


A growing body of evidence suggests a role for season of birth in determining susceptibility to a wide range of psychiatric disorders such as schizophrenia, bipolar disorder, major depression and suicidal behaviour. Reference Davies, Welham, Chant, Torrey and McGrath1,Reference Torrey, Rawlings, Ennis, Merrill and Flores2 This hypothesis has been investigated in people with anorexia nervosa and other eating disorders; Reference Rezaul, Persaud, Takei and Treasure3–Reference Winje, Willoughby and Lask8 however, although an excess of spring births has been suggested, results are conflicting and rarely achieve statistical significance. The reasons for this conflict are at least twofold. First, season-of-birth studies require a large number of cases to achieve sufficient statistical power to detect small differences in seasonal births between patients and controls. However, these studies only looked at a few hundred people with anorexia, resulting in less than 30% power to detect the presence of a seasonal risk factor with an odds ratio of 1.2. Second, differences in the statistical tests used may provide another explanation for conflicting results. Standard techniques such as a simple chi-squared tests (used in most of the previous studies on anorexia) are easy to perform but non-standard techniques such as harmonic and spectral analysis are more powerful and suitable for this type of investigation. Reference Hakko9 We therefore performed a meta-analysis on four UK cohorts of individuals with anorexia nervosa, making this the largest study to assess the presence of a season-of-birth effect in anorexia.
Method
The PubMed database was searched using the search strings “anorexia nervosa AND season”, “anorexia AND month” and “ anorexia AND birth” to identify relevant articles. Given the potential confounding role of country-specific factors such as different social and nutritional habits, disease prevalence, birth trends and latitude, we decided to include only studies from the UK. Online Table DS1 shows the main features and findings of the studies included in the meta-analysis.
A pooled total of 1293 anorexia nervosa births were compared with those of the general population born between 1950 and 1980 (n = 21 914 037) obtained from the UK Office for National Statistics (www.statistics.gov.uk/). This birth interval (1950–1980) matches that of the individuals with anorexia. To assess the presence of a month-of-birth effect in anorexia nervosa, we used both the Walter & Elwood's seasonality Reference Walter and Elwood10 and chi-squared tests. With the Walter & Elwood's seasonality test it is possible to estimate within-year fluctuations with a 12-month periodicity (simple harmonic seasonal variation). Our study had a power of 80% to detect the presence of a seasonal factor with an odds ratio (OR) of 1.2.
Results
The monthly distributions of anorexia births and general population births across the year are shown inFig. 1. Using the Walter & Elwood's test, the birth distribution of those in the anorexia nervosa group was found to be significantly different from that of the general population (P = 0.02). To confirm these findings we performed a chi-squared analysis. Similarly, the birth distribution of those in the anorexia nervosa group significantly differed from that of the general population, being higher in the first half of the year compared with the second half (OR = 1.13, 95% CI 1.01–1.26, P = 0.025). Further analyses highlighted an excess of anorexia nervosa births from March to June (OR = 1.15, 95% CI 1.03–1.29, P = 0.012) and a deficit from September to October (OR = 0.8, 95% CI 0.68–0.94, P = 0.007) in comparison with the rest of the year. The peak-to-trough ratio was then evaluated comparing the periods March–June with September–October (OR = 1.31, 95% CI 1.1–1.56, P = 0.001).
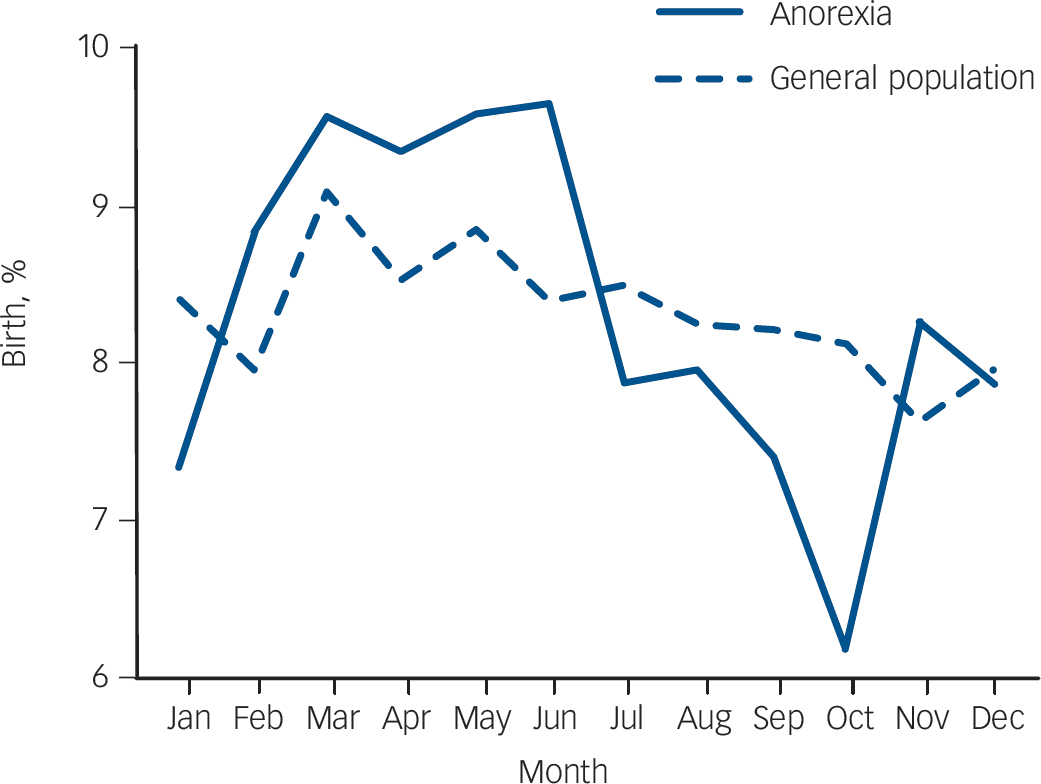
Fig. 1 Percentage distribution of births in individuals with anorexia and the general population.
Discussion
In line with the ‘fetal origin of adult disease’ hypothesis, formulated by David Barker, it is now acknowledged that early-life exposure to environmental factors may influence the risk of late-onset diseases. Reference Langley-Evans and McMullen11 Here we provide clear evidence in support of a season-of-birth effect in anorexia nervosa. A number of studies have shown such an effect in psychiatric disorders. Thus, the presence of similar findings in anorexia is perhaps not surprising. By using a large sample size of people with anorexia nervosa and controls and adopting both standard (chi-squared) and non-standard (Walter & Elwood) statistical approaches, we were able to confirm more confidently what other studies had previously only suggested. Consistent with our findings, an excess of anorexia and bulimia nervosa births during the spring was observed in other studies, raising the possibility that the same factor(s) could also influence susceptibility to other eating disorders. However, small sample sizes, inappropriate statistical methodologies and conflicting results did not allow any definite conclusion. Reference Winje, Willoughby and Lask8 Intriguingly, a similar excess of spring births has also been observed in major depression, perhaps suggesting the presence of shared environmental risk factors acting early in life. Reference Torrey, Rawlings, Ennis, Merrill and Flores2 Also of interest is a recent study reporting an interaction between the D4 dopamine receptor gene and season of birth influencing body weight regulation in women with bulimia nervosa. Reference Levitan, Kaplan, Davis, Lam and Kennedy12
It is important to understand that the season-of-birth effect can be considered as a marker of several environmental agents influencing disease risk. The excess of spring births could be the consequence of environmental factor(s) acting at any time from conception to the first postnatal months. Thus, the identification of the relevant factors remains a challenging goal. However, seasonal changes in temperature, sunlight exposure and consequent vitamin D levels, maternal nutrition and infections are all strong candidate factors. Intriguingly, vitamin D levels have been shown to be associated with psychiatric disorders. Reference Kinney, Teixeira, Hsu, Napoleon, Crowley and Miller13 Although the presence of low vitamin D levels in people with psychiatric illness may be the consequence of reverse causation, further support for a role for vitamin D comes from functional studies showing that it is also involved in neuroprotection and brain development. Reference Fernandes de Abreu, Eyles and Feron14,Reference Eyles, Feron, Cui, Kesby, Harms and Ko15
To conclude, using the largest cohort of people with anorexia to date, we demonstrated that susceptibility to anorexia nervosa is significantly influenced by the season of birth, with higher rates in those individuals born in the spring and lower ones in those born in the autumn. Future studies with even larger sample sizes in different populations and at different latitudes are needed to confirm these findings. Identification of the relevant seasonal risk factors will undoubtedly be important for future disease prevention strategies.
Funding
This work was supported by the Wellcome Trust ().



 Open access
Open access
eLetters
No eLetters have been published for this article.