



Every year, over a third of the total European population suffers from psychiatric disorders. Major psychiatric disorders (such as bipolar disorder or schizophrenia) are associated with increased mortality with a median potential life loss of 10 years. This mortality gap between psychiatric disorders and the general population has increased in recent decades. Overall, 17% of the mortality of individuals with mental disorders is due to unnatural causes, including intentional (suicide) and unintentional (accidents or aggressions) causes.Reference Walker, McGee and Druss1 People with bipolar disorder have been found to have an increased standardised mortality ratio of 7.4 due to unnatural causes compared with the general population.Reference Hayes, Miles, Walters, King and Osborn2 In 2010, schizophrenia and bipolar disorder accounted for 7.4% (5.0–9.8) and 7.0% (4.4–10.3) of the total disability-adjusted life-years caused by mental and substance use disorders,Reference Whiteford, Degenhardt, Rehm, Baxter, Ferrari and Erskine3 respectively. These disorders have been associated with increased early mortality.Reference Kessing, Vradi, McIntyre and Andersen4,Reference Laursen5 Recent studies have suggested that patients with bipolar disorder or schizophrenia may not benefit from the same advances in the care of their physical health compared with the general population.Reference Ayerbe, Forgnone, Foguet-Boreu, González, Addo and Ayis6,Reference Fond, Tinland, Boucekine, Girard, Loubière and Auquier7 During the past decade, mortality rates following major trauma have steadily declined in the general population,Reference Skaga, Eken and Søvik8 but little is known about mortality in patients with severe psychiatric disorders. Bipolar disorder has been associated with an increased risk of fractureReference Su, Cheng, Huang, Lee, Yang and Lu9,Reference Hsu, Hsu, Chang, Lee, Chong and Wang10 and traffic accidents.Reference Chen, Yang, Lee, Wong, Ponton and Lee11 Both bipolar disorder and schizophrenia have been associated with inability to drive due to illness or treatment issues.Reference Laux and Brunnauer12 Despite decades of preventative measures, bipolar disorder and schizophrenia are still associated with high rates of suicide attempts, including violent suicide attempts with self-administered injuries. However, little is known about the care received by these patients who have unnatural causes of death, i.e. traumatic injury and self-harm. One may hypothesise that patients with severe mental disorders may not benefit from the same care as people without psychiatric disorders due to doctor- (e.g. stigmatisation) or patient-related factors (e.g. opposition, unawareness of the need for care, observance issues).
The objective of our study was to determine if the 30-day in-patient mortality from traumatic injury was increased in people with bipolar disorder and schizophrenia compared with people without psychiatric disorders.
Method
Study design and data source
This was a population-based study of all trauma patients in French institutions between 1 January 2016 and 31 December 2016, using the French national hospitalisations database (the Programme de Médicalisation des Systèmes d'Information [PMSI] or information systems medicalisation programme) in which administrative and medical information (diagnoses and surgical procedures) is systematically collected. The PMSI is based on diagnosis-related groups and all diagnoses are coded according to the ICD-10 (1992).Reference Boudemaghe and Belhadj13
Trauma patients were identified in accordance with a previous French study.Reference Bège, Pauly, Orleans, Boyer and Leone14 Trauma patients were first identified using a code of trauma (beginning with S or T according to the ICD-10 chapter ‘Injury, Poisoning and Certain Other Consequences from External Causes’) as the principal diagnosis of admission into an acute care unit. Second, we selected patients using the Trauma Audit & Research Network (TARN) criteriaReference Alexandrescu, O'Brien, Lyons, Lecky, Audit and Network15 (for more details, see16). Lastly, as dementia may be a specific cause of trauma (with increased risk of falling) and is increased in people with bipolar disorder and schizophrenia, patients with a diagnosis of dementia were excluded from the database (ICD-10 codes: F00*, F01*, F02*, F03*, F051*, G30*, G311*).
From this selection, we defined the following populations.
(a) Two groups of patients with psychiatric disorder (bipolar disorder group, schizophrenia group): these patients had diagnoses of bipolar disorder or schizophrenia according to the specific ICD-10 codes from the acute care hospitalisations database and the psychiatric hospitalisation database (F20*, F22* or F25* for schizophrenia; F30* or F31* for bipolar disorder).
(b) Two groups of mentally healthy controls: the controls were patients without psychiatric conditions according to the specific ICD codes (chapter F*) and without a psychiatric admission. Matching between patients with mental disorders and controls was performed using a 1:3 ratio according to four criteria: age, gender, social deprivation and geographical region of residence.
Outcome measure
The study outcome was the 30-day in-patient mortality.
Collected data
The following data were collected.
(a) Sociodemographic characteristics: age, gender and social deprivation index.Reference Rey, Jougla, Fouillet and Hémon17 The social deprivation index is constructed on the commune scale (smallest administrative unit in France), using the following socioeconomic data: percentage of high school graduates, median household income, percentage of blue-collar workers and unemployment rate. This index is based on the first component of a principal component analysis accounting for 68% of the total variation and can be used as a proxy of the social environment. We categorised this index according to quartiles from Q1 (least deprived) to Q4 (more deprived).
(b) Comorbidities based on the Charlson comorbidity index using the algorithm developed by Quan and colleagues.Reference Quan, Sundararajan, Halfon, Fong, Burnand and Luthi18 This index measures the burden of disease by weighting 17 different comorbid conditions. The score varies from 0 (fewer comorbid conditions) to 24 (more comorbid conditions).
(c) Trauma severity characteristics based on the following indicators: ICD-10-based Injury Severity Score (ICISS)Reference Gedeborg, Warner, Chen, Gulliver, Cryer and Robitaille19 with stratification according to Gedeborg and colleagues of minor (0.941–1.0), moderate (0.665–0.940), serious (0.355–0.664), severe (0.220–0.354) and critical severity (0–0.219); intensive care unit (ICU) admission; injury regions (head and neck, thorax, abdomen, limbs and multi-organ trauma which is defined by more than one trauma); blood transfusion; and surgery (presence of a surgical code on the French ‘Classification Commune des Actes Médicaux’ list). Length of stay in the acute care unit was also collected.
Ethics
Research on retrospective data are excluded from the framework of the French Law Number 2012-300 of 5 March 2012 relating to the research involving human participants, as modified by the Order Number 2016-800 of 16 June 2016. Neither the French competent authority (Agence Nationale de Sécurité du Médicament et des Produits de Santé, ANSM) approval nor the French ethics committee (Comités de Protection des Personnes, CPP) approval is required in this context.
Statistical analysis
The analyses were conducted in four steps.
First, we compared patients with psychiatric disorder (bipolar disorder group, schizophrenia group) and their respective matched controls (two control groups) for sociodemographic characteristics, comorbidities and trauma severity characteristics, using univariate conditional logistic regressions (to take into account correlations due to the 1:3 matching). For the quantitative variables, we used univariate mixed models with a matched cluster as a random effect.
Second, we explored the association between bipolar disorder, schizophrenia and mortality. Kaplan–Meier curves and log rank tests were performed. We also performed univariate and multivariate Cox proportional hazards analyses with a sandwich estimator (to take into account correlations due to the 1:3 matching) to estimate the hazard ratios and their corresponding 95% confidence intervals. The adjustment variables (i.e. sociodemographic characteristics, comorbidities and trauma severity characteristics) were included using a three-block step procedure to explore their influence on the relationships between bipolar disorder, schizophrenia and mortality. We carried out a three-step multivariate model for bipolar disorder and for schizophrenia: model 1 included age, gender and social deprivation index (block 1); model 2 included block 1 and Charlson comorbidity index (block 2); and model 3 included block 2 and trauma severity (i.e. head and neck trauma, blood transfusion, surgery, ICISS severity score and ICU admission).
Third, we compared the characteristics of bipolar disorder and schizophrenia using χ2 tests.
Fourth, where the information was available we explored the different causes of trauma which we categorised as follows: self-administered injuries (ICD codes X60–Z00*, except those listed for assaults), accidents (ICD codes V01*–X60*) and assaults (X85*, X89*, X91*–X99*).
Statistical significance was defined as P < 0.05. All statistical analyses were performed with SAS 9.4 for Windows (SAS Institute).
Results
Overall, 144 058 hospital admissions for traumatic injury were identified in France in 2016. From these we identified 1245 patients with bipolar disorder and 1891 patients with schizophrenia. After removing patients with dementia, a total of 1059 patients with bipolar disorder and 1575 patients with schizophrenia were matched with their mentally healthy controls (n = 3177 and n = 4725, respectively; flow chart on Fig. 1). Their characteristics are presented in Table 1.

Fig. 1 Flow chart showing the inclusion criteria for the study. BD, bipolar disorder; SZ, schizophrenia.
Table 1 Comparison of 1059 patients with bipolar disorder and 1575 with schizophrenia versus 1:3 matched mentally healthy controls

Matching between cases and controls was performed using a 1:3 ratio according to four criteria: age, gender, social deprivation and geographical region of residence. Q, quartile (from Q1 to Q4); ICISS, ICD-10-based Injury Severity Score.
*P < 0.05.
Comparison between patients with bipolar disorder and their controls
Compared with their respective controls, 1059 patients with bipolar disorder had more comorbidities with higher rates of renal disease (5.5 v. 3.8%, P = 0.017), peripheral vascular disease (4.3 v. 2.3%, P < 0.001), hemiplegia or paraplegia (6.8 v. 5.0%, P = 0.044), mild liver disease (5.5 v. 1.5%, P < 0.001), AIDS/HIV (1.1 v. 0.2%, P < 0.001), diabetes without complications (12.7 v. 8.1%, P < 0.001), cerebrovascular disease (7.4 v. 4.7%, P = 0.001), chronic pulmonary disease (9.2 v. 4.1%, P < 0.001) and myocardial infarction (4.2 v. 2.9%, P = 0.049). Patients with bipolar disorder had higher trauma severity, more ICU admissions (33.7 v. 26.4%, P < 0.001) and more multiple organ lesions (54. 9 v. 48.0%, P < 0.001), head and neck trauma (36.0 v. 26.2%, P < 0.001) and thorax trauma (42. 6 v. 36.9%, P < 0.001). Patients with bipolar disorder also had more blood transfusions (14.0 v. 8.6%, P < 0.001) but fewer surgical procedures (54.3 v. 57.9%, P = 0.042) than their respective controls (Table 1).
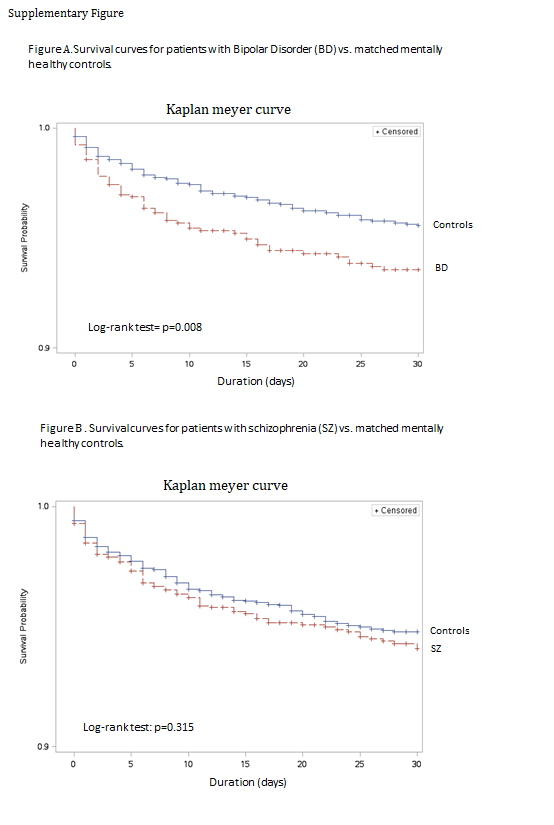
A total of 60 (5.7%) of the 1059 patients with bipolar disorder died within the 30 days after admission versus 105 (3.3%) controls (hazard ratio 1.53, CI 95% [1.12–2.09], P = 0.007) (Table 2). The Kaplan–Meier survival curves are shown in Supplementary Figures available at https://doi.org/10.1192/bjp.2019.139. These curves show a significant difference in survival time between patients with bipolar disorder and their controls (log rank test P = 0.008). In the multivariate analysis (Fig. 2), bipolar disorder diagnosis remained significantly associated with increased mortality after adjustment for sociodemographic characteristics (adjusted hazard ratio 1.56, CI 95% [1.14–2.13], P = 0.005; model 1) and after adjustment for comorbidities (adjusted hazard ratio 1.50, CI 95% [1.09–2.06], P = 0.012; model 2). After adjustment for trauma severity, bipolar disorder diagnosis was not significantly associated with 30-day in-patient mortality (P > 0.05; model 3).

Fig. 2 Results from the multivariate analysis. (a) Forest plots showing adjusted hazard ratios of 30-day in-patient mortality in the population of people with bipolar disorder and their matched mentally healthy controls (multivariate Cox regression analysis). (b) Forest plots showing adjusted hazard ratios of 30-day in-patient mortality in the population of people with schizophrenia and their matched mentally healthy controls (multivariate Cox regression analysis).
Table 2 Factors associated with 30-day in-patient mortality in people with bipolar disorder, people with schizophrenia and their matched mentally healthy controls (univariate Cox model)

Q, quartile (from Q1 to Q4); ICISS, ICD-10-based Injury Severity Score.
*P < 0.05.
Comparison between patients with schizophrenia and their controls
Compared with their respective controls, 1575 patients with schizophrenia had more comorbidities with higher rates of renal disease (4.3 v. 2.8%, P = 0.003), peripheral vascular disease (3.0 v. 1.8%, P = 0.004), peptic ulcer disease (1.4 v. 0.3%, P < 0.001), hemiplegia or paraplegia (7.9 v. 4.8%, P < 0.001), moderate or severe liver disease (2.4 v. 0.2%, P < 0.001), mild liver disease (5.7 v. 1.0%, P < 0.001), leukaemia and lymphoma (5.5 v. 4.2%, P = 0.031), AIDS/HIV (1.3 v. 0.4%, P < 0.001), diabetes with and without complications (3.2 v. 1.7%, P < 0.001 and 11.6 v. 6.8%, P < 0.001, respectively), cerebrovascular disease (7.3 v. 4.3%, P < 0.001), chronic pulmonary disease (9.0 v. 3.6%, P < 0.001) and congestive heart failure (6.4 v. 4.5%, P = 0.002). Individuals with schizophrenia had higher trauma severity, more ICU admissions (41.0 v. 31.8%, P < 0.001), more multiple organ lesions (56.7 v. 53.7%, P = 0.037), head and neck trauma (37.3 v. 29.8%, P < 0.001) and limb trauma (54.8 v. 51.5%, P < 0.001) than controls. Individuals with schizophrenia also had more blood transfusions (13.4 v. 8.3%, P < 0.0001), but there was no difference in surgical procedures.
A total of 80 (5.1%) of the 1575 patients with schizophrenia died within the 30 days after admission versus 181 (3.8%) controls (Table 2). The Kaplan–Meier survival curves are presented in Supplementary Figures and there were no significant differences in survival time between individuals with schizophrenia and their respective controls (log rank test P = 0.315). In the multivariate analysis (Fig. 2), schizophrenia diagnosis was not associated with mortality in any of the block-step analyses.
Comparison between patients with bipolar disorder and schizophrenia
Compared with those with bipolar disorder, individuals with schizophrenia had more ICU admissions (41.0 v. 33.7%, P < 0.001), less abdominal or limb trauma (33.0 v. 28.7%, P = 0.019 and 54.8 v. 49.0%, P = 0.004, respectively) and more surgical procedures (60.7 v. 54.3%, P = 0.001) (Supplementary Table). There was no statistically significant difference in 30-day mortality between people with bipolar disorder and schizophrenia (P = 0.511).
Trauma circumstances
Trauma circumstances were identified for 465 (44%) people with bipolar disorder and 659 (42%) people with schizophrenia. Bipolar disorder and schizophrenia diagnoses were both significantly associated with higher rates of self-administered injuries (bipolar disorder 24.9% v. controls 0.6%, P < 0.001; schizophrenia 31.1% v. controls 1.3%, P < 0.001) and lower rates of accidents (bipolar disorder 79.8% v. controls 98.3%, P < 0.001; schizophrenia 71.0% v. controls 97.0%, P = 0.001). There was no statistically significant difference in assault.
Compared with bipolar disorder, patients with schizophrenia had higher rates of self-administered injuries (31.1 v. 25.0%, P = 0.024) and assaults (3.5 v. 1.5%, P = 0.042) and lower rates of accidents (79.8 v. 71.0%, P < 0.001).
Self-administered injury was associated with 30-day mortality after adjustment for age, gender, social deprivation and psychiatric diagnosis.
Discussion
The first major finding of our study is the increased mortality rate of 5.1–5.7% in people with bipolar disorder or schizophrenia versus 3.3–3.8% in their respective controls. However, these mortality rates are lower than that of our entire database (5.9%),Reference Bège, Pauly, Orleans, Boyer and Leone14 probably due to the exclusion of dementia diagnoses. Indeed, this exclusion may have decreased the mean age, comorbidities and trauma severity in our sample. To our knowledge, this is the first time that these findings are reported in psychiatric patients; no study released from TARN has explored the association between trauma mortality and mental health. Our results suggest that mortality is increased only in people with bipolar disorder (but not in people with schizophrenia) due to trauma severity but not sociodemographic characteristics and comorbidities.
People with bipolar disorder and schizophrenia were found to have higher trauma severity and more self-administered injuries than their matched controls. These findings suggest that people with severe mental illnesses may have more severe suicide attempts. For example, the larger number of head and neck trauma and blood transfusions may be due to the use of sharp objects to cut their throats.Reference Hayes, Miles, Walters, King and Osborn2 People with schizophrenia were found to have more ICU admissions than controls and people with bipolar disorder. These results may be explained by a higher risk of intentional falls in people with schizophrenia, for example. The present database did not include more specific circumstances of trauma, which should be explored in further studies.
This study has also yielded important findings on comorbidities of people with severe mental illness. First, people with bipolar disorder and schizophrenia have more cardiovascular diseases, diabetes and liver and renal diseases. The increased rates of comorbid cardiovascular and diabetes are well known and have led some authors to describe severe psychiatric disorders as multisystem inflammatory diseases. Renal disease in psychiatric patients may be due to diabetes medication and lithium prescriptions. Second, patients with bipolar disorder and schizophrenia had rates of HIV/AIDS that were more than threefold higher than their matched controls. This is consistent with current literature reporting 2.6- to 4-fold higher rates of HIV among people with severe psychiatric disorders compared with the general population.Reference Bauer-Staeb, Jörgensen, Lewis, Dalman, Osborn and Hayes20 No data on HIV prevalence in people with bipolar disorder/schizophrenia in France have been published to date. Future studies should determine the HIV prevalence in people with severe mental illnesses in the whole French population to guide future health prevention programmes.
Limitations
Some illness characteristics (age at onset, duration of untreated illness, illness duration, psychiatric comorbidities and addictive behaviour) were not available in this medico-administrative database. Although being White has been associated with an increased risk of suicide in people with schizophrenia,Reference Cassidy, Yang, Kapczinski and Passos21 no ethnicity variables are reported in this study due to French laws. Smoking status was not available, although psychiatric patients have been found to smoke tobacco more frequently than the general population. However, tobacco has been shown to play only a minimal role in trauma-related mortality. Data on alcohol use disorder were also not systematically collected, but it has been shown to be increased in major psychiatric disorders. The background regimen of psychiatric patients was not available in our database and may have a role in trauma occurrence, such as traffic accidents.Reference Chen, Yang, Lee, Wong, Ponton and Lee11,Reference Laux and Brunnauer12 However, to date no current data suggest that psychotropic drugs affect trauma mortality.
Strengths
The strength of this study is the inclusion of more than 144 000 patients. To our knowledge, this is the largest epidemiological study performed in the field of trauma in France. We used a dedicated method of patient selection which has been validated by TARN.Reference Bouamra, Wrotchford, Hollis, Vail, Woodford and Lecky22 Professionals can use this study to provide accurate and relevant information to patients and their relatives.
Perspectives
Altogether these results suggest that a bipolar disorder diagnosis along with increased trauma severity and intentional injury should be added as independent risk factors for increased 30-day mortality after hospital admission. These results should be replicated in populations with other psychiatric diseases. Lithium is the most well-known mood stabiliser prescribed to people with bipolar disorder and schizoaffective disorder and it has been associated with a reduced risk of self-harm and unintentional injury.Reference Hayes, Pitman, Marston, Walters, Geddes and King23 It may therefore be suggested that people with bipolar disorder with a history of trauma may benefit from lithium therapy if they are responsive to this medication and if their renal profile is compatible with lithium therapy (as lithium may increase the risk of nephrotoxicity). Future studies should determine whether lithium onset in patients with bipolar disorder and schizoaffective disorder may decrease the risk of trauma. Moreover, lithium has been associated with increased motoneuron survival and regrowth by inhibiting glycogen synthase kinase 3β activation, which may be helpful in the case of severe traumas with neuronal injuries.Reference Fu, Tang, Ling, Li, Cheng and Song24,Reference Su, Yuan, Qin, Yang, Wong and So25 Lithium has also shown neuroprotective effects after traumatic brain injuries by multiple additional mechanisms including inflammation modulation, anti-apoptotic effects and increased growth factors. In people with bipolar disorder, the use of antidepressants has been associated with a lower risk of traffic accidents.Reference Chen, Yang, Lee, Wong, Ponton and Lee11 Benzodiazepines have been associated with higher impulsivity, disinhibition, aggressiveness and lower attention in people with bipolar disorder and schizophrenia, and these medications may be involved in increased falls, traffic accidents, aggression and suicidal behaviour.Reference Laux and Brunnauer12 Benzodiazepines should therefore be withdrawn as soon and as often as possible in people with bipolar disorder and schizophrenia who have been hospitalised for trauma. We took social deprivation into account in this study, but trauma should be further explored in the subpopulation of homeless people with severe mental disorders who have specific illnesses and treatment issues.Reference Fond, Tinland, Boucekine, Girard, Loubière and Auquier7
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjp.2019.139.
Funding
This work was funded by Assistance Publique des Hôpitaux de Marseille and Aix-Marseille University.








eLetters
No eLetters have been published for this article.