high-risk contexts. Given the potential for trait-like persistence to generalise across contexts, male smokers with low persistence who are attempting to quit smoking, may experience greater, sustained urge across contexts in which they are exposed to cigarette paraphernalia, tobacco smoke and other cues proximally related to nicotine self-administration.
In contrast to males, there was no difference in reactivity or subsequent extinction trajectories among women that related to persistence. In part, this outcome could be attributed to the overall low urge reactivity observed among female participants using this study's exposure procedures. Similar relative non-responsiveness of subsamples to exposure procedures is evident in CET approaches targeting other dependence disorders, and may suggest that the cue complex was not sufficiently salient to the subsample of female smokers. The lower reactivity of females relative to males in this study parallels other research demonstrating that women experience less reinforcement from nicotine than men (Perkins, Donny, & Caggiula, Reference Perkins, Donny and Caggiula1999). Indeed, other studies have demonstrated that gender may moderate reductions in urge elicited by negative affect (not smoking cues) (Unrod et al., Reference Unrod, Drobes, Stasiewicz, Ditre, Heckman and Miller2014). Perhaps, a cue exposure paradigm that is more salient to women may elicit adequate variability in urge reactivity needed to test the persistence hypothesis in women. Future research could consider using urge-eliciting contexts that include social cues or negative affect cues to test this hypothesis with female smokers.
Our results suggest treatment implications. Identifying individuals with low persistence could improve tailoring of behavioural strategies that shape persistence or provide more intensive coping skills training for those individuals. Early studies on persistence point to this implication, wherein training individuals to persist in high effort tasks could generalise to other behaviours necessary for ongoing treatment success (Nation & Woods, Reference Nation and Woods1980; Quinn et al., Reference Quinn, Brandon and Copeland1996). In addition to behavioural strategies, anti-craving medications that facilitate extinction of cue reactivity (e.g., Kamboj et al., Reference Kamboj, Massey-Chase, Rodney, Das, Almahdi and Curran2011; O'Brien, Reference O'Brien2005) may be an appropriate adjunct to CBT counselling for those who have greater challenges managing urges to smoke.
However, our results should be interpreted with caution due to the following limitations. This study used a small sample, which included non-treatment seeking current smokers and recent ex-smokers. The small subsamples precluded exploring smoking status group differences. Thus, our results may not generalise to all recent quitters, or those motivated to quit smoking. Also, the procedures included implementation of massed cue exposure trials over one long session using a single urge-eliciting context. Such approaches may have limitations when translated to practice due to post extinction renewal or reinstatement effects (Collins & Brandon, Reference Collins and Brandon2002; Conklin & Tiffany, Reference Conklin and Tiffany2002) and may restrict the manipulation of reactivity compared to procedures that employ a greater variety of cues and contexts. Future studies could test more translatable and tailored models of cue exposure, perhaps initially assessing moderators or individual differences in reactivity (Karekla et al., Reference Karekla, Champi, Panayiotou and Collins2015; Panayiotou et al., Reference Panayiotou, Karekla, Champi and Collins2014; Unrod et al., Reference Unrod, Drobes, Stasiewicz, Ditre, Heckman and Miller2014) affected by differences in conditioning history to identify the most salient cues to use with individual smokers in exposure sessions. Alternatively, clinicians could use spaced trial procedures across multiple sessions and contexts to improve generalisability of extinction learning. Despite the limitations, this study provides a first look into the influence of persistence on variability in smoking cue reactivity over time.
In conclusion, our results suggest that individual differences in persistence relate to abstinent smokers’ urge reactivity in a high-risk context. Specifically, men with low persistence reported greater sustained urge reactivity across multiple cue exposure trials compared to men with high persistence in an analogue context that included smoking cues most immediately associated with smoking behaviour (e.g., the sight, smell and tactile cues related to cigarette smoking). That the data did not bear similar results among women is likely due to the limited reactivity (low urge) among women to the experimental procedures. More can be learned about how trait-like persistence may relate to the magnitude and duration of abstinent smokers’ urge in situations that elicit strong urges. Because persistence is a modifiable individual difference characteristic, greater knowledge about a persistence – smoking urge association could guide targets of intervention tailoring to reduce relapse risk among abstinent smokers. To test the potential utility in translating this evidence to CET for nicotine dependence, future intervention research could explore the influence of boosting persistence as well as guiding coping skills during repeated exposure trials. Both the learned industriousness theory and associative learning theories suggest that such translation of cue exposure methods could facilitate extinction learning and promote effective compensatory coping for urge management, thereby improving the potential impact of behavioural intervention strategies in smoking cessation treatment.
Acknowledgements
The authors thank Jamie Dahm and James Kingham for data collection and management.
Financial Support
This research was supported by grants from the American Cancer Society Internal Research Grant mechanism distributed by the University of Pennsylvania Cancer Center and the Pennsylvania Department of Health Tobacco Fund distributed by Temple University to Collins. The funding sources were not involved in study design, collection, analysis, interpretation of data, writing this manuscript, or the decision to submit the manuscript for publication.
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.




